

What People Want: Exercise and Personalized Intervention as Preferred Strategies to Improve Well-Being and Prevent Chronic Diseases

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Lifestyle Assessment
- Physical activity (weekly physical activity volume) [21], using the following formulas to assess the moderate-intensity physical activity volume (in MET·minutes/week):where BW denotes brisk walking activity, which was estimated at approximately 3.3 METs/minute; m(BW) stands for the number of minutes/day of brisk walking performed in a number d(BW) of days/week; analogously, M refers to other moderate-intensity activities, which were estimated at approximately 4.0 METs/minute; and m(M) is the number of minutes/day of other moderate-intensity activities performed in a number d(M) of days/week. The vigorous-intensity physical activity volume (in MET·minutes/week) was derived using the following:moderate-intensity = 3.3 × m(BW) × d(BW) + 4.0 × m(M) × d(M),where V stands for vigorous-intensity activities, estimated at approximately 8.0 METs/minute, and m(V) is the number of minutes/day of vigorous-intensity activities performed in a number d(V) of days/week. Finally, the total weekly physical activity volume (in MET·minutes/week) was derived by the sum of the two scores (1) and (2):vigorous-intensity = 8.0 × m(V) × d(V),total volume = moderate-intensity + vigorous-intensity.
- Perception of somatic symptoms (short 4SQ), fatigue, and stress were guessed using a self-administered questionnaire [17,18], providing ordinal self-rated Likert scales from 0 (“very good”) to 10 (“very bad”) for each measure. Short 4SQ considers four somatic symptoms; thus, the total score, equal to the sum of the 0–10 scores on the single somatic symptom scales, ranges from 0 to 40.
- Smoking behavior: all subjects who reported having never smoked or had stopped smoking for more than one year were considered non-smokers.
2.2. Statistics
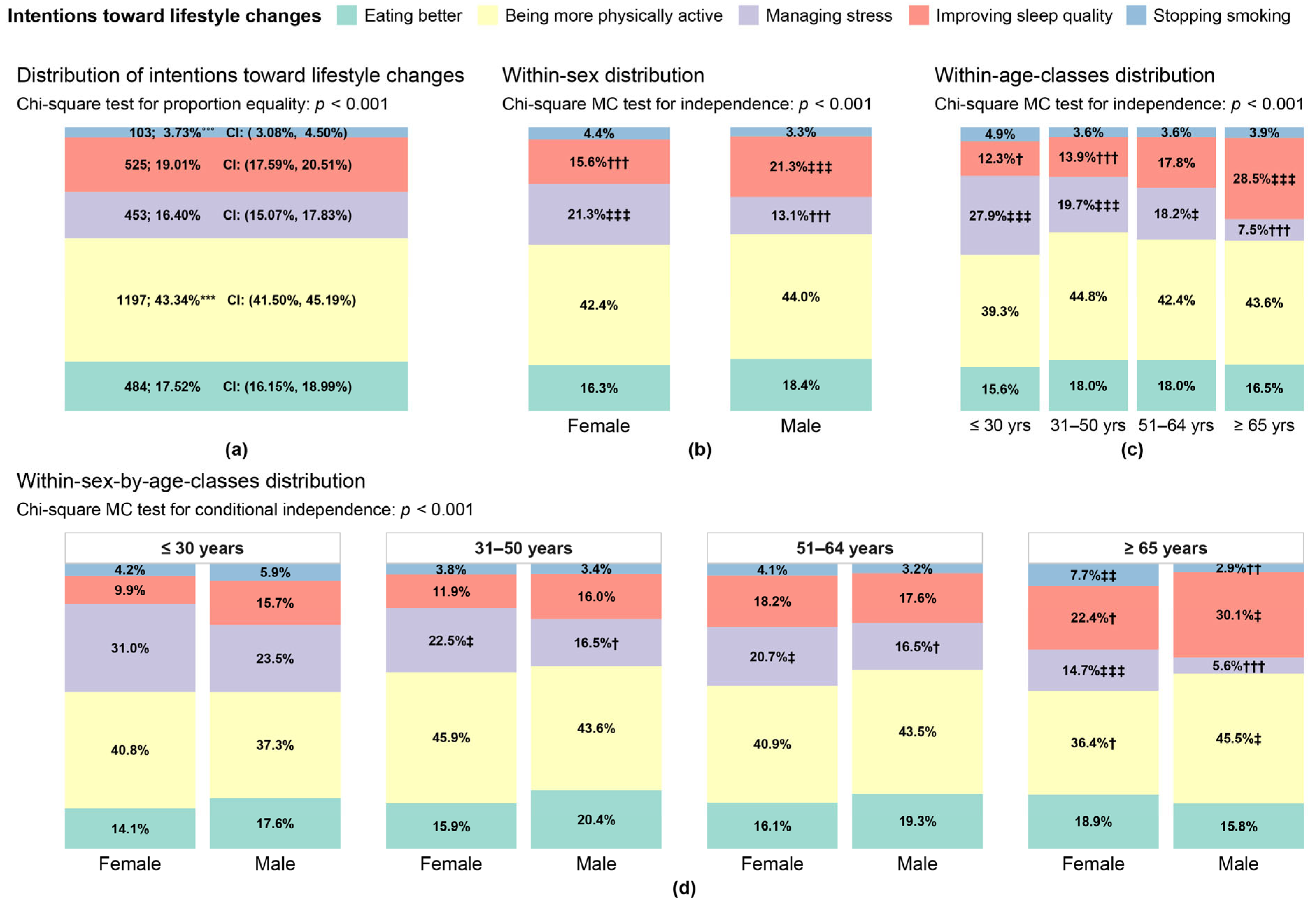
2.2.1. Subjects’ Intentions Toward Lifestyle Changes
- Considering the (marginal) distribution of the response items, the Chi-square test for equal proportions and Z-tests for pairwise comparisons (with Bonferroni p-value adjustments) were performed to detect the most prevalent response selected by the respondents;
- Regarding the joint distribution of the response items with sex, the Chi-square MC test for distributional independence was performed along with Z-tests to discover significant associations between sex and subjects’ intentions toward lifestyle changes;
- The same procedure in point b was applied to the joint distribution of the response items with age classes to discover significant associations between age classes and subjects’ intentions toward lifestyle changes;
- Finally, considering the conditional distribution of the response items with sex within age classes, the Chi-square MC test for independence of the response items and sex conditioned on age classes was performed along with Z-tests to discover significant associations between sex and subjects’ intentions toward lifestyle changes for each age class.
2.2.2. Target Actions to Improve Lifestyles and Willingness to Invest Economically in Them
2.2.3. Profiling of Subjects’ Typologies Through Classification Trees
- Manifesting a specific intention toward lifestyle changes;
- Choosing at least one target action to improve lifestyles rather than indicating no actions;
- Selecting the two most popular target actions resulted from the survey.
- Pre-processing: before building the CTs, the goodness of the predictors was assessed in order to discard from the CT construction variables with too low heterogeneity on the subjects (in the extreme case, there would be one single category common to all the subjects) or too high heterogeneity on the subjects (in the extreme case, there would be one single distinct category for each subject);
- Pruning: During the preliminary stage, the CTs were built as wide as possible on the full dataset, with the predictors designated by pre-processing to obtain the largest number of combinations among predictor categories that explained the observed subjects’ class memberships. Then, by the procedure explained in Appendix A, we reduced the CT size and found the best-pruned subtree for each CT to obtain the most important predictors along with their category combinations;
- CT validation: We appraised the performance of the best-pruned subtrees (from here on, more simply indicated as CTs) and the validity of the CT predictors selected by pruning (step 2) from two different perspectives: the CT description quality, which was assessed on the full dataset by also comparing it with the results of a random classifier through a permutation test, and the prediction capability of the selected CT predictors, which was assessed through a bagging procedure implemented by randomly generated training and test sets (see Appendix A) [20]. Both evaluations were carried out by computing the following validation measures based on comparing the subjects’ observed class memberships (i.e., a priori classification) with the predicted ones (i.e., predicted classification) [19]: accuracy (Acc), which gives the total percentage of subjects correctly classified by the CT; sensitivity (Sens), or also the true positive rate, which gives the percentage of subjects with the “positive” event that the CT correctly detects; specificity (Spec), or also the true negative rate, which gives the percentage of subjects with the “negative” event (i.e., the complementary of the “positive” event) that the CT correctly detects; the positive predictive value (PPV), or also precision, which gives the proportion of subjects indicated by the CT as having the positive event that are actually a true positive; and the negative predictive value (NPV), which gives the proportion of subjects indicated by the CT as having negative events that are actually true negatives. We also considered the following two additional measures that are useful for imbalanced data, because they limit the optimistic evaluation of CTs based on accuracy and, at the same time, give importance both to the true positive and true negative rate: balanced accuracy (BalAcc), which is the arithmetic mean of sensitivity and specificity, and the adjusted F-measure (AGF), which is a modification of the F-measures (among which there is F1) introduced to overcome some of their limitations [24].
3. Results
3.1. Subjects’ Intentions Toward Lifestyle Changes
3.2. Target Actions to Improve Lifestyles and Subjects’ Willingness to Invest Economically in Them
3.3. Subjects’ Typologies Profiled Through Classification Trees
3.3.1. Classification Tree for Subjects’ Intentions Toward Lifestyle Changes
- Among the subjects declaring to perceive a high quality of sleep (7–10, left branch), those who are non-smokers and with a low–medium level of perceived stress (0–3, 4–6) have a higher probability (estimated at 0.523) of desiring to be more physically active than the other intentions. The subjects also declaring a high level of perceived stress (7–10) and being a little physically active (total METs < 600) have a higher probability (estimated at 0.578) of desiring to be more physically active. However, if they are already physically active (total METs ≥ 600), they are more likely to prefer to focus on managing stress (with a probability estimated at 0.550). Perceived stress plays an important role in the case of smokers as well. If these subjects perceive a medium–high stress level (4–6, 7–10), they are more likely to desire to be more physically active (with a probability estimated at 0.465), while if their perceived level of stress is low (0–3), they are more likely to intend to quit smoking (with a probability estimated at 0.441);
- Among the subjects declaring to perceive a low–medium quality of sleep (0–3, 4–6, right branch), the total MET physical activity volume results in the unique most important predictor, subjects who are little physically active (total METs < 600), are more likely to desire to be more physically active (with a probability estimated at 0.512). In contrast, those already physically active (total METs ≥ 600) have a higher probability (estimated at 0.397) of desiring to improve sleep quality.
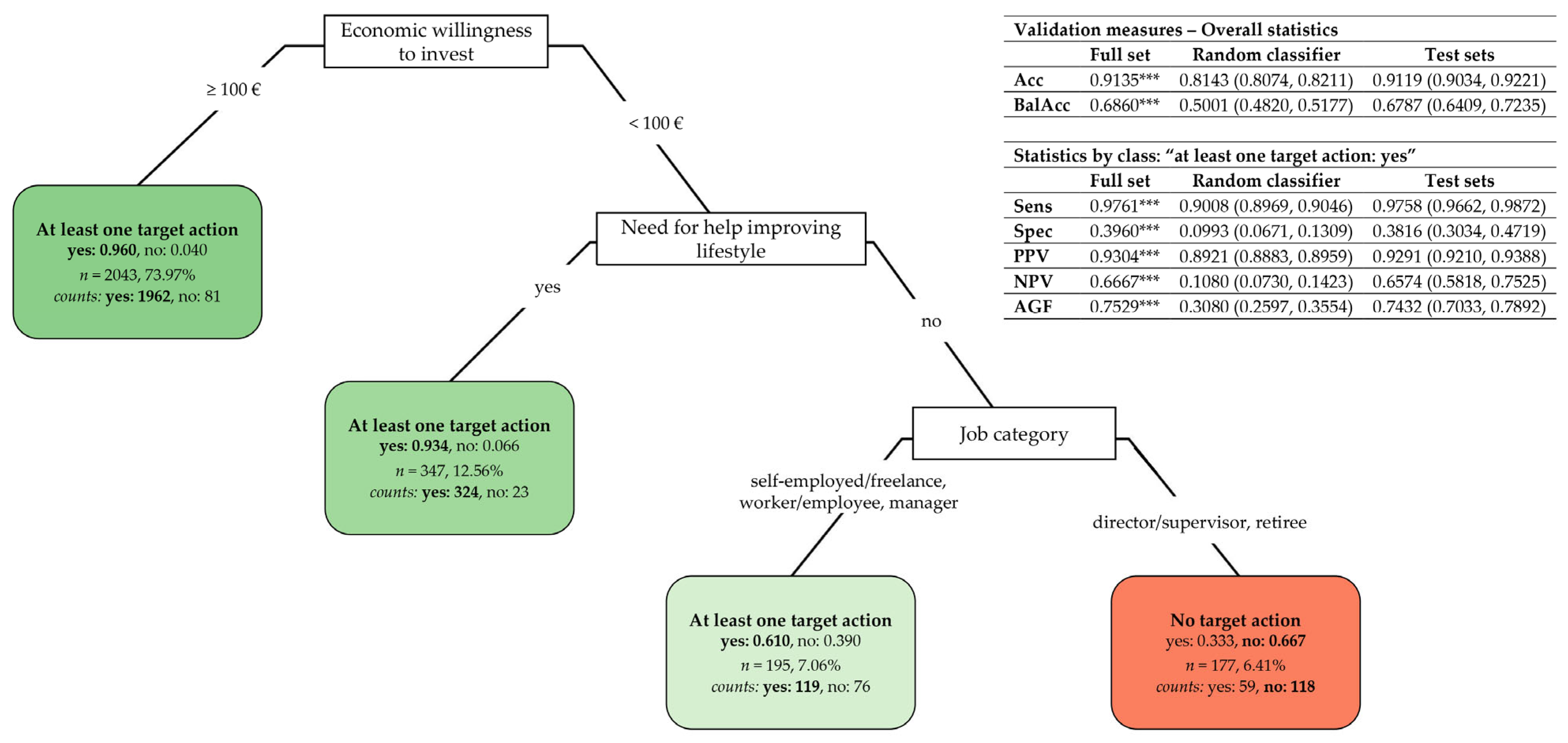
3.3.2. Classification Tree of “At Least One Target Action” Against “No Action”
- Subjects willing to invest EUR 100 or more (left branch) have a very high probability (estimated at 0.960) of choosing at least one target action;
- Among the subjects willing to invest less than EUR 100 (right branch), those declaring they need help in improving their lifestyle have a higher probability (estimated at 0.934) of choosing at least one action. Otherwise, job category becomes an important predictor: directors/supervisors and retirees are more likely to choose no action (with a probability estimated at 0.667), while other job categories are associated with a higher probability (estimated at 0.610) of selecting at least one action.
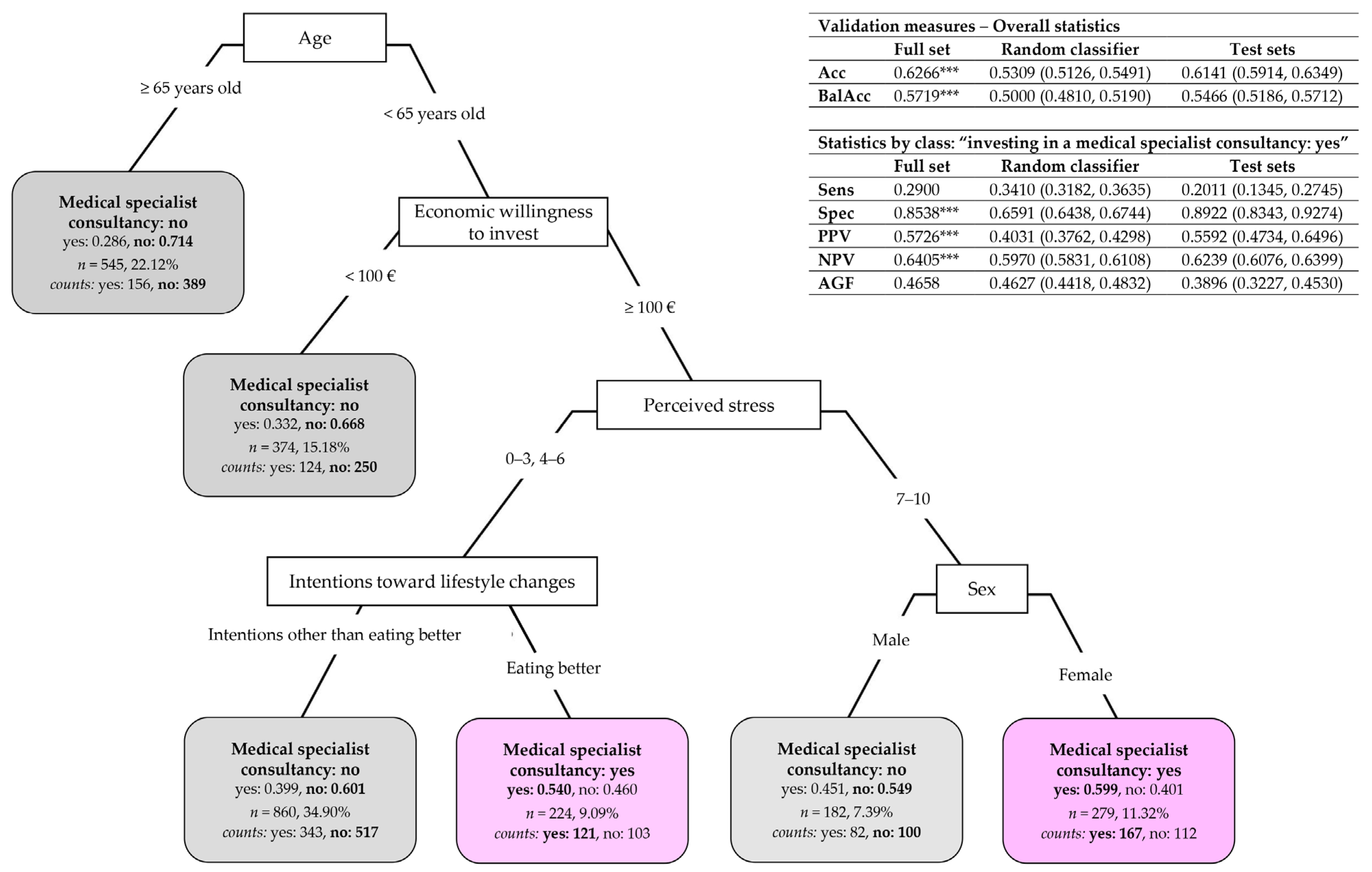
3.3.3. Classification Tree of Target Action “Having a Medical Specialist Consultancy”
- Subjects over 65 (left branch) have a very high probability (estimated at 0.714) of not choosing to have a medical specialist consultant;
- Among the subjects under 65 (right branch), those declaring they are willing to invest less than EUR 100 are more likely to not be interested in having a medical specialist consultant (with a probability estimated at 0.668). Otherwise, perceived stress plays an important role in subjects willing to invest EUR 100 or more. In particular, on the one hand, if subjects have a low–medium level of perceived stress (0–3, 4–6) and intend to eat better, then they are more likely to invest in a medical specialist consultant (with a probability estimated at 0.540); otherwise, if they have intentions other than eating better, they are more likely to be uninterested in having a medical specialist consultant (with a probability estimated at 0.601). On the other hand, if subjects have a high level of perceived stress (7–10) and are females, they are more likely to invest in a medical specialist consultant (with a probability estimated at 0.599). In contrast, males have a higher probability (estimated at 0.549) of not investing in a medical specialist consultant.
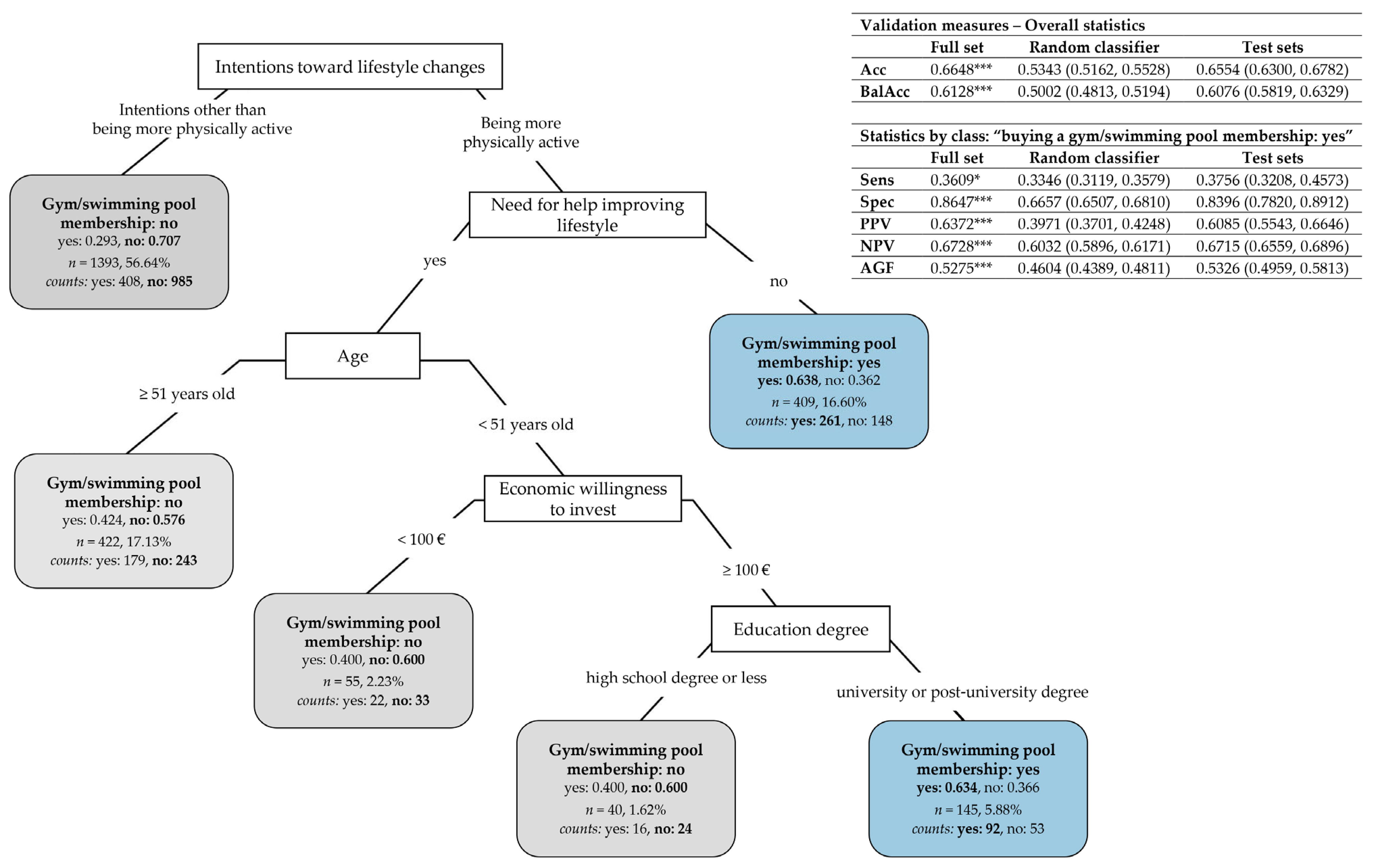
3.3.4. Classification Tree of Target Action “Buying a Gym/Swimming Pool Membership”
- Subjects who have intentions other than becoming more physically active (left branch) have a very high probability (estimated at 0.707) of not investing in a gym/swimming pool membership;
- Among the subjects who intend to be more physically active (right branch), those declaring they need no help in improving their lifestyle are more likely to buy a gym/swimming pool membership (with an estimated probability of 0.638). Otherwise, the other three predictors become important among subjects needing help in improving their lifestyle. In particular, subjects over 51 are more likely not to invest in a gym/swimming pool membership (with an estimated probability of 0.576). On the contrary, in subjects under 51, this investment depends, above all, on their economic willingness, so they are more likely to not buy a gym/swimming pool membership if their willing amount of investment is less than EUR 100 (with a probability estimated at 0.600). In the case of subjects willing to invest more than EUR 100, their choice for buying, or not, a gym/swimming pool membership depends on their education degree: if they are graduates or postgraduates, they are more inclined to invest in a gym/swimming pool membership (with a probability estimated at 0.634); otherwise, they are not (with an estimated probability of 0.600).
4. Discussion
- The perceived quality of sleep, the total volume of physical activity, smoking habits, and perceived stress resulted in the most important predictors that might explain subjects’ intentions of being more physically active (Figure 3);
- The economic willingness to invest, the need, or not, for help in improving their lifestyle, and job category are the most important selected predictors that might explain subjects’ willingness to invest in at least one target action (Figure 4);
- Age, the economic willingness to invest, perceived stress, the intention to eat better, and sex are the most important predictors that might explain subjects’ willingness to invest in a medical specialist consultant (Figure 5);
- The intention to be more physically active, the need, or not, for help in improving their lifestyle, age, the economic willingness to invest, and education degree are the most important predictors that might explain subjects’ willingness to invest in a gym/swimming pool membership (Figure 6).
- Subjects characterized by a higher probability of desiring to become more physically active (Figure 3) are those who perceive a low–medium level of sleep quality (0–3, 4–6) and do not meet the WHO’s recommended dose of aerobic exercise (total METs < 600); or have a very positive perception of sleep quality (7–10) but are smokers with a medium–high level of perceived stress (4–6, 7–10); or are non-smokers with a low–medium level of perceived stress (0–3, 4–6); or are non-smokers with high-stress perception (7–10) not meeting the WHO’s recommended dose of aerobic exercise (total METs < 600);
- Subjects characterized by a higher probability of being willing to invest in at least one target action to improve their lifestyle (Figure 4) are those who indicate a willingness to invest more than EUR 100; or among those willing to invest less than EUR 100 are those needing help to improve their lifestyle; or are those needing no help and being employed in specific job categories (i.e., self-employed/freelancers, workers/employees, and managers);
- Subjects characterized by a higher probability of willing to invest in a medical specialist consultant for receiving a tailored prescription of a lifestyle program (Figure 5) are those under 65 and willing to invest more than EUR 100, with a low–medium level of perceived stress (0–3, 4–6) and the desire to have healthier nutrition; or are women under 65 that are willing to invest more than EUR 100 and who have a high level of perceived stress (7–10);
- Subjects characterized by a higher probability of buying a gym/swimming pool membership (Figure 6) are those who desire to become more physically active and declare no need for help in improving their lifestyle; or, among the subjects needing help, those under 51 declaring to be willing to invest more than EUR 100 and who are graduates or postgraduates.
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Pre-processing: To assess the goodness of the predictors, we computed two indices for each: (A) a “frequency ratio”, i.e., the ratio between the frequency of the most prevalent category over the second most prevalent category. Predictors with such a ratio above the cutoff of 95/5 were discarded from the CT construction, because they were considered to be of too low heterogeneity on the subjects; (B) a “percentage of unique categories”, i.e., the percentage of distinct categories out of the total number (N = 2762) of subjects. Predictors with such a percentage above the cutoff of 10 were discarded from the CT construction, because they were considered to be of too high heterogeneity in the subjects.
- Pruning: During the preliminary stage, the CTs were built as wide as possible on the full dataset, with the so-called complexity parameter set to 0 [19] to obtain the largest number of combinations among predictor categories that explained the observed subjects’ class memberships. In order to avoid, however, building CTs with too huge a dimensionality, the minimum number of subjects that had to exist in a CT node for a new split to be conducted was set to 30, and the minimum number of subjects in each CT leaf (i.e., a terminal CT node) was set to 10. Then, we assessed the best value for the complexity parameter through a 10-fold cross-validation procedure along with the “1 standard error rule” [19,20] to find the best-pruned subtree for each CT.
- CT validation: We carried out a bagging procedure [20] to assess the performance of the best-pruned subtrees derived from the above procedure (from here on, more simply indicated as CTs) from the perspective of the prediction capability of the selected CT predictors. To apply bagging, which stands for “bootstrap aggregation”, we first randomly split the full dataset into a training set with 70% of the subjects and a test set with 30% of the subjects. We applied a stratified random sampling scheme to ensure that all the categories of the CT response variables were present in the training and test sets (approximately in the same proportions as the full dataset). Second, by the bagging approach, we generated B = 200 bootstrap samples of the training set, and a given CT was trained on them to obtain 200 bagged CTs. Then, for a given subject (in the training set or test set), 200 different predictions of his/her class membership on the CT response variable were available so that, by the principle of the majority vote [20], his/her unique predicted class membership was given as the most commonly predicted class among the 200 predictions. This bagging procedure was repeated 100 times from the random generation of training and test sets to predicting each subject’s class membership. To evaluate the CT performance in terms of both description and prediction capabilities, we computed the following validation measures [19]: accuracy (Acc), sensitivity (Sens), specificity (Spec), positive predictive value (PPV, also said precision), negative predictive value (NPV), balanced accuracy (BalAcc), and the AGF measure [24] on both the full dataset and the 100 training and test sets. In the latter case, we provided the mean values for each measure computed over the 100 repetitions and 95% confidence intervals built with the percentile method. In particular, the final best-pruned subtree derived from the application of the “1 standard error rule” in step 2 was selected as the one with the highest mean value of balanced accuracy significantly greater than 0.5 at the 0.05 significance level, as assessed through the 95% confidence intervals built on the test sets. The subtrees thus detected for each case, a, b, and c, in Section 2.2.3 were regarded as the final selected CTs to keep in the analysis. Moreover, in the multi-class classification problem of the subjects’ intentions toward lifestyle changes, balanced accuracy and AGF were computed as overall validation measures through the macro approach, i.e., by calculating the unweighted arithmetic means of balanced accuracy and AGF by class measures. Considering the nature of the considered predictors, essentially socio-demographic and behavioral variables, we considered acceptable values of AGF significantly greater than 0.5 (as assessed through the 95% confidence intervals built on the test sets). As a final assessment performed on the full dataset, we compared the performance of the final CTs with random classifiers built by randomly generating K labels for the classes of the CT response variables with probabilities equal to the proportions in the data. Such labels were regarded as randomly predicted classes to be compared with the true classes in the a priori classifications. To this end, the K labels of each random classifier were randomly permuted 10,000 times, and the above validation measures were computed using the true classes as references. The means of the validation measures and 95% confidence intervals (with the percentile method) were then computed to summarize the random classifier performance on the 10,000 random permutations. Finally, to compare the performance of a specific CT with its counterpart random classifier, a permutation test was applied for each validation measure, , in order to verify the null hypothesis of superior performance of the random classifier RC: against the alternative of superior performance of the final CT: .
Appendix B
Appendix B.1. Preliminary Data Inspection

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Classes (In Years Old) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ≤30 Years | 31–50 Years | 51–64 Years | ≥65 Years | Total | ||||||
| Variables | N | % | N | % | N | % | N | % | N | % |
| Sex ††† | ||||||||||
| Female | 71 | 58.20 *** | 453 | 52.74 *** | 440 | 40.40 | 143 | 20.66 *** | 1107 | 40.08 |
| Male | 51 | 41.80 *** | 406 | 47.26 *** | 649 | 59.60 | 549 | 79.34 *** | 1655 | 59.92 |
| Total | 122 | 100.00 | 859 | 100.00 | 1089 | 100.00 | 692 | 100.00 | 2762 | 100.00 |
| Education degree ††† | ||||||||||
| Primary/middle school | 0 | 0.00 | 4 | 0.47 *** | 23 | 2.11 | 22 | 3.18 *** | 49 | 1.77 |
| High school | 5 | 4.10 *** | 175 | 20.37 *** | 442 | 40.59 * | 430 | 62.14 *** | 1052 | 38.09 |
| University degree | 65 | 53.28 * | 470 | 54.71 *** | 508 | 46.65 | 209 | 30.20 *** | 1252 | 45.33 |
| Post-university degree | 52 | 42.62 *** | 210 | 24.45 *** | 116 | 10.65 *** | 31 | 4.48 *** | 409 | 14.81 |
| Total | 122 | 100.00 | 859 | 100.00 | 1089 | 100.00 | 692 | 100.00 | 2762 | 100.00 |
| Job category ††† | ||||||||||
| Self-employed/freelance | 2 | 1.64 | 14 | 1.63 * | 37 | 3.40 ** | 14 | 2.02 | 67 | 2.43 |
| Worker/employee | 103 | 84.42 *** | 335 | 39.00 *** | 248 | 22.77 ** | 15 | 2.17 *** | 701 | 25.38 |
| Manager | 12 | 9.84 *** | 343 | 39.93 *** | 403 | 37.01 *** | 24 | 3.47 *** | 782 | 28.31 |
| Director/supervisor | 5 | 4.10 *** | 167 | 19.44 | 345 | 31.68 *** | 41 | 5.92 *** | 558 | 20.20 |
| Retiree | 0 | 0.00 *** | 0 | 0.00 *** | 56 | 5.14 *** | 598 | 86.42 *** | 654 | 23.68 |
| Total | 122 | 100.00 | 859 | 100.00 | 1089 | 100.00 | 692 | 100.00 | 2762 | 100.00 |
| Smoking ††† | ||||||||||
| No | 93 | 76.23 *** | 715 | 83.24 *** | 963 | 88.43 | 636 | 91.91 *** | 2407 | 87.15 |
| Yes | 29 | 23.77 *** | 144 | 16.76 *** | 126 | 11.57 | 56 | 8.09 *** | 355 | 12.85 |
| Total | 122 | 100.00 | 859 | 100.00 | 1089 | 100.00 | 692 | 100.00 | 2762 | 100.00 |
| Need for help in improving lifestyle | ||||||||||
| No | 55 | 45.08 | 393 | 45.75 | 496 | 45.55 | 327 | 47.25 | 1271 | 46.02 |
| Yes | 67 | 54.92 | 466 | 54.25 | 593 | 54.45 | 365 | 52.75 | 1491 | 53.98 |
| Total | 122 | 100.00 | 859 | 100.00 | 1089 | 100.00 | 692 | 100.00 | 2762 | 100.00 |
| Female | Male | Total | ||||
|---|---|---|---|---|---|---|
| Variables | N | % | N | % | N | % |
| Age in class (years old) ††† | ||||||
| ≤30 years | 71 | 6.41 *** | 51 | 3.08 *** | 122 | 4.42 |
| 31–50 years | 453 | 40.92 *** | 406 | 24.53 *** | 859 | 31.10 |
| 51–64 years | 440 | 39.75 | 649 | 39.21 | 1089 | 39.43 |
| ≥65 years | 143 | 12.92 *** | 549 | 33.17 *** | 692 | 25.05 |
| Total | 1107 | 100.00 | 1655 | 100.00 | 2762 | 100.00 |
| Education degree ††† | ||||||
| Primary/middle school | 23 | 2.08 | 26 | 1.57 | 49 | 1.77 |
| High school | 394 | 35.59 * | 658 | 39.76 * | 1052 | 38.09 |
| University degree | 489 | 44.17 | 763 | 46.10 | 1252 | 45.33 |
| Post-university degree | 201 | 18.16 *** | 208 | 12.57 *** | 409 | 14.81 |
| Total | 1107 | 100.00 | 1655 | 100.00 | 2762 | 100.00 |
| Job category ††† | ||||||
| Self-employed/freelance | 31 | 2.80 | 36 | 2.18 | 67 | 2.43 |
| Worker/employee | 453 | 40.92 *** | 248 | 14.98 *** | 701 | 25.38 |
| Manager | 308 | 27.82 | 474 | 28.64 | 782 | 28.31 |
| Director/supervisor | 154 | 13.91 *** | 404 | 24.41 *** | 558 | 20.20 |
| Retiree | 161 | 14.55 *** | 493 | 29.79 *** | 654 | 23.68 |
| Total | 1107 | 100.00 | 1655 | 100.00 | 2762 | 100.00 |
| Smoking †† | ||||||
| No | 942 | 85.09 ** | 1465 | 88.52 ** | 2407 | 87.15 |
| Yes | 165 | 14.91 ** | 190 | 11.48 ** | 355 | 12.85 |
| Total | 1107 | 100.00 | 1655 | 100.00 | 2762 | 100.00 |
| Need for help in improving lifestyle ††† | ||||||
| No | 456 | 41.19 *** | 815 | 49.24 *** | 1271 | 46.02 |
| Yes | 651 | 58.81 *** | 840 | 50.76 *** | 1491 | 53.98 |
| Total | 1107 | 100.00 | 1655 | 100.00 | 2762 | 100.00 |
| Age Classes (In Years Old) | |||||
|---|---|---|---|---|---|
| Variables | ≤30 Years | 31–50 Years | 51–64 Years | ≥65 Years | Total |
| Anthropometrics | |||||
| Weight (kg) ***,††† | 62.50 ± 8.50 | 69.00 ± 11.00 | 74.00 ± 10.00 | 74.5 ± 8.00 | 72.00 ± 10.00 |
| Height (cm) * | 172.00 ± 8.00 | 171.00 ± 7.00 | 173.00 ± 6.00 | 172.50 ± 5.50 | 172.00 ± 6.00 |
| Waist circumference (cm) ***,††† | 76.50 ± 10.50 | 84.00 ± 11.00 | 90.00 ± 9.00 | 96.00 ± 7.00 | 90.00 ± 10.00 |
| Body Mass Index—BMI (kg/m2) ***,††† | 21.87 ± 1.89 | 23.33 ± 2.14 | 24.14 ± 2.10 | 24.82 ± 1.93 | 24.02 ± 2.17 |
| Lifestyle variables | |||||
| Hours/night of sleep 2 | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 |
| Total METs (minutes/week) **,††† | 1170.85 ± 770.95 | 777.00 ± 610.80 | 975.00 ± 645.00 | 850.50 ± 553.50 | 882.50 ± 642.50 |
| AHA diet score | 2.00 ± 1.00 | 2.00 ± 1.00 | 2.00 ± 1.00 | 2.00 ± 1.00 | 2.00 ± 1.00 |
| Perceived somatic symptom scales | |||||
| Short 4SQ ***,††† | 9.00 ± 6.00 | 5.00 ± 5.00 | 4.00 ± 4.00 | 2.00 ± 2.00 | 4.00 ± 4.00 |
| Fatigue ***,††† | 6.00 ± 2.00 | 5.00 ± 2.00 | 3.00 ± 2.00 | 2.00 ± 2.00 | 3.00 ± 2.00 |
| Stress ***,††† | 6.00 ± 2.00 | 5.00 ± 2.00 | 4.00 ± 2.00 | 1.00 ± 1.00 | 3.00 ± 2.00 |
| Perceived quality scales | |||||
| Sleep | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 |
| Health | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 |
| Job performance ***,††† | 8.00 ± 1.00 | 8.00 ± 1.00 | 8.00 ± 1.00 | 5.00 ± 5.00 | 8.00 ± 1.00 |
| Variables | Female | Male | Total |
|---|---|---|---|
| Anthropometrics | |||
| Weight (kg) ***,††† | 60.00 ± 6.00 | 78.00 ± 7.00 | 72.00 ± 10.00 |
| Height (cm) ***,††† | 165.00 ± 5.00 | 177.00 ± 5.00 | 172.00 ± 6.00 |
| Waist circumference (cm) ***,††† | 80.00 ± 10.00 | 95.00 ± 7.00 | 90.00 ± 10.00 |
| Body Mass Index—BMI (kg/m2) ***,††† | 22.15 ± 2.08 | 24.90 ± 1.86 | 24.02 ± 2.17 |
| Lifestyle variables | |||
| Hours/night of sleep 2 | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 |
| Total METs (minutes/week) ***,†† | 786.00 ± 594.00 | 975.00 ± 655.00 | 882.50 ± 642.50 |
| AHA diet score | 2.00 ± 1.00 | 2.00 ± 1.00 | 2.00 ± 1.00 |
| Perceived somatic symptom scales | |||
| Short 4SQ ***,††† | 6.00 ± 5.00 | 3.00 ± 3.00 | 4.00 ± 4.00 |
| Fatigue ***,††† | 5.00 ± 3.00 | 3.00 ± 2.00 | 3.00 ± 2.00 |
| Stress ***,††† | 5.00 ± 3.00 | 3.00 ± 2.00 | 3.00 ± 2.00 |
| Perceived quality scales | |||
| Sleep | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 |
| Health | 7.00 ± 1.00 | 7.00 ± 1.00 | 7.00 ± 1.00 |
| Job performance | 8.00 ± 1.00 | 8.00 ± 1.00 | 8.00 ± 1.00 |
Appendix B.2. Classification Trees
| WC 2 | count | % | BMI | count | % | Hours/night of sleep | count | % |
|---|---|---|---|---|---|---|---|---|
| no risk | 1414 | 51.19% | <25 | 1721 | 62.31% | 1–5 | 376 | 13.61% |
| medium risk | 623 | 22.56% | [25, 30) | 863 | 31.25% | 6–7 | 1829 | 66.22% |
| high risk | 725 | 26.25% | ≥30 | 178 | 6.44% | 8–12 | 533 | 19.30% |
| 2762 | 100.00% | 2762 | 100.00% | missing | 24 | 0.87% | ||
| 2762 | 100.00% | |||||||
| Total METs | count | % | AHA score | count | % | Short 4SQ | count | % |
| <600 | 1042 | 37.73% | 0–1 | 574 | 20.78% | 0–3 | 1332 | 48.23% |
| ≥600 | 1720 | 62.27% | 2–3 | 1858 | 67.27% | 4–8 | 659 | 23.86% |
| 2762 | 100.00% | 4–5 | 330 | 11.95% | 9–36 | 771 | 27.91% | |
| 2762 | 100.00% | 2762 | 100.00% | |||||
| Fatigue | count | % | Stress | count | % | Sleep q | count | % |
| 0–3 | 1451 | 52.53% | 0–3 | 1424 | 51.56% | 0–3 | 251 | 9.09% |
| 4–6 | 682 | 24.69% | 4–6 | 700 | 25.34% | 4–6 | 1030 | 37.29% |
| 7–10 | 629 | 22.77% | 7–10 | 638 | 23.10% | 7–10 | 1481 | 53.62% |
| 2762 | 100.00% | 2762 | 100.00% | 2762 | 100.00% | |||
| Health q | count | % | Job perf q | count | % | |||
| 0–3 | 69 | 2.50% | 0–3 | 365 | 13.22% | |||
| 4–6 | 822 | 29.76% | 4–6 | 236 | 8.54% | |||
| 7–10 | 1871 | 67.74% | 7–10 | 2161 | 78.24% | |||
| 2762 | 100.00% | 2762 | 100.00% |
| Pre-Processing 2 | After Pruning | |||||||
|---|---|---|---|---|---|---|---|---|
| CT in Cases a and b | CT in Cases c and d | Overall Variable Importance 2 | ||||||
| Predictors | Freq Ratio | % Unique | Freq Ratio | % Unique | VI CT-a | VI CT-b | VI CT-c | VI CT-d |
| sex | 1.495 | 0.072 | 1.432 | 0.081 | 0.371 | 0.695 | 8.423 | 0 |
| age | 1.268 | 0.145 | 1.216 | 0.162 | 0.413 | 0.496 | 33.300 | 4.771 |
| educ degr | 1.190 | 0.145 | 1.246 | 0.162 | 0 | 0 | 0 | 4.061 |
| job cat | 1.116 | 0.181 | 1.085 | 0.203 | 0.397 | 8.808 | 2.778 | 0.702 |
| smoking | 6.780 | 0.072 | 6.558 | 0.081 | 15.075 | 0 | 0 | 0.631 |
| help | 1.173 | 0.072 | 1.444 | 0.081 | 0 | 44.290 | 0 | 14.626 |
| WC | 1.950 | 0.109 | 2.011 | 0.122 | 0.377 | 0 | 0 | 0 |
| BMI | 1.994 | 0.109 | 2.024 | 0.122 | 0.377 | 0 | 1.151 | 1.342 |
| h/n sleep | 3.432 | 0.109 | 3.600 | 0.122 | 0.753 | 0 | 0 | 0 |
| tot METs | 1.651 | 0.072 | 1.699 | 0.081 | 24.280 | 0 | 0 | 0.610 |
| AHA | 3.237 | 0.109 | 3.233 | 0.122 | 0.742 | 0 | 0 | 0 |
| short 4SQ | 1.728 | 0.109 | 1.589 | 0.122 | 0.472 | 0.339 | 2.433 | 0 |
| fatigue | 2.128 | 0.109 | 1.950 | 0.122 | 2.197 | 0.715 | 2.555 | 0.668 |
| stress | 2.034 | 0.109 | 1.869 | 0.122 | 17.264 | 0.725 | 14.183 | 0.677 |
| sleep q | 1.438 | 0.109 | 1.425 | 0.122 | 35.725 | 0 | 1.233 | 0 |
| health q | 2.276 | 0.109 | 2.307 | 0.122 | 1.194 | 0 | 0 | 0.777 |
| job perf q | 5.921 | 0.109 | 6.958 | 0.122 | 0.363 | 0.419 | 1.503 | 0 |
| econ inv | 1.581 | 0.145 | 2.084 | 0.162 | 0 | 43.513 | 18.808 | 2.821 |
| intentions 3 | 2.280 | 0.181 | 2.429 | 0.203 | ---- | 0 | 13.633 | 68.314 |
References
- Promoting Well-Being. Available online: https://www.who.int/activities/promoting-well-being (accessed on 29 March 2025).
- Lucini, D.; Luconi, E.; Giovanelli, L.; Marano, G.; Bernardelli, G.; Guidetti, R.; Morello, E.; Cribellati, S.; Brambilla, M.M.; Biganzoli, E.M. Assessing Lifestyle in a Large Cohort of Undergraduate Students: Significance of Stress, Exercise and Nutrition. Nutrients 2024, 16, 4339. [Google Scholar] [CrossRef] [PubMed]
- Lucini, D.; Pagani, E.; Capria, F.; Galiano, M.; Marchese, M.; Cribellati, S.; Parati, G. Age Influences on Lifestyle and Stress Perception in the Working Population. Nutrients 2023, 15, 399. [Google Scholar] [CrossRef] [PubMed]
- Kraus, W.E.; Bittner, V.; Appel, L.; Blair, S.N.; Church, T.; Després, J.P.; Franklin, B.A.; Miller, T.D.; Pate, R.R.; Taylor-Piliae, R.E.; et al. The National Physical Activity Plan: A Call to Action from the American Heart Association: A Science Advisory from the American Heart Association. Circulation 2015, 131, 1932–1940. [Google Scholar] [CrossRef]
- Writing Committee Members; Virani, S.S.; Newby, L.K.; Arnold, S.V.; Bittner, V.; Brewer, L.C.; Demeter, S.H.; Dixon, D.L.; Fearon, W.F.; Hess, B.; et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2023, 82, 833–955. [Google Scholar] [CrossRef]
- Lucini, D.; Pagani, E.; Capria, F.; Galliano, M.; Marchese, M.; Cribellati, S. Evidence of Better Psychological Profile in Working Population Meeting Current Physical Activity Recommendations. Int. J. Environ. Res. Public Health 2021, 18, 8991. [Google Scholar] [CrossRef] [PubMed]
- Health and Well-Being|European Foundation for the Improvement of Living and Working Conditions. Available online: https://www.eurofound.europa.eu/en/topic/health-and-well-being (accessed on 30 March 2025).
- European Network Workplace Health Promotion. Luxembourg Declaration on Workplace Health Promotion in the European Union 2 Luxembourg Declaration on Workplace Health Promotion; European Network Workplace Health Promotion: Vieste, Italy, 2007. [Google Scholar]
- Ottawa Charter for Health Promotion. Health Promot. Int. 1986, 1, 405. [CrossRef]
- Verra, S.E.; Benzerga, A.; Jiao, B.; Ruggeri, K. Health Promotion at Work: A Comparison of Policy and Practice Across Europe. Saf. Health Work. 2019, 10, 21–29. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Calitz, C.; Arena, R.; Baase, C.; Isaac, F.W.; Lloyd-Jones, D.; Peterson, E.D.; Pronk, N.; Sanchez, E.; Terry, P.E.; et al. Workplace Wellness Recognition for Optimizing Workplace Health a Presidential Advisory from the American Heart Association. Circulation 2015, 131, e480–e497. [Google Scholar] [CrossRef]
- Goetzel, R.Z.; Henke, R.M.; Tabrizi, M.; Pelletier, K.R.; Loeppke, R.; Ballard, D.W.; Grossmeier, J.; Anderson, D.R.; Yach, D.; Kelly, R.K.; et al. Do Workplace Health Promotion (Wellness) Programs Work? J. Occup. Environ. Med. 2014, 56, 927–934. [Google Scholar] [CrossRef]
- Song, Z.; Baicker, K. Effect of a Workplace Wellness Program on Employee Health and Economic Outcomes: A Randomized Clinical Trial. JAMA 2019, 321, 1491–1501. [Google Scholar] [CrossRef]
- Rongen, A.; Robroek, S.J.W.; Van Lenthe, F.J.; Burdorf, A. Workplace Health Promotion: A Meta-Analysis of Effectiveness. Am. J. Prev. Med. 2013, 44, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Rao, G.; Burke, L.E.; Spring, B.J.; Ewing, L.J.; Turk, M.; Lichtenstein, A.H.; Cornier, M.A.; Spence, J.D.; Coons, M. New and Emerging Weight Management Strategies for Busy Ambulatory Settings: A Scientific Statement from the American Heart Association Endorsed by the Society of Behavioral Medicine. Circulation 2011, 124, 1182–1203. [Google Scholar] [CrossRef] [PubMed]
- Hassard, J.; Muylaert, K.; Namysl, A.; Kazenas, A.; Flaspoler, E. Motivation for Employers to Carry Out Workplace Health Promotion: Literature Review; European Agency for Safety and Health at Work: Bilbao, Spain, 2012. [Google Scholar] [CrossRef]
- Lucini, D.; Zanuso, S.; Blair, S.; Pagani, M. A Simple Healthy Lifestyle Index as a Proxy of Wellness: A Proof of Concept. Acta Diabetol. 2015, 52, 81–89. [Google Scholar] [CrossRef]
- Lucini, D.; Solaro, N.; Lesma, A.; Gillet, V.B.; Pagani, M. Health Promotion in the Workplace: Assessing Stress and Lifestyle with an Intranet Tool. J. Med. Internet Res. 2011, 13, e88. [Google Scholar] [CrossRef]
- Breiman, L.; Friedman, J.H.; Olshen, R.A.; Stone, C.J. Classification and Regression Trees; Chapman & Hall/CRC: New York, NY, USA, 1993. [Google Scholar]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning: With Applications in R; Springer: New York, NY, USA, 2013. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and Setting National Goals for Cardiovascular Health Promotion and Disease Reduction: The American Heart Association’s Strategic Impact Goal through 2020 and Beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef]
- Gibbons, J.D.; Chakraborti, S. Nonparametric Statistical Inference, 5th ed.; Chapman and Hall/CRC: New York, NY, USA, 2010. [Google Scholar]
- Maratea, A.; Petrosino, A.; Manzo, M. Adjusted F-measure and kernel scaling for imbalanced data learning. Inf. Sci. 2014, 257, 331–341. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2024; Available online: https://www.r-project.org/ (accessed on 23 May 2025).
- Hothorn, T.; Hornik, K.; van de Wiel, M.A.; Zeileis, A. Implementing a class of permutation tests: The coin package. J. Stat. Softw. 2008, 28, 1–23. [Google Scholar] [CrossRef]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis. Springer: New York, NY, USA, 2016. [Google Scholar]
- Therneau, T.; Atkinson, B. rpart: Recursive Partitioning and Regression Trees; R Package Version 4.1.24. 2025. Available online: https://CRAN.R-project.org/package=rpart (accessed on 23 May 2025).
- Milborrow, S. rpart.plot: Plot “rpart” Models. An Enhanced Version of “plot.rpart”; R Package Version 3.1.2. 2024. Available online: https://CRAN.R-project.org/package=rpart.plot (accessed on 23 May 2025).
- Kuhn, M. Building predictive models in R using the caret package. J. Stat. Softw. 2008, 28, 1–26. [Google Scholar] [CrossRef]
- Correndo, A.A.; Rosso, L.H.M.; Hernandez, C.H.; Bastos, L.M.; Nieto, L.; Holzworth, D.; Ciampitti, I.A. metrica: An R package to evaluate prediction performance of regression and classification point-forecast models. J. Open Source Softw. 2022, 7, 4655. [Google Scholar] [CrossRef]
- Alfaro, E.; Gámez, M.; García, N. adabag: An R package for classification with boosting and bagging. J. Stat. Softw. 2013, 54, 1–35. [Google Scholar] [CrossRef]
- Visseren, F.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Grundy, S.M.; Pasternak, R.; Greenland, P.; Smith, S.; Fuster, V. Assessment of Cardiovascular Risk by Use of Multiple-Risk-Factor Assessment Equations: A Statement for Healthcare Professionals from the American Heart Association and the American College of Cardiology. Circulation 1999, 100, 1481–1492. [Google Scholar] [CrossRef] [PubMed]
- Heneghan, C.; Mahtani, K.R. Is It Time to End General Health Checks? BMJ Evid. Based Med. 2020, 25, 115–116. [Google Scholar] [CrossRef]
- Iacobucci, G. Fewer People Are Attending NHS Health Checks, Show Figures. BMJ 2019, 367, l6098. [Google Scholar] [CrossRef] [PubMed]
- Hoebel, J.; Starker, A.; Jordan, S.; Richter, M.; Lampert, T. Determinants of Health Check Attendance in Adults: Findings from the Cross-Sectional German Health Update (GEDA) Study. BMC Public Health 2014, 14, 913. [Google Scholar] [CrossRef]
- Chien, S.Y.; Chuang, M.C.; Chen, I.P. Why People Do Not Attend Health Screenings: Factors That Influence Willingness to Participate in Health Screenings for Chronic Diseases. Int. J. Environ. Res. Public Health 2020, 17, 3495. [Google Scholar] [CrossRef]
- Schülein, S.; Taylor, K.J.; Schriefer, D.; Blettner, M.; Klug, S.J. Participation in Preventive Health Check-Ups among 19,351 Women in Germany. Prev. Med. Rep. 2017, 6, 23. [Google Scholar] [CrossRef]
- Krogsbøll, L.T.; Jørgensen, K.J.; Gøtzsche, P.C. General Health Checks in Adults for Reducing Morbidity and Mortality from Disease. Cochrane Database Syst. Rev. 2019, 2019, CD009009. [Google Scholar] [CrossRef]
- Alageel, S.; Gulliford, M.C. Health Checks and Cardiovascular Risk Factor Values over Six Years’ Follow-up: Matched Cohort Study Using Electronic Health Records in England. PLoS Med. 2019, 16, e1002863. [Google Scholar] [CrossRef] [PubMed]
- Kherad, O.; Carneiro, A.V. General Health Check-Ups: To Check or Not to Check? A Question of Choosing Wisely. Eur. J. Intern. Med. 2023, 109, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Hashimoto, H.; Lee, J.S.; Kawakubo, K.; Mori, K.; Akabayashi, A. Distinct Impact of Education and Income on Habitual Exercise: A Cross-Sectional Analysis in a Rural City in Japan. Soc. Sci. Med. 2011, 73, 1683–1688. [Google Scholar] [CrossRef]
- Kari, J.T.; Viinikainen, J.; Böckerman, P.; Tammelin, T.H.; Pitkänen, N.; Lehtimäki, T.; Pahkala, K.; Hirvensalo, M.; Raitakari, O.T.; Pehkonen, J. Education Leads to a More Physically Active Lifestyle: Evidence Based on Mendelian Randomization. Scand. J. Med. Sci. Sports 2020, 30, 1194–1204. [Google Scholar] [CrossRef]
- Pascoe, M.C.; Hetrick, S.E.; Parker, A.G. The Impact of Stress on Students in Secondary School and Higher Education. Int. J. Adolesc. Youth 2020, 25, 104–112. [Google Scholar] [CrossRef]
- Kivimäki, M.; Pentti, J.; Ferrie, J.E.; Batty, G.D.; Nyberg, S.T.; Jokela, M.; Virtanen, M.; Alfredsson, L.; Dragano, N.; Fransson, E.I.; et al. Work Stress and Risk of Death in Men and Women with and without Cardiometabolic Disease: A Multicohort Study. Lancet Diabetes Endocrinol. 2018, 6, 705–713. [Google Scholar] [CrossRef]
- Lucini, D.; Pagani, M. Exercise Prescription to Foster Health and Well-Being: A Behavioral Approach to Transform Barriers into Opportunities. Int. J. Environ. Res. Public Health 2021, 18, 968. [Google Scholar] [CrossRef]
- Yorks, D.M.; Frothingham, C.A.; Schuenke, M.D. Effects of Group Fitness Classes on Stress and Quality of Life of Medical Students. J. Am. Osteopath. Assoc. 2017, 117, e17–e25. [Google Scholar] [CrossRef]
- McEwen, B.S.; Akil, H. Revisiting the Stress Concept: Implications for Affective Disorders. J. Neurosci. 2020, 40, 12–21. [Google Scholar] [CrossRef]
- Tari, A.R.; Walker, T.L.; Huuha, A.M.; Sando, S.B.; Wisloff, U. Neuroprotective Mechanisms of Exercise and the Importance of Fitness for Healthy Brain Ageing. Lancet 2025, 405, 1093–1118. [Google Scholar] [CrossRef]
- Stress Management: Enhance Your Well-Being by Reducing Stress and Building Resilience—Harvard Health. Available online: https://www.health.harvard.edu/mind-and-mood/stress-management-enhance-your-well-being-by-reducing-stress-and-building-resilience (accessed on 30 March 2025).
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C.; et al. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. J. Clin. Sleep Med. 2015, 11, 591–592. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO Guidelines on Physical Activity and Sedentary Behaviour for Children and Adolescents Aged 5–17 Years: Summary of the Evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef] [PubMed]
- Zapalac, K.; Miller, M.; Champagne, F.A.; Schnyer, D.M.; Baird, B. The Effects of Physical Activity on Sleep Architecture and Mood in Naturalistic Environments. Sci. Rep. 2024, 14, 5637. [Google Scholar] [CrossRef]
- Xie, W.; Lu, D.; Liu, S.; Li, J.; Li, R. The Optimal Exercise Intervention for Sleep Quality in Adults: A Systematic Review and Network Meta-Analysis. Prev. Med. 2024, 183, 107955. [Google Scholar] [CrossRef]
- Kasiak, P.; Kowalski, T.; Rębiś, K.; Klusiewicz, A.; Ładyga, M.; Sadowska, D.; Wilk, A.; Wiecha, S.; Barylski, M.; Poliwczak, A.R.; et al. Is the Ventilatory Efficiency in Endurance Athletes Different?—Findings from the NOODLE Study. J. Clin. Med. 2024, 13, 490. [Google Scholar] [CrossRef]
- Śliż, D.; Wiecha, S.; Gąsior, J.S.; Kasiak, P.S.; Ulaszewska, K.; Postuła, M.; Małek, Ł.A.; Mamcarz, A. The Influence of Nutrition and Physical Activity on Exercise Performance after Mild COVID-19 Infection in Endurance Athletes-CESAR Study. Nutrients 2022, 14, 5381. [Google Scholar] [CrossRef]

| Economic Willingness to Invest (One Choice) | ||||||
|---|---|---|---|---|---|---|
| Target Actions to Improve Lifestyles (Multiple Choices) | <100 € | 100–299.99 € | 300–499.99 € | ≥500 € | Total Number of Respondents Choosing the Action | Total Number of Respondents Not Choosing the Action |
| Buying healthier food ††† | 78 (10.85%) *** | 264 (23.22%) ** | 137 (25.56%) ** | 96 (25.95%) ** | 575 (20.82%) s.c.: 17.39% | 2187 (79.18%) |
| Having a medical specialist consultant ††† | 153 (21.28%) *** | 471 (41.41%) *** | 225 (41.98%) *** | 144 (38.92%) | 993 (35.95%) s.c.: 35.45% | 1769 (64.05%) |
| Buying a gym/swimming pool membership ††† | 162 (22.53%) *** | 421 (37.03%) | 228 (42.54%) *** | 167 (45.14%) *** | 978 (35.41%) s.c.: 40.39% | 1784 (64.59%) |
| Buying sports equipment/clothing ††† | 61 (8.48%) *** | 159 (13.98%) | 105 (19.59%) *** | 77 (20.81%) *** | 402 (14.55%) s.c.: 23.88% | 2360 (85.45%) |
| Participating in stress management training | 85 (11.82%) | 182 (16.01%) | 74 (13.81%) | 57 (15.41%) | 398 (14.41%) s.c.: 30.40% | 2364 (85.59%) |
| Performing medical tests (check-ups) ††† | 77 (10.71%) *** | 232 (20.40%) | 137 (25.56%) *** | 109 (29.46%) *** | 555 (20.09%) s.c.: 19.64% | 2207 (79.91%) |
| Participating in stop-smoking programs | 19 (2.64%) | 37 (3.25%) | 13 (2.43%) | 8 (2.16%) | 77 (2.79%) s.c.: 35.06% | 2685 (97.21%) |
| Other actions † | 81 (11.27%) *** | 84 (7.39%) * | 37 (6.90%) | 31 (8.38%) | 233 (8.44%) s.c.: 70.82% | 2529 (91.56%) |
| No action ††† | 217 (30.18%) *** | 45 (3.96%) *** | 12 (2.24%) *** | 24 (6.49%) ** | 298 (10.79%) | 2464 (89.21%) |
| Distribution of economic willingness to invest (% out of 2762 subjects) | 719 (26.03%) | 1137 (41.17%) | 536 (19.40%) | 370 (13.40%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solaro, N.; Pagani, E.; Oggionni, G.; Giovanelli, L.; Capria, F.; Galiano, M.; Marchese, M.; Cribellati, S.; Lucini, D. What People Want: Exercise and Personalized Intervention as Preferred Strategies to Improve Well-Being and Prevent Chronic Diseases. Nutrients 2025, 17, 1819. https://doi.org/10.3390/nu17111819
Solaro N, Pagani E, Oggionni G, Giovanelli L, Capria F, Galiano M, Marchese M, Cribellati S, Lucini D. What People Want: Exercise and Personalized Intervention as Preferred Strategies to Improve Well-Being and Prevent Chronic Diseases. Nutrients. 2025; 17(11):1819. https://doi.org/10.3390/nu17111819
Chicago/Turabian StyleSolaro, Nadia, Eleonora Pagani, Gianluigi Oggionni, Luca Giovanelli, Francesco Capria, Michele Galiano, Marcello Marchese, Stefano Cribellati, and Daniela Lucini. 2025. "What People Want: Exercise and Personalized Intervention as Preferred Strategies to Improve Well-Being and Prevent Chronic Diseases" Nutrients 17, no. 11: 1819. https://doi.org/10.3390/nu17111819
APA StyleSolaro, N., Pagani, E., Oggionni, G., Giovanelli, L., Capria, F., Galiano, M., Marchese, M., Cribellati, S., & Lucini, D. (2025). What People Want: Exercise and Personalized Intervention as Preferred Strategies to Improve Well-Being and Prevent Chronic Diseases. Nutrients, 17(11), 1819. https://doi.org/10.3390/nu17111819