
Adherence to Mediterranean Diet and Implications for Cardiovascular Risk Prevention

 ,
,  ,
,  , , and
, , and 
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Dietary Habits and MedDiet Adherence
2.3. Evaluation of Body Composition
2.4. Cardiovascular Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AI@75 | Augmentation index normalized to a heart rate of 75 beats per minute |
| AIP | Atherogenic Index of Plasma |
| APOE | Apolipoprotein E |
| AS | Arterial Stiffness |
| BAI | Body Adiposity Index |
| BCM | Body Cell Mass |
| BIA | Bioelectrical Impedance Analysis |
| BMI | Body Mass Index |
| BP | Blood Pressure |
| BSA | Body Surface Area |
| c-Dia BP | Central Diastolic Blood Pressure |
| C-HDL | High-Density Lipoprotein Cholesterol |
| cIMT | Carotid Intima-Media Thickness |
| C-LDL | Low-Density Lipoprotein Cholesterol |
| c-Sys BP | Central Systolic Blood Pressure |
| C-TOT | Total Cholesterol |
| CVD | Cardiovascular Diseases |
| DXA | Dual-Energy X-Ray Absorptiometry |
| EVO | Extra Virgin Olive Oil |
| FFM | Fat-Free Mass |
| FFQ | Food Frequency Questionnaire |
| FM | Fat Mass |
| FT3 | Free triiodiotironine |
| GOT | Glutamic Oxalo-Acetic Transaminase |
| GPT | Glutamate Pyruvate Transaminase |
| HDL | High-Density Lipoprotein |
| HR | Heart Rate |
| HOMA-IR | Homeostatic Model Assessment for Insulin Resistance |
| IMAT | Intramuscular Adipose Tissue |
| IVRT | Isovolumic Relaxation Time |
| IVSd | Inter-Ventricular Septum Thickness |
| LA | Left Atrial |
| LDL | Low-Density Lipoprotein |
| LM | Lean Mass |
| Lp(a) | Lipoprotein (a) |
| LV | Left Ventricular |
| LVH | Left Ventricle Hypertrophy |
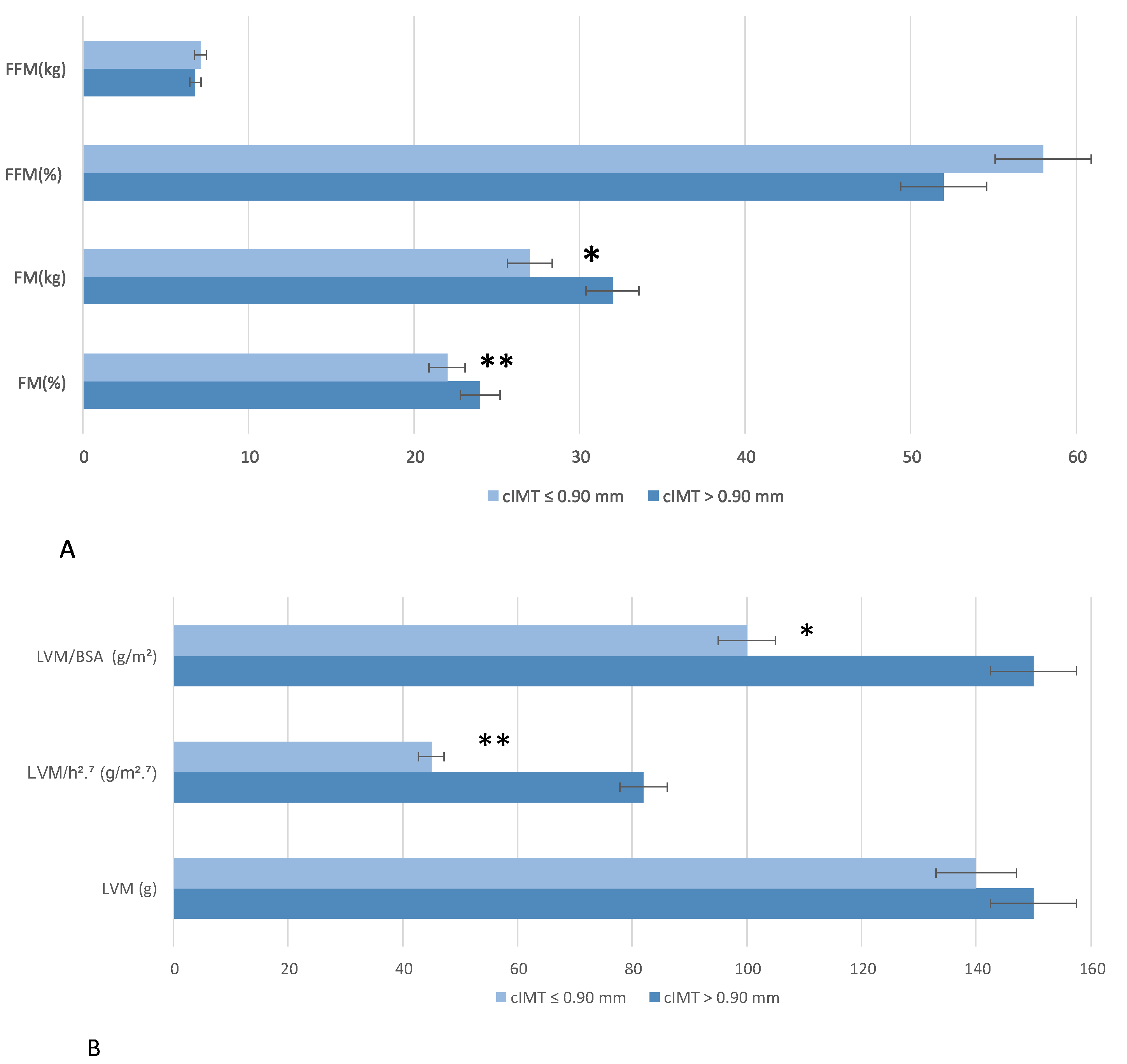
| LVM | Left Ventricle Mass |
| LVM/BSA | Left Ventricle Mass/Body surface area |
| LVM/h2.7 | Left Ventricle Mass/height2.7 |
| MEDAS | Mediterranean Diet Adherence Screener |
| MedDiet | Mediterranean Diet |
| PhA | Phase Angle |
| PWTd | Posterior Wall Thickness |
| PWV | Pulse Wave Velocity |
| SAT | Subcutaneous Adipose Tissue |
| SD | Standard Deviation |
| Sys | Systolic Blood Pressure |
| TBB | Total Body Bone Mass |
| TBW | Total Body Water |
| TDI | Tissue Doppler Imaging |
| TSA | Supra-Aortic Trunks |
| VAT | Visceral Adipose Tissue |
| WHR | Waist-To-Hip Ratio |
Appendix A
Appendix A.1

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions | Yes = 1/No = 0 |
|---|---|
| 1. Is olive oil the main culinary fat used? | |
| 2. Are four tablespoons of olive oil used each day? | |
| 3. Are two servings (of 200 g each) of vegetables eaten each day? | |
| 4. Are three servings of fruit (of 80 g each) eaten each day? | |
| 5. Is <1 serving (100–150 g) of red meat/hamburgers/other meat products eaten each day? | |
| 6. Was <1 serving (12 g) of butter, margarine, or cream eaten each day? | |
| 7. Is <1 serving (330 mL) of sweet or sugar-sweetened carbonated beverages consumed each day? | |
| 8. Are three glasses (of 125 mL) of wine consumed each week? | |
| 9. Are three servings (of 150 g) of legumes consumed each week? | |
| 10. Are three servings of fish (100–150 g) or seafood (200 g) eaten each week? | |
| 11. Is <3 servings of commercial sweets/pastries eaten each week? | |
| 12. Is one serving (of 30 g) of nuts consumed each week? | |
| 13. Is chicken, turkey, or rabbit routinely eaten instead of veal, pork, hamburger, or sausage? | |
| 14. Are pasta, vegetable, or rice dishes flavored with garlic, tomato, leek, or onion eaten ≥twice a week? |
Appendix A.2
| n Sample = 55 | |
|---|---|
| FM% (Siri) | 28.00 ± 9.00 |
| BAI (%) | 28.60 ± 5.50 |
| Mean handgrip max strenght (Kg) | 35.00 ± 11.00 |
| PhA (°) | 5.89 ± 0.88 |
| Z (ohm) | 532.00 ± 92.00 |
| FM (kg) | 23.00 ± 9.00 |
| FM (%) | 29.00 ± 9.00 |
| FFM (kg) | 55.00 ± 13.00 |
| FFM (%) | 70.00 ± 10.00 |
| BCM (kg) | 30.00 ± 8.00 |
| BCM (%) | 39.00 ± 7.00 |
| BCMI (kg/m2) | 10.50 ± 2.18 |
| Total Fat (g) | 22.17 ± 9.77 |
| Total Lean (g) | 51.56 ± 11.41 |
| FM % | 28.00 ± 11.00 |
| IMAT | 0.91 ± 0.45 |
| ASMMI | 8.03 ± 1.24 |
| VAT/SAT | 0.34 ± 0.17 |
| HGB (g/dL) | 13.79 ± 1.18 |
| HTC (%) | 41.55 ± 2.69 |
| Glycemia (mg/dL) | 93.00 ± 13.00 |
| Insulin (uUI/mL) | 8.42 ± 2.12 |
| C-TOT (mg/dL) | 213.00 ± 43.00 |
| C-HDL (mg/dL) | 61.00 ± 22.00 |
| C-LDL (mg/dL) | 131.00 ± 33.00 |
| TG (mg/dL) | 115.00 ± 52.00 |
| GOT (U/lt) | 28.00 ± 19.00 |
| GPT (U/lt) | 26.00 ± 14.00 |
| Azotemia (mg/dL) | 27.00 ± 10.00 |
| Creatinine (mg/dL) | 0.83 ± 0.12 |
| Uric Acid (mg/dL) | 4.97 ± 1.23 |
| Lipoprotein(a) | 43.00 ± 38.00 |
| TSH microUI/mL | 2.17 ± 1.00 |
| ft3/ft4 | 2.71 ± 1.26 |
| PTL | 308.17 ± 363.55 |
| Lymphocytes | 2.08 ± 464.00 |
| Neutrophilis | 3.32 ± 905.00 |
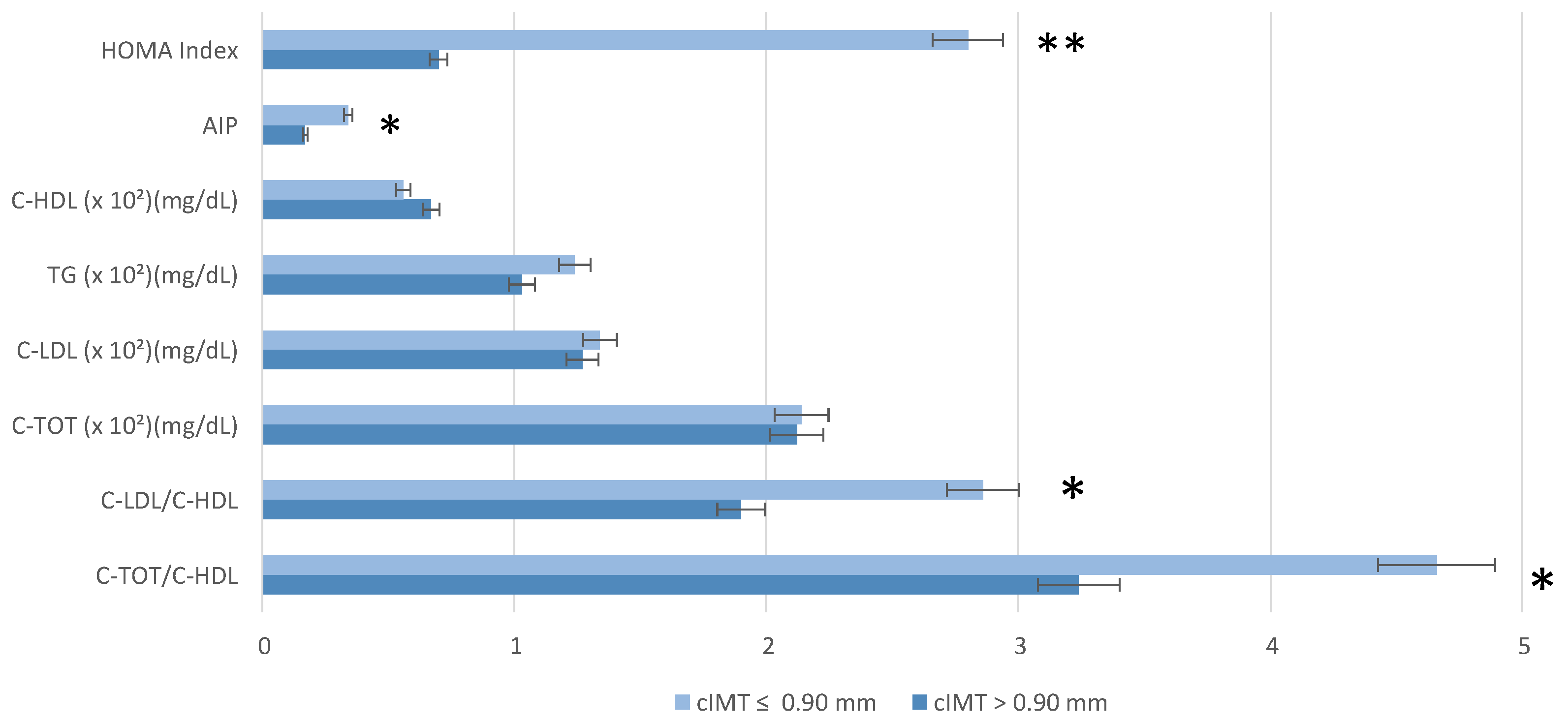
| Homa-Index | 1.63 ± 4.62 |
| TyG | 8.47 ± 0.50 |
| tg/hdl | 2.40 ± 1.97 |
| C-TOT/C-HDL | 4.03 ± 1.96 |
| C-LDL/C-HDL | 2.47 ± 1.58 |
| AIP | 0.26 ± 0.32 |
| PLR | 148.00 ± 150.00 |
| NLR | 1.66 ± 0.51 |
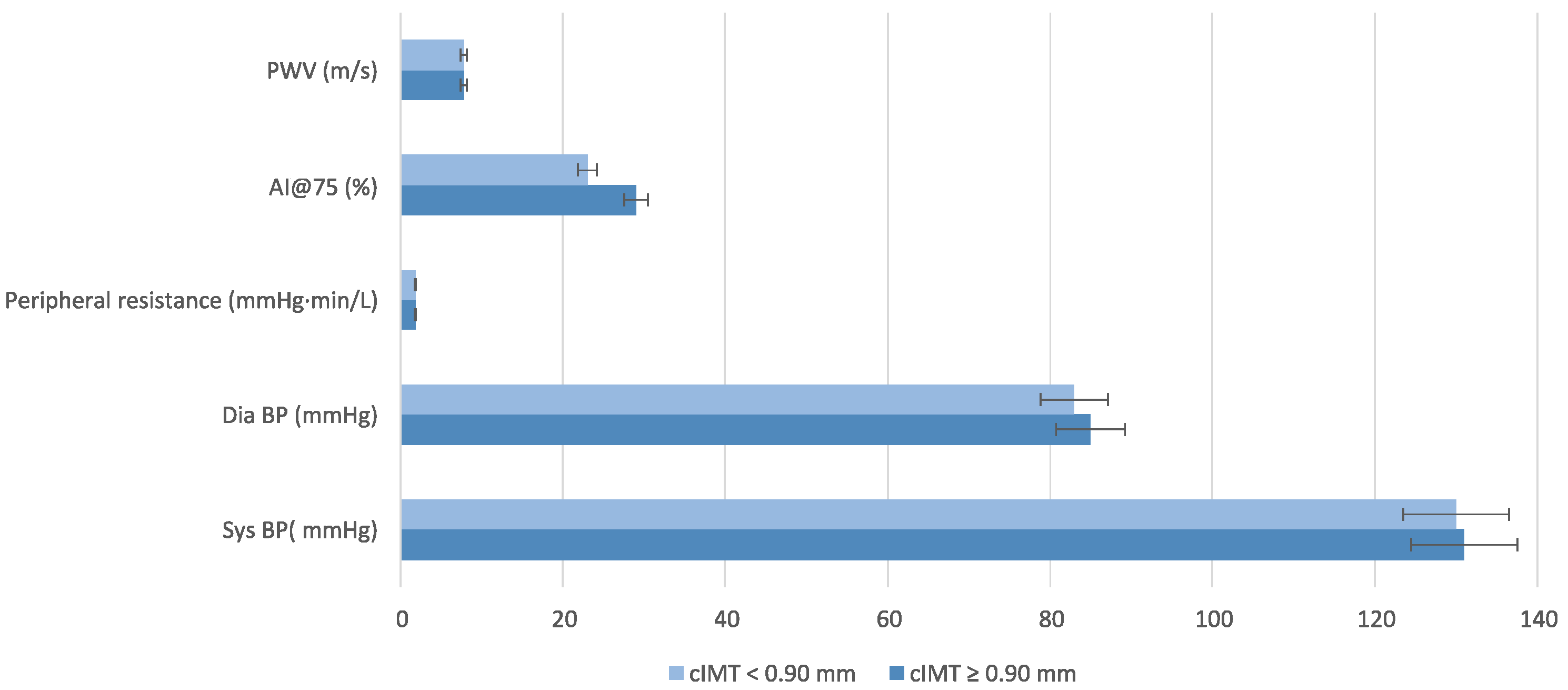
| Systolic BP (mmHg) | 130.00 ± 16.00 |
| Diastolic BP(mmHg) | 84.00 ± 11.00 |
| PAM | 105.00 ± 12.00 |
| Pulse Pressure (mmHg) | 47.00 ± 11.00 |
| Heart Rate (1/min) | 68.00 ± 10.00 |
| cSis (mmHg) | 120.00 ± 21.00 |
| cDia (mmHg) | 85.00 ± 11.00 |
| Peripheral Resistance (Dyn × s/cm5) | 1.81 ± 236.00 |
| AI@75 | 26.00 ± 11.00 |
| PWV (m/s) | 7.87 ± 1.02 |
| cIMT | 0.83 ± 0.16 |
References
- Tattersall, M.C.; Hansen, S.L.; McClelland, R.L.; Korcarz, C.E.; Hansen, K.M.; Post, W.S.; Shapiro, M.D.; Stein, J.H. Importance of Age and Sex in Carotid Artery Plaque Detection and Cardiovascular Disease Risk. JAMA Cardiol. 2025, 10, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Juhasz, V.; Suero-Abreu, G.A.; Neilan, T.G. Immune Checkpoint Inhibitors and Myocardial Infarction. J. Thromb. Thrombolysis 2025, 83, 102334. [Google Scholar] [CrossRef] [PubMed]
- Arnold, N.; Koenig, W. Inflammation in Atherosclerotic Cardiovascular Disease: From Diagnosis to Treatment. Eur. J. Clin. Investig. 2025, e70020. [Google Scholar] [CrossRef] [PubMed]
- Muiesan, M.L.; Virdis, A.; Tocci, G.; Borghi, C.; Cicero, A.F.G.; Ferri, C.; Pirro, M.; Corsini, A.; Volpe, M. 2024 Consensus Document of the Italian Society of Arterial Hypertension (SIIA) and the Italian Society of Cardiovascular Prevention (SIPREC): Update on LDL Cholesterol Lowering in Patients with Arterial Hypertension. High Blood Press. Cardiovasc. Prev. 2025, 32, 151–163. [Google Scholar] [CrossRef]
- Pala, B.; Tocci, G.; Nardoianni, G.; Barbato, E.; Amedei, A. Gut Microbiome and Carotid Artery Intima-Media Thickness: A Narrative Review of the Current Scenario. Diagnostics 2024, 14, 2463. [Google Scholar] [CrossRef]
- Tocci, G.; Presta, V. Increased Arterial Stiffness and Haemorrhagic Transformation in Ischaemic Stroke after Thrombolysis: A New Marker of Risk for Cerebrovascular Events and Complications. Int. J. Cardiol. 2017, 243, 471–472. [Google Scholar] [CrossRef]
- Wang, M.; McGraw, K.R.; Monticone, R.E.; Pintus, G. Unraveling Elastic Fiber-Derived Signaling in Arterial Aging and Related Arterial Diseases. Biomolecules 2025, 15, 153. [Google Scholar] [CrossRef]
- Iacobellis, G. Epicardial Fat Links Obesity to Cardiovascular Diseases. Prog. Cardiovasc. Dis. 2023, 78, 27–33. [Google Scholar] [CrossRef]
- Ortega-Loubon, C.; Fernández-Molina, M.; Singh, G.; Correa, R. Obesity and Its Cardiovascular Effects. Diabetes Metab. Res. 2019, 35, e3135. [Google Scholar] [CrossRef]
- Akoumianakis, I.; Antoniades, C. The Interplay between Adipose Tissue and the Cardiovascular System: Is Fat Always Bad? Cardiovasc. Res. 2017, 113, 999–1008. [Google Scholar] [CrossRef]
- Koenen, M.; Hill, M.A.; Cohen, P.; Sowers, J.R. Obesity, Adipose Tissue and Vascular Dysfunction. Circ. Res. 2021, 128, 951–968. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.K.; Antoniades, C. The Role of Adipose Tissue in Cardiovascular Health and Disease. Nat. Rev. Cardiol. 2019, 16, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Frank, G.; Cianci, R.; Caldarelli, M.; Leggeri, G.; Raffaelli, G.; Pizzocaro, E.; Cirillo, M.; De Lorenzo, A. Exploring the Exposome Spectrum: Unveiling Endogenous and Exogenous Factors in Non-Communicable Chronic Diseases. Diseases 2024, 12, 176. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Frank, G.; De Lorenzo, A. Nutrition for Prevention and Control of Chronic Degenerative Diseases and COVID-19. Nutrients 2023, 15, 2253. [Google Scholar] [CrossRef]
- Marchetti, M.; Gualtieri, P.; De Lorenzo, A.; Trombetta, D.; Smeriglio, A.; Ingegneri, M.; Cianci, R.; Frank, G.; Schifano, G.; Bigioni, G.; et al. Dietary ω-3 Intake for the Treatment of Morning Headache: A Randomized Controlled Trial. Front. Neurol. 2022, 13, 987958. [Google Scholar] [CrossRef]
- Nestel, P.J.; Mori, T.A. Dietary Patterns, Dietary Nutrients and Cardiovascular Disease. Rev. Cardiovasc. Med. 2022, 23, 17. [Google Scholar] [CrossRef]
- Fukumoto, Y. Nutrition and Cardiovascular Diseases. Nutrients 2021, 14, 94. [Google Scholar] [CrossRef]
- Jimenez-Torres, J.; Alcalá-Diaz, J.F.; Torres-Peña, J.D.; Gutierrez-Mariscal, F.M.; Leon-Acuña, A.; Gómez-Luna, P.; Fernández-Gandara, C.; Quintana-Navarro, G.M.; Fernandez-Garcia, J.C.; Perez-Martinez, P.; et al. Mediterranean Diet Reduces Atherosclerosis Progression in Coronary Heart Disease: An Analysis of the CORDIOPREV Randomized Controlled Trial. Stroke 2021, 52, 3440–3449. [Google Scholar] [CrossRef]
- Gualtieri, P.; Marchetti, M.; Frank, G.; Cianci, R.; Bigioni, G.; Colica, C.; Soldati, L.; Moia, A.; De Lorenzo, A.; Di Renzo, L. Exploring the Sustainable Benefits of Adherence to the Mediterranean Diet during the COVID-19 Pandemic in Italy. Nutrients 2022, 15, 110. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Frank, G.; De Santis, G.L.; Cianci, R.; Bigioni, G.; De Lorenzo, A. Sex Differences in the Efficacy of Mediterranean Diet Treatment: A Nutrigenomics Pilot Study. Genes 2023, 14, 1980. [Google Scholar] [CrossRef]
- Buscemi, S.; Rosafio, G.; Vasto, S.; Massenti, F.M.; Grosso, G.; Galvano, F.; Rini, N.; Barile, A.M.; Maniaci, V.; Cosentino, L.; et al. Validation of a Food Frequency Questionnaire for Use in Italian Adults Living in Sicily. Int. J. Food Sci. Nutr. 2015, 66, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Frank, G.; Cianci, R.; Raffaelli, G.; Peluso, D.; Bigioni, G.; De Lorenzo, A. Sex-Specific Adherence to the Mediterranean Diet in Obese Individuals. Nutrients 2024, 16, 3076. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Itani, L.; El Ghoch, M.; Gualtieri, P.; Frank, G.; Raffaelli, G.; Pellegrini, M.; Di Renzo, L. Difference in Body Composition Patterns between Age Groups in Italian Individuals with Overweight and Obesity: When BMI Becomes a Misleading Tool in Nutritional Settings. Nutrients 2024, 16, 2415. [Google Scholar] [CrossRef]
- Haun, D.R.; Pitanga, F.J.G.; Lessa, I. Razão Cintura/Estatura Comparado a Outros Indicadores Antropométricos de Obesidade Como Preditor de Risco Coronariano Elevado. Rev. Assoc. Med. Bras. 2009, 55, 705–711. [Google Scholar] [CrossRef]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A Better Index of Body Adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef]
- Di Renzo, L.; Marchetti, M.; Cioccoloni, G.; Gratteri, S.; Capria, G.; Romano, L.; Soldati, L.; Mele, M.C.; Merra, G.; Cintoni, M.; et al. Role of Phase Angle in the Evaluation of Effect of an Immuno-Enhanced Formula in Post-Surgical Cancer Patients: A Randomized Clinical Trial. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1322–1334. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Sasso, G.F.; Andreoli, A.; Sorge, R.; Candeloro, N.; Cairella, M. Improved Prediction Formula for Total Body Water Assessment in Obese Women. Int. J. Obes. Relat. Metab. Disord. 1995, 19, 535–538. [Google Scholar]
- De Lorenzo, A.; Itani, L.; El Ghoch, M.; Frank, G.; De Santis, G.L.; Gualtieri, P.; Di Renzo, L. The Association between Sarcopenic Obesity and DXA-Derived Visceral Adipose Tissue (VAT) in Adults. Nutrients 2024, 16, 1645. [Google Scholar] [CrossRef]
- Bauer, J.; Thornton, J.; Heymsfield, S.; Kelly, K.; Ramirez, A.; Gidwani, S.; Gallagher, D. Dual-Energy X-Ray Absorptiometry Prediction of Adipose Tissue Depots in Children and Adolescents. Pediatr. Res. 2012, 72, 420–425. [Google Scholar] [CrossRef]
- Mancia, G.; Kreutz, R.; Brunström, M.; Burnier, M.; Grassi, G.; Januszewicz, A.; Muiesan, M.L.; Tsioufis, K.; Agabiti-Rosei, E.; Algharably, E.A.E.; et al. 2023 ESH Guidelines for the Management of Arterial Hypertension The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J. Hypertens. 2023, 41, 1874–2071. [Google Scholar] [CrossRef] [PubMed]
- Hametner, B.; Wassertheurer, S.; Kropf, J.; Mayer, C.; Eber, B.; Weber, T. Oscillometric Estimation of Aortic Pulse Wave Velocity: Comparison with Intra-Aortic Catheter Measurements. Blood Press Monit 2013, 18, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Nichols, W.W.; Singh, B.M. Augmentation Index as a Measure of Peripheral Vascular Disease State. Curr. Opin. Cardiol. 2002, 17, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Paiva, A.M.G.; Mota-Gomes, M.A.; Brandão, A.A.; Silveira, F.S.; Silveira, M.S.; Okawa, R.T.P.; Feitosa, A.D.M.; Sposito, A.C.; Nadruz, W. Reference Values of Office Central Blood Pressure, Pulse Wave Velocity, and Augmentation Index Recorded by Means of the Mobil-O-Graph PWA Monitor. Hypertens. Res. 2020, 43, 1239–1248. [Google Scholar] [CrossRef]
- Lancellotti, P.; Galderisi, M.; Edvardsen, T.; Donal, E.; Goliasch, G.; Cardim, N.; Magne, J.; Laginha, S.; Hagendorff, A.; Haland, T.F.; et al. Echo-Doppler Estimation of Left Ventricular Filling Pressure: Results of the Multicentre EACVI Euro-Filling Study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 961–968. [Google Scholar] [CrossRef]
- Levy, D.; Garrison, R.J.; Savage, D.D.; Kannel, W.B.; Castelli, W.P. Prognostic Implications of Echocardiographically Determined Left Ventricular Mass in the Framingham Heart Study. N. Engl. J. Med. 1990, 322, 1561–1566. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart. J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Perrone-Filardi, P.; Coca, A.; Galderisi, M.; Paolillo, S.; Alpendurada, F.; de Simone, G.; Donal, E.; Kahan, T.; Mancia, G.; Redon, J.; et al. Non-Invasive Cardiovascular Imaging for Evaluating Subclinical Target Organ Damage in Hypertensive Patients: A Consensus Paper from the European Association of Cardiovascular Imaging (EACVI), the European Society of Cardiology Council on Hypertension, and the European Society of Hypertension (ESH). Eur. Heart J. Cardiovasc. Imaging 2017, 18, 945–960. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Wu, T.-T.; Gao, Y.; Zheng, Y.-Y.; Ma, Y.-T.; Xie, X. Atherogenic Index of Plasma (AIP): A Novel Predictive Indicator for the Coronary Artery Disease in Postmenopausal Women. Lipids Health Dis. 2018, 17, 197. [Google Scholar] [CrossRef]
- Greco, A.; Finocchiaro, S.; Spagnolo, M.; Faro, D.C.; Mauro, M.S.; Raffo, C.; Sangiorgio, G.; Imbesi, A.; Laudani, C.; Mazzone, P.M.; et al. Lipoprotein(a) as a Pharmacological Target: Premises, Promises, and Prospects. Circulation 2025, 151, 400–415. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Molani-Gol, R.; Rafraf, M. Effects of the Mediterranean Diet on the Secondary Prevention of Cardiovascular Diseases: A Systematic Review of Randomised Controlled Trials. Int. J. Food Sci. Nutr. 2025, 76, 226–238. [Google Scholar] [CrossRef]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-Style Diet for the Primary and Secondary Prevention of Cardiovascular Disease. Cochrane Database Syst. Rev. 2019, 3, CD009825. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E. Benefits of the Mediterranean Diet: Insights from the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef]
- Ros, E.; Martínez-González, M.A.; Estruch, R.; Salas-Salvadó, J.; Fitó, M.; Martínez, J.A.; Corella, D. Mediterranean Diet and Cardiovascular Health: Teachings of the PREDIMED Study. Adv. Nutr. 2014, 5, 330S–336S. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Dietary Patterns, Mediterranean Diet, and Cardiovascular Disease. Curr. Opin. Lipidol. 2014, 25, 20–26. [Google Scholar] [CrossRef]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J. Gerontol. Ser. A 2018, 73, 318–326. [Google Scholar] [CrossRef]
- Almevall, A.D.; Wennberg, P.; Liv, P.; Nyman, E.; Lindvall, K.; Norberg, M.; Chorell, E.; Wennberg, M. Midlife Mediterranean Diet is Associated with Subclinical Carotid Atherosclerosis in Late Midlife. Eur J Prev Cardiol. 2025, zwaf155. [Google Scholar] [CrossRef]
- Gómez Sánchez, M.; Gómez Sánchez, L.; Patino-Alonso, M.C.; Alonso-Domínguez, R.; Sánchez-Aguadero, N.; Lugones-Sánchez, C.; Rodríguez Sánchez, E.; García Ortiz, L.; Gómez-Marcos, M.A. Adherence to the Mediterranean Diet in Spanish Population and Its Relationship with Early Vascular Aging according to Sex and Age: EVA Study. Nutrients 2020, 12, 1025. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Deng, Y.; Ma, Y.; Man, S.; Yang, X.; Yu, C.; Lv, J.; Liu, H.; Wang, B.; Li, L. Adherence to a Healthy Diet and Risk of Multiple Carotid Atherosclerosis Subtypes: Insights from the China MJ Health Check-Up Cohort. Nutrients 2024, 16, 2338. [Google Scholar] [CrossRef] [PubMed]
- Rychter, A.M.; Naskręt, D.; Zawada, A.; Ratajczak, A.E.; Dobrowolska, A.; Krela-Kaźmierczak, I. What Can We Change in Diet and Behaviour in Order to Decrease Carotid Intima-Media Thickness in Patients with Obesity? J. Pers. Med. 2021, 11, 505. [Google Scholar] [CrossRef]
- Ivey, K.L.; Lewis, J.R.; Hodgson, J.M.; Zhu, K.; Dhaliwal, S.S.; Thompson, P.L.; Prince, R.L. Association between Yogurt, Milk, and Cheese Consumption and Common Carotid Artery Intima-Media Thickness and Cardiovascular Disease Risk Factors in Elderly Women. Am. J. Clin. Nutr. 2011, 94, 234–239. [Google Scholar] [CrossRef]
- Haring, B.; Wang, W.; Fretts, A.; Shimbo, D.; Lee, E.T.; Howard, B.V.; Roman, M.J.; Devereux, R.B. Red Meat Consumption and Cardiovascular Target Organ Damage (from the Strong Heart Study). J. Hypertens. 2017, 35, 1794–1800. [Google Scholar] [CrossRef]
- Wang, D.; Karvonen-Gutierrez, C.A.; Jackson, E.A.; Elliott, M.R.; Appelhans, B.M.; Barinas-Mitchell, E.; Bielak, L.F.; Huang, M.-H.; Baylin, A. Western Dietary Pattern Derived by Multiple Statistical Methods Is Prospectively Associated with Subclinical Carotid Atherosclerosis in Midlife Women. J. Nutr. 2020, 150, 579–591. [Google Scholar] [CrossRef]
- Key, T.J.; Appleby, P.N.; Bradbury, K.E.; Sweeting, M.; Wood, A.; Johansson, I.; Kühn, T.; Steur, M.; Weiderpass, E.; Wennberg, M.; et al. Consumption of Meat, Fish, Dairy Products, and Eggs and Risk of Ischemic Heart Disease: A Prospective Study of 7198 Incident Cases Among 409 885 Participants in the Pan-European EPIC Cohort. Circulation 2019, 139, 2835–2845. [Google Scholar] [CrossRef]
- Tzelefa, V.; Tsirimiagkou, C.; Argyris, A.; Moschonis, G.; Perogiannakis, G.; Yannakoulia, M.; Sfikakis, P.; Protogerou, A.D.; Karatzi, K. Associations of Dietary Patterns with Blood Pressure and Markers of Subclinical Arterial Damage in Adults with Risk Factors for CVD. Public Health Nutr. 2021, 24, 6075–6084. [Google Scholar] [CrossRef]
- Santangelo, C.; Varì, R.; Scazzocchio, B.; De Sancti, P.; Giovannini, C.; D’Archivio, M.; Masella, R. Anti-Inflammatory Activity of Extra Virgin Olive Oil Polyphenols: Which Role in the Prevention and Treatment of Immune-Mediated Inflammatory Diseases? Endocr. Metab. Immune Disord. Drug Targets 2017, 18, 36–50. [Google Scholar] [CrossRef]
- Wongwarawipat, T.; Papageorgiou, N.; Bertsias, D.; Siasos, G.; Tousoulis, D. Olive Oil-Related Anti-Inflammatory Effects on Atherosclerosis: Potential Clinical Implications. Endocr. Metab. Immune Disord. Drug Targets 2017, 18, 51–62. [Google Scholar] [CrossRef]
- Nocella, C.; Cammisotto, V.; Fianchini, L.; D’Amico, A.; Novo, M.; Castellani, V.; Stefanini, L.; Violi, F.; Carnevale, R. Extra Virgin Olive Oil and Cardiovascular Diseases: Benefits for Human Health. Endocr. Metab. Immune Disord. Drug Targets 2017, 18, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.L.; Comperatore, M.; Barona, J.; Calle, M.C.; Andersen, C.; McIntosh, M.; Najm, W.; Lerman, R.H.; Fernandez, M.L. A Mediterranean-Style, Low-Glycemic-Load Diet Decreases Atherogenic Lipoproteins and Reduces Lipoprotein (a) and Oxidized Low-Density Lipoprotein in Women with Metabolic Syndrome. Metabolism 2012, 61, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Lampsas, S.; Xenou, M.; Oikonomou, E.; Pantelidis, P.; Lysandrou, A.; Sarantos, S.; Goliopoulou, A.; Kalogeras, K.; Tsigkou, V.; Kalpis, A.; et al. Lipoprotein(a) in Atherosclerotic Diseases: From Pathophysiology to Diagnosis and Treatment. Molecules 2023, 28, 969. [Google Scholar] [CrossRef] [PubMed]
- Yari, Z.; Tabibi, H.; Najafi, I.; Hedayati, M.; Movahedian, M. Effects of soy isoflavones on serum lipids and lipoprotein (a) in peritoneal dialysis patients. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1382–1388. [Google Scholar] [CrossRef]
- Nikoohemmat, M.; Ahmadi, A.R.; Valizadeh, A.; Moteshakereh, S.M.; Yari-Boroujeni, R.; Seifi, Z.; Valizadeh, M.; Abiri, B. Association between Body Composition Indices and Vascular Health: A Systematic Review and Meta-Analysis. Eat Weight Disord. 2025, 30, 3. [Google Scholar] [CrossRef]
- Kang, P.S.; Neeland, I.J. Body Fat Distribution, Diabetes Mellitus, and Cardiovascular Disease: An Update. Curr. Cardiol. Rep. 2023, 25, 1555–1564. [Google Scholar] [CrossRef]
- Kubra Ata Ozturk, H.; Zeybek, V.; Kurtulus Dereli, A.; Acar, K.; Dogu Kılıc, I.; Tekin, O.; Akca, A. The Relationships between Anthropometric Measurements, Organ Weights and Intracranial, Carotid and Coronary Atherosclerosis. BMC Cardiovasc. Disord. 2025, 25, 155. [Google Scholar] [CrossRef]
- Lear, S.A.; Sarna, L.K.; Siow, T.J.; Mancini, G.B.J.; Siow, Y.L.; Karmin, O. Oxidative Stress Is Associated with Visceral Adipose Tissue and Subclinical Atherosclerosis in a Healthy Multi-Ethnic Population. Appl. Physiol. Nutr. Metab. 2012, 37, 1164–1170. [Google Scholar] [CrossRef]
- Chartrand, D.J.; Murphy-Després, A.; Alméras, N.; Lemieux, I.; Larose, E.; Després, J.-P. Overweight, Obesity, and CVD Risk: A Focus on Visceral/Ectopic Fat. Curr. Atheroscler. Rep. 2022, 24, 185–195. [Google Scholar] [CrossRef]
- Hyun, Y.J.; Koh, S.J.; Chae, J.S.; Kim, J.Y.; Kim, O.Y.; Lim, H.H.; Jang, Y.; Park, S.; Ordovas, J.M.; Lee, J.H. Atherogenecity of LDL and Unfavorable Adipokine Profile in Metabolically Obese, Normal-weight Woman. Obesity 2008, 16, 784–789. [Google Scholar] [CrossRef]
- Alanazi, M.A.; Alshehri, K.; Alerwy, F.H.; Alrasheed, T.; Lahza, H.F.M.; Aref Albezrah, N.K.; Alghabban, Y.I.; Mohammed Abdulghani, M.A. Abdominal Volume Index Is Associated with Higher Oxidized LDL, High Blood Pressure and Lower HDL among Obese Adults. BMC Endocr. Disord. 2025, 25, 56. [Google Scholar] [CrossRef] [PubMed]
- Song, X.-T.; Rui, Y.-F.; Fan, L.; Yan, Z.-N. Echocardiographic Association of Epicardial Adipose Tissue with Ascending Aorta Elasticity in Patients with Type 2 Diabetes Mellitus. Angiology 2023, 74, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Covassin, N.; Sert-Kuniyoshi, F.H.; Singh, P.; Romero-Corral, A.; Davison, D.E.; Lopez-Jimenez, F.; Jensen, M.D.; Somers, V.K. Experimental Weight Gain Increases Ambulatory Blood Pressure in Healthy Subjects: Implications of Visceral Fat Accumulation. Mayo Clin. Proc. 2018, 93, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Liu, X.; Lo, K.; Huang, Y.; Feng, Y. The Effect of Total Cholesterol/High-Density Lipoprotein Cholesterol Ratio on Mortality Risk in the General Population. Front. Endocrinol. 2022, 13, 1012383. [Google Scholar] [CrossRef]
- Millán, J.; Pintó, X.; Muñoz, A.; Zúñiga, M.; Rubiés-Prat, J.; Pallardo, L.F.; Masana, L.; Mangas, A.; Hernández-Mijares, A.; González-Santos, P.; et al. Lipoprotein Ratios: Physiological Significance and Clinical Usefulness in Cardiovascular Prevention. Vasc. Health Risk Manag. 2009, 5, 757–765. [Google Scholar]
- Zeitouni, M.; Sabouret, P.; Kerneis, M.; Silvain, J.; Collet, J.-P.; Bruckert, E.; Montalescot, G. 2019 ESC/EAS Guidelines for Management of Dyslipidaemia: Strengths and Limitations. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, 324–333. [Google Scholar] [CrossRef]
- González-González, J.G.; Violante-Cumpa, J.R.; Zambrano-Lucio, M.; Burciaga-Jimenez, E.; Castillo-Morales, P.L.; Garcia-Campa, M.; Solis, R.C.; González-Colmenero, A.D.; Rodríguez-Gutiérrez, R. HOMA-IR as a Predictor of Health Outcomes in Patients with Metabolic Risk Factors: A Systematic Review and Meta-Analysis. High Blood Press. Cardiovasc. Prev. 2022, 29, 547–564. [Google Scholar] [CrossRef]
- Scott, D.A.; Ponir, C.; Shapiro, M.D.; Chevli, P.A. Associations between Insulin Resistance Indices and Subclinical Atherosclerosis: A Contemporary Review. Am. J. Prev. Cardiol. 2024, 18, 100676. [Google Scholar] [CrossRef]
- Armstrong, A.C.; Gidding, S.; Gjesdal, O.; Wu, C.; Bluemke, D.A.; Lima, J.A.C. LV Mass Assessed by Echocardiography and CMR, Cardiovascular Outcomes, and Medical Practice. JACC Cardiovasc. Imaging 2012, 5, 837–848. [Google Scholar] [CrossRef]

| n Sample = 55 | |
|---|---|
| Males | 29.00 (52.70) |
| Females | 26.00 (47.30) |
| Age | 52.00± 12.00 |
| BMI (kg/m2) | 27.30 ± 4.70 |
| Neck circumference (cm) | 36.00 ± 3.81 |
| Waist circumference (cm) | 87.00 ± 12.00 |
| Abdomen circumference (cm) | 95.00 ± 10.00 |
| Hip circumference (cm) | 101.00 ± 8.00 |
| WHR | 0.86 ± 0.10 |
| Left arm circumference (cm) | 31.10 ± 3.60 |
| Left middle thigh circumference (cm) | 53.10 ± 5.40 |
| Thigh left root circumference (cm) | 60.00 ± 9.00 |
| Wrist circumference (cm) | 18.13 ± 8.78 |
| Bicipital Fold (mm) | 11.00 ± 5.90 |
| Tricipital Fold (mm) | 18.00 ± 8.00 |
| Subscapular fold (mm) | 20.00 ± 8.00 |
| Suprailiac fold (mm) | 13.51 ± 6.20 |
| Dislipidemia (%) | 5.45 |
| Anti-hypertensive Drugs (%) | 36.36 |
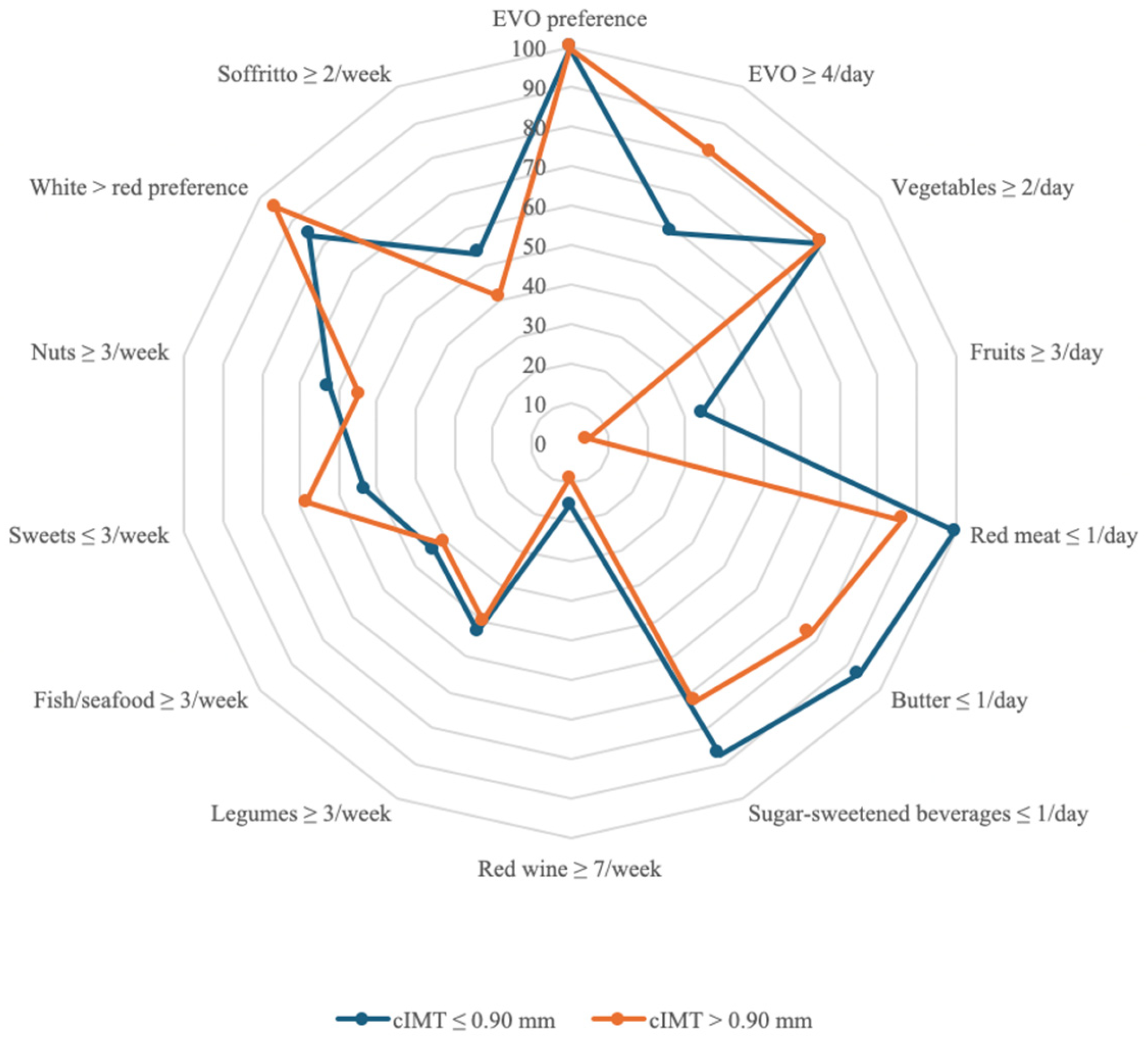
| cIMT ≤ 0.90 mm (n = 32) | cIMT > 0.90 mm (n = 23) | |
|---|---|---|
| EVO preference | 32 (100.00) | 22 (100.00) |
| EVO ≥ 4/day | 19 (59.40) | 18 (81.80) |
| Vegetables ≥ 2/day | 26 (81.25) | 18 (81.80) |
| Fruits ≥ 3/day | 11 (34.40) | 1 (4.50) |
| Red meat ≤ 1/day | 32 (100.00) | 19 (86.40) |
| Butter ≤ 1/day | 30 (93.75) | 17 (77.30) |
| Sugar-sweetened beverages ≤ 1/day | 28 (87.50) | 16 (72.70) |
| Red wine ≥ 7/week | 5 (15.60) | 2 (9.10) |
| Legumes ≥ 3/week | 17 (53.10) | 11 (50.00) |
| Fish/seafood ≥ 3/week | 14 (43.75) | 9 (40.90) |
| Sweets ≤ 3/week | 17 (53.10) | 15 (68.20) |
| Nuts ≥ 3/week | 20 (62.50) | 12 (54.50) |
| White > red preference | 27 (84.40) | 21 (95.40) |
| Soffritto ≥ 2/week | 17 (53.10) | 9 (40.90) |
| MEDAS Score | 9.25 ± 2.01 | 8.63 ± 1.74 |
| Low Adherence | 1 | 0 |
| Medium Adherence | 15 | 15 |
| High Adherence | 16 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frank, G.; Pala, B.; Gualtieri, P.; Tocci, G.; La Placa, G.; Di Renzo, L. Adherence to Mediterranean Diet and Implications for Cardiovascular Risk Prevention. Nutrients 2025, 17, 1991. https://doi.org/10.3390/nu17121991
Frank G, Pala B, Gualtieri P, Tocci G, La Placa G, Di Renzo L. Adherence to Mediterranean Diet and Implications for Cardiovascular Risk Prevention. Nutrients. 2025; 17(12):1991. https://doi.org/10.3390/nu17121991
Chicago/Turabian StyleFrank, Giulia, Barbara Pala, Paola Gualtieri, Giuliano Tocci, Giada La Placa, and Laura Di Renzo. 2025. "Adherence to Mediterranean Diet and Implications for Cardiovascular Risk Prevention" Nutrients 17, no. 12: 1991. https://doi.org/10.3390/nu17121991
APA StyleFrank, G., Pala, B., Gualtieri, P., Tocci, G., La Placa, G., & Di Renzo, L. (2025). Adherence to Mediterranean Diet and Implications for Cardiovascular Risk Prevention. Nutrients, 17(12), 1991. https://doi.org/10.3390/nu17121991