
The Influence of Acute and Chronic Exercise on Appetite and Appetite Regulation in Patients with Prediabetes or Type 2 Diabetes Mellitus—A Systematic Review



Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Selection Process
2.4. Data Collection Process
2.5. Data Items (Outcomes)
2.6. Risk of Bias Assessment
2.7. Synthesis Methods
3. Results
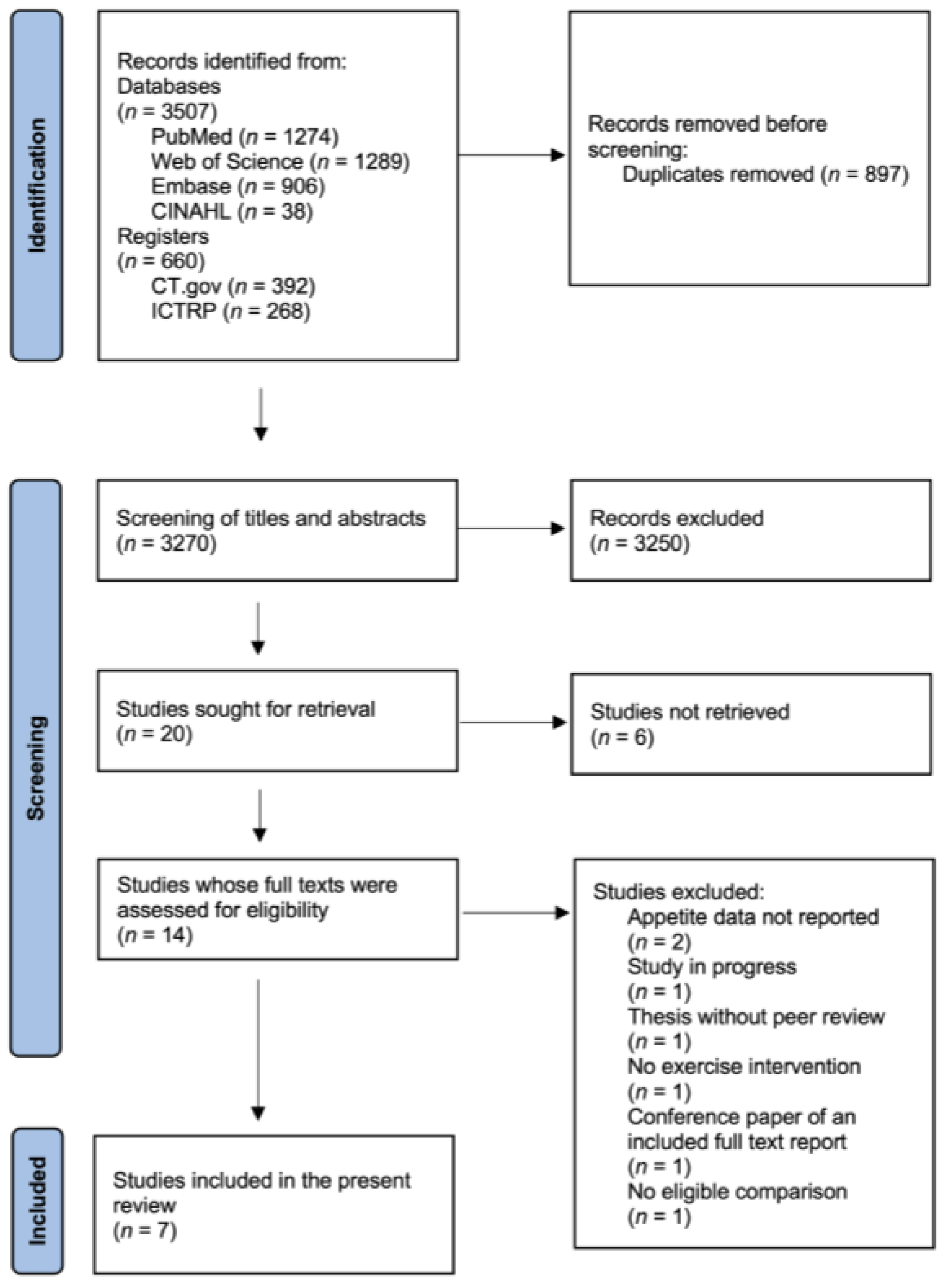
3.1. Study Selection
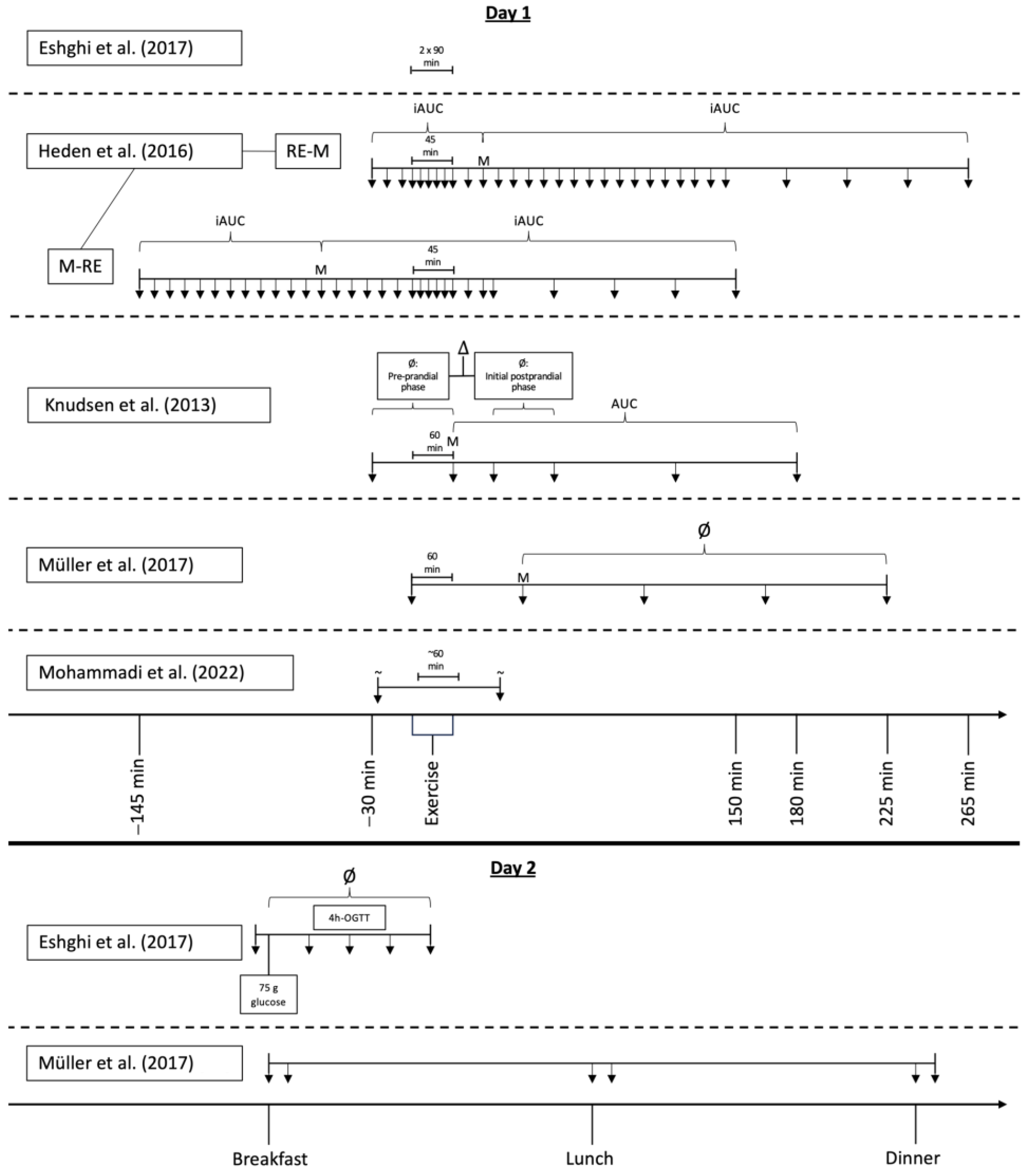
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Effects of Acute Exercise on Appetite and Appetite Regulation in Patients with T2DM Compared to Control Conditions (without Exercise)
3.5. Effects of Chronic Exercise on Appetite and Appetite Regulation in Patients with Prediabetes or T2DM
3.6. Effects of Exercise on Appetite and Appetite Regulation in Patients with T2DM versus Normal Glucose Tolerance
3.7. Adverse Events and Patients’ Adherence to the Study Protocol
4. Discussion
Limitations and Merits of the Present Review
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| (d)AG | (Des-)acylated ghrelin |
| (i)AUC | (Incremental) area under the curve |
| AE | Aerobic endurance exercise |
| AT | Aerobic endurance training |
| BMI | Body mass index |
| CENTRAL | Cochrane Central Register of Controlled Trials |
| CINAHL | Cumulative Index to Nursing and Allied Health Literature |
| CKK | Cholecystokinin |
| CT.gov | ClinicalTrials.gov |
| GIP | Glucose-dependent insulinotropic peptide |
| GLP-1 | Glucagon-like peptide-1 |
| HbA1c | Glycated hemoglobin |
| HIIT | High-intensity interval training |
| HRpeak | Maximal heart rate |
| ICTRP | International Clinical Trials Registry Platform |
| M | Meal |
| NGT | Normal glucose tolerance |
| OGTT | Oral glucose tolerance test |
| PEDro | Physiotherapy Evidence Database |
| PFC | Prospective food consumption |
| PICO | Patient Intervention Comparison Outcome |
| PP | Pancreatic polypeptide |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PYY | Peptide tyrosine tyrosine |
| RE | Resistance exercise |
| RM | Repetition maximum |
| RT | Resistance training |
| T2DM | Type 2 diabetes mellitus |
| TG | Total ghrelin |
| VO2peak | Maximal oxygen uptake |
| VT | Ventilatory threshold |
| Wmax | Maximal work capacity |
References
- NCD Risk Factor Collaboration. Worldwide trends in diabetes since 1980: A pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 2016, 387, 1513–1530. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016.
- Vazquez, G.; Duval, S.; Jacobs, D.R., Jr.; Silventoinen, K. Comparison of body mass index, waist circumference, and waist/hip ratio in predicting incident diabetes: A meta-analysis. Epidemiol. Rev. 2007, 29, 115–128. [Google Scholar] [CrossRef]
- Lindström, J.; Ilanne-Parikka, P.; Peltonen, M.; Aunola, S.; Eriksson, J.G.; Hemiö, K.; Hämäläinen, H.; Härkönen, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; et al. Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: Follow-up of the Finnish Diabetes Prevention Study. Lancet 2006, 368, 1673–1679. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Gaglia, J.L.; Hilliard, M.E.; Isaacs, D.; et al. 3. Prevention or Delay of Diabetes and Associated Comorbidities: Standards of Care in Diabetes—2023. Diabetes Care 2022, 46, S41–S48. [Google Scholar] [CrossRef]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 5. Facilitating Positive Health Behaviors and Well-being to Improve Health Outcomes: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46, S68–S96. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Edholm, O.G.; Adam, J.M.; Healy, M.J.; Wolff, H.S.; Goldsmith, R.; Best, T.W. Food intake and energy expenditure of army recruits. Br. J. Nutr. 1970, 24, 1091–1107. [Google Scholar] [CrossRef]
- Edholm, O.G.; Fletcher, J.G.; Widdowson, E.M.; McCance, R.A. The energy expenditure and food intake of individual men. Br. J. Nutr. 1955, 9, 286–300. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.; Morgan, L.; Truby, H. A review of the effects of exercise on appetite regulation: An obesity perspective. Int. J. Obes. 2008, 32, 1337–1338. [Google Scholar] [CrossRef]
- Blundell, J.E.; Finlayson, G.; Gibbons, C.; Caudwell, P.; Hopkins, M. The biology of appetite control: Do resting metabolic rate and fat-free mass drive energy intake? Physiol. Behav. 2015, 152, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Klok, M.D.; Jakobsdottir, S.; Drent, M.L. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: A review. Obes. Rev. 2007, 8, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Considine, R.V.; Sinha, M.K.; Heiman, M.L.; Kriauciunas, A.; Stephens, T.W.; Nyce, M.R.; Ohannesian, J.P.; Marco, C.C.; McKee, L.J.; Bauer, T.L.; et al. Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N. Engl. J. Med. 1996, 334, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Kissileff, H.R.; Pi-Sunyer, F.X.; Thornton, J.; Smith, G.P. C-terminal octapeptide of cholecystokinin decreases food intake in man. Am. J. Clin. Nutr. 1981, 34, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Verdich, C.; Flint, A.; Gutzwiller, J.P.; Näslund, E.; Beglinger, C.; Hellström, P.M.; Long, S.J.; Morgan, L.M.; Holst, J.J.; Astrup, A. A meta-analysis of the effect of glucagon-like peptide-1 (7-36) amide on ad libitum energy intake in humans. J. Clin. Endocrinol. Metab. 2001, 86, 4382–4389. [Google Scholar] [CrossRef] [PubMed]
- Batterham, R.L.; Le Roux, C.W.; Cohen, M.A.; Park, A.J.; Ellis, S.M.; Patterson, M.; Frost, G.S.; Ghatei, M.A.; Bloom, S.R. Pancreatic polypeptide reduces appetite and food intake in humans. J. Clin. Endocrinol. Metab. 2003, 88, 3989–3992. [Google Scholar] [CrossRef] [PubMed]
- Batterham, R.L.; Cowley, M.A.; Small, C.J.; Herzog, H.; Cohen, M.A.; Dakin, C.L.; Wren, A.M.; Brynes, A.E.; Low, M.J.; Ghatei, M.A.; et al. Gut hormone PYY(3-36) physiologically inhibits food intake. Nature 2002, 418, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Wren, A.M.; Seal, L.J.; Cohen, M.A.; Brynes, A.E.; Frost, G.S.; Murphy, K.G.; Dhillo, W.S.; Ghatei, M.A.; Bloom, S.R. Ghrelin enhances appetite and increases food intake in humans. J. Clin. Endocrinol. Metab. 2001, 86, 5992. [Google Scholar] [CrossRef] [PubMed]
- Hosoda, H.; Kojima, M.; Matsuo, H.; Kangawa, K. Ghrelin and des-acyl ghrelin: Two major forms of rat ghrelin peptide in gastrointestinal tissue. Biochem. Biophys. Res. Commun. 2000, 279, 909–913. [Google Scholar] [CrossRef]
- Schubert, M.M.; Desbrow, B.; Sabapathy, S.; Leveritt, M. Acute exercise and subsequent energy intake. A Meta-Analysis. Appetite 2013, 63, 92–104. [Google Scholar] [CrossRef]
- Schubert, M.M.; Sabapathy, S.; Leveritt, M.; Desbrow, B. Acute exercise and hormones related to appetite regulation: A meta-analysis. Sports Med. 2014, 44, 387–403. [Google Scholar] [CrossRef] [PubMed]
- King, N.A.; Burley, V.J.; Blundell, J.E. Exercise-induced suppression of appetite: Effects on food intake and implications for energy balance. Eur. J. Clin. Nutr. 1994, 48, 715–724. [Google Scholar] [PubMed]
- King, N.A.; Hopkins, M.; Caudwell, P.; Stubbs, R.J.; Blundell, J.E. Individual variability following 12 weeks of supervised exercise: Identification and characterization of compensation for exercise-induced weight loss. Int. J. Obes. 2008, 32, 177–184. [Google Scholar] [CrossRef]
- Martin, C.K.; Johnson, W.D.; Myers, C.A.; Apolzan, J.W.; Earnest, C.P.; Thomas, D.M.; Rood, J.C.; Johannsen, N.M.; Tudor-Locke, C.; Harris, M.; et al. Effect of different doses of supervised exercise on food intake, metabolism, and non-exercise physical activity: The E-MECHANIC randomized controlled trial. Am. J. Clin. Nutr. 2019, 110, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Pontzer, H.; Durazo-Arvizu, R.; Dugas, L.R.; Plange-Rhule, J.; Bovet, P.; Forrester, T.E.; Lambert, E.V.; Cooper, R.S.; Schoeller, D.A.; Luke, A. Constrained Total Energy Expenditure and Metabolic Adaptation to Physical Activity in Adult Humans. Curr. Biol. 2016, 26, 410–417. [Google Scholar] [CrossRef]
- King, N.A.; Caudwell, P.P.; Hopkins, M.; Stubbs, J.R.; Naslund, E.; Blundell, J.E. Dual-process action of exercise on appetite control: Increase in orexigenic drive but improvement in meal-induced satiety. Am. J. Clin. Nutr. 2009, 90, 921–927. [Google Scholar] [CrossRef]
- Martins, C.; Kulseng, B.; King, N.A.; Holst, J.J.; Blundell, J.E. The effects of exercise-induced weight loss on appetite-related peptides and motivation to eat. J. Clin. Endocrinol. Metab. 2010, 95, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Caudwell, P.; Finlayson, G.; Gibbons, C.; Hopkins, M.; King, N.; Näslund, E.; Blundell, J.E. Resting metabolic rate is associated with hunger, self-determined meal size, and daily energy intake and may represent a marker for appetite. Am. J. Clin. Nutr. 2013, 97, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Weise, C.M.; Hohenadel, M.G.; Krakoff, J.; Votruba, S.B. Body composition and energy expenditure predict ad-libitum food and macronutrient intake in humans. Int. J. Obes. 2014, 38, 243–251. [Google Scholar] [CrossRef]
- Jones, T.E.; Basilio, J.L.; Brophy, P.M.; McCammon, M.R.; Hickner, R.C. Long-term exercise training in overweight adolescents improves plasma peptide YY and resistin. Obesity 2009, 17, 1189–1195. [Google Scholar] [CrossRef]
- Morishima, T.; Kurihara, T.; Hamaoka, T.; Goto, K. Whole body, regional fat accumulation, and appetite-related hormonal response after hypoxic training. Clin. Physiol. Funct. Imaging 2014, 34, 90–97. [Google Scholar] [CrossRef]
- Rosenkilde, M.; Reichkendler, M.H.; Auerbach, P.; Toräng, S.; Gram, A.S.; Ploug, T.; Holst, J.J.; Sjödin, A.; Stallknecht, B. Appetite regulation in overweight, sedentary men after different amounts of endurance exercise: A randomized controlled trial. J. Appl. Physiol. 2013, 115, 1599–1609. [Google Scholar] [CrossRef] [PubMed]
- Guelfi, K.J.; Donges, C.E.; Duffield, R. Beneficial effects of 12 weeks of aerobic compared with resistance exercise training on perceived appetite in previously sedentary overweight and obese men. Metabolism 2013, 62, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Anthony, K.; Reed, L.J.; Dunn, J.T.; Bingham, E.; Hopkins, D.; Marsden, P.K.; Amiel, S.A. Attenuation of insulin-evoked responses in brain networks controlling appetite and reward in insulin resistance: The cerebral basis for impaired control of food intake in metabolic syndrome? Diabetes 2006, 55, 2986–2992. [Google Scholar] [CrossRef] [PubMed]
- de Lartigue, G.; Barbier de la Serre, C.; Espero, E.; Lee, J.; Raybould, H.E. Diet-induced obesity leads to the development of leptin resistance in vagal afferent neurons. Am. J. Physiol. Endocrinol. Metab. 2011, 301, E187–E195. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, R.J.; Francis, H.M. The hippocampus and the regulation of human food intake. Psychol. Bull. 2017, 143, 1011–1032. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Thabane, L.; Thomas, T.; Ye, C.; Paul, J. Posing the research question: Not so simple. Can. J. Anaesth. 2009, 56, 71–79. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46, S19–S40. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- DigitizeIt. Automatisches Digitalisieren von Graphen und Diagrammen in (x,y)-Daten. Available online: https://www.digitizeit.xyz/de/ (accessed on 11 November 2023).
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Martínez, P.; Ramirez-Campillo, R.; Alix-Fages, C.; Gene-Morales, J.; García-Ramos, A.; Colado, J.C. Chronic Resistance Training Effects on Serum Adipokines in Type 2 Diabetes Mellitus: A Systematic Review. Healthcare 2023, 11, 594. [Google Scholar] [CrossRef] [PubMed]
- Meuffels, F.M.; Isenmann, E.; Strube, M.; Lesch, A.; Oberste, M.; Brinkmann, C. Exercise Interventions Combined With Dietary Supplements in Type 2 Diabetes Mellitus Patients-A Systematic Review of Relevant Health Outcomes. Front. Nutr. 2022, 9, 817724. [Google Scholar] [CrossRef] [PubMed]
- Eshghi, S.; Fletcher, K.; Myette-Cote, E.; Durrer, C.; Gabr, R.; Little, J.; Senior, P.; Steinback, C.; Davenport, M.; Bell, G.; et al. Glycemic and metabolic effects of two long bouts of moderate-intensity exercise in men with normal glucose tolerance or type 2 diabetes. Front. Endocrinol. 2017, 8, 154. [Google Scholar] [CrossRef] [PubMed]
- Heden, T.; Liu, Y.; Kanaley, J. Impact of Exercise Timing on Appetite Regulation in Individuals with Type 2 Diabetes. Med. Sci. Sports Exerc. 2016, 48, 182–189. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Knudsen, S.; Karstoft, K.; Solomon, T. Impaired postprandial fullness in Type 2 diabetic subjects is rescued by acute exercise independently of total and acylated ghrelin. J. Appl. Physiol. 2013, 115, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Müller, I.; Wedell-Neergaard, A.; Solomon, T.; Karstoft, K. The impact of acute bouts of interval and continuous walking on energy-intake and appetite regulation in subjects with type 2 diabetes. Front. Endocrinol. 2017, 5, 13524. [Google Scholar] [CrossRef] [PubMed]
- Heiston, E.; Eichner, N.; Gilbertson, N.; Gaitan, J.; Kranz, S.; Weltman, A.; Malin, S. Two weeks of exercise training intensity on appetite regulation in obese adults with prediabetes. J. Appl. Physiol. 2019, 126, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Vidanage, D.; Wasalathanthri, S.; Hettiarachchi, P. Long-term aerobic and combined exercises enhance the satiety response and modulate the energy intake in patients with type 2 diabetes mellitus (T2DM): A randomized controlled trial. BMC Sports Sci. Med. Rehabil. 2023, 15, 48. [Google Scholar] [CrossRef]
- Mohammadi, A.; Bijeh, N.; Moazzami, M.; Kazem, K.; Rahimi, N. Effect of Exercise Training on Spexin Level, Appetite, Lipid Accumulation Product, Visceral Adiposity Index, and Body Composition in Adults With Type 2 Diabetes. Biol. Res. Nurs. 2022, 24, 152–162. [Google Scholar] [CrossRef]
- Douglass, R.; Heckman, G. Drug-related taste disturbance: A contributing factor in geriatric syndromes. Can. Fam. Physician 2010, 56, 1142–1147. [Google Scholar] [PubMed]
- Schiffman, S.S. Influence of medications on taste and smell. World J. Otorhinolaryngol. Head Neck Surg. 2018, 4, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.K.H.; Chen, Y.; He, M.; Lin, C.; Bian, Z.; Wong, A.O.L. Mouse Spexin: (II) Functional Role as a Satiety Factor inhibiting Food Intake by Regulatory Actions Within the Hypothalamus. Front. Endocrinol. 2021, 12, 681647. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Ju, M.; Fang, P.; Zhang, Z. Emerging central and peripheral actions of spexin in feeding behavior, leptin resistance and obesity. Biochem. Pharmacol. 2022, 202, 115121. [Google Scholar] [CrossRef] [PubMed]
- Broom, D.R.; Batterham, R.L.; King, J.A.; Stensel, D.J. Influence of resistance and aerobic exercise on hunger, circulating levels of acylated ghrelin, and peptide YY in healthy males. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 296, R29–R35. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.; Morgan, L.M.; Bloom, S.R.; Robertson, M.D. Effects of exercise on gut peptides, energy intake and appetite. J. Endocrinol. 2007, 193, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Balaguera-Cortes, L.; Wallman, K.E.; Fairchild, T.J.; Guelfi, K.J. Energy intake and appetite-related hormones following acute aerobic and resistance exercise. Appl. Physiol. Nutr. Metab. 2011, 36, 958–966. [Google Scholar] [CrossRef]
- Beaulieu, K.; Blundell, J.E.; van Baak, M.A.; Battista, F.; Busetto, L.; Carraça, E.V.; Dicker, D.; Encantado, J.; Ermolao, A.; Farpour-Lambert, N.; et al. Effect of exercise training interventions on energy intake and appetite control in adults with overweight or obesity: A systematic review and meta-analysis. Obes. Rev. 2021, 22 (Suppl. 4), e13251. [Google Scholar] [CrossRef]
- Bellicha, A.; van Baak, M.A.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; Carraça, E.V.; Dicker, D.; Encantado, J.; Ermolao, A.; et al. Effect of exercise training on weight loss, body composition changes, and weight maintenance in adults with overweight or obesity: An overview of 12 systematic reviews and 149 studies. Obes. Rev. 2021, 22 (Suppl. 4), e13256. [Google Scholar] [CrossRef]
- Dascalu, A.M.; Serban, D.; Tanasescu, D.; Vancea, G.; Cristea, B.M.; Stana, D.; Nicolae, V.A.; Serboiu, C.; Tribus, L.C.; Tudor, C.; et al. The Value of White Cell Inflammatory Biomarkers as Potential Predictors for Diabetic Retinopathy in Type 2 Diabetes Mellitus (T2DM). Biomedicines 2023, 11, 2106. [Google Scholar] [CrossRef]
- Tatikola, S.P.; Natarajan, V.; Desai, V.K.; Asirvatham, A.R.; Rajsekhar, H. Effect of various exercise protocols on neuropathic pain in individuals with type 2 diabetes with peripheral neuropathy: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2022, 16, 102603. [Google Scholar] [CrossRef] [PubMed]
- King, N.A.; Caudwell, P.; Hopkins, M.; Byrne, N.M.; Colley, R.; Hills, A.P.; Stubbs, J.R.; Blundell, J.E. Metabolic and behavioral compensatory responses to exercise interventions: Barriers to weight loss. Obesity 2007, 15, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.M.; Bouchard, C.; Church, T.; Slentz, C.; Kraus, W.E.; Redman, L.M.; Martin, C.K.; Silva, A.M.; Vossen, M.; Westerterp, K.; et al. Why do individuals not lose more weight from an exercise intervention at a defined dose? An energy balance analysis. Obes. Rev. 2012, 13, 835–847. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Databases | Search Terms |
|---|---|
| PubMed, Web of Science | (“diabetes” OR “diabetic” OR “T2D” OR “T2DM” OR “insulin resistance” OR “insulin-resistant” OR “prediabetes” OR “type 2 diabetes” OR “impaired glucose control”) AND (“physical activit*” OR “training” OR “exercise” OR “sport” OR “endurance activit*” OR “aerobic activit*” OR “resistance training” OR “strength training” OR “muscle-strengthening” OR “weight-lifting program” OR “high-intensity interval training” OR “HIIT” OR “physical conditioning” OR “walking” OR “sedentary time” OR “sedentary lifestyle” OR “sitting time”) AND (“energy intake” OR “caloric intake” OR “calorie intake” OR “food intake” OR “meal size” OR “energy density” OR “feeding behavio*” OR “food preference*” OR “eating behavio*” OR “satiation” OR “motivation to eat” OR “food choice” OR “food selection” OR “desire to eat” OR “food reward” OR “food craving*” OR “appetite” OR “hunger” OR “compensatory eating” OR “appetite control” OR “satiety” OR “fullness” OR “energy balance” OR “energy intake” OR “test meal” OR “prospective food consumption”) AND (“controlled” OR “control group” OR “trial”) All fields. No filters. No automatic term mapping. |
| Cochrane Central Register of Controlled Trials | (“diabetes” OR “diabetic” OR “T2D” OR “T2DM” OR “insulin resistance” OR “insulin-resistant” OR “prediabetes” OR “type 2 diabetes” OR “impaired glucose control”) AND (“physical activity” OR “training” OR “exercise” OR “sport” OR “endurance activity” OR “aerobic activity” OR “resistance training” OR “strength training” OR “muscle-strengthening” OR “weight-lifting program” OR “high-intensity interval training” OR “HIIT” OR “physical conditioning” OR “walking” OR “sedentary time” OR “sedentary lifestyle” OR “sitting time”) AND (“energy intake” OR “caloric intake” OR “calorie intake” OR “food intake” OR “meal size” OR “energy density” OR “feeding behavior” OR “food preference” OR “eating behavior” OR “satiation” OR “motivation to eat” OR “food choice” OR “food selection” OR “desire to eat” OR “food reward” OR “food craving” OR “appetite” OR “hunger” OR “compensatory eating” OR “appetite control” OR “satiety” OR “fullness” OR “energy balance” OR “energy intake” OR “test meal” OR “prospective food consumption”) AND (“controlled” OR “control group” OR “trial”) All fields. Filters: Trials. No searching of word variations. |
| Study | Study Design | Trials | Duration of Intervention | Participants’ Characteristics | Exercise Type | Appetite Ratings | Appetite Hormones | ||
|---|---|---|---|---|---|---|---|---|---|
| N (m/f) | Age (Years) | BMI (kg/m2) | |||||||
| Eshghi et al. (2017) [46] | Randomized crossover (2 groups) |
| 1 day | 12 (12/0) T2DM: 6 NGT: 6 | T2DM: 61 ± 9 NGT: 43 ± 11 | T2DM: 25 ± 4 NGT: 27 ± 3 |  |
|
|
| Heden et al. (2016) [47] | Randomized crossover |
| 1 day | 12 (5/7) | 47 ± 12 | 37 ± 6 |  |
|
|
| Knudsen et al. (2013) [48] | Randomized crossover (2 groups) |
| 1 day | 15 (15/0) T2DM: 8 NGT: 7 | T2DM: 61 ± 2 NGT: 57 ± 1 | T2DM: 28 ± 1 NGT: 27 ± 2 |  |
|
|
| Müller et al. (2017) [49] | Randomized crossover |
| 1 day | 13 (8/5) | 65 ± 2 | 33 ± 1 | |
|
|
| Mohammadi et al. (2022) [52] | Randomized parallel group design → PP |
| 12 weeks | 28 (28/0) AE/AT: 10 RE/RT: 9 Control: 9 | ≤50 | AE/AT: 29 ± 2 RE/RT: 29 ± 2 Control: 29 ± 2 | |
|
|
| Heiston et al. (2019) [50] | Randomized parallel group design → PP |
| 2 weeks | 28 (6/22) AT: 14 (3/11) HIIT: 14 (3/11) | AT: 62 ± 2 HIIT: 60 ± 2 | AT: 35 ± 2 HIIT: 32 ± 1 | |
|
|
| Vidanage et al. (2023) [51] | Randomized parallel group design → PP |
| 6 months | 103 AT: 36 AT + RT: 34 Control: 33 | AT: 49 ± 6 AT + RT: 53 ± 5 Control: 51 ± 5 (data from n = 36 in each group at baseline) | AT: 24 ± 4 AT + RT: 25 ± 4 Control: 25 ± 3 (data from n = 36 in each group at baseline) | + |
|
|
, walking/running; , resistance exercise; , cycling.| Study | Exercise | Diet | Medication | ||
|---|---|---|---|---|---|
| Type | Modality | Supervised | |||
| Eshghi et al. (2017) [46] | Aerobic endurance exercise | Walking on a treadmill; 1-month exercise habituation phase before the intervention days (3 sessions per week at 80% of VT, until participants could walk for 90 min continuously); Two separate exercise bouts on one intervention day; 3.5 h rest between the two exercise bouts; 90 min per exercise bout; 80% of VT | Yes | Standardized diet with maintenance calories; two meals each after exercise on testing days. The first exercise bout was performed in the fasted state. | Metformin was paused 12 h before and during each testing day. No insulin. |
| Heden et al. (2016) [47] | Resistance exercise | Leg presses, seated calf raises, seated chest flies, seated back flies, back extensions, shoulder raises, leg curls, and abdominal crunches; 1 warm-up set, 2 working sets per exercise; 10 repetitions per set; 50% of 10-RM during warm up sets, 100% of 10-RM during working sets; 1–2 min rest between sets | Yes | Standardized diet with maintenance calories; three meals on testing days. | Usual medication (not specified) continued. No insulin. |
| Knudsen et al. (2013) [48] | Aerobic endurance exercise | Cycle ergometry; 60 min; 50% of Wmax, 60–90 rpm | Yes | Same mean energy intake and macronutrient distribution for 3 days on each trial. Controlled by using diet records. Exercise started after an overnight fasting period. | Antidiabetic, antihypertensive, and statin drugs were paused 3 days before and during each testing day. Drugs used: metformin (n = 7), DPP4 inhibitors and sulfonylureas (n = 1), antihypertensive drugs (n = 2), and statins (n = 4). No insulin. |
| Müller et al. (2017) [49] | Endurance exercise (aerobic (AE) and high-intensity exercise (HIIT)) | Walking on a treadmill; 60 min; AE: 73% of VO2peak HIIT: 3 min at 54% of VO2peak followed by 3 min at 89% of VO2peak | Yes | Same diet for 24 h before intervention days. Achieved by replicating a diet record of the habitual diet of the participants during the first trial. Same standardized breakfast prior to exercise on the intervention days. | Antidiabetic medication (not specified) paused 2 days before and during each testing day. No insulin. |
| Mohammadi et al. (2022) [52] | Aerobic endurance training (AT) Resistance training (RT) | 12 weeks; 3 sessions/week; AT: Walking/running on a treadmill; exercise duration and intensity increased over the course of the study; 10–15 min warm up, 10–35 min workout, 10–15 min cool down; 50–70% of HRmax RT: Leg presses, chest presses, leg extensions, leg flexions, lat pulldowns, overhead presses, arm curls, and triceps pushdowns; number of sets and intensity of 1-RM increased over the course of the study; 3–4 sets/exercise, 55–80% of 1-RM; 60–120 s rest between sets | Yes | Instruction to maintain habitual diet. Participants were instructed to consume the same diet during the week prior to the intervention and the week prior to the post-test evaluation. Controlled by using food frequency questionnaires. | Not further specified. Intake of any medication was forbidden 24 h before testing. No insulin. |
| Heiston et al. (2019) [50] | Endurance training (aerobic or HIIT) | 12 sessions over 13 days; cycle ergometry; 60 min/session; AT: 70% of HRpeak HIIT: 3 min at 90% of HRpeak followed by 3 min of 50% of HRpeak | Yes | Instruction to maintain habitual diet. Participants were instructed to consume a diet containing ~250 g of carbohydrates during the 24 h before pre-intervention testing. The diet record was replicated during the 24 h before post-intervention testing. | No antidiabetic or weight-loss-inducing medication. No insulin. |
| Vidanage et al. (2023) [51] | Aerobic endurance training (AT) Aerobic endurance training (AT) + resistance training (RT) | 6 months; AT: Brisk walking; at least 150 min/week, 3–5 days/week; RT: Exercises with resistance bands for biceps, triceps, hamstrings, quadriceps, and pectoralis major muscle; 20 min/day; 2–3 days/week | No | No instructions. | Individuals on medication known to influence taste were excluded [53,54]. No insulin. |
| Item 1 # | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Eshghi et al. (2017) [46] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Heden et al. (2016) [47] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Knudsen et al. (2013) [48] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Müller et al. (2017) [49] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Mohammadi et al. (2022) [52] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 6 |
| Heiston et al. (2019) [50] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Vidanage et al. (2023) [51] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Study | Trial | Hunger | Fullness | PFC | Satiety | Nausea | Desire to Eat Sweet | AG | TG | PP | PYY | Leptin | GIP | GLP-1 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Eshghi et al. (2017) [46] | AE | → | (→) ↓: In the fasted state on day 2 | (→) ↑: Postprandial average during the 4 h OGTT on day 2 | - | - | (→) ↑: Postprandial average during the 4 h OGTT on day 2 | - | - | - | - | - | (→) ↑: After the 2nd exercise session on day 1 and in the fasted state on day 2 | (→) ↑: In the fasted state on day 2 |
| Heden et al. (2016) [47] | RE-M | (→) ↓: 25, 240, and 270 min post-exercise | (→) ↑: Pre-meal iAUC, during exercise (30 and 40 min after start), and 5 and 25 min after end of exercise | - | - | - | - | (→) ↓: Pre-meal iAUC, during exercise (40 min after start), and 25 and 60 min post-exercise | - | → | → | - | - | - |
| M-RE | (→) ↓: 10, 120, and 150 min post-exercise | (→) ↑: 120 and 150 min post-exercise | - | - | - | - | → | - | (→) ↓: During exercise (15 min after start) | → | - | - | - | |
| Knudsen et al. (2013) [48] | AE | → | (→) ↑: 180 min AUC post-exercise | → | - | → | - | → | → | - | - | - | - | - |
| Müller et al. (2017) [49] | HIIT | → | (→) ↑: 45 min post-exercise | → | - | → | - | → | - | → | → | → | - | - |
| AE | → | → | → | - | → | - | → | - | → | → | → | - | - | |
| Mohammadi et al. (2022) [52] | RE | ↑ After the first and last exercise sessions 1 | → | ↑ After the first and last exercise sessions 1 | → | - | - | - | - | - | - | - | - | - |
| AE | → | → | → | → | - | - | - | - | - | - | - | - | - |
| Study | Trial | Hunger | Fullness | PFC | Satiety | Spexin |
|---|---|---|---|---|---|---|
| Mohammadi et al. (2022) [52] | AT | → | → | → | → | ↑ In the fasted state after 12 weeks |
| RT | → | → | → | → | ↑ In the fasted state after 12 weeks | |
| Vidanage et al. (2023) [51] 1 | AT | (→) ↓: 30 min pre-meal (in the fasted state) and 30 min post-meal after 6 months | - | - | (→) ↑: 30 min pre-meal (in the fasted state) after 6 months | - |
| AT + RT | (→) ↓: 30 min pre-meal (in the fasted state) and 30 min post-meal after 6 months | - | - | (→) ↑: 30 min pre-meal (in the fasted state); 30 min and 60 min post-meal after 6 months | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konitz, C.; Schwensfeier, L.; Predel, H.-G.; Brinkmann, C. The Influence of Acute and Chronic Exercise on Appetite and Appetite Regulation in Patients with Prediabetes or Type 2 Diabetes Mellitus—A Systematic Review. Nutrients 2024, 16, 1126. https://doi.org/10.3390/nu16081126
Konitz C, Schwensfeier L, Predel H-G, Brinkmann C. The Influence of Acute and Chronic Exercise on Appetite and Appetite Regulation in Patients with Prediabetes or Type 2 Diabetes Mellitus—A Systematic Review. Nutrients. 2024; 16(8):1126. https://doi.org/10.3390/nu16081126
Chicago/Turabian StyleKonitz, Christoph, Leon Schwensfeier, Hans-Georg Predel, and Christian Brinkmann. 2024. "The Influence of Acute and Chronic Exercise on Appetite and Appetite Regulation in Patients with Prediabetes or Type 2 Diabetes Mellitus—A Systematic Review" Nutrients 16, no. 8: 1126. https://doi.org/10.3390/nu16081126
APA StyleKonitz, C., Schwensfeier, L., Predel, H.-G., & Brinkmann, C. (2024). The Influence of Acute and Chronic Exercise on Appetite and Appetite Regulation in Patients with Prediabetes or Type 2 Diabetes Mellitus—A Systematic Review. Nutrients, 16(8), 1126. https://doi.org/10.3390/nu16081126