Abstract
Zinc is an essential trace element involved in diverse physiological processes in humans. Zinc deficiency is common in patients with chronic kidney disease (CKD), including those undergoing hemodialysis. This narrative review synthesizes both experimental and clinical findings on zinc status in CKD patients. Literature was primarily retrieved from PubMed using the keywords “zinc” AND (“CKD” OR “hemodialysis”) AND at least one of the following: “cardiovascular disease (CVD)”, “vascular calcification”, “anemia”, “blood pressure”, OR “infection”. In vitro, studies have shown that zinc suppressed phosphate-induced vascular calcification while zinc deficiency directly promoted calcification. Clinically, serum zinc levels were positively correlated with calcification propensity in patients with CKD. In vivo zinc deficiency has been implicated in elevated blood pressure, Moreover, zinc supplementation enhanced erythropoiesis and improved responsiveness to erythropoiesis-stimulating agents in both animal models and humans. We recently reported that low serum zinc levels are associated with increased mortality in hemodialysis patients with hypoalbuminemia. Previous randomized controlled trials (RCTs) suggest a daily dose of approximately 45 mg of zinc for 2 months mitigates inflammation, oxidative stress, and malnutrition in patients undergoing hemodialysis. Emerging evidence suggests that vascular calcification, hypertension, and renal anemia are newly recognized features of zinc deficiency and are established risk factors for CKD progression, CVD, and mortality. However, the impact of zinc supplementation on these clinical outcomes remains inconclusive. Further RCTs are required to establish zinc supplementation as an effective therapeutic strategy for improving various outcomes in patients with CKD including hemodialysis.
1. Introduction
Zinc is an essential trace element and the second most abundant divalent cation in the body [1]. Zinc deficiency is a global issue, affecting over two billion people [2]. In patients with CKD, including those undergoing hemodialysis, zinc deficiency results from multiple factors, including inadequate dietary intake due to uremia-related anorexia and dietary restrictions, impaired absorption caused by certain medications, increased urinary zinc excretion associated with CKD progression, and zinc removal during dialysis [3,4,5]. Additionally, in a rodent model of CKD induced by 5/6 nephrectomy, elevated intestinal luminal phosphate levels caused by hyperphosphatemia and/or dietary phosphate intake impaired intestinal zinc absorption, leading to zinc deficiency [6] (Figure 1). Zinc concentrations are categorized according to the guidelines for zinc deficiency by the Japanese Society of Clinical Nutrition as follows: deficiency (<60 μg/dL), marginal deficiency (≥60 to <80 μg/dL), and normal (≥80 μg/dL) [7]. Marginal zinc deficiency is commonly observed in patients with pre-dialysis CKD, whereas zinc deficiency is predominant among those undergoing hemodialysis [8]. We have previously demonstrated a reduced blood zinc levels in patients with CKD including those undergoing hemodialysis [8]. A recent meta-analysis, which included 42 studies with patients with CKD (n = 460), hemodialysis (n = 2047), and healthy controls (n = 1657) showed that blood zinc levels in patients with CKD and hemodialysis were significantly lower than those in healthy controls (mean difference = −22.86 μg/dL, 95% CI −33.25 to −12.46; mean difference = −13.64 μg/dL, 95% CI −21.47 to −53.80, respectively) [9].
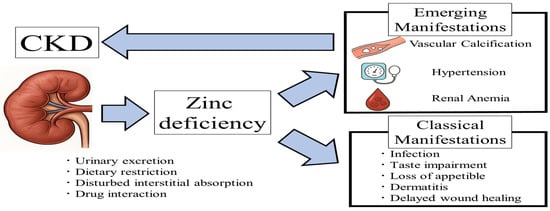
Figure 1.
Associations between CKD and clinical manifestations of zinc deficiency.
The daily requirement of zinc for adults throughout the world vary and are as follows: WHO—for females 3.0–9.8 mg/d, and for males 4.2–14.0 mg/day; the European Food Safety Agency—7.5–12.7 mg/day for females and 9.4–16.3 mg/day for males, the amount depending on the phytate in the diet [10]; and dietary intake of zinc in Japan for adults—9–10 mg/day for males and 7–8 mg/day for females [11], although intake is insufficient in 60–70% of both genders aged over 20 years [7]. Additionally, zinc intake was found to be lower in patients with advanced stage CKD as compared with those without advanced stage CKD who participated in the National Health and Nutrition Examination Survey conducted in the United States [12]. Patients with zinc deficiency including CKD are initially recommended to consume zinc-enriched foods, e.g., oysters, scallops, tofu, rice, and fermented soybeans (Natoo) [7].
When dietary therapy is insufficient, the Practical Guideline recommends administering zinc to patients with zinc deficiency at a dosage of 50–100 mg/day for adults [7]. Organic compounds such as zinc histidinate, zinc gluconate and zinc orotate show a comparatively better tolerability than inorganic zinc sulfate and zinc chloride [13]. A total of 20 RCTs have investigated zinc supplementation in patients undergoing hemodialysis (Table 1) [14,15,16,17,18,19]. These findings suggest that a daily dose of approximately 45 mg of zinc for 2 months resulted in increased serum zinc levels, SOD activity, and dietary protein intake, as well as reduced levels of C-reactive protein (CRP) and malondialdehyde [18]. Another meta-analysis reported that zinc supplementation led to increases in body weight and/or body mass index (BMI) in patients undergoing hemodialysis [20].

Table 1.
Summary of RCTs of zinc supplementation in patients with hemodialysis.
In patients with CKD, including those undergoing hemodialysis, zinc deficiency arises from multiple factors. In addition to classical manifestations of zinc deficiency, emerging evidence highlights vascular calcification, hypertension, and renal anemia as newly recognized features of zinc deficiency. These emerging manifestations have been identified as the risk factors for CKD progression. Abbreviations: CKD, chronic kidney disease.
Zinc serves as an essential cofactor for the activity of approximately 300 zinc-containing enzymes, including DNA polymerase, RNA polymerase, alcohol dehydrogenase, carbonic anhydrase, and superoxide dismutase (SOD) [36,37]. Bioinformatics research suggests that approximately 2800 human proteins may function as zinc-binding proteins [38]. In addition to traditional symptoms of zinc deficiency such as taste impairment [39], anorexia and loss of appetite [40], dermatitis [41], delayed wound healing [42], and infection [43], other clinical manifestations including vascular calcification, hypertension, and renal anemia, have been increasingly recognized in patients with CKD [44] (Figure 1). These emerging features of zinc deficiency are associated with adverse outcomes, including progressive kidney dysfunction, cardiovascular disease (CVD) events, and increased mortality. Regarding other trace elements, including magnesium and selenium, low serum levels of these elements have been consistently associated with CKD progression in pre-dialysis patients [45,46,47], as well as with all-cause mortality in patients undergoing hemodialysis [48,49]. However, evidence regarding the association between serum zinc levels and these clinical outcomes remains relatively limited.
The purpose of this review is therefore to clarify the clinical implications of zinc deficiency in patients with CKD, particularly those undergoing hemodialysis, and to provide a comprehensive overview of experimental and clinical studies investigating zinc supplementation strategies. This narrative review synthesizes both experimental and clinical findings on zinc status in CKD patients. Literature was primarily retrieved from PubMed using the keywords “zinc” AND (“CKD” OR “hemodialysis”) AND at least one of the following: “CVD” “vascular calcification”, “anemia”, “blood pressure”, OR “infection”. These studies have investigated various dosages and frequencies, as well as the potential effects of zinc supplementation in CKD. Through this review, we aim to emphasize the need for well-designed future clinical trials to confirm the therapeutic value of zinc supplementation in this population.
2. Zinc and Calcification
2.1. Vasculature Smooth Muscle Cells
Phosphate was first identified as essential for calcification in vascular smooth muscle cells (VSMCs) more than 25 years ago [50]. Since then, numerous studies have investigated potential factors that could mitigate phosphate-induced calcification. Among these, magnesium [51,52] and zinc [53,54] have been identified as playing critical roles in inhibiting phosphate-induced calcification in VSMCs. Regarding zinc, zinc sulfate was shown to blunt phosphate-induced calcification and decrease messenger RNA expression of osteogenic markers. The inhibition of cellular calcification by zinc is partly mediated through the zinc-sensing receptor GPR39 [54,55,56]. In the experiment using primary human aortic VSMCs and klotho-hypomorphic, subtotal nephrectomy, and cholecalciferol-overload mouse calcification models, zinc activated tumor necrosis factor α-induced protein 3 (TNFAIP3), which inhibits nuclear factor kappa B (NF-κB) activation and osteo-/chondrogenic reprogramming, thereby suppressing phosphate-induced calcification in VSMCs [54]. Additionally, zinc sulfate inhibited VSMCs calcification induced by high glucose levels through the suppression of NF-κB activation [56].
Interestingly, zinc deficiency has also been reported to directly promote calcification. In rat aortic VSMCs under zinc-deficient conditions, the expression of Pit1, a sodium-dependent phosphate transporter that facilitates phosphate uptake and regulates calcification was significantly upregulated. Subsequently, treatment with a Pit1 inhibitor ameliorated these calcifications in rat aortic VSMCs [57]. Furthermore, excessive zinc specifically inhibited the in vitro osteogenic differentiation of bone marrow-derived mesenchymal stem cells (BMSCs) by regulating phosphate uptake. This resulted in the downregulation of key osteo-chondrogenic transcription factors Runt-related transcription factor 2 (RUNX2) and SRY-box transcription factor 9 (SOX9), along with their target genes osteocalcin (OCN) and alkaline phosphatase (ALP) [58]. These in vitro findings suggest that zinc may be a critical microelement for inhibiting phosphate-induced calcification.
2.2. Serum Calcification Propensity: T50
In serum, precipitation of supersaturated calcium and phosphate is prevented by the formation of amorphous calciprotein particles (CPPs) [59,60]. CPPs is a colloidal mineral–protein complex mainly composed of solid-phase phosphate, calcium, and serum protein fetuin-A [61,62]. Small and spherical CPPs (primary CPPs) which contain amorphous calcium phosphate clusters, spontaneously convert into aggregate and transform into larger and irregular-shaped ones (secondary CPPs). These secondary CPPs contain crystallized calcium phosphate and exhibit cytotoxic and proinflammatory properties, promoting inflammation, atherosclerosis, and vascular calcification [63,64].
Serum calcification propensity, referred to as T50 [65] is biomarker of vascular calcification [66]. T50 is measured using nephelometry, which detects laser light scatter in turbid samples. The assay relies on the formation of primary CPPs by addition of exogenous calcium and phosphate to a human serum sample. The T50 value represents the time required for 50% of primary CPPs to convert into secondary CPPs. A shorter T50 indicates a higher propensity for calciprotein crystallization, reflecting increased calcification stress [65]. Notably, a shorter T50 has been associated with arterial calcification [67] and a higher risk for CVD events and all-cause mortality in patients with CKD including hemodialysis [66,67,68,69,70,71]. Therefore, T50 is considered as a surrogate marker of calcification stress and is closely associated with CVD risk in those patients.
A positive correlation between serum zinc levels and T50 has been observed in both individuals with normal kidney function (r = 0.328, p = 0.013) and patients with CKD (r = 0.265, p = 0.002) [54]. Similarly, our cross-sectional study involving 132 patients with type 2 diabetes mellitus and varying kidney function also reported a positive correlation (r = 0.219, p = 0.012) [72], in which serum T50 was determined in duplicate over a period of 600 min per measurement using a nephelometer (Nephelostar Plus®, BMG Labtech, Saitama, Japan), and the measurement results were analyzed using the MARS software (BMG Labtech, Saitama, Japan). We also demonstrated that addition of a physiological concentration of exogenous zinc chloride significantly increased serum T50 [72]. Furthermore, a recent study found that higher serum zinc levels were associated with a longer T50 and a lower hydrodynamic radius of secondary CPPs in patients with CKD including those undergoing hemodialysis (r = 0.488, p < 0.001) [73]. When 100 µM zinc (corresponding to 6538 µg/L) was added to serum samples from healthy volunteers, T50 was prolonged. In contrast, a much higher concentration of 1 mM was required to reduce the hydrodynamic radius of secondary CPPs, suggesting that the direct effect of zinc may have a greater impact on T50 than on the size of secondary CPPs [40]. Even in polyethylene glycol hydrogels, not in serum, zinc was shown to inhibit the transformation of amorphous calcium phosphate (ACP) into hydroxyapatite [74]. In additive-free composite, ACP transformed into brushite within minutes. In contrast, in the presence of zinc, zinc-doped ACP was very stable and did not show any signs of crystallization for up to 20 days. In ACP, zinc ion readily substitutes calcium, suppressing crystallization by decreasing solubility [75]. It is thus likely that zinc suppresses the transformation from amorphous primary CPPs into secondary CPPs, containing crystalline hydroxyapatite, in serum. Although the precise mechanism by which zinc prolongs T50 remains unclear, its inhibitory effect on hydroxyapatite formation in vitro [76] may contribute to this phenomenon.
2.3. Vasculature Change
Coronary artery calcification (CAC) is highly prevalent in patients with CKD [77]. The CAC score has been strongly and significantly associated with an increased risk of subsequent CVD and all-cause mortality, as evidenced by findings from the Chronic Renal Insufficiency Cohort study [78]. Regarding zinc and CAC scores, whole blood zinc levels in patients with CKD were found to be significantly and negatively correlated (r = −0.601, p < 0.001) [79].
Abdominal aorta calcification (AAC) is also common in CKD and is recognized as an independent predictor of cardiovascular mortality in both the general population and patients with CKD [80,81]. Serum zinc levels were significantly and negatively associated with AAC score in patients undergoing hemodialysis (r = −0.43, p = 0.005) [82]. Among non-institutionalized CKD patients in the United States, whose mean dietary zinc intake was 10.5 mg/day, each 1 mg/day increase in zinc intake was associated with a reduced risk of severe AAC after adjustment for age, gender, and ethnicity [12].
Carotid intima-media thickness (CIMT) is a valuable marker of subclinical atherosclerosis [83]. In a study of middle-aged and older adults, individuals with lower zinc intake exhibited greater CIMT compared to those with higher intake. [84]. Similarly, serum zinc levels were associated with CIMT in patients undergoing hemodialysis (r = −0.70, p < 0.01) [85].
The pulse wave velocity (PWV) of the aorta is a key indicator of arterial wall stiffness and a predictor of CVD mortality and all-cause mortality in patients undergoing hemodialysis [86]. In non-diabetic hemodialysis patients, zinc levels were identified as independent predictors of brachial-ankle PWV (β = −9.85, p = 0.047) after adjustment for hypoalbuminemia and CRP levels [87].
The effect of zinc supplementation on vascular changes in humans has not been reported. However, in vivo studies have shown that zinc sulfate ameliorated vascular calcification in hyperphosphatemic kl/kl mice. This was demonstrated through aortic Alizarin Red staining, von Kossa staining of thoracic aorta sections, and quantification of calcium content in the aortic arch [54].
Since zinc deficiency is common in patients with CKD, the inhibitory effects of zinc on hydroxyapatite formation (i.e., prolongation of T50) and the suppression of calcification-related transcription factors may be impaired in patients with CKD. Findings from basic research on zinc in relation to VSMCs and T50, along with clinical studies on zinc and markers of vascular calcification and atherosclerosis, suggest that zinc could help suppress the progression of CKD, CVD events, and mortality by preventing phosphate-induced calcification (Figure 2). Further clinical trials are warranted to determine whether zinc supplementation can improve T50 and/or attenuate vascular calcification in patients with CKD and those undergoing hemodialysis.
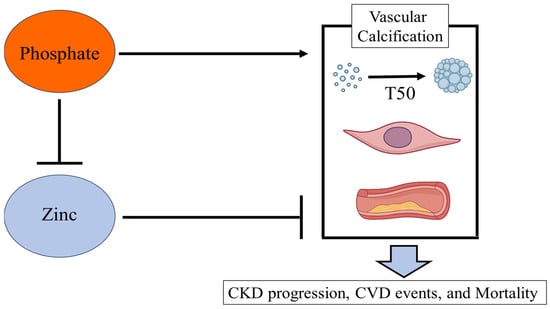
Figure 2.
Associations between zinc and phosphate in vascular calcification and clinical outcomes.
Phosphate promotes the transition from primary calciprotein CPPs to secondary CPPs, a process that plays a pivotal role in vascular calcification and contributes to the progression of CKD, CVD events, and mortality. Experimental studies have demonstrated that zinc suppresses phosphate-induced vascular calcification. Conversely, hyperphosphatemia and excessive dietary phosphate intake can impair intestinal zinc absorption, potentially leading to zinc deficiency. Abbreviations: CKD, chronic kidney disease; CPPs, calciprotein particles; CVD, cardiovascular disease.
3. Zinc and Blood Pressure
A meta-analysis revealed an association between serum zinc levels and increased blood pressure across various region including Africa, North America, Asia, and Europe [88]. In hypertension model rats, dietary zinc restriction exacerbated systolic blood pressure [89], whereas zinc supplementation attenuated blood pressure response [90]. Although the precise mechanisms by which zinc contributes to blood pressure control remain uncertain, it has been suggested that zinc may enhance the activity of nitric oxide synthase (NOS), leading to increased nitric oxide (NO) production and vasodilation [91]. It has been proposed that zinc may also enhance the activity of superoxide scavenger enzymes, thereby facilitating the removal of superoxide radicals [92,93]. Therefore, zinc deficiency may impair downstream actions of endothelial NO, leading to insufficient vasodilation. Additionally, zinc has recently been shown to play a regulatory role in renal sodium reabsorption in the distal nephron [94]. While approximately 70% of sodium is reabsorbed in the proximal tubules, fine-tuning of renal sodium handling occurs in the distal nephron. In C57BL/6 mice, zinc deficiency induced hypertension because of impaired renal sodium excretion [94]. Interestingly, under high-salt conditions, zinc deficiency may significantly affect urinary sodium reabsorption by altering renal tubular epithelial sodium transporters, thereby contributing to hypertension in C57BL/6 mice [95]. Future studies are needed to explore the potential of zinc supplementation as a strategy to prevent blood pressure elevation in patients with CKD and those undergoing hemodialysis.
4. Zinc and Anemia
Zinc deficiency may contribute to the development of anemia by increasing the fragility of erythrocyte membranes, decreasing iron availability and impairing erythropoiesis [96,97]. The fragility of erythrocyte membranes is thought to result from a reduction in sulfhydryl groups within membrane-bound Na+/K+-ATPase and Ca2+-ATPase enzymes, which weakens membrane integrity and renders red blood cells more susceptible to hemolysis [98]. The differentiation and proliferation of erythroblasts critically require the zinc finger transcription factor GATA-1. Zinc deficiency impairs GATA-1 function, thereby disrupting erythroid maturation and leading to anemia [99]. Several studies using animal models have also indicated that zinc deficiency impairs erythropoiesis, highlighting the essential role of zinc in this process [97,100,101]. Zinc supplementation has been shown to stimulate erythropoiesis in rats with phenylhydrazine-induced anemia and those with 5/6 nephrectomy-induced anemia, as well as to promote red blood cell formation in the bone marrow [102]. In patients undergoing hemodialysis, zinc deficiency has been associated with reduced responsiveness to erythropoiesis-stimulating agent (ESA) [103]. In addition, the mechanical stimulation of hemodialysis may cause the rupture of red blood cells leading to anemia in patients undergoing hemodialysis [96]. Supplementation with polaprezinc, a zinc-containing compound (zinc L-carnosine), at a dose of 34 mg of elemental zinc per day has been found to improve anemia and decrease ESA doses from 7125 ± 1196 IU/week to 5427 ± 2860 IU/week [104]. Additionally, administration of polaprezinc for 12 months has been shown to reduce both the ESA dosage and the erythropoietin responsiveness index, which is calculated as weekly ESA dose (units) divided by dry weight (kg) and hemoglobin level (g/dL), in patients undergoing hemodialysis. The ESA dosage decreased from approximately 110 to 80 U/kg/week, and the erythropoietin responsiveness index decreased from 11 to 8, respectively [21]. Further research is needed to evaluate whether zinc supplementation can improve responsiveness to ESA and alleviate renal anemia in patients with CKD.
Hypoxia-inducible factor stabilizers (HIF stabilizers), also known as HIF prolyl hydroxylase inhibitors (HIF-PHIs), are used to treat anemia in CKD by stimulating the production of endogenous erythropoietin and improving iron metabolism [105]. However, recent findings have highlighted that HIF-PHIs also play a pivotal role in vascular calcification in VSMCs [106,107]. Specifically, HIF-1α may accelerate calcium deposition by upregulating the expression of the master regulator of osteogenic differentiation [106]. FG4592, an orally bioavailable PHI, promotes phosphate uptake in VSMCs and phosphate-induced loss of smooth muscle cell markers (ACTA-2, MYH11, SM22a) and enhances osteochondrogenic gene expression (Msx-2, BMP-2, Sp7). Zinc inhibits FG4592-aggravated calcification caused by high phosphate by maintaining the VSMC phenotype, decreasing phosphate uptake, and lowering osteochondrogenic gene expression and levels of PDK4, as well as preserving Runx2 phosphorylation and cell variability [53]. Additionally, in mice with CKD fed an adenine and high-phosphate diet, treatment with a HIF-PHI was found to accelerate aortic calcification, as assessed using Osteosense dye [108]. To date, no studies have reported such effects of HIF-PHI treatment on vascular calcification in humans. However, caution is warranted when administering HIF-PHIs to patients with CKD, given the potential risk of promoting vascular calcification [109]. Notably, zinc inhibits FG4592-aggravated calcification caused by high phosphate by maintaining the VSMC phenotype, decreasing phosphate uptake, and lowering osteochondrogenic gene expression and levels of PDK4, as well as preserving Runx2 phosphorylation and cell variability [53].
Although it may be challenging to investigate whether HIF-PHIs promote vascular calcification and whether zinc supplementation could mitigate this effect in CKD patients with advanced vascular calcification, such clinical trials remain essential. They could provide valuable insights into developing novel strategies for managing renal anemia while accounting for vascular insights into developing novel strategies for managing renal anemia while accounting for vascular calcification risks.
5. Zinc and Other Diseases
5.1. Diabetes
Zinc deficiency constitutes a significant risk factor for diabetes, given its essential role as a cofactor in the synthesis, storage, and secretion of insulin by the pancreas [110]. Zinc deficiency may compromise pancreatic insulin synthesis and secretion, and diminish glucose uptake by peripheral tissues, thereby promoting the development of insulin resistance, a defining feature of diabetes mellitus [111]. A recent meta-analysis demonstrated that zinc supplementation significantly reduced fasting blood glucose, glycosylated hemoglobin (HbA1c), serum insulin, and insulin resistance as estimated by the homeostasis model assessment (HOMA-IR) [112].
Several experimental models have indicated that zinc supplementation upregulates metallothionein and nuclear factor erythroid 2–related factor 2 (Nrf2), which may represent key mechanisms linking zinc deficiency to renal function decline in diabetes [113,114]. Additionally, several short-term RCTs in patients with type 2 diabetes have shown that zinc supplementation can reduce urinary microalbumin levels [115,116,117]. However, its effect on kidney function remains controversial, possibly due to the preserved kidney function of participants and the relatively short duration of zinc supplementation in these previous RCTs. Further studies are needed to evaluate the reno-protective effects of zinc supplementation on massive proteinuria and kidney function in patients with advanced stages of CKD with diabetes.
5.2. Infection
Zinc deficiency has been reported to impair immunity [118], as it plays a crucial role in regulating the immune response, particularly T-cell–mediated functions [119]. There is substantial evidence linking zinc deficiency to several infectious disease, including malaria, HIV, tuberculosis, measles, and respiratory infections such as COVID-19 pneumonia [120]. Among elderly individuals in nursing homes, those with low serum zinc levels (<70 μg/dL) had a significantly higher incidence and longer duration of pneumoniae [20], as well as all-cause mortality during 1-year follow-up [121]. In patients with CKD stage 5, low serum zinc levels (<50 μg/dL) were associated with a higher risk of infection-related hospitalization [122]. Furthermore, in patients undergoing hemodialysis or peritoneal dialysis, each 1 mg/dL decrease in serum zinc level was associated with a 2.0% increased risk of hospitalization for infection [43].
Zinc supplementation at 30 mg/day for 3 months for nursing home elderly (aged ≥65 y) enhanced T cell function measured by increased anti-CD3/CD28 and phytohemagglutinin-stimulated T cell proliferation [123]. Moreover, zinc supplementation has been shown to reduce the risk of infection in the elderly [124]. A meta-analysis of six randomized controlled trials involving 2216 patients with severe pneumonia suggested that zinc supplementation as an adjunct to standard treatment is effective in reducing mortality associated with severe pneumonia [125]. Systematic reviews and meta-analyses of RCTs in patients undergoing hemodialysis have shown that approximately 45 mg of zinc for 2 months zinc supplementation significantly reduces CRP and malondialdehyde, while enhancing SOD activity [18,126]. These findings suggest that zinc supplementation may play a crucial role in increasing serum zinc levels, enhancing immune function, and preventing infectious diseases such as pneumonia in patients with CKD, including those undergoing hemodialysis.
5.3. Cardiac Diastolic Dysfunction
Diastolic dysfunction is associated with adverse outcomes including CVD mortality and major CVD events in patients undergoing hemodialysis [127]. In addition to traditional risk factors, such as older age, diabetes, and hypertension, zinc deficiency-related factors including oxidative stress, malnutrition, and inflammation have also been shown to contribute to impaired myocardial relaxation and ventricular stiffness [128,129]. In patients not requiring kidney replacement therapy, a recent meta-analysis of 27 case–control studies revealed that individuals with idiopathic dilated cardiomyopathy had significantly lower serum zinc levels, whereas no such association was observed in those with ischemic cardiomyopathy [130]. In patients undergoing hemodialysis, lower serum zinc levels were significantly associated with an increased left atrial volume index > 34 mL/m2 and E/e’ ratio > 15 [131]. Although the exact mechanism regarding zinc deficiency and diastolic dysfunction remain unclear, current findings suggest that zinc deficiency may play a contributory role in the development of diastolic dysfunction. Further studies are needed to determine whether zinc supplementation can mitigate cardiac dysfunction in patients undergoing hemodialysis.
6. Zinc and Progression of Kidney Disease
Serum zinc levels vary significantly across different stages of CKD, with a notable decrease observed in individuals with late-stage CKD [132]. In a cohort of 194 patients with CKD stages 1–4, more advanced CKD stages were independently associated with lower serum zinc levels, even after adjustment for age, sex, smoking status, educational attainment, diabetes, hypertension, and BMI (p for trend = 0.002) [133].
Previous observational study in patients with CKD investigating the relationship between zinc levels and kidney function have shown that individuals in the low-zinc group had a significantly increased risk of experiencing the primary outcome, which included progression to end-stage kidney disease or death, with a hazard ratio of 1.81 (95% confidence interval: 1.02–3.24) [134]. Additionally, low plasma zinc levels were correlated with a greater decline in kidney function (r = 0.185, p = 0.023) [4]. Recent basic research has examined whether zinc deficiency itself causes pathological changes [135]. In zinc-deficient rats, glomerulosclerosis and interstitial fibrosis along with increased urinary microalbumin and serum creatinine levels were observed. Zinc deficiency may trigger the activation of reactive oxygen species (ROS) and mitochondrial dysfunction, leading to glomerulosclerosis and interstitial fibrosis, respectively. Notably, zinc supplementation significantly ameliorated these pathological alterations [135]. Future clinical trials are needed to evaluate whether zinc supplementation can mitigate kidney function decline in patients with CKD.
IgA nephropathy and nephrotic syndrome are clinically significant causes of CKD. In IgA nephropathy-prone gddY mice, a high-zinc diet resulted in significantly lower mesangial IgA deposition, serum IgA levels, and urinary protein levels compared to a normal-zinc die [136]. Dietary zinc levels may influence the immune process of nephritogenic IgA production by modulating dendritic cell activity, particularly via the Toll-like receptor 4 pathway [136].
Although the precise mechanisms remain unclear, accumulating evidence has highlighted an association between serum zinc levels and the risk of relapse in children with steroid-sensitive nephrotic syndrome, as reported in a recent systematic review [137]. This review demonstrated a significant relationship between reduced serum zinc levels and disease severity. Moreover, zinc supplementation was suggested to support sustained remission and reduce relapse rates [137]. Given the potential efficacy of zinc supplementation in achieving remission in patients with IgA nephropathy and nephrotic syndrome, further clinical studies are warranted.
7. Zinc and CVD Events
Epidemiological studies examining the relationship between zinc levels and the risk of CVD events were summarized in a previous review [138], which demonstrated that low serum zinc levels are associated with an increased risk of CVD events. Another systematic review of prospective cohort studies investigating the association between zinc status and CVD events found that higher serum zinc levels were associated with a lower risk of CVD events [139], particularly in patients referred for coronary angiography [140] and patients with type 2 diabetes mellitus [141]. Evidence regarding this topic in patients with CKD is very limited. In a study of 170 CKD patients followed for 40 months, during which 59 CVD events occurred, a Kaplan–Meier analysis with a log-rank test revealed that patients in the lower zinc level group had a higher risk of CVD occurrence. Furthermore, univariate Cox hazard regression analyses demonstrated that zinc levels were significantly associated with a reduced risk of CVD events (hazard ratio of 0.97 (95% confidence interval: 0.04–0.99)). However, this association was no longer significant in multivariate Cox regression analyses [79]. Regarding hemodialysis patients, a longitudinal study involving 42 incident hemodialysis patients followed for 2.5 years, during which 20 CVD events occurred, found no significant association between lower zinc levels and an increased risk of CVD [5]. The relatively small sample size of this study represents a key limitation. Of interest, the association between serum concentrations of other trace elements, such as magnesium and selenium, and CVD events in patients undergoing hemodialysis has also not been clearly established. Further research involving larger cohorts is needed to more clearly elucidate the relationship between trace element levels, including serum zinc, and CVD in patients with CKD and those undergoing hemodialysis.
8. Zinc and Mortality in Patients with Hemodialysis
To date, no studies have reported a possible association between serum zinc levels and mortality in patients with pre-dialysis CKD. In contrast, the association between serum zinc levels and mortality in patients undergoing hemodialysis remains controversial (Table 2). A study using a backward stepwise Cox analysis identified older age, hypoalbuminemia, and zinc deficiency as independent predictors of mortality in a cohort of 111 patients on maintenance dialysis, including both hemodialysis and peritoneal dialysis [43]. In patients with incident hemodialysis (n = 142), the association between serum zinc levels and all-cause mortality was not significant after adjustment for potential confounders including serum albumin and CRP [5]. Prevalent patients on maintenance hemodialysis (n = 61) showed no significant association of serum zinc with mortality [142]. The sample sizes of the three studies were relatively small, with the number of deaths ranging from 11 to 15, which limited the ability to perform sufficient statistical adjustments and draw solid conclusions. In a larger study involving incident hemodialysis patients (n = 1278), multivariable-adjusted analysis using a forward stepwise approach by which covariates were selected from many potential confounders including serum albumin showed that lower zinc levels were not associated with an increased risk of death [49]. The inconsistencies in the findings of previous studies may be attributable, at least in part, to the influence of confounding factors such as serum albumin and CRP. Notably, approximately 60–80% of circulating zinc is bound to albumin in the serum [143], highlighting the importance of accounting for this factor in statistical analyses.
Table 2.
Summary of observational studies regarding the association between serum zinc levels or zinc intake and mortality in patients with hemodialysis.
Recently, we have investigated the potential association between serum zinc levels and all-cause mortality in a prospective cohort of 1662 prevalent patients undergoing maintenance hemodialysis [144]. Although the serum zinc level was a significant predictor of mortality in a model adjusted for 17 covariates excluding serum albumin, it was not an independent predictor of mortality when the serum albumin level was included. To address serum albumin as a stratification variable rather than a confounder, the cohort was stratified into two groups based on the median serum albumin level (3.7 g/dL). Among patients with lower serum albumin levels, the risk of death was significantly higher in those with lower zinc levels (≤68 µg/dL) compared to their higher zinc counterparts. In contrast, no significant difference in mortality risk was observed between zinc levels among patients with higher serum albumin levels [144]. Our findings indicate that a lower serum zinc level could be a significant factor associated with a higher risk of mortality in patients on maintenance hemodialysis, particularly in those with low serum albumin levels.
Regarding zinc intake, a prospective cohort study of 582 patients undergoing hemodialysis demonstrated a higher mortality risk in those with zinc intake below the recommended values (8 mg per day for women and 10 mg per day for men), even after adjusting for age, diabetes status, gender, dialysis vintage, albumin levels, lean tissue index, energy intake per kilogram, and physical activity levels [145]. RCTs are needed to determine whether zinc supplementation or increased dietary intake could reduce mortality in patients undergoing hemodialysis, particularly those with lower serum albumin levels.
9. Clinical Consideration in Zinc Supplementation
Based on the previously presented RCTs, zinc supplementation exceeding 45 mg/day may be necessary to increase serum zinc levels in patients undergoing hemodialysis [8]. However, careful consideration is required for zinc supplementation, as it may impair intestinal copper absorption, potentially leading to copper deficiency and pancytopenia [103]. A previous RCT comparing zinc acetate hydrate (containing 50 mg of zinc) with polaprezinc (containing 34 mg of zinc) showed that serum zinc levels were significantly increased in hemodialysis patients treated with zinc acetate hydrate. However, serum copper levels were significantly lower in the zinc acetate hydrate group compared to the polaprezinc group [16]. These findings suggest that monitoring serum zinc and copper levels is essential during zinc supplementation therapy to avoid trace element imbalances and pancytopenia.
10. Future Clinical Trials
To date, several important questions regarding zinc intervention in patients with CKD and those undergoing hemodialysis remain unanswered: (1) the serum zinc levels at which intervention should be initiated; (2) the optimal method of zinc administration (e.g., dietary modification, supplementation, oral formulations, or incorporation into dialysis solutions) and the appropriate duration of treatment; (3) the specific clinical outcomes expected to improve with zinc intervention (e.g., anemia, hypertension, infections, CKD progression, cardiovascular events, or mortality); and (4) the cost-effectiveness of zinc intervention strategies. Although current studies provide evidence to support the role of zinc in mitigating various complications related to CKD, robust clinical trial data remains limited. Most existing RCTs have focused on surrogate endpoints such as serum zinc levels, oxidative stress, and nutritional status, rather than hard clinical outcomes such as CKD progression, CVD events, or mortality. Consequently, the therapeutic potential of zinc supplementation in improving long-term outcomes in patients with CKD, including those undergoing hemodialysis, remains to be conclusively established. Large-scale, well-designed observational studies using target trial emulation or RCTs are needed to determine the clinical efficacy, optimal dosage, safety, and long-term benefits of zinc supplementation in this population.
11. Conclusions
Zinc deficiency is common in patients with CKD, including those undergoing hemodialysis. In addition to classical manifestations of zinc deficiency, emerging evidence highlights vascular calcification, hypertension, and renal anemia as newly recognized features of zinc deficiency. These emerging manifestations have been identified as the risk factors for CKD progression, CVD events, and mortality. Experimental studies have demonstrated the antagonistic effects of zinc on hypertension, renal anemia, infections, and phosphate-induced vascular calcification.
The important limitation of this review is the marked heterogeneity among the included studies. The reviewed evidence encompasses a wide range of study designs, zinc formulations, dosages, treatment durations, and patient populations, including different stages of CKD and dialysis modalities (hemodialysis, peritoneal dialysis). These variations pose significant challenges in synthesizing the findings into unified conclusions and may limit both the generalizability and clinical applicability of the results. Nonetheless, this review provides a meaningful overview of the current state of evidence, which may serve as a critical foundation for future RCTs aimed at establishing robust clinical evidence for zinc supplementation in patients with CKD and those undergoing hemodialysis.
Author Contributions
Wrote the manuscript: S.N.; critically reviewed and corrected all versions of the manuscript: T.M., F.M., K.M. and M.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
ChatGPT was used in part for the creation of the abbreviation table and figures. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Abbreviations
The following abbreviations are used in this manuscript:
| AAC | Abdominal aortic calcification |
| ALP | Alkaline Phosphatase |
| BMI | Body mass index |
| BMSCs | Bone Marrow-Derived Mesenchymal Stem Cells |
| CIMT | Carotid intima-media thickness |
| CKD | Chronic kidney disease |
| eGFR | Estimated glomerular filtration rate |
| CPP | Calciprotein particle |
| CRP | C-reactive protein |
| CVD | Cardiovascular disease |
| ESA | Erythropoiesis-stimulating agent |
| HbA1c | Glycosylated hemoglobin |
| HIF | Hypoxia-inducible factor |
| HIF-PHIs | Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitors |
| HOMAIR | Homeostasis model assessment-estimated insulin resistance |
| Nrf2 | Nuclear Factor Erythroid 2–Related Factor 2 |
| NF-κB | nuclear factor kappa light chain enhancer of activated B |
| NO | Nitric Oxide |
| NOS | Nitric Oxide Synthase |
| OCN | Osteocalcin |
| PWV | Pulse wave velocity |
| RCT | Randomized controlled trial |
| RUNX2 | Runt-Related Transcription Factor 2 |
| SOD | Superoxide Dismutase |
| SOX9 | SRY-Box Transcription Factor 9 |
| T50 | Serum calcification propensity |
| TNF | Tumor necrosis factor |
| TNFAIP3 | TNFα-induced protein 3 |
| VSMC | vasculature smooth muscle cell |
References
- King, J.C.; Shames, D.M.; Woodhouse, L.R. Zinc homeostasis in humans. J. Nutr. 2000, 130, 1360S–1366S. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.S. Discovery of human zinc deficiency: 50 years later. J. Trace Elem. Med. Biol. 2012, 26, 66–69. [Google Scholar] [CrossRef]
- Mahajan, S.K.; Bowersox, E.M.; Rye, D.L.; Abu-Hamdan, D.K.; Prasad, A.S.; McDonald, F.D.; Biersack, K.L. Factors underlying abnormal zinc metabolism in uremia. Kidney Int. Suppl. 1989, 27, S269–S273. [Google Scholar] [PubMed]
- Damianaki, K.; Lourenco, J.M.; Braconnier, P.; Ghobril, J.P.; Devuyst, O.; Burnier, M.; Lenglet, S.; Augsburger, M.; Thomas, A.; Pruijm, M. Renal handling of zinc in chronic kidney disease patients and the role of circulating zinc levels in renal function decline. Nephrol. Dial. Transpl. 2020, 35, 1163–1170. [Google Scholar] [CrossRef]
- Toida, T.; Toida, R.; Ebihara, S.; Takahashi, R.; Komatsu, H.; Uezono, S.; Sato, Y.; Fujimoto, S. Association between Serum Zinc Levels and Clinical Index or the Body Composition in Incident Hemodialysis Patients. Nutrients 2020, 12, 3187. [Google Scholar] [CrossRef] [PubMed]
- Okumura, Y.; Abe, K.; Sakai, S.; Kamei, Y.; Mori, Y.; Adachi, Y.; Takikawa, M.; Kitamura, A.; Ohminami, H.; Ohnishi, K.; et al. Elevated luminal inorganic phosphate suppresses intestinal Zn absorption in 5/6 nephrectomized rats. Am. J. Physiol. Ren. Physiol. 2024, 326, F411–F419. [Google Scholar] [CrossRef]
- Kodama, H.; Tanaka, M.; Naito, Y.; Katayama, K.; Moriyama, M. Japan’s Practical Guidelines for Zinc Deficiency with a Particular Focus on Taste Disorders, Inflammatory Bowel Disease, and Liver Cirrhosis. Int. J. Mol. Sci. 2020, 21, 2941. [Google Scholar] [CrossRef]
- Nakatani, S.; Mori, K.; Shoji, T.; Emoto, M. Association of Zinc Deficiency with Development of CVD Events in Patients with CKD. Nutrients 2021, 13, 1680. [Google Scholar] [CrossRef]
- Elgenidy, A.; Amin, M.A.; Awad, A.K.; Husain-Syed, F.; Aly, M.G. Serum Zinc Levels in Chronic Kidney Disease Patients, Hemodialysis Patients, and Healthy Controls: Systematic Review and Meta-Analysis. J. Ren. Nutr. 2023, 33, 103–115. [Google Scholar] [CrossRef]
- Gibson, R.S.; King, J.C.; Lowe, N. A Review of Dietary Zinc Recommendations. Food Nutr. Bull. 2016, 37, 443–460. [Google Scholar] [CrossRef]
- Inoue, Y. Dietary reference intakes of trace elements for Japanese and problems in clinical fields. Nihon Rinsho. Jpn. J. Clin. Med. 2016, 74, 1066–1073. [Google Scholar]
- Chen, W.; Eisenberg, R.; Mowrey, W.B.; Wylie-Rosett, J.; Abramowitz, M.K.; Bushinsky, D.A.; Melamed, M.L. Association between dietary zinc intake and abdominal aortic calcification in US adults. Nephrol. Dial. Transpl. 2020, 35, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.L.; et al. ESPEN micronutrient guideline. Clin. Nutr. 2022, 41, 1357–1424. [Google Scholar] [CrossRef]
- Hosseini, R.; Montazerifar, F.; Shahraki, E.; Karajibani, M.; Mokhtari, A.M.; Dashipour, A.R.; Ferns, G.A.; Jalali, M. The Effects of Zinc Sulfate Supplementation on Serum Copeptin, C-Reactive Protein and Metabolic Markers in Zinc-Deficient Diabetic Patients on Hemodialysis: A Randomized, Double-Blind, Placebo-Controlled Trial. Biol. Trace Elem. Res. 2022, 200, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Haddadian-Khouzani, S.; Shahidi, S.; Askari, G.; Clark, C.C.T.; Rouhani, M.H. The efficacy and safety of zinc gluconate supplementation on quality of life, sleep quality, and serum albumin in hemodialysis patients: A randomized clinical trial. Eur. J. Integr. Med. 2022, 55, 102183. [Google Scholar] [CrossRef]
- Okamoto, T.; Hatakeyama, S.; Konishi, S.; Okita, K.; Tanaka, Y.; Imanishi, K.; Takashima, T.; Saitoh, F.; Suzuki, T.; Ohyama, C. Comparison of zinc acetate hydrate and polaprezinc for zinc deficiency in patients on maintenance hemodialysis: A single-center, open-label, prospective randomized study. Ther. Apher. Dial. 2020, 24, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Escobedo-Monge, M.F.; Ayala-Macedo, G.; Sakihara, G.; Peralta, S.; Almaraz-Gomez, A.; Barrado, E.; Marugan-Miguelsanz, J.M. Effects of Zinc Supplementation on Nutritional Status in Children with Chronic Kidney Disease: A Randomized Trial. Nutrients 2019, 11, 2671. [Google Scholar] [CrossRef]
- Wang, L.J.; Wang, M.Q.; Hu, R.; Yang, Y.; Huang, Y.S.; Xian, S.X.; Lu, L. Effect of Zinc Supplementation on Maintenance Hemodialysis Patients: A Systematic Review and Meta-Analysis of 15 Randomized Controlled Trials. Biomed. Res. Int. 2017, 2017, 1024769. [Google Scholar] [CrossRef]
- Tonelli, M.; Wiebe, N.; Thompson, S.; Kinniburgh, D.; Klarenbach, S.W.; Walsh, M.; Bello, A.K.; Faruque, L.; Field, C.; Manns, B.J.; et al. Trace element supplementation in hemodialysis patients: A randomized controlled trial. BMC Nephrol. 2015, 16, 52. [Google Scholar] [CrossRef]
- Abdollahi, S.; Toupchian, O.; Jayedi, A.; Meyre, D.; Tam, V.; Soltani, S. Zinc Supplementation and Body Weight: A Systematic Review and Dose-Response Meta-analysis of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 398–411. [Google Scholar] [CrossRef]
- Kobayashi, H.; Abe, M.; Okada, K.; Tei, R.; Maruyama, N.; Kikuchi, F.; Higuchi, T.; Soma, M. Oral zinc supplementation reduces the erythropoietin responsiveness index in patients on hemodialysis. Nutrients 2015, 7, 3783–3795. [Google Scholar] [CrossRef]
- El-Shazly, A.N.; Ibrahim, S.A.; El-Mashad, G.M.; Sabry, J.H.; Sherbini, N.S. Effect of zinc supplementation on body mass index and serum levels of zinc and leptin in pediatric hemodialysis patients. Int. J. Nephrol. Renov. Dis. 2015, 8, 159–163. [Google Scholar] [CrossRef]
- Argani, H.; Mahdavi, R.; Ghorbani-haghjo, A.; Razzaghi, R.; Nikniaz, L.; Gaemmaghami, S.J. Effects of zinc supplementation on serum zinc and leptin levels, BMI, and body composition in hemodialysis patients. J. Trace Elem. Med. Biol. 2014, 28, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Pakfetrat, M.; Shahroodi, J.R.; Zolgadr, A.A.; Larie, H.A.; Nikoo, M.H.; Malekmakan, L. Effects of zinc supplement on plasma homocysteine level in end-stage renal disease patients: A double-blind randomized clinical trial. Biol. Trace Elem. Res. 2013, 153, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Mazani, M.; Argani, H.; Rashtchizadeh, N.; Ghorbanihaghjo, A.; Hamdi, A.; Estiar, M.A.; Nezami, N. Effects of zinc supplementation on antioxidant status and lipid peroxidation in hemodialysis patients. J. Ren. Nutr. 2013, 23, 180–184. [Google Scholar] [CrossRef]
- Guo, C.H.; Wang, C.L. Effects of zinc supplementation on plasma copper/zinc ratios, oxidative stress, and immunological status in hemodialysis patients. Int. J. Med. Sci. 2013, 10, 79–89. [Google Scholar] [CrossRef]
- Rahimi-Ardabili, B.; Argani, H.; Ghorbanihaghjo, A.; Rashtchizadeh, N.; Naghavi-Behzad, M.; Ghorashi, S.; Nezami, N. Paraoxonase enzyme activity is enhanced by zinc supplementation in hemodialysis patients. Ren. Fail. 2012, 34, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Roozbeh, J.; Hedayati, P.; Sagheb, M.M.; Sharifian, M.; Hamidian Jahromi, A.; Shaabani, S.; Jalaeian, H.; Raeisjalali, G.A.; Behzadi, S. Effect of zinc supplementation on triglyceride, cholesterol, LDL, and HDL levels in zinc-deficient hemodialysis patients. Ren. Fail. 2009, 31, 798–801. [Google Scholar] [CrossRef]
- Rashidi, A.A.; Salehi, M.; Piroozmand, A.; Sagheb, M.M. Effects of zinc supplementation on serum zinc and C-reactive protein concentrations in hemodialysis patients. J. Ren. Nutr. 2009, 19, 475–478. [Google Scholar] [CrossRef]
- Nava, H.J.; Amato, D. Effect of zinc supplements on the levels of pre-albumin and transferrin in patients with dialysis. Rev. Investig. Clínica 2005, 57, 123–125. [Google Scholar]
- Matson, A.; Wright, M.; Oliver, A.; Woodrow, G.; King, N.; Dye, L.; Blundell, J.; Brownjohn, A.; Turney, J. Zinc supplementation at conventional doses does not improve the disturbance of taste perception in hemodialysis patients. J. Ren. Nutr. 2003, 13, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, C.A.; Liepa, G.; Murphy, M.D.; Suneson, J.; Vanbeber, A.D.; Gorman, M.A.; Cochran, C. The effects of zinc supplementation on serum zinc and cholesterol concentrations in hemodialysis patients. J. Ren. Nutr. 2002, 12, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Candan, F.; Gultekin, F.; Candan, F. Effect of vitamin C and zinc on osmotic fragility and lipid peroxidation in zinc-deficient haemodialysis patients. Cell Biochem. Funct. 2002, 20, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Jern, N.A.; VanBeber, A.D.; Gorman, M.A.; Weber, C.G.; Liepa, G.U.; Cochran, C.C. The effects of zinc supplementation on serum zinc concentration and protein catabolic rate in hemodialysis patients. J. Ren. Nutr. 2000, 10, 148–153. [Google Scholar] [CrossRef]
- Brodersen, H.P.; Holtkamp, W.; Larbig, D.; Beckers, B.; Thiery, J.; Lautenschlager, J.; Probst, H.J.; Ropertz, S.; Yavari, A. Zinc supplementation and hepatitis B vaccination in chronic haemodialysis patients: A multicentre study. Nephrol. Dial. Transpl. 1995, 10, 1780. [Google Scholar]
- Prasad, A.S. Zinc: Role in immunity, oxidative stress and chronic inflammation. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 646–652. [Google Scholar] [CrossRef]
- MacDonald, R.S. The role of zinc in growth and cell proliferation. J. Nutr. 2000, 130, 1500S–1508S. [Google Scholar] [CrossRef]
- Andreini, C.; Banci, L.; Bertini, I.; Rosato, A. Counting the zinc-proteins encoded in the human genome. J. Proteome Res. 2006, 5, 196–201. [Google Scholar] [CrossRef]
- Henkin, R.I. Zinc in taste function: A critical review. Biol. Trace Elem. Res. 1984, 6, 263–280. [Google Scholar] [CrossRef]
- Lask, B.; Fosson, A.; Rolfe, U.; Thomas, S. Zinc deficiency and childhood-onset anorexia nervosa. J. Clin. Psychiatry 1993, 54, 63–66. [Google Scholar]
- Gray, N.A.; Dhana, A.; Stein, D.J.; Khumalo, N.P. Zinc and atopic dermatitis: A systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.S. Clinical manifestations of zinc deficiency. Annu. Rev. Nutr. 1985, 5, 341–363. [Google Scholar] [CrossRef]
- Yang, C.Y.; Wu, M.L.; Chou, Y.Y.; Li, S.Y.; Deng, J.F.; Yang, W.C.; Ng, Y.Y. Essential trace element status and clinical outcomes in long-term dialysis patients: A two-year prospective observational cohort study. Clin. Nutr. 2012, 31, 630–636. [Google Scholar] [CrossRef]
- Cardozo, L.; Mafra, D. Don’t forget the zinc. Nephrol. Dial. Transpl. 2020, 35, 1094–1098. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Nagler, E.V.; Verbeke, F.; Van Biesen, W.; Vanholder, R. Hypomagnesemia and the risk of death and GFR decline in chronic kidney disease. Am. J. Med. 2013, 126, 825–831. [Google Scholar] [CrossRef]
- Wu, C.Y.; Wong, C.S.; Chung, C.J.; Wu, M.Y.; Huang, Y.L.; Ao, P.L.; Lin, Y.F.; Lin, Y.C.; Shiue, H.S.; Su, C.T.; et al. The association between plasma selenium and chronic kidney disease related to lead, cadmium and arsenic exposure in a Taiwanese population. J. Hazard. Mater. 2019, 375, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.Z.; Huang, Y.; Zheng, X.F.; Feng, R.; Li, X.Y.; Zheng, Z.G.; Jiang, B.J.; Du, S.; Chen, H.G.; Xu, Y. The association between serum magnesium and chronic kidney disease in Chinese adults: A cross-sectional study. BMC Public Health 2024, 24, 187. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Fujii, N.; Shoji, T.; Hayashi, T.; Rakugi, H.; Isaka, Y. Hypomagnesemia is a significant predictor of cardiovascular and non-cardiovascular mortality in patients undergoing hemodialysis. Kidney Int. 2014, 85, 174–181. [Google Scholar] [CrossRef]
- Tonelli, M.; Wiebe, N.; Bello, A.; Field, C.J.; Gill, J.S.; Hemmelgarn, B.R.; Holmes, D.T.; Jindal, K.; Klarenbach, S.W.; Manns, B.J.; et al. Concentrations of Trace Elements and Clinical Outcomes in Hemodialysis Patients: A Prospective Cohort Study. Clin. J. Am. Soc. Nephrol. 2018, 13, 907–915. [Google Scholar] [CrossRef]
- Jono, S.; McKee, M.D.; Murry, C.E.; Shioi, A.; Nishizawa, Y.; Mori, K.; Morii, H.; Giachelli, C.M. Phosphate regulation of vascular smooth muscle cell calcification. Circ. Res. 2000, 87, E10–E17. [Google Scholar] [CrossRef]
- Kircelli, F.; Peter, M.E.; Sevinc Ok, E.; Celenk, F.G.; Yilmaz, M.; Steppan, S.; Asci, G.; Ok, E.; Passlick-Deetjen, J. Magnesium reduces calcification in bovine vascular smooth muscle cells in a dose-dependent manner. Nephrol. Dial. Transpl. 2012, 27, 514–521. [Google Scholar] [CrossRef]
- Louvet, L.; Buchel, J.; Steppan, S.; Passlick-Deetjen, J.; Massy, Z.A. Magnesium prevents phosphate-induced calcification in human aortic vascular smooth muscle cells. Nephrol. Dial. Transpl. 2013, 28, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Nagy, A.; Petho, D.; Gall, T.; Zavaczki, E.; Nyitrai, M.; Posta, J.; Zarjou, A.; Agarwal, A.; Balla, G.; Balla, J. Zinc Inhibits HIF-Prolyl Hydroxylase Inhibitor-Aggravated VSMC Calcification Induced by High Phosphate. Front. Physiol. 2019, 10, 1584. [Google Scholar] [CrossRef]
- Voelkl, J.; Tuffaha, R.; Luong, T.T.D.; Zickler, D.; Masyout, J.; Feger, M.; Verheyen, N.; Blaschke, F.; Kuro, O.M.; Tomaschitz, A.; et al. Zinc Inhibits Phosphate-Induced Vascular Calcification through TNFAIP3-Mediated Suppression of NF-κB. J. Am. Soc. Nephrol. 2018, 29, 1636–1648. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Gordillo-Martinez, F.; Jiang, L.; He, P.; Hong, W.; Wei, X.; Staines, K.A.; Macrae, V.E.; Zhang, C.; Yu, D.; et al. Zinc ameliorates human aortic valve calcification through GPR39 mediated ERK1/2 signalling pathway. Cardiovasc. Res. 2021, 117, 820–835. [Google Scholar] [CrossRef]
- Henze, L.A.; Estepa, M.; Pieske, B.; Lang, F.; Eckardt, K.U.; Alesutan, I.; Voelkl, J. Zinc Ameliorates the Osteogenic Effects of High Glucose in Vascular Smooth Muscle Cells. Cells 2021, 10, 3083. [Google Scholar] [CrossRef]
- Alcantara, E.H.; Kwon, J.H.; Kang, M.K.; Cho, Y.E.; Kwun, I.S. Zinc Deficiency Promotes Calcification in Vascular Smooth Muscle Cells Independent of Alkaline Phosphatase Action and Partly Impacted by Pit1 Upregulation. Nutrients 2024, 16, 291. [Google Scholar] [CrossRef] [PubMed]
- Balogh, E.; Toth, A.; Csiki, D.M.; Jeney, V. Zinc Ameliorates High Pi and Ca-Mediated Osteogenic Differentiation of Mesenchymal Stem Cells. Nutrients 2024, 16, 4012. [Google Scholar] [CrossRef]
- Heiss, A.; Jahnen-Dechent, W.; Endo, H.; Schwahn, D. Structural dynamics of a colloidal protein-mineral complex bestowing on calcium phosphate a high solubility in biological fluids. Biointerphases 2007, 2, 16–20. [Google Scholar] [CrossRef]
- Heiss, A.; DuChesne, A.; Denecke, B.; Grotzinger, J.; Yamamoto, K.; Renne, T.; Jahnen-Dechent, W. Structural basis of calcification inhibition by α2-HS glycoprotein/fetuin-A. Formation of colloidal calciprotein particles. J. Biol. Chem. 2003, 278, 13333–13341. [Google Scholar] [CrossRef]
- Jahnen-Dechent, W.; Smith, E.R. Nature’s remedy to phosphate woes: Calciprotein particles regulate systemic mineral metabolism. Kidney Int. 2020, 97, 648–651. [Google Scholar] [CrossRef]
- Jahnen-Dechent, W.; Pasch, A. Solving the insoluble: Calciprotein particles mediate bulk mineral transport. Kidney Int. 2023, 103, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Kuro, O.M. Phosphate as a Pathogen of Arteriosclerosis and Aging. J. Atheroscler. Thromb. 2021, 28, 203–213. [Google Scholar] [CrossRef]
- Aghagolzadeh, P.; Bachtler, M.; Bijarnia, R.; Jackson, C.; Smith, E.R.; Odermatt, A.; Radpour, R.; Pasch, A. Calcification of vascular smooth muscle cells is induced by secondary calciprotein particles and enhanced by tumor necrosis factor-alpha. Atherosclerosis 2016, 251, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Pasch, A.; Farese, S.; Graber, S.; Wald, J.; Richtering, W.; Floege, J.; Jahnen-Dechent, W. Nanoparticle-based test measures overall propensity for calcification in serum. J. Am. Soc. Nephrol. 2012, 23, 1744–1752. [Google Scholar] [CrossRef] [PubMed]
- Pluquet, M.; Kamel, S.; Choukroun, G.; Liabeuf, S.; Laville, S.M. Serum Calcification Propensity Represents a Good Biomarker of Vascular Calcification: A Systematic Review. Toxins 2022, 14, 637. [Google Scholar] [CrossRef]
- Bundy, J.D.; Cai, X.; Mehta, R.C.; Scialla, J.J.; de Boer, I.H.; Hsu, C.Y.; Go, A.S.; Dobre, M.A.; Chen, J.; Rao, P.S.; et al. Serum Calcification Propensity and Clinical Events in CKD. Clin. J. Am. Soc. Nephrol. 2019, 14, 1562–1571. [Google Scholar] [CrossRef]
- Mori, K.; Shoji, T.; Nakatani, S.; Uedono, H.; Ochi, A.; Yoshida, H.; Imanishi, Y.; Morioka, T.; Tsujimoto, Y.; Kuro, O.M.; et al. Differential associations of fetuin-A and calcification propensity with cardiovascular events and subsequent mortality in patients undergoing hemodialysis. Clin. Kidney J. 2024, 17, sfae042. [Google Scholar] [CrossRef]
- Pasch, A.; Block, G.A.; Bachtler, M.; Smith, E.R.; Jahnen-Dechent, W.; Arampatzis, S.; Chertow, G.M.; Parfrey, P.; Ma, X.; Floege, J. Blood Calcification Propensity, Cardiovascular Events, and Survival in Patients Receiving Hemodialysis in the EVOLVE Trial. Clin. J. Am. Soc. Nephrol. 2017, 12, 315–322. [Google Scholar] [CrossRef]
- Lorenz, G.; Steubl, D.; Kemmner, S.; Pasch, A.; Koch-Sembdner, W.; Pham, D.; Haller, B.; Bachmann, Q.; Mayer, C.C.; Wassertheurer, S.; et al. Worsening calcification propensity precedes all-cause and cardiovascular mortality in haemodialyzed patients. Sci. Rep. 2017, 7, 13368. [Google Scholar] [CrossRef]
- Smith, E.R.; Ford, M.L.; Tomlinson, L.A.; Bodenham, E.; McMahon, L.P.; Farese, S.; Rajkumar, C.; Holt, S.G.; Pasch, A. Serum calcification propensity predicts all-cause mortality in predialysis CKD. J. Am. Soc. Nephrol. 2014, 25, 339–348. [Google Scholar] [CrossRef]
- Nakatani, S.; Mori, K.; Sonoda, M.; Nishide, K.; Uedono, H.; Tsuda, A.; Emoto, M.; Shoji, T. Association between Serum Zinc and Calcification Propensity (T50) in Patients with Type 2 Diabetes Mellitus and In Vitro Effect of Exogenous Zinc on T50. Biomedicines 2020, 8, 337. [Google Scholar] [CrossRef] [PubMed]
- Sohail, A.; Obereigner, J.; Mitter, G.; Schmid, T.; Hofer, A.S.; Schuster, G.; Hugl, A.; Dorninger, A.H.; Mandl, M.; Pasch, A.; et al. Association of serum zinc with mineral stress in chronic kidney disease. Clin. Kidney J. 2024, 17, sfae258. [Google Scholar] [CrossRef]
- Schweikle, M.; Bjornoy, S.H.; van Helvoort, A.T.J.; Haugen, H.J.; Sikorski, P.; Tiainen, H. Stabilisation of amorphous calcium phosphate in polyethylene glycol hydrogels. Acta Biomater. 2019, 90, 132–145. [Google Scholar] [CrossRef] [PubMed]
- Gross, K.A.; Komarovska, L.; Viksna, A. Efficient zinc incorporation into hydroxyapatite through crystallization of an amorphous phase could extend the properties of zinc apatites. J. Aust. Ceram. Soc. 2013, 49, 129–135. [Google Scholar]
- Candidato, R.T., Jr.; Thouzellier, C.; Pawlowski, L. Evaluation of the in-vitro behavior of nanostructured hydroxyapatite and zinc doped hydroxyapatite coatings obtained using solution precursor plasma spraying. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 106, 2101–2108. [Google Scholar] [CrossRef]
- Kestenbaum, B.R.; Adeney, K.L.; de Boer, I.H.; Ix, J.H.; Shlipak, M.G.; Siscovick, D.S. Incidence and progression of coronary calcification in chronic kidney disease: The Multi-Ethnic Study of Atherosclerosis. Kidney Int. 2009, 76, 991–998. [Google Scholar] [CrossRef]
- Chen, J.; Budoff, M.J.; Reilly, M.P.; Yang, W.; Rosas, S.E.; Rahman, M.; Zhang, X.; Roy, J.A.; Lustigova, E.; Nessel, L.; et al. Coronary Artery Calcification and Risk of Cardiovascular Disease and Death Among Patients With Chronic Kidney Disease. JAMA Cardiol. 2017, 2, 635–643. [Google Scholar] [CrossRef]
- Zhang, D.; Zhu, Y.; Li, H.; Wang, Y.; Niu, Z.; Zhou, W.; Wang, D. Associations of Whole Blood Zinc Levels with Coronary Artery Calcification and Future Cardiovascular Events in CKD Patients. Biol. Trace Elem. Res. 2024, 202, 46–55. [Google Scholar] [CrossRef]
- Wilson, P.W.; Kauppila, L.I.; O’Donnell, C.J.; Kiel, D.P.; Hannan, M.; Polak, J.M.; Cupples, L.A. Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation 2001, 103, 1529–1534. [Google Scholar] [CrossRef]
- Peeters, M.J.; van den Brand, J.A.; van Zuilen, A.D.; Koster, Y.; Bots, M.L.; Vervloet, M.G.; Blankestijn, P.J.; Wetzels, J.F.; the MASTERPLAN Study Group. Abdominal aortic calcification in patients with CKD. J. Nephrol. 2017, 30, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Sayed, O.; Ahmed, S.; Ismail, H.; Elfeshawy, M.; Ibrahim, M. Zinc and Abdominal Aortic Calcification in Patients under Regular Hemodialysis. Al-Azhar Int. Med. J. 2022, 3, 205–211. [Google Scholar] [CrossRef]
- Yang, C.W.; Guo, Y.C.; Li, C.I.; Liu, C.S.; Lin, C.H.; Liu, C.H.; Wang, M.C.; Yang, S.Y.; Li, T.C.; Lin, C.C. Subclinical Atherosclerosis Markers of Carotid Intima-Media Thickness, Carotid Plaques, Carotid Stenosis, and Mortality in Community-Dwelling Adults. Int. J. Env. Res. Public Health 2020, 17, 4745. [Google Scholar] [CrossRef]
- Yang, Y.J.; Choi, B.Y.; Chun, B.Y.; Kweon, S.S.; Lee, Y.H.; Park, P.S.; Kim, M.K. Dietary zinc intake is inversely related to subclinical atherosclerosis measured by carotid intima-media thickness. Br. J. Nutr. 2010, 104, 1202–1211. [Google Scholar] [CrossRef]
- Ari, E.; Kaya, Y.; Demir, H.; Asicioglu, E.; Keskin, S. The correlation of serum trace elements and heavy metals with carotid artery atherosclerosis in maintenance hemodialysis patients. Biol. Trace Elem. Res. 2011, 144, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Shoji, T.; Emoto, M.; Shinohara, K.; Kakiya, R.; Tsujimoto, Y.; Kishimoto, H.; Ishimura, E.; Tabata, T.; Nishizawa, Y. Diabetes mellitus, aortic stiffness, and cardiovascular mortality in end-stage renal disease. J. Am. Soc. Nephrol. 2001, 12, 2117–2124. [Google Scholar] [CrossRef]
- Ishioka, K.; Hidaka, S.; Fujiwara, N.; Yamano, M.; Mochida, Y.; Oka, M.; Maesato, K.; Moriya, H.; Ohtake, T.; Kobayashi, S. Association between zinc deficiency and aorta stiffness in non-diabetic hemodialysis patients. PLoS ONE 2023, 18, e0268875. [Google Scholar] [CrossRef]
- Li, Z.; Wang, W.; Liu, H.; Li, S.; Zhang, D. The association of serum zinc and copper with hypertension: A meta-analysis. J. Trace Elem. Med. Biol. 2019, 53, 41–48. [Google Scholar] [CrossRef]
- Sato, M.; Yanagisawa, H.; Nojima, Y.; Tamura, J.; Wada, O. Zn deficiency aggravates hypertension in spontaneously hypertensive rats: Possible role of Cu/Zn-superoxide dismutase. Clin. Exp. Hypertens. 2002, 24, 355–370. [Google Scholar] [CrossRef]
- Dimitrova, A.A.; Strashimirov, D.; Betova, T.; Russeva, A.; Alexandrova, M. Zinc content in the diet affects the activity of Cu/ZnSOD, lipid peroxidation and lipid profile of spontaneously hypertensive rats. Acta Biol. Hung. 2008, 59, 305–314. [Google Scholar] [CrossRef]
- Zalewski, P.D.; Beltrame, J.F.; Wawer, A.A.; Abdo, A.I.; Murgia, C. Roles for endothelial zinc homeostasis in vascular physiology and coronary artery disease. Crit. Rev. Food Sci. Nutr. 2019, 59, 3511–3525. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.M.; Mofrad, M.D.; Borges do Nascimento, I.J.; Milajerdi, A.; Mokhtari, T.; Esmaillzadeh, A. Correction to: The effect of zinc supplementation on blood pressure: A systematic review and dose-response meta-analysis of randomized-controlled trials. Eur. J. Nutr. 2020, 59, 1829. [Google Scholar] [CrossRef] [PubMed]
- Nakazono, K.; Watanabe, N.; Matsuno, K.; Sasaki, J.; Sato, T.; Inoue, M. Does superoxide underlie the pathogenesis of hypertension? Proc. Natl. Acad. Sci. USA 1991, 88, 10045–10048. [Google Scholar] [CrossRef]
- Gonzalez-Vicente, A.; Hong, N.J.; Yang, N.; Cabral, P.D.; Berthiaume, J.M.; Dominici, F.P.; Garvin, J.L. Dietary Fructose Increases the Sensitivity of Proximal Tubules to Angiotensin II in Rats Fed High-Salt Diets. Nutrients 2018, 10, 1244. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Takata, T.; Hanada, H.; Taniguchi, S.; Hamada, S.; Mae, Y.; Iyama, T.; Kanda, T.; Isomoto, H. Zinc deficiency induces hypertension by paradoxically amplifying salt sensitivity under high salt intake in mice. Clin. Exp. Nephrol. 2024, 28, 728–739. [Google Scholar] [CrossRef]
- Xie, Y.; Liu, F.; Zhang, X.; Jin, Y.; Li, Q.; Shen, H.; Fu, H.; Mao, J. Benefits and risks of essential trace elements in chronic kidney disease: A narrative review. Ann. Transl. Med. 2022, 10, 1400. [Google Scholar] [CrossRef]
- Jeng, S.S.; Chen, Y.H. Association of Zinc with Anemia. Nutrients 2022, 14, 4918. [Google Scholar] [CrossRef]
- Xia, J.; Browning, J.D.; O’Dell, B.L. Decreased plasma membrane thiol concentration is associated with increased osmotic fragility of erythrocytes in zinc-deficient rats. J. Nutr. 1999, 129, 814–819. [Google Scholar] [CrossRef]
- Tanimura, N.; Liao, R.; Wilson, G.M.; Dent, M.R.; Cao, M.; Burstyn, J.N.; Hematti, P.; Liu, X.; Zhang, Y.; Zheng, Y.; et al. GATA/Heme Multi-omics Reveals a Trace Metal-Dependent Cellular Differentiation Mechanism. Dev. Cell 2018, 46, 581–594.e4. [Google Scholar] [CrossRef]
- King, L.E.; Fraker, P.J. Zinc deficiency in mice alters myelopoiesis and hematopoiesis. J. Nutr. 2002, 132, 3301–3307. [Google Scholar] [CrossRef]
- Konomi, A.; Yokoi, K. Zinc deficiency decreases plasma erythropoietin concentration in rats. Biol. Trace Elem. Res. 2005, 107, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Feng, H.L.; Chen, Y.H.; Jeng, S.S. Effect of Zinc Supplementation on Renal Anemia in 5/6-Nephrectomized Rats and a Comparison with Treatment with Recombinant Human Erythropoietin. Int. J. Mol. Sci. 2019, 20, 4985. [Google Scholar] [CrossRef]
- Fukasawa, H.; Furuya, R.; Kaneko, M.; Nakagami, D.; Ishino, Y.; Kitamoto, S.; Omata, K.; Yasuda, H. Clinical Significance of Trace Element Zinc in Patients with Chronic Kidney Disease. J. Clin. Med. 2023, 12, 1667. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, T.; Horike, H.; Fujiki, S.; Kitada, S.; Sasaki, T.; Kashihara, N. Zinc deficiency anemia and effects of zinc therapy in maintenance hemodialysis patients. Ther. Apher. Dial. 2009, 13, 213–219. [Google Scholar] [CrossRef]
- Haase, V.H. HIF-prolyl hydroxylases as therapeutic targets in erythropoiesis and iron metabolism. Hemodial. Int. 2017, 21 (Suppl. S1), S110–S124. [Google Scholar] [CrossRef] [PubMed]
- Mokas, S.; Lariviere, R.; Lamalice, L.; Gobeil, S.; Cornfield, D.N.; Agharazii, M.; Richard, D.E. Hypoxia-inducible factor-1 plays a role in phosphate-induced vascular smooth muscle cell calcification. Kidney Int. 2016, 90, 598–609. [Google Scholar] [CrossRef]
- Zhu, Y.; Ma, W.Q.; Han, X.Q.; Wang, Y.; Wang, X.; Liu, N.F. Advanced glycation end products accelerate calcification in VSMCs through HIF-1alpha/PDK4 activation and suppress glucose metabolism. Sci. Rep. 2018, 8, 13730. [Google Scholar] [CrossRef]
- Toth, A.; Csiki, D.M.; Nagy, B., Jr.; Balogh, E.; Lente, G.; Ababneh, H.; Szoor, A.; Jeney, V. Daprodustat Accelerates High Phosphate-Induced Calcification Through the Activation of HIF-1 Signaling. Front. Pharmacol. 2022, 13, 798053. [Google Scholar] [CrossRef]
- Nakanishi, T.; Kuragano, T. Growing concerns about using hypoxia-inducible factor prolyl hydroxylase inhibitors for the treatment of renal anemia. Clin. Kidney J. 2024, 17, sfae051. [Google Scholar] [CrossRef]
- Farooq, M. Zinc Deficiency is Associated with Poor Glycemic Control. J. Coll. Physicians Surg. Pak. 2019, 29, 253–257. [Google Scholar] [CrossRef]
- Tamura, Y. The Role of Zinc Homeostasis in the Prevention of Diabetes Mellitus and Cardiovascular Diseases. J. Atheroscler. Thromb. 2021, 28, 1109–1122. [Google Scholar] [CrossRef]
- Daneshvar, M.; Ghaheri, M.; Safarzadeh, D.; Karimi, F.; Adib-Hajbagheri, P.; Ahmadzade, M.; Haedi, A. Effect of zinc supplementation on glycemic biomarkers: An umbrella of interventional meta-analyses. Diabetol. Metab. Syndr. 2024, 16, 124. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.; Ichikawa, T.; Li, J.; Si, Q.; Yang, H.; Chen, X.; Goldblatt, C.S.; Meyer, C.J.; Li, X.; Cai, L.; et al. Diabetic downregulation of Nrf2 activity via ERK contributes to oxidative stress-induced insulin resistance in cardiac cells in vitro and in vivo. Diabetes 2011, 60, 625–633. [Google Scholar] [CrossRef]
- Tang, Y.; Yang, Q.; Lu, J.; Zhang, X.; Suen, D.; Tan, Y.; Jin, L.; Xiao, J.; Xie, R.; Rane, M.; et al. Zinc supplementation partially prevents renal pathological changes in diabetic rats. J. Nutr. Biochem. 2010, 21, 237–246. [Google Scholar] [CrossRef]
- Farvid, M.S.; Jalali, M.; Siassi, F.; Hosseini, M. Comparison of the effects of vitamins and/or mineral supplementation on glomerular and tubular dysfunction in type 2 diabetes. Diabetes Care 2005, 28, 2458–2464. [Google Scholar] [CrossRef] [PubMed]
- Kadhim, H.M.; Ismail, S.H.; Hussein, K.I.; Bakir, I.H.; Sahib, A.S.; Khalaf, B.H.; Hussain, S.A. Effects of melatonin and zinc on lipid profile and renal function in type 2 diabetic patients poorly controlled with metformin. J. Pineal Res. 2006, 41, 189–193. [Google Scholar] [CrossRef]
- Parham, M.; Amini, M.; Aminorroaya, A.; Heidarian, E. Effect of zinc supplementation on microalbuminuria in patients with type 2 diabetes: A double blind, randomized, placebo-controlled, cross-over trial. Rev. Diabet. Stud. 2008, 5, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Mocchegiani, E.; Giacconi, R.; Muzzioli, M.; Cipriano, C. Zinc, infections and immunosenescence. Mech. Ageing Dev. 2000, 121, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Beck, F.W.; Prasad, A.S.; Kaplan, J.; Fitzgerald, J.T.; Brewer, G.J. Changes in cytokine production and T cell subpopulations in experimentally induced zinc-deficient humans. Am. J. Physiol. 1997, 272, E1002–E1007. [Google Scholar] [CrossRef]
- Gammoh, N.Z.; Rink, L. Zinc in Infection and Inflammation. Nutrients 2017, 9, 624. [Google Scholar] [CrossRef]
- Meydani, S.N.; Barnett, J.B.; Dallal, G.E.; Fine, B.C.; Jacques, P.F.; Leka, L.S.; Hamer, D.H. Serum zinc and pneumonia in nursing home elderly. Am. J. Clin. Nutr. 2007, 86, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Saka, Y.; Naruse, T.; Matsumoto, J.; Takeda, Y.; Onogi, C.; Yokoi, J.; Kato, A.; Tawada, N.; Noda, Y.; Niwa, S.; et al. Low Serum Zinc Concentration Is Associated With Infection Particularly in Patients With Stage 5 Chronic Kidney Disease Medicated with Proton Pump Inhibitors. J. Ren. Nutr. 2021, 31, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Barnett, J.B.; Dao, M.C.; Hamer, D.H.; Kandel, R.; Brandeis, G.; Wu, D.; Dallal, G.E.; Jacques, P.F.; Schreiber, R.; Kong, E.; et al. Effect of zinc supplementation on serum zinc concentration and T cell proliferation in nursing home elderly: A randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2016, 103, 942–951. [Google Scholar] [CrossRef]
- Prasad, A.S.; Beck, F.W.; Bao, B.; Fitzgerald, J.T.; Snell, D.C.; Steinberg, J.D.; Cardozo, L.J. Zinc supplementation decreases incidence of infections in the elderly: Effect of zinc on generation of cytokines and oxidative stress. Am. J. Clin. Nutr. 2007, 85, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Song, Y. Efficacy of zinc given as an adjunct to the treatment of severe pneumonia: A meta-analysis of randomized, double-blind and placebo-controlled trials. Clin. Respir. J. 2018, 12, 857–864. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Djafarian, K.; Mojtahed, A.; Varkaneh, H.K.; Shab-Bidar, S. The effect of zinc supplementation on plasma C-reactive protein concentrations: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pharmacol. 2018, 834, 10–16. [Google Scholar] [CrossRef]
- Huang, J.C.; Su, H.M.; Wu, P.Y.; Lee, J.J.; Lee, W.H.; Chen, S.C.; Chiu, Y.W.; Hsu, Y.L.; Chang, J.M.; Chen, H.C. Ratio of Early Mitral Inflow Velocity to the Global Diastolic Strain Rate and Global Left Ventricular Longitudinal Systolic Strain Predict Overall Mortality and Major Adverse Cardiovascular Events in Hemodialysis Patients. Dis. Markers 2019, 2019, 7512805. [Google Scholar] [CrossRef]
- Ogawa, T.; Nitta, K. Clinical Impact of Left Ventricular Diastolic Dysfunction in Chronic Kidney Disease. Contrib. Nephrol. 2018, 195, 81–91. [Google Scholar] [CrossRef]
- Escoli, R.; Carvalho, M.J.; Cabrita, A.; Rodrigues, A. Diastolic Dysfunction, an Underestimated New Challenge in Dialysis. Ther. Apher. Dial. 2019, 23, 108–117. [Google Scholar] [CrossRef]
- Yu, X.; Huang, L.; Zhao, J.; Wang, Z.; Yao, W.; Wu, X.; Huang, J.; Bian, B. The Relationship between Serum Zinc Level and Heart Failure: A Meta-Analysis. Biomed. Res. Int. 2018, 2018, 2739014. [Google Scholar] [CrossRef]
- Mohtashamian, A.; Soleimani, A.; Gilasi, H.R.; Kheiripour, N.; Moeini Taba, S.M.; Sharifi, N. Association of Zinc Status with Matrix Metalloproteinases, Advanced Glycation End-Products, and Blood Pressure in Patients with Chronic Kidney Disease. Biol. Trace Elem. Res. 2023, 201, 4275–4285. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.-T.; Shiu, Y.-L.; Chen, C.-A.; Lin, H.-Y.; Huang, Y.-L.; Lin, C.-C. Changes in levels of copper, iron, zinc, and selenium in patients at different stages of chronic kidney disease. Genom. Med. Biomark. Health Sci. 2012, 4, 128–130. [Google Scholar] [CrossRef]
- Kung, W.J.; Shih, C.T.; Lee, C.H.; Lin, C.C. The Divalent Elements Changes in Early Stages of Chronic Kidney Disease. Biol. Trace Elem. Res. 2018, 185, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Tokuyama, A.; Kanda, E.; Itano, S.; Kondo, M.; Wada, Y.; Kadoya, H.; Kidokoro, K.; Nagasu, H.; Sasaki, T.; Kashihara, N. Effect of zinc deficiency on chronic kidney disease progression and effect modification by hypoalbuminemia. PLoS ONE 2021, 16, e0251554. [Google Scholar] [CrossRef]
- Huang, Z.; Liao, Y.; Zheng, Y.; Ye, S.; Zhang, Q.; Yu, X.; Liu, X.; Li, N. Zinc Deficiency Causes Glomerulosclerosis and Renal Interstitial Fibrosis Through Oxidative Stress and Increased Lactate Metabolism in Rats. Biol. Trace Elem. Res. 2024, 203, 2084–2098. [Google Scholar] [CrossRef]
- Maiguma, M.; Suzuki, Y.; Suzuki, H.; Okazaki, K.; Aizawa, M.; Muto, M.; Tomino, Y. Dietary zinc is a key environmental modifier in the progression of IgA nephropathy. PLoS ONE 2014, 9, e90558. [Google Scholar] [CrossRef]
- Mbanefo, N.R.; Uwaezuoke, S.N.; Eneh, C.I.; Odimegwu, C.L.; Chikani, U.N.; Muoneke, U.V.; Nwolisa, C.E.; Odo, K.E.; Ogbuka, F.N.; Akwue, A.T. Can Oral Zinc Supplementation Reduce Relapses in Childhood Steroid-Sensitive Nephrotic Syndrome? A Systematic Review. Int. J. Nephrol. Renov. Dis. 2023, 16, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Hara, T.; Yoshigai, E.; Ohashi, T.; Fukada, T. Zinc in Cardiovascular Functions and Diseases: Epidemiology and Molecular Mechanisms for Therapeutic Development. Int. J. Mol. Sci. 2023, 24, 7152. [Google Scholar] [CrossRef]
- Chu, A.; Foster, M.; Samman, S. Zinc Status and Risk of Cardiovascular Diseases and Type 2 Diabetes Mellitus-A Systematic Review of Prospective Cohort Studies. Nutrients 2016, 8, 707. [Google Scholar] [CrossRef]
- Pilz, S.; Dobnig, H.; Winklhofer-Roob, B.M.; Renner, W.; Seelhorst, U.; Wellnitz, B.; Boehm, B.O.; Marz, W. Low serum zinc concentrations predict mortality in patients referred to coronary angiography. Br. J. Nutr. 2009, 101, 1534–1540. [Google Scholar] [CrossRef]
- Soinio, M.; Marniemi, J.; Laakso, M.; Pyorala, K.; Lehto, S.; Ronnemaa, T. Serum zinc level and coronary heart disease events in patients with type 2 diabetes. Diabetes Care 2007, 30, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Knehtl, M.; Piko, N.; Ekart, R.; Hojs, R.; Bevc, S. Serum zinc values, ankle brachial index and mortality in hemodialysis patients. BMC Nephrol. 2022, 23, 355. [Google Scholar] [CrossRef]
- Prasad, A.S.; Oberleas, D. Binding of zinc to amino acids and serum proteins in vitro. J. Lab. Clin. Med. 1970, 76, 416–425. [Google Scholar]
- Nakatani, S.; Shoji, T.; Morioka, F.; Nakaya, R.; Ueda, M.; Uedono, H.; Tsuda, A.; Morioka, T.; Fujii, H.; Yoshida, H.; et al. Association between Serum Zinc and All-Cause Mortality in Patients Undergoing Maintenance Hemodialysis: The Osaka Dialysis Complication Study (ODCS). Nutrients 2024, 16, 3270. [Google Scholar] [CrossRef]
- Garagarza, C.; Valente, A.; Caetano, C.; Ramos, I.; Sebastiao, J.; Pinto, M.; Oliveira, T.; Ferreira, A.; Sousa Guerreiro, C. Zinc Deficient Intake in Hemodialysis Patients: A Path to a High Mortality Risk. J. Ren. Nutr. 2022, 32, 87–93. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).