


The Joint Association of Diet Quality and Sleep Regularity with Incident Cardiovascular Disease in the Multi-Ethnic Study of Atherosclerosis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
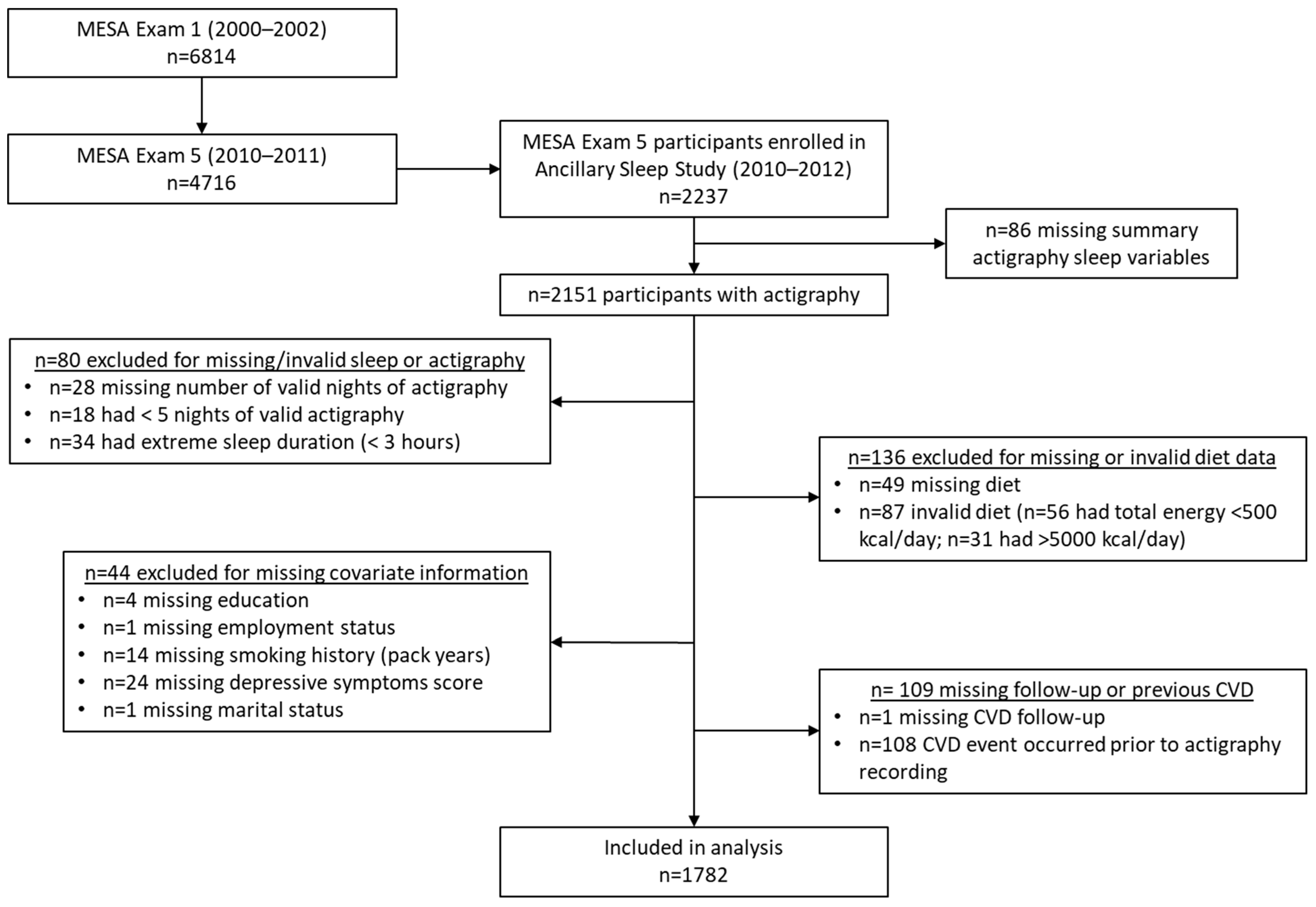
2.1. Study Population
2.2. Sleep Assessment
2.3. Diet Assessment
2.4. Ascertainment of Cardiovascular Endpoints
2.5. Assessment of Covariates
2.6. Statistics and Reproducibility
3. Results
3.1. Description of Sample
3.2. Individual Associations
3.3. Joint and Individual Associations in Comparison to a Common Reference Group
3.4. Interaction
4. Discussion
4.1. Strengths and Limitations
4.2. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lloyd-Jones, D.M.; Allen, N.B.; Anderson, C.A.; Black, T.; Brewer, L.C.; Foraker, R.E.; Grandner, M.A.; Lavretsky, H.; Perak, A.M.; Sharma, G.; et al. Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct of Cardiovascular Health: A Presidential Advisory From the American Heart Association. Circulation 2022, 146, E18–E43. [Google Scholar] [CrossRef] [PubMed]
- Morze, J.; Danielewicz, A.; Hoffmann, G.; Schwingshackl, L. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: A Second Update of a Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2020, 120, 1998–2031.e15. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.-P.; Grandner, M.A.; Brown, D.; Conroy, M.B.; Jean-Louis, G.; Coons, M.; Bhatt, D.L. Sleep Duration and Quality: Impact on Lifestyle Behaviors and Cardiometabolic Health: A Scientific Statement from the American Heart Association. Circulation 2016, 134, e367–e386. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, A.B.; Knutson, K.L.; Zee, P.C. Circadian disruption and human health. J. Clin. Invest. 2021, 131, e148286. [Google Scholar] [CrossRef] [PubMed]
- Scheer, F.A.J.L.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef]
- McMahon, D.M.; Burch, J.B.; Youngstedt, S.D.; Wirth, M.D.; Hardin, J.W.; Hurley, T.G.; Blair, S.N.; Hand, G.A.; Shook, R.P.; Drenowatz, C.; et al. Relationships between chronotype, social jetlag, sleep, obesity and blood pressure in healthy young adults. Chronobiol. Int. 2019, 36, 493–509. [Google Scholar] [CrossRef]
- Hulsegge, G.; Picavet, H.S.J.; Van Der Beek, A.J.; Verschuren, W.M.M.; Twisk, J.W.; Proper, K.I. Shift work, chronotype and the risk of cardiometabolic risk factors. Eur. J. Public Health 2019, 29, 128–134. [Google Scholar] [CrossRef]
- Sletten, T.L.; Weaver, M.D.; Foster, R.G.; Gozal, D.; Klerman, E.B.; Rajaratnam, S.M.; Roenneberg, T.; Takahashi, J.S.; Turek, F.W.; Vitiello, M.V.; et al. The importance of sleep regularity: A consensus statement of the National Sleep Foundation sleep timing and variability panel. Sleep Health 2023, 9, 801–820. [Google Scholar] [CrossRef]
- Huang, T.; Mariani, S.; Redline, S. Sleep Irregularity and Risk of Cardiovascular Events: The Multi-Ethnic Study of Atherosclerosis. J. Am. Coll. Cardiol. 2020, 75, 991–999. [Google Scholar] [CrossRef]
- Huang, T.; Redline, S. Cross-sectional and Prospective Associations of Actigraphy-Assessed Sleep Regularity with Metabolic Abnormalities: The Multi-Ethnic Study of Atherosclerosis. Diabetes Care 2019, 42, 1422–1429. [Google Scholar] [CrossRef]
- Cribb, L.; Sha, R.; Yiallourou, S.; Grima, N.A.; Cavuoto, M.; Baril, A.-A.; Pase, M.P. Sleep regularity and mortality: A prospective analysis in the UK Biobank. eLife 2023, 12, RP88359. [Google Scholar] [CrossRef] [PubMed]
- Full, K.M.; Huang, T.; Shah, N.A.; Allison, M.A.; Michos, E.D.; Duprez, D.A.; Redline, S.; Lutsey, P.L. Sleep Irregularity and Subclinical Markers of Cardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis. J. Am. Heart Assoc. 2023, 12, e027361. [Google Scholar] [CrossRef] [PubMed]
- Spruyt, K.; Molfese, D.L.; Gozal, D. Sleep Duration, Sleep Regularity, Body Weight, and Metabolic Homeostasis in School-aged Childrene352. Pediatrics 2011, 127, 345. [Google Scholar] [CrossRef]
- St-Onge, M.P.; Zuraikat, F.M. Reciprocal Roles of Sleep and Diet in Cardiovascular Health: A Review of Recent Evidence and a Potential Mechanism. Curr. Atheroscler. Rep. 2019, 21, 11. [Google Scholar] [CrossRef]
- Zuraikat, F.M.; Wood, R.A.; Barragán, R.; St-Onge, M.P. Sleep and Diet: Mounting Evidence of a Cyclical Relationship. Annu Rev Nutr. 2021, 41, 309–332. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Uemura, H.; Katsuura-Kamano, S.; Nakamoto, M.; Hiyoshi, M.; Takami, H.; Sawachika, F.; Juta, T.; Arisawa, K. Relationship of dietary factors and habits with sleep-wake regularity. Asia Pac. J. Clin. Nutr. 2013, 22, 457–465. [Google Scholar]
- Tajiri, E.; Yoshimura, E.; Hatamoto, Y.; Shiratsuchi, H.; Tanaka, S.; Shimoda, S. Acute Sleep Curtailment Increases Sweet Taste Preference, Appetite and Food Intake in Healthy Young Adults: A Randomized Crossover Trial. Behav. Sci. 2020, 10, 47. [Google Scholar] [CrossRef] [PubMed]
- Mamalaki, E.; A Anastasiou, C.; Ntanasi, E.; Tsapanou, A.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Scarmeas, N.; Yannakoulia, M. Associations between the mediterranean diet and sleep in older adults: Results from the hellenic longitudinal investigation of aging and diet study. Geriatr. Gerontol. Int. 2018, 18, 1543–1548. [Google Scholar] [CrossRef]
- Godos, J.; Ferri, R.; Caraci, F.; Cosentino, F.I.I.; Castellano, S.; Galvano, F.; Grosso, G. Adherence to the Mediterranean Diet is Associated with Better Sleep Quality in Italian Adults. Nutrients 2019, 11, 976. [Google Scholar] [CrossRef]
- Ferranti, R.; Marventano, S.; Castellano, S.; Giogianni, G.; Nolfo, F.; Rametta, S.; Matalone, M.; Mistretta, A. Sleep quality and duration is related with diet and obesity in young adolescent living in Sicily, Southern Italy. Sleep. Sci. 2016, 9, 117–122. [Google Scholar] [CrossRef]
- Potts, K.S.; Wallace, M.E.; Gustat, J.; Ley, S.H.; Qi, L.; Bazzano, L.A. Sleep apnoea symptoms and sleepiness associate with future diet quality: A prospective analysis in the Bogalusa Heart Study. Br. J. Nutr. 2024, 132, 1214–1223. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.W.; Li, Y.; Winkelman, J.W.; Hu, F.B.; Rimm, E.B.; Gao, X. Probable insomnia is associated with future total energy intake and diet quality in men. Am. J. Clin. Nutr. 2016, 104, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Potts, K.S.; Gustat, J.; Wallace, M.E.; Ley, S.H.; Qi, L.; Bazzano, L.A. Diet quality in young adulthood and sleep at midlife: A prospective analysis in the Bogalusa Heart Study. Nutr. J. 2024, 23, 128. [Google Scholar] [CrossRef]
- Southwell, P.R.; Evans, C.R.; Hunt, J.N. Effect of a Hot Milk Drink on Movements During Sleep. Br. Med. J. 1972, 2, 429–431. [Google Scholar] [CrossRef]
- Saito, H.; Cherasse, Y.; Suzuki, R.; Mitarai, M.; Ueda, F.; Urade, Y. Zinc-rich oysters as well as zinc-yeast- and astaxanthin-enriched food improved sleep efficiency and sleep onset in a randomized controlled trial of healthy individuals. Mol. Nutr. Food Res. 2017, 61, 1600882. [Google Scholar] [CrossRef]
- Garrido, M.; Paredes, S.D.; Cubero, J.; Lozano, M.; Toribio-Delgado, A.F.; Muñoz, J.L.; Reiter, R.J.; Barriga, C.; Rodríguez, A.B. Jerte Valley cherry-enriched diets improve nocturnal rest and increase 6-sulfatoxymelatonin and total antioxidant capacity in the urine of middle-aged and elderly humans. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Castro-Diehl, C.; Wood, A.C.; Redline, S.; Reid, M.; A Johnson, D.; Maras, J.E.; Jacobs, D.R.; Shea, S.; Crawford, A.; St-Onge, M.-P.; et al. Mediterranean diet pattern and sleep duration and insomnia symptoms in the Multi-Ethnic Study of Atherosclerosis. Sleep 2018, 41, zsy158. [Google Scholar] [CrossRef]
- Wang, Y.; Fan, H.; Ren, Z.; Liu, X.; Niu, X. Sleep disorder, Mediterranean diet, and all-cause and cause-specific mortality: A prospective cohort study. BMC Public Health 2023, 23, 904. [Google Scholar] [CrossRef]
- Bild, D.E.; Bluemke, D.A.; Burke, G.L.; Detrano, R.; Diez Roux, A.V.; Folsom, A.R.; Greenland, P.; Jacobs, D.R., Jr.; Kronmal, R.; Liu, K.; et al. Multi-Ethnic Study of Atherosclerosis: Objectives and Design. Am. J. Epidemiol. 2002, 156, 871–881. [Google Scholar] [CrossRef]
- Chen, X.; Wang, R.; Zee, P.; Lutsey, P.L.; Javaheri, S.; Alcántara, C.; Jackson, C.L.; Williams, M.A.; Redline, S. Racial/Ethnic Differences in Sleep Disturbances: The Multi-Ethnic Study of Atherosclerosis (MESA). Sleep 2015, 38, 877–888. [Google Scholar] [CrossRef]
- Oakley, N.R. Validation with Polysomnography of the Sleepwatch Sleep/Wake Scoring Algorithm used by the Actiwatch Activity Monitoring System; technical report; Mini-Mitter: Bend, OR, USA, 1997. [Google Scholar]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Levine, D.W.; Lewis, M.A.; Bowen, D.J.; Kripke, D.F.; Kaplan, R.M.; Naughton, M.J.; Shumaker, S.A. Reliability and validity of Women’s Health Initiative Insomnia Rating Scale. Psychol. Assess. 2003, 15, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Horne, J.A.; Östberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Adan, A.; Almirall, H. Horne & Östberg morningness-eveningness questionnaire: A reduced scale. Personal. Individ. Differ. 1991, 12, 241–253. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012. [Google Scholar] [CrossRef]
- Nettleton, J.A.; Steffen, L.M.; Mayer-Davis, E.J.; Jenny, N.S.; Jiang, R.; Herrington, D.M.; Jacobs, D.R. Dietary patterns are associated with biochemical markers of inflammation and endothelial activation in the Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Clin. Nutr. 2006, 83, 1369–1379. [Google Scholar] [CrossRef]
- Mayer-Davis, E.J.; Vitolins, M.Z.; Carmichael, S.L.; Hemphill, S.; Tsaroucha, G.; Rushing, J.; Levin, S. Validity and Reproducibility of a Food Frequency Interview in a Multi-Cultural Epidemiologic Study. Ann. Epidemiol. 1999, 9, 314–324. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative Dietary Indices Both Strongly Predict Risk of Chronic Disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Bluemke, D.A.; Kronmal, R.A.; Lima, J.A.; Liu, K.; Olson, J.; Burke, G.L.; Folsom, A.R. The relationship of left ventricular mass and geometry to incident cardiovascular events: The MESA (Multi-Ethnic Study of Atherosclerosis) study. J. Am. Coll. Cardiol. 2008, 52, 2148–2155. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Irwin, M.L.; Addy, C.L.; Whitt, M.C.; Stolarczyk, L.M. Moderate physical activity patterns of minority women: The Cross-Cultural Activity Participation Study. J. Womens Health Gend. Based Med. 1999, 8, 805–813. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2003, 26 (Suppl. 1), s5–s20. [Google Scholar] [CrossRef]
- The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch. Intern. Med. 1997, 157, 2413–2446. [CrossRef]
- VanderWeele, T.J.; Knol, M.J. A Tutorial on Interaction. Epidemiol. Methods 2014, 3, 33–72. [Google Scholar] [CrossRef]
- Li, R.; Chambless, L. Test for Additive Interaction in Proportional Hazards Models. Ann. Epidemiol. 2007, 17, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W.; Lemeshow, S. Confidence interval estimation of interaction. Epidemiology 1992, 3, 452–456. [Google Scholar] [CrossRef]
- Rothman, K.J. The Estimation of Synergy or Antagonism. Am. J. Epidemiol. 1976, 103, 506–511. [Google Scholar] [CrossRef]
- Alli, B.Y. InteractionR: An R package for full reporting of effect modification and interaction. Softw. Impacts 2021, 10, 100147. [Google Scholar] [CrossRef]
- Zou, G.Y. On the Estimation of Additive Interaction by Use of the Four-by-two Table and Beyond. Am. J. Epidemiol. 2008, 168, 212–224. [Google Scholar] [CrossRef]
- Wood, S.N. Fast Stable Restricted Maximum Likelihood and Marginal Likelihood Estimation of Semiparametric Generalized Linear Models. J. R. Stat. Soc. Ser. B Stat. Methodol. 2011, 73, 3–36. [Google Scholar] [CrossRef]
- Wasserstein, R.L.; Lazar, N.A. The ASA’s Statement on p-Values: Context, Process, and Purpose. Am. Stat. 2016, 70, 129–133. [Google Scholar] [CrossRef]
- Potts, K.; Bazzano, L. Diet Quality and Sleep Characteristics in Midlife: The Bogalusa Heart Study. Curr. Dev. Nutr. 2022, 6 (Suppl. 1), 387. [Google Scholar] [CrossRef]
- Dashti, H.S.; Zuurbier, L.A.; de Jonge, E.; Voortman, T.; Jacques, P.F.; Lamon-Fava, S.; Scheer, F.A.J.L.; Jong, J.C.K.; Hofman, A.; Ordovás, J.M.; et al. Actigraphic sleep fragmentation, efficiency and duration associate with dietary intake in the Rotterdam Study. J. Sleep Res. 2016, 25, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Reid, M.; E Maras, J.; Shea, S.; Wood, A.C.; Castro-Diehl, C.; A Johnson, D.; Huang, T.; Jacobs, D.R.; Crawford, A.; St-Onge, M.-P.; et al. Association between diet quality and sleep apnea in the Multi-Ethnic Study of Atherosclerosis. Sleep 2019, 42, zsy194. [Google Scholar] [CrossRef] [PubMed]
- Kessler, K.; Hornemann, S.; Petzke, K.J.; Kemper, M.; Kramer, A.; Pfeiffer, A.F.H.; Pivovarova, O.; Rudovich, N. The effect of diurnal distribution of carbohydrates and fat on glycaemic control in humans: A randomized controlled trial. Sci. Rep. 2017, 7, 44170. [Google Scholar] [CrossRef]
- Kawasaki, Y.; Akamatsu, R.; Fujiwara, Y.; Omori, M.; Sugawara, M.; Yamazaki, Y.; Matsumoto, S.; Iwakabe, S.; Kobayashi, T. Later chronotype is associated with unhealthful plant-based diet quality in young Japanese women. Appetite 2021, 166, 105468. [Google Scholar] [CrossRef]
- McHill, A.W.; Hull, J.T.; Klerman, E.B. Chronic Circadian Disruption and Sleep Restriction Influence Subjective Hunger, Appetite, and Food Preference. Nutrients 2022, 14, 1800. [Google Scholar] [CrossRef]
- Scheer, F.A.J.L.; Morris, C.J.; Shea, S.A. The internal circadian clock increases hunger and appetite in the evening independent of food intake and other behaviors. Obesity 2013, 21, 421–423. [Google Scholar] [CrossRef]
- Mousavi, S.A.; Mirzababaei, A.; Shiraseb, F.; Clark, C.C.T.; Mirzaei, K. The association between modified Nordic diet with sleep quality and circadian rhythm in overweight and obese woman: A cross-sectional study. Eat. Weight. Disord. 2022, 27, 1835–1845. [Google Scholar] [CrossRef]
- Zuraikat, F.M.; St-Onge, M.P.; Makarem, N.; Boege, H.L.; Xi, H.; Aggarwal, B. Evening Chronotype Is Associated with Poorer Habitual Diet in US Women, with Dietary Energy Density Mediating a Relation of Chronotype with Cardiovascular Health. J. Nutr. 2021, 151, 1150–1158. [Google Scholar] [CrossRef]
- Xiao, Q.; Garaulet, M.; Scheer, F.A.J.L. Meal timing and obesity: Interactions with macronutrient intake and chronotype. Int. J. Obes. 2019, 43, 1701–1711. [Google Scholar] [CrossRef]
- Garaulet, M.; Gomez-Abellan, P.; Alburquerque-Bejar, J.J.; Lee, Y.C.; Ordovas, J.M.; Scheer, F.A.J.L. Timing of food intake predicts weight loss effectiveness. Int. J. Obes. 2013, 37, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Arble, D.M.; Bass, J.; Laposky, A.D.; Vitaterna, M.H.; Turek, F.W. Circadian timing of food intake contributes to weight gain. Obesity 2009, 17, 2100–2102. [Google Scholar] [CrossRef] [PubMed]
- Asher, G.; Sassone-Corsi, P. Time for Food: The Intimate Interplay between Nutrition, Metabolism, and the Circadian Clock. Cell 2015, 161, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Duncan, D.T.; Kawachi, I.; Redline, S. The Social Epidemiology of Sleep; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Johansson, L.; Thelle, D.S.; Solvoll, K.; Bjørneboe, G.E.; Drevon, C.A. Healthy dietary habits in relation to social determinants and lifestyle factors. Br. J. Nutr. 1999, 81, 211–220. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Sleep Timing Regularity | Diet Quality | ||||
|---|---|---|---|---|---|
| Total Sample a | Regular a | Irregular a | High a | Low a | |
| n | 1782 | 962 | 820 | 930 | 852 |
| CVD cases/person-years | 188/14,323.9 | 97/7853.1 | 91/6470.8 | 88/7579.9 | 100/6744.0 |
| Rate per 10,000 person-years | 131.25 | 123.52 | 140.63 | 116.10 | 148.28 |
| Age, years | 68.2 ± 9.1; 67 [14] | 68.7 ± 8.9; 68 [15] | 67.6 ± 9.3; 66 [14] | 68.6 ± 9.0; 68 [15] | 67.7 ± 9.1; 66 [15] |
| Women | 977 (54.8) | 536 (55.7) | 441 (53.8) | 538 (57.9) | 439 (51.5) |
| Race/ethnicity | |||||
| White | 699 (39.2) | 431 (44.8) | 268 (32.7) | 392 (42.2) | 307 (36.0) |
| Chinese | 205 (11.5) | 100 (10.4) | 105 (12.8) | 154 (16.6) | 51 (6.0) |
| Black | 480 (26.9) | 202 (21.0) | 278 (33.9) | 196 (21.1) | 284 (33.3) |
| Hispanic/Latino | 398 (22.3) | 229 (23.8) | 169 (20.6) | 188 (20.2) | 210 (24.7) |
| Education | |||||
| <High school | 235 (13.4) | 124 (12.9) | 111 (13.5) | 109 (11.7) | 126 (14.8) |
| High school degree | 284 (16.5) | 165 (17.2) | 119 (14.5) | 125 (13.4) | 159 (18.7) |
| Some college | 532 (29.9) | 280 (29.1) | 252 (30.7) | 245 (26.3) | 287 (33.7) |
| College degree | 731 (41.0) | 393 (40.9) | 338 (41.2) | 451 (48.5) | 280 (32.9) |
| Employed | 440 (24.7) | 233 (24.2) | 207 (25.2) | 211 (22.7) | 229 (26.9) |
| Shiftwork | 177 (10.1) | 79 (8.3) | 98 (12.1) | 88 (9.6) | 89 (10.5) |
| Married | 1093 (61.3) | 615 (63.9) | 478 (58.3) | 575 (61.8) | 518 (60.8) |
| Smoking history (pack-years) | 9.9 ± 18.6; 0 [12.6] | 9.5 (17.3); 0 [12.9] | 10.4 (20); 0 [12.5] | 8.4 (16.5); 0 [10.5] | 11.5 (20.5); 0 [15] |
| Smoking status | |||||
| Never | 845 (47.5) | 459 (47.7) | 386 (47.1) | 467 (50.3) | 378 (44.4) |
| Former | 810 (45.5) | 452 (47.0) | 358 (43.7) | 414 (44.6) | 396 (46.5) |
| Current | 126 (7.1) | 51 (5.3) | 75 (9.2) | 48 (5.2) | 78 (9.2) |
| Physical activity, MET-h/week | 91.3 ± 103.2; 62.1 [89.2] | 89.1 ± 87.1; 64.1 [83.5] | 93.9 ± 119.4; 59.4 [95.4] | 89.9 ± 88.4; 63.7 [88.9] | 92.8 ± 117.4; 60.8 [91.1] |
| Depressive symptoms | 252 (14.1) | 103 (10.7) | 149 (18.2) | 114 (12.3) | 138 (16.2) |
| CES-D score | 8.1 ± 7.5; 6 [9] | 7.4 ± 7.0; 6 [8] | 9.0 ± 8.0; 7 [10] | 7.5 ± 7.1; 6 [9] | 8.9 ± 7.9; 7 [10] |
| Body Mass Index, kg/m2 | 28.7 ± 5.6; 27.9 [7.3] | 28.5 ± 5.4; 27.7 [7.1] | 28.9 ± 5.7; 28.3 [7.4] | 27.5 ± 5.0; 26.9 [6.6] | 30.0 ± 5.9; 29.2 [7.3] |
| Sleep | |||||
| Nights of actigraphy | 7 ± 0.5; 7 [0] | 7 ± 0.4; 7 [0] | 7 ± 0.6; 7 [0] | 7 ± 0.4; 7 [0] | 7.0 ± 0.6; 7 [0] |
| Season of actigraphy | |||||
| Winter (December–February) | 238 (13.2) | 125 (13.0) | 113 (13.8) | 115 (12.4) | 123 (14.4) |
| Spring (March–May) | 294 (16.5) | 169 (17.6) | 125 (15.2) | 163 (17.5) | 131 (15.4) |
| Summer (June–August) | 339 (19.0) | 187 (19.4) | 152 (18.5) | 197 (21.2) | 142 (16.7) |
| Fall (September–November) | 911 (51.1) | 481 (50.0) | 430 (52.4) | 455 (48.9) | 456 (53.5) |
| Average sleep duration, hours | 6.6 ± 1.2; 6.7 [1.5] | 6.9 ± 1.0; 7.0 [1.2] | 6.1 ± 1.3; 6.2 [1.7] | 6.6 ± 1.2; 6.7 [1.4] | 6.5 ± 1.3; 6.6 [1.6] |
| SD of sleep duration, minutes | 75.3 ± 37.5; 68.8 [49.5] | 56.2 ± 26.3; 52.3 [31.8] | 97.6 ± 36.4; 93.0 [46.3] | 74.3 ± 38.3; 68.3 [51.9] | 76.3 ± 36.6; 69.6 [48.1] |
| Irregular sleep duration (SD sleep duration > 90 min) | 545 (30.6) | 102 (10.6) | 443 (54.0) | 282 (30.3) | 263 (30.9) |
| SD of sleep onset time, minutes | 79.8 ± 93.4; 55.9 [53.6] | 35.8 ± 13.5; 35.7 [21.5] | 131.6 ± 117.5; 92.1 [53.1] | 78.7 ± 95.7; 54.0 [53.9] | 81.1 ± 90.9; 57.9 [54.0] |
| Irregular sleep timing (SD sleep onset > 60 min) | 820 (46.0) | 0 (0.0) | 820 (100.0) | 404 (43.4) | 416 (48.8) |
| Chronotype | |||||
| Morning | 904 (51.3) | 528 (55.5) | 376 (46.4) | 490 (53.6) | 414 (48.9) |
| Intermediate | 725 (41.2) | 375 (39.4) | 350 (43.2) | 362 (39.6) | 363 (42.9) |
| Evening | 133 (7.6) | 49 (5.2) | 84 (10.4) | 63 (6.9) | 70 (8.3) |
| Insomnia symptoms | 617 (35.1) | 308 (32.4) | 309 (38.3) | 314 (34.5) | 303 (35.8) |
| Excessive daytime sleepiness | 246 (14.0) | 111 (11.6) | 135 (16.7) | 111 (12.1) | 135 (15.9) |
| Diet | |||||
| Energy intake, kcal/d | 1719.3 ± 809.1; 1567.1 [1027.5] | 1659.0 ± 737.3; 1539.0 [889.6] | 1790.1 ± 881.1; 1607.0 [1230.9] | 1746.8 ± 799.0; 1591.3 [989.6] | 1689.4 ± 819.4; 1533.5 [1089.5] |
| AHEI-2010 | 59.3 ± 10.8; 58.7 [15.6] | 60.0 ± 10.7; 59.7 [15.4] | 58.5 ± 11.0; 57.9 [15.5] | 67.6 ± 6.7; 66.7 [9.3] | 50.1 ± 6.0; 51.3 [8.5] |
| Low diet quality | 852 (47.8) | 436 (45.3) | 416 (50.7) | 0 (0.0) | 852 (100.0) |
| High Diet Quality | Low Diet Quality | ||||||
|---|---|---|---|---|---|---|---|
| Frequency (%) | CVD Cases/ Person-Years | Event Rate a | Frequency (%) | CVD Cases/ Person-Years | Event Rate a | ||
| Sleep timing regularity | Regular | 526 (29.5) | 47/4332.2 | 108.5 | 436 (24.5) | 50/3521.0 | 142.0 |
| Irregular | 404 (22.7) | 41/3247.7 | 126.2 | 416 (23.3) | 50/3223.0 | 155.1 | |
| Sleep duration regularity | Regular | 648 (36.4) | 58/5295.4 | 109.5 | 589 (33.1) | 67/4783.4 | 140.1 |
| Irregular | 282 (15.8) | 30/2284.5 | 131.3 | 263 (14.8) | 33/1960.5 | 168.3 | |
| Model 1 | Model 2 | Model 3 | ||
|---|---|---|---|---|
| HR (95% CI) | HR (95% CI) | HR (95% CI) | ||
| Diet quality | ||||
| Continuous | AHEI total score (per SD increase) | 0.87 (0.75, 1.02) | 0.88 (0.75, 1.04) | 0.88 (0.75, 1.04) |
| Binary | High diet quality (AHEI ≥ median) | Ref. | Ref. | Ref. |
| Low quality diet (AHEI < median) | 1.38 (1.03, 1.86) | 1.36 (1.00, 1.85) | 1.35 (0.99, 1.84) | |
| Categorical | Quintile 5 (highest quality diet) | Ref. | Ref. | Ref. |
| Quintile 4 | 0.72 (0.45, 1.13) | 0.70 (0.44, 1.11) | 0.70 (0.45, 1.12) | |
| Quintile 3 | 0.86 (0.55, 1.34) | 0.81 (0.52, 1.28) | 0.82 (0.52, 1.30) | |
| Quintile 2 | 0.84 (0.53, 1.34) | 0.82 (0.50, 1.32) | 0.82 (0.51, 1.33) | |
| Quintile 1 (lowest quality diet) | 1.43 (0.93, 2.19) | 1.38 (0.88, 2.16) | 1.35 (0.86, 2.12) | |
| p for trend a | 0.117 | 0.181 | 0.208 | |
| Sleep timing regularity | ||||
| Continuous | SD sleep onset (per 1 h increase) | 1.11 (1.03, 1.20) | 1.11 (1.03, 1.20) | 1.10 (1.02, 1.19) |
| Binary | Regular (SD sleep onset < 60 min) | Ref. | Ref. | Ref. |
| Irregular (SD sleep onset ≥ 60 min) | 1.25 (0.94, 1.67) | 1.23 (0.92, 1.65) | 1.21 (0.91, 1.63) | |
| Categorical b | SD sleep onset < 30 min | Ref. | Ref. | Ref. |
| SD sleep onset 30 to <60 min | 0.94 (0.63, 1.42) | 0.93 (0.62, 1.41) | 0.92 (0.61, 1.40) | |
| SD sleep onset 60 to <90 min | 1.12 (0.73, 1.73) | 1.10 (0.71, 1.70) | 1.08 (0.70, 1.69) | |
| SD sleep onset ≥ 90 min | 1.29 (0.84, 1.98) | 1.28 (0.83, 1.97) | 1.24 (0.80, 1.91) | |
| p for trend a | 0.144 | 0.170 | 0.219 | |
| Sleep duration regularity | ||||
| Continuous b | SD sleep duration (per 1 h increase) | 1.26 (1.01, 1.58) | 1.25 (1.00, 1.57) | 1.24 (0.98, 1.55) |
| Binary | Regular (SD sleep duration < 90 min) | Ref. | Ref. | Ref. |
| Irregular (SD sleep duration ≥ 90 min) | 1.28 (0.94, 1.73) | 1.27 (0.93, 1.72) | 1.25 (0.92, 1.71) | |
| Categorical | SD sleep duration < 60 min | Ref. | Ref. | Ref. |
| SD sleep duration 60 to <90 min | 1.21 (0.85, 1.74) | 1.17 (0.85, 1.68) | 1.15 (0.80, 1.66) | |
| SD sleep duration 90 to <120 min | 1.30 (0.87, 1.94) | 1.25 (0.84, 1.88) | 1.23 (0.82, 1.85) | |
| SD sleep duration ≥ 120 min | 1.55 (0.98, 2.44) | 1.54 (0.98, 2.43) | 1.52 (0.96, 2.41) | |
| p for trend a | 0.046 | 0.059 | 0.073 | |
| Diet Quality | |||
|---|---|---|---|
| High (AHEI ≥ Median) | Low (AHEI < Median) | ||
| Sleep timing regularity | |||
| Effect of low (vs. high) diet quality within strata of sleep timing regularity | |||
| Regular (SD sleep onset time < 60 min) | 1.00 | 1.37 (0.91, 2.08) | 1.37 (0.91, 2.08) |
| Irregular (SD sleep onset time ≥ 60 min) | 1.24 (0.81, 1.90) | 1.56 (1.03, 2.37) | 1.26 (0.82, 1.94) |
| Effect of irregular sleep timing (vs. regular) within strata of diet quality | 1.24 (0.81, 1.90) | 1.14 (0.76, 1.71) | |
| Multiplicative interaction a | 0.92 (0.51, 1.64) | Interaction-p b, using continuous AHEI and SD sleep onset: 0.340 | |
| Additive interaction (RERI) c | −0.05 (−1.00, 0.66) | ||
| Sleep duration regularity | |||
| Effect of low (vs. high) diet quality within strata of sleep duration regularity | |||
| Regular (SD sleep duration < 90 min) | 1.00 | 1.31 (0.91, 1.90) | 1.31 (0.91, 1.90) |
| Irregular (SD sleep duration ≥ 90 min) | 1.23 (0.78, 1.92) | 1.70 (1.09, 2.67) | 1.39 (0.84, 1.99) |
| Effect of irregular sleep duration (vs. regular) within strata of diet quality | 1.23 (0.78, 1.92) | 1.30 (0.85, 1.99) | |
| Multiplicative interaction a | 1.06 (0.58, 1.96) | Interaction-p b, for continuous AHEI and SD sleep duration: 0.805 | |
| Additive interaction (RERI) c | 0.17 (−0.78, 1.04) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potts, K.S.; Veldkamp, C.; Wood, A.C.; Michos, E.D.; Noordam, R.; Huang, T.; Redline, S.; Wang, H. The Joint Association of Diet Quality and Sleep Regularity with Incident Cardiovascular Disease in the Multi-Ethnic Study of Atherosclerosis. Nutrients 2025, 17, 1750. https://doi.org/10.3390/nu17111750
Potts KS, Veldkamp C, Wood AC, Michos ED, Noordam R, Huang T, Redline S, Wang H. The Joint Association of Diet Quality and Sleep Regularity with Incident Cardiovascular Disease in the Multi-Ethnic Study of Atherosclerosis. Nutrients. 2025; 17(11):1750. https://doi.org/10.3390/nu17111750
Chicago/Turabian StylePotts, Kaitlin S., Claire Veldkamp, Alexis C. Wood, Erin D. Michos, Raymond Noordam, Tianyi Huang, Susan Redline, and Heming Wang. 2025. "The Joint Association of Diet Quality and Sleep Regularity with Incident Cardiovascular Disease in the Multi-Ethnic Study of Atherosclerosis" Nutrients 17, no. 11: 1750. https://doi.org/10.3390/nu17111750
APA StylePotts, K. S., Veldkamp, C., Wood, A. C., Michos, E. D., Noordam, R., Huang, T., Redline, S., & Wang, H. (2025). The Joint Association of Diet Quality and Sleep Regularity with Incident Cardiovascular Disease in the Multi-Ethnic Study of Atherosclerosis. Nutrients, 17(11), 1750. https://doi.org/10.3390/nu17111750