
Bean Consumption during Childhood Is Associated with Improved Nutritional Outcomes in the First Two Years of Life


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Sample
2.2. Exposures
2.3. Nutrition Outcome Measures
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
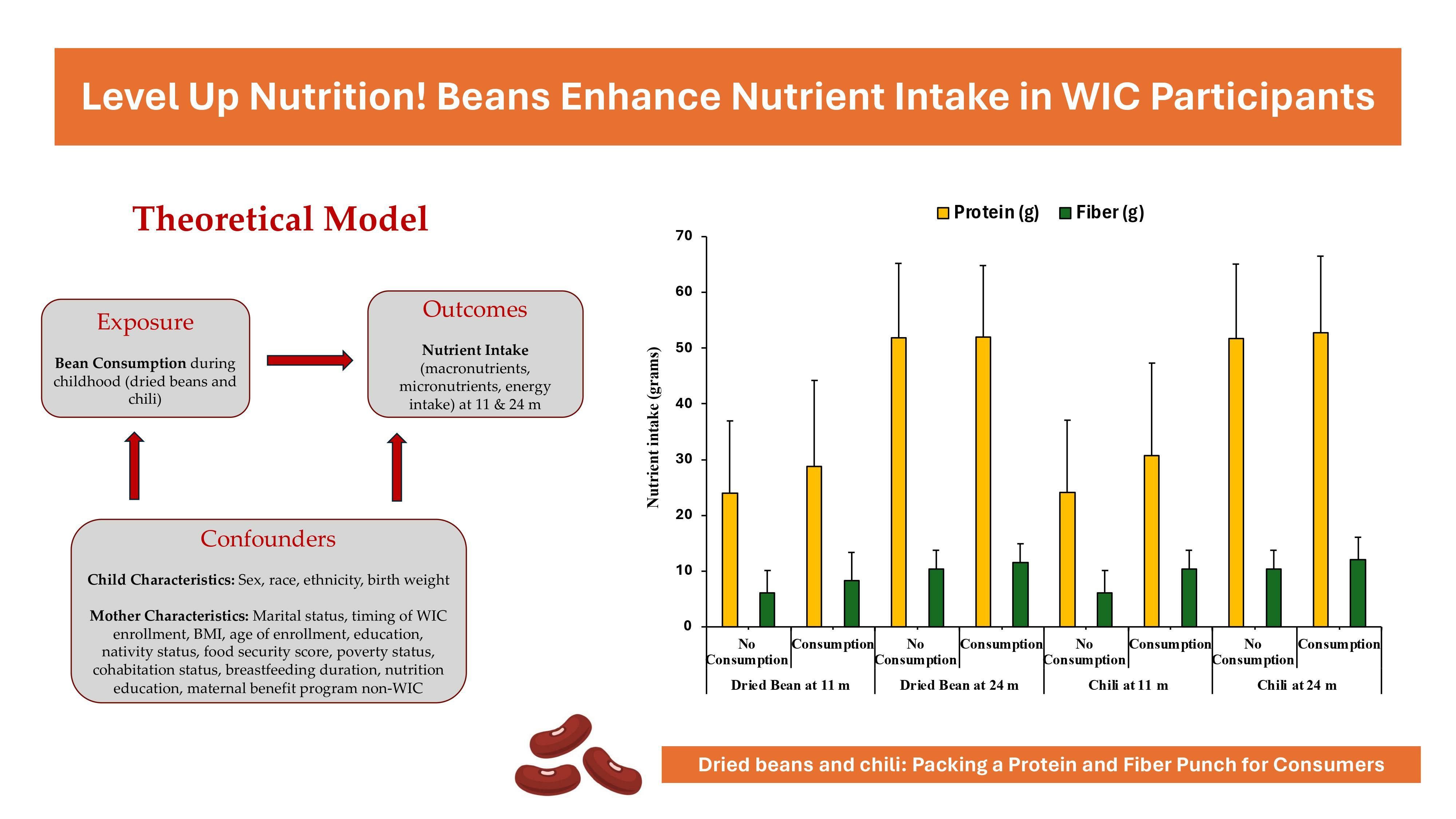
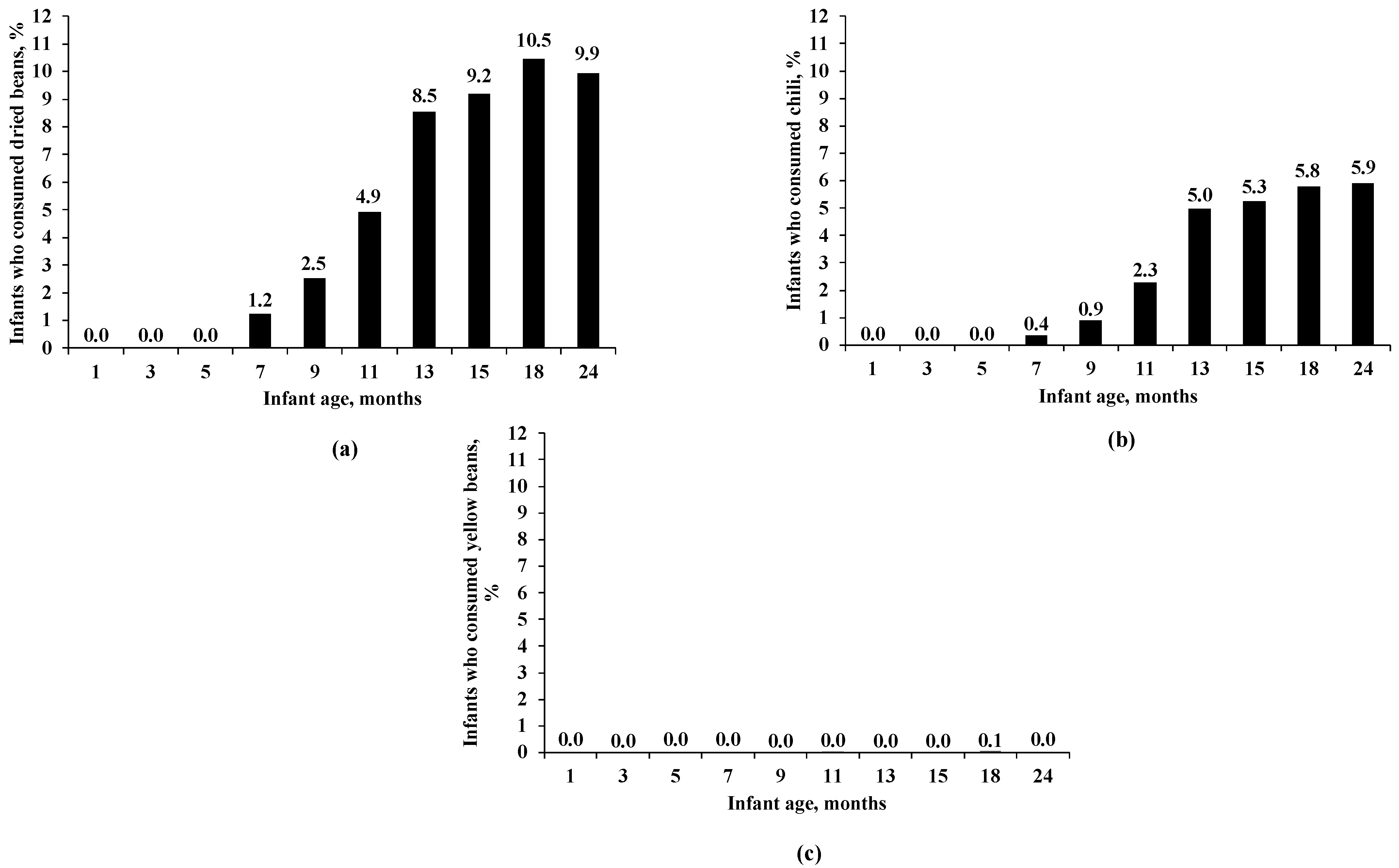
3.2. Age Trend of Bean Consumption
3.3. Socio-Demographics for Infant Dried Bean Consumption
3.4. Socio-Demographics for Infant Chili Consumption
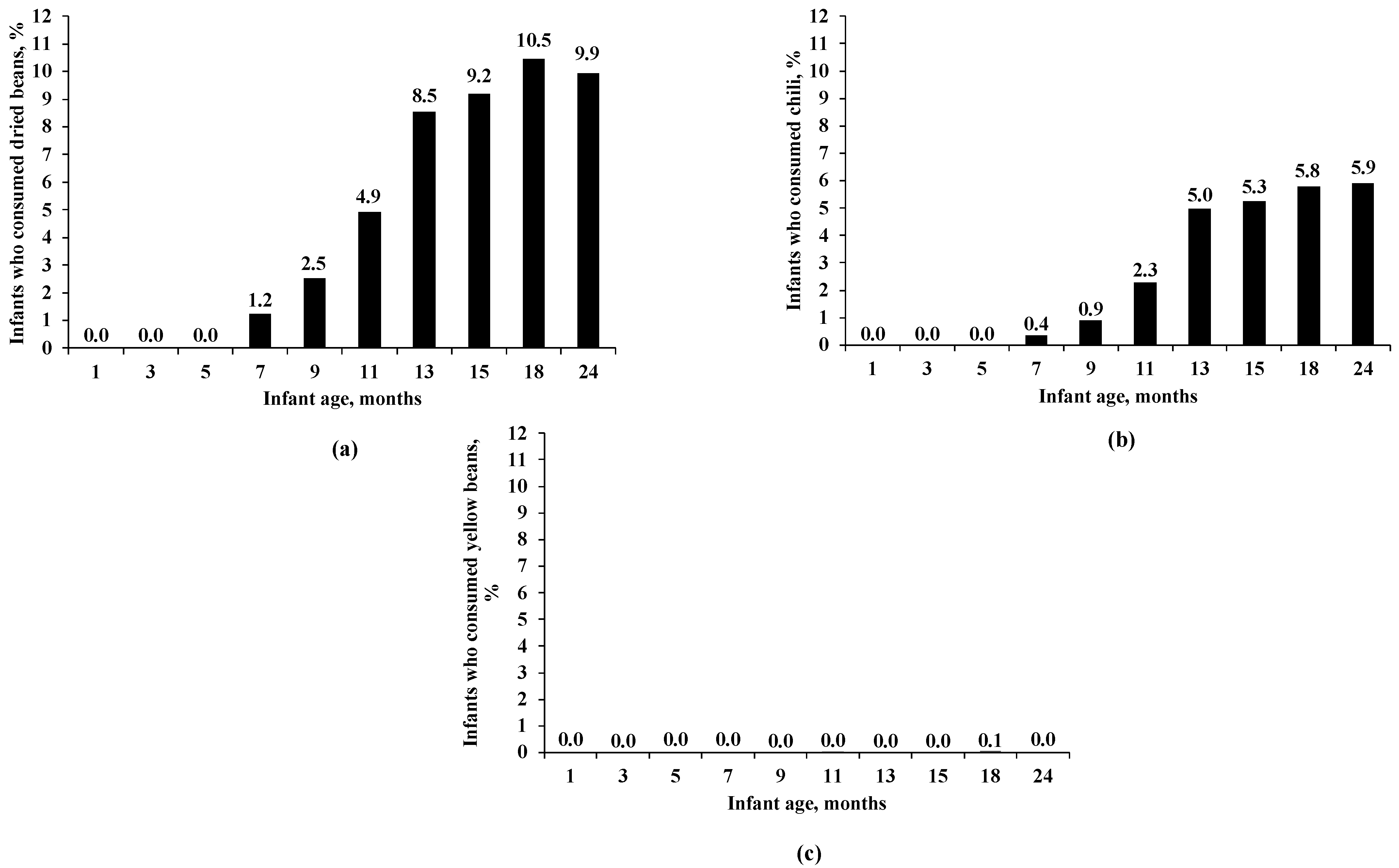
3.5. Nutrient Intake by Child’s Dried Bean Consumption
3.6. Nutritional Outcomes for Infant Chili Consumption
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Choudhary, D.; Rideout, T.C.; Cameron, C.E.; Lehman, H.K.; Oken, E.; Rifas-Shiman, S.L.; Wen, X. Egg Introduction during Infancy is Associated with Lower Fat Mass Index in Females at Early Adolescence. J. Nutr. 2023, 153, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Guglielmo, D.; Welsh, J.A. Consumption of sugars, saturated fat, and sodium among US children from infancy through preschool age, NHANES 2009–2014. Am. J. Clin. Nutr. 2018, 108, 868–877. [Google Scholar] [CrossRef] [PubMed]
- Brion, M.J.; Ness, A.R.; Davey Smith, G.; Emmett, P.; Rogers, I.; Whincup, P.; Lawlor, D.A. Sodium intake in infancy and blood pressure at 7 years: Findings from the Avon Longitudinal Study of Parents and Children. Eur. J. Clin. Nutr. 2008, 62, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Emmerik, N.E.; de Jong, F.; van Elburg, R.M. Dietary Intake of Sodium during Infancy and the Cardiovascular Consequences Later in Life: A Scoping Review. Ann. Nutr. Metab. 2020, 76, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Rousham, E.K.; Goudet, S.; Markey, O.; Griffiths, P.; Boxer, B.; Carroll, C.; Petherick, E.S.; Pradeilles, R. Unhealthy Food and Beverage Consumption in Children and Risk of Overweight and Obesity: A Systematic Review and Meta-Analysis. Adv. Nutr. 2022, 13, 1669–1696, Correction in Adv. Nutr. 2022, 13, 2064. [Google Scholar] [CrossRef] [PubMed]
- Maalouf, J.; Cogswell, M.E.; Bates, M.; Yuan, K.; Scanlon, K.S.; Pehrsson, P.; Gunn, J.P.; Merritt, R.K. Sodium, sugar, and fat content of complementary infant and toddler foods sold in the United States, 2015. Am. J. Clin. Nutr. 2017, 105, 1443–1452. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, M.E. Cryoglobulinemia in infectious mononucleosis: Quantitation and characterization of the cryoproeins. J. Lab. Clin. Med. 1968, 71, 754–765. [Google Scholar]
- Hutchinson, J.; Rippin, H.; Threapleton, D.; Jewell, J.; Kanamäe, H.; Salupuu, K.; Caroli, M.; Antignani, A.; Pace, L.; Vassallo, C. High sugar content of European commercial baby foods and proposed updates to existing recommendations. Matern. Child Nutr. 2021, 17, e13020. [Google Scholar] [CrossRef]
- Kong, K.L.; Burgess, B.; Morris, K.S.; Re, T.; Hull, H.R.; Sullivan, D.K.; Paluch, R.A. Association Between Added Sugars from Infant Formulas and Rapid Weight Gain in US Infants and Toddlers. J. Nutr. 2021, 151, 1572–1580. [Google Scholar] [CrossRef]
- Bailey, R.L.; Stang, J.S.; Davis, T.A.; Naimi, T.S.; Schneeman, B.O.; Dewey, K.G.; Donovan, S.M.; Novotny, R.; Kleinman, R.E.; Taveras, E.M.; et al. Dietary and Complementary Feeding Practices of US Infants, 6 to 12 Months: A Narrative Review of the Federal Nutrition Monitoring Data. J. Acad. Nutr. Diet. 2022, 122, 2337–2345.e1. [Google Scholar] [CrossRef]
- Albrechtsen, D.H.; Evensen, S.A.; Froland, S.; Stavem, P.; Lie, S.O.; Steinbakk, M.; Rollag, H.; Solheim, B.; Thorsby, E.; Jacobsen, A.B.; et al. Allogeneic bone marrow transplantation in Norway. Tidsskr. Nor. Laegeforen. 1987, 107, 2222–2224. [Google Scholar] [PubMed]
- Switkowski, K.M.; Aris, I.M.; Gingras, V.; Oken, E.; Young, J.G. Estimated causal effects of complementary feeding behaviors on early childhood diet quality in a US cohort. Am. J. Clin. Nutr. 2022, 115, 1105–1114. [Google Scholar] [CrossRef] [PubMed]
- D’Auria, E.; Borsani, B.; Pendezza, E.; Bosetti, A.; Paradiso, L.; Zuccotti, G.V.; Verduci, E. Complementary Feeding: Pitfalls for Health Outcomes. Int. J. Environ. Res. Public Health 2020, 17, 7931. [Google Scholar] [CrossRef] [PubMed]
- Mudryj, A.N.; Yu, N.; Aukema, H.M. Nutritional and health benefits of pulses. Appl. Physiol. Nutr. Metab. 2014, 39, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Singh, N. Pulses: An overview. J. Food Sci. Technol. 2017, 54, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, D.C.; Marinangeli, C.P.F.; Pigat, S.; Bompola, F.; Campbell, J.; Pan, Y.; Curran, J.M.; Cai, D.J.; Jaconis, S.Y.; Rumney, J. Pulse Intake Improves Nutrient Density among US Adult Consumers. Nutrients 2021, 13, 2668. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, D.C.; Lawrence, F.R.; Hartman, T.J.; Curran, J.M. Consumption of dry beans, peas, and lentils could improve diet quality in the US population. J. Am. Diet. Assoc. 2009, 109, 909–913. [Google Scholar] [CrossRef]
- Mudryj, A.N.; Yu, N.; Hartman, T.J.; Mitchell, D.C.; Lawrence, F.R.; Aukema, H.M. Pulse consumption in Canadian adults influences nutrient intakes. Br. J. Nutr. 2012, 108 (Suppl. 1), S27–S36. [Google Scholar] [CrossRef]
- Mitchell, D.C.; Webster, A.; Garrison, B. Terminology Matters: Advancing Science to Define an Optimal Pulse Intake. Nutrients 2022, 14, 655. [Google Scholar] [CrossRef]
- Marinangeli, C.P.F.; Curran, J.; Barr, S.I.; Slavin, J.; Puri, S.; Swaminathan, S.; Tapsell, L.; Patterson, C.A. Enhancing nutrition with pulses: Defining a recommended serving size for adults. Nutr. Rev. 2017, 75, 990–1006. [Google Scholar] [CrossRef]
- Tungmunnithum, D.; Drouet, S.; Lorenzo, J.M.; Hano, C. Effect of traditional cooking and in vitro gastrointestinal digestion of the ten most consumed beans from the fabaceae family in Thailand on their phytochemicals, antioxidant and anti-diabetic potentials. Plants 2021, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Harrison, G.G.; Hirschman, J.D.; Owens, T.A.; McNutt, S.W.; Sallack, L.E. WIC Infant and Toddler Feeding Practices Study: Protocol design and implementation. Am. J. Clin. Nutr. 2014, 99, 742S–746S. [Google Scholar] [CrossRef] [PubMed]
- Borger, C.; Paolicelli, C.; Sun, B.; Zimmerman, T.P.; Dixit-Joshi, S. Duration of WIC Participation and Early Feeding Practices Are Associated with Meeting the Added Sugars Recommendation at Age 3 Years. J. Nutr. Educ. Behav. 2022, 54, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.E.; Martinez, C.E.; Ritchie, L.D.; Paolicelli, C.; Reat, A.; Borger, C.; Whaley, S.E. Longer Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) participation duration is associated with higher diet quality at age 5 years. J. Nutr. 2022, 152, 1974–1982. [Google Scholar] [CrossRef] [PubMed]
- Montville, J.B.; Ahuja, J.K.; Martin, C.L.; Heendeniya, K.Y.; Omolewa-Tomobi, G.; Steinfeldt, L.C.; Anand, J.; Adler, M.E.; LaComb, R.P.; Moshfegh, A. USDA food and nutrient database for dietary studies (FNDDS), 5.0. Procedia Food Sci. 2013, 2, 99–112. [Google Scholar] [CrossRef]
- Winham, D.M.; Tisue, M.E.; Palmer, S.M.; Cichy, K.A.; Shelley, M.C. Dry Bean Preferences and Attitudes among Midwest Hispanic and Non-Hispanic White Women. Nutrients 2019, 11, 178. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Galiano, J.M.; Amezcua-Prieto, C.; Salcedo-Bellido, I.; Gonzalez-Mata, G.; Bueno-Cavanillas, A.; Delgado-Rodriguez, M. Maternal dietary consumption of legumes, vegetables and fruit during pregnancy, does it protect against small for gestational age? BMC Pregnancy Childbirth 2018, 18, 486. [Google Scholar] [CrossRef] [PubMed]
- Borger, C.; Weinfield, N.S.; Paolicelli, C.; Sun, B.; May, L. Prenatal and postnatal experiences predict breastfeeding patterns in the WIC Infant and Toddler Feeding Practices Study-2. Breastfeed. Med. 2021, 16, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, M.P.; Anderson, C.E. Differences in early childhood dietary behaviors by infant feeding type and sex. J. Nutr. 2021, 151, 2001–2009. [Google Scholar] [CrossRef]
- Thompson, H.J. The Dietary Guidelines for Americans (2020–2025): Pulses, Dietary Fiber, and Chronic Disease Risk—A Call for Clarity and Action; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2021; Volume 13, p. 4034. [Google Scholar]
- Gidding, S.S.; Dennison, B.A.; Birch, L.L.; Daniels, S.R.; Gillman, M.W.; Lichtenstein, A.H.; Rattay, K.T.; Steinberger, J.; Stettler, N.; Van Horn, L.; et al. Dietary recommendations for children and adolescents: A guide for practitioners: Consensus statement from the American Heart Association. Circulation 2005, 112, 2061–2075. [Google Scholar] [CrossRef]
- Vieira, E.D.; Gomes, A.M.; Gil, A.M.; Vasconcelos, M.W. Pulses’ benefits in children’s diets: A narrative review. J. Obes. Chronic Dis. 2021, 5, 13–22. [Google Scholar]
- Gellar, L.; Rovner, A.J.; Nansel, T.R. Whole grain and legume acceptability among youths with type 1 diabetes. Diabetes Educ. 2009, 35, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Anzman-Frasca, S.; Savage, J.S.; Marini, M.E.; Fisher, J.O.; Birch, L.L. Repeated exposure and associative conditioning promote preschool children’s liking of vegetables. Appetite 2012, 58, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Nicklaus, S. Development of food variety in children. Appetite 2009, 52, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.; Crawford, D. Family food environments as determinants of preschool-aged children’s eating behaviours: Implications for obesity prevention policy. A review. Aust. J. Nutr. Diet. 2001, 58, 19–26. [Google Scholar]
- Wiig, K.; Smith, C. The art of grocery shopping on a food stamp budget: Factors influencing the food choices of low-income women as they try to make ends meet. Public Health Nutr. 2009, 12, 1726–1734. [Google Scholar] [CrossRef]
- Henn, K.; Goddyn, H.; Olsen, S.B.; Bredie, W.L. Identifying behavioral and attitudinal barriers and drivers to promote consumption of pulses: A quantitative survey across five European countries. Food Qual. Prefer. 2022, 98, 104455. [Google Scholar] [CrossRef]
- Palmer, S.M.; Winham, D.M.; Oberhauser, A.M.; Litchfield, R.E. Socio-Ecological Barriers to Dry Grain Pulse Consumption among Low-Income Women: A Mixed Methods Approach. Nutrients 2018, 10, 1108. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Rahman, N.; Du, S.; Ramsing, R.; Sullivan, V.; Nussbaumer, E.; Love, D.; Bloem, M.W. Patterns of Legume Purchases and Consumption in the United States. Front. Nutr. 2021, 8, 732237. [Google Scholar] [CrossRef]
- Schmidt, O.P. Taxonomy of bronchitis. Prax. Pneumol. 1973, 27, 281–288. [Google Scholar]
- Teshome, G.B.; Whiting, S.J.; Green, T.J.; Mulualem, D.; Henry, C.J. Scaled-up nutrition education on pulse-cereal complementary food practice in Ethiopia: A cluster-randomized trial. BMC Public Health 2020, 20, 1437. [Google Scholar] [CrossRef] [PubMed]
- Jayalath, V.H.; de Souza, R.J.; Sievenpiper, J.L.; Ha, V.; Chiavaroli, L.; Mirrahimi, A.; Di Buono, M.; Bernstein, A.M.; Leiter, L.A.; Kris-Etherton, P.M.; et al. Effect of dietary pulses on blood pressure: A systematic review and meta-analysis of controlled feeding trials. Am. J. Hypertens. 2014, 27, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Winham, D.M.; Thompson, S.V.; Heer, M.M.; Davitt, E.D.; Hooper, S.D.; Cichy, K.A.; Knoblauch, S.T. Black Bean Pasta Meals with Varying Protein Concentrations Reduce Postprandial Glycemia and Insulinemia Similarly Compared to White Bread Control in Adults. Foods 2022, 11, 1652. [Google Scholar] [CrossRef] [PubMed]
- Bajka, B.H.; Pinto, A.M.; Perez-Moral, N.; Saha, S.; Ryden, P.; Ahn-Jarvis, J.; van der Schoot, A.; Bland, C.; Berry, S.E.; Ellis, P.R.; et al. Enhanced secretion of satiety-promoting gut hormones in healthy humans after consumption of white bread enriched with cellular chickpea flour: A randomized crossover study. Am. J. Clin. Nutr. 2022, 117, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, Y.; Fulgoni, V.L., 3rd. Bean consumption is associated with greater nutrient intake, reduced systolic blood pressure, lower body weight, and a smaller waist circumference in adults: Results from the National Health and Nutrition Examination Survey 1999–2002. J. Am. Coll. Nutr. 2008, 27, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Hermsdorff, H.H.; Zulet, M.A.; Abete, I.; Martinez, J.A. A legume-based hypocaloric diet reduces proinflammatory status and improves metabolic features in overweight/obese subjects. Eur. J. Nutr. 2011, 50, 61–69. [Google Scholar] [CrossRef]
- Davies, M.J. Anatomic features in victims of sudden coronary death. Coronary artery pathology. Circulation 1992, 85, I19–I24. [Google Scholar]

{kind=link}
{kind=link}
| N = (3039) | |
|---|---|
| Sample Characteristics * | n (%) |
| Child’s sex | |
| Male | 1549 (51.0) |
| Female | 1490 (49.0) |
| Child’s race | |
| Black or African American | 814 (27.3) |
| White | 1664 (55.8) |
| All other | 505 (16.9) |
| Child’s ethnicity | |
| Hispanic or Latino | 1245 (41.4) |
| Not Hispanic or Latino | 1763 (58.6) |
| Child’s birth weight | |
| Low | 223 (7.3) |
| Normal | 2778 (91.4) |
| High | 38 (1.3) |
| Maternal marital status | |
| Married | 950 (31.3) |
| Not married | 2089 (68.7) |
| Maternal timing of WIC enrollment | |
| 1st trimester | 969 (31.9) |
| 2nd trimester | 1205 (39.7) |
| 3rd trimester | 461 (15.2) |
| Postnatal | 404 (13.3) |
| Maternal BMI at screening | |
| Normal or underweight | 1327 (43.7) |
| Overweight | 822 (27.1) |
| Obese | 890 (29.3) |
| Maternal age of enrollment | |
| 16–19 years | 336 (11.1) |
| 20–25 years | 1243 (40.9) |
| 26 years or older | 1460 (48.0) |
| Maternal highest education | |
| 9th grade or less | 282 (9.3) |
| 10th or 11th grade | 431 (14.2) |
| 12th grade | 1140 (37.6) |
| More than 12th grade | 1179 (38.9) |
| Maternal nativity status | |
| Mother born in U.S. | 2262 (74.5) |
| Mother not born in U.S. | 776 (25.5) |
| Maternal food security score | |
| High or marginal food security | 1555 (51.2) |
| Low food security | 956 (31.5) |
| Very low food security | 528 (17.4) |
| Maternal poverty status | |
| 75% of poverty guideline or below | 1914 (63.0) |
| Above 75% but no more than 130% of poverty guideline | 826 (27.2) |
| Above 130% of poverty guideline | 299 (9.8) |
| Maternal cohabitation status | |
| Mother living with father of the baby | 1657 (54.6) |
| Mother not living with father of the baby | 1379 (45.4) |
| Maternal breastfeeding duration | |
| No breastfeeding or 0 m | 526 (17.9) |
| Greater than 0 m but ≤3 m | 1407 (47.9) |
| Greater than 3 m but ≤6 m | 340 (11.6) |
| Greater than >6 m | 665 (22.6) |
| Maternal nutrition education | |
| Received training on formula only | 552 (18.2) |
| Received training on cereal only | 289 (9.5) |
| Received training on both | 1574 (51.8) |
| Received training on neither | 549 (18.1) |
| Not applicable | 75 (2.5) |
| Maternal benefit program non-WIC | |
| Does not participate in any other benefit programs | 476 (15.7) |
| Participates in SNAP or in SNAP and other programs | 1518 (50.0) |
| Participates in other programs excluding SNAP | 1045 (34.4) |
| Dried Beans Consumed at 11 m | p-Value | Dried Beans Consumed at 24 m | p-Value | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Child’s sex | ||||
| Male | 58 (4.9) | 0.998 | 136 (10.9) | 0.123 |
| Female | 56 (4.9) | 109 (9.0) | ||
| Child’s race | ||||
| Black or African American | 7 (1.3) | <0.001 | 37 (5.2) | <0.001 |
| White | 84 (6.3) | 154 (11.8) | ||
| All other | 20 (5.1) | 47 (11.6) | ||
| Child’s ethnicity | ||||
| Hispanic or Latino | 86 (8.5) | <0.001 | 183 (18.7) | <0.001 |
| Not Hispanic or Latino | 27 (2.1) | 60 (4.1) | ||
| Child’s birth weight | ||||
| Low | 8 (4.9) | 0.454 | 12 (6.7) | 0.265 |
| Normal | 106 (5.0) | 229 (10.2) | ||
| High | 0 (0.0) | 4 (13.3) | ||
| Maternal marital status | ||||
| Married | 50 (6.8) | 0.005 | 100 (12.9) | 0.001 |
| Not married | 64 (4.1) | 145 (8.6) | ||
| Maternal timing of WIC enrollment | ||||
| 1st trimester | 43 (5.5) | 0.635 | 95 (11.9) | 0.072 |
| 2nd trimester | 43 (4.6) | 96 (9.9) | ||
| 3rd trimester | 18 (5.3) | 29 (7.9) | ||
| Postnatal | 10 (3.7) | 25 (7.7) | ||
| Maternal BMI at screening | ||||
| Normal or underweight | 47 (4.5) | 0.257 | 109 (10.3) | 0.866 |
| Overweight | 35 (6.2) | 66 (9.7) | ||
| Obese | 32 (4.6) | 70 (9.6) | ||
| Maternal age of enrollment | ||||
| 16–19 years | 12 (4.7) | 0.970 | 27 (10.5) | 0.174 |
| 20–25 years | 46 (4.9) | 84 (8.6) | ||
| 26 years or older | 56 (5.0) | 134 (10.9) | ||
| Maternal highest education | ||||
| 9th grade or less | 17 (7.5) | 0.240 | 42 (18.5) | <0.001 |
| 10th or 11th grade | 18 (5.4) | 36 (10.7) | ||
| 12th grade | 37 (4.3) | 80 (8.8) | ||
| More than 12th grade | 42 (4.7) | 86 (8.7) | ||
| Maternal nativity status | ||||
| Mother born in U.S. | 64 (3.8) | <0.001 | 115 (6.3) | <0.001 |
| Mother not born in U.S. | 50 (8.0) | 130 (20.7) | ||
| Maternal food security score | ||||
| High or marginal food security | 59 (4.9) | 0.109 | 130 (10.5) | 0.194 |
| Low food security | 43 (5.9) | 82 (10.4) | ||
| Very low food security | 12 (3.1) | 33 (7.6) | ||
| Maternal poverty status | ||||
| 75% of poverty guideline or below | 70 (4.8) | 0.737 | 154 (9.9) | 0.521 |
| Above 75% but no more than 130% | 30 (4.7) | 72 (10.7) | ||
| Above 130% of poverty guideline | 14 (6.0) | 19 (8.1) | ||
| Maternal cohabitation status | ||||
| Mother living with father of the baby | 74 (5.7) | 0.046 | 149 (11.2) | 0.024 |
| Mother not living with father of the baby | 40 (3.9) | 96 (8.5) | ||
| Maternal breastfeeding duration | ||||
| No breastfeeding or 0 m | 7 (1.9) | <0.001 | 24 (5.7) | <0.001 |
| Greater than 0 m but ≤3 m | 48 (4.4) | 98 (8.8) | ||
| Greater than 3 m but ≤6 m | 15 (5.9) | 33 (11.5) | ||
| Greater than 6 m | 42 (8.0) | 78 (13.7) | ||
| Maternal nutrition education | ||||
| Received training on formula only | 25 (5.8) | 0.718 | 50 (11.2) | 0.595 |
| Received training on cereal only | 12 (5.3) | 29 (11.8) | ||
| Received training on both | 51 (4.3) | 119 (9.4) | ||
| Received training on neither | 23 (5.6) | 43 (9.4) | ||
| Not applicable | 3 (4.5) | 4 (7.0) | ||
| Maternal benefit program non-WIC | ||||
| Did not participate in any programs | 21 (5.5) | 0.691 | 36 (9.8) | 0.001 |
| Participates in SNAP and other programs | 52 (4.5) | 98 (8.0) | ||
| Participates in programs other than SNAP | 41 (5.2) | 111 (12.9) | ||
| Chili Consumed at 11 m | p-Value | Chili Consumed at 24 m | p-Value | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Child’s sex | ||||
| Male | 22 (1.9) | 0.168 | 67 (5.4) | 0.218 |
| Female | 31 (2.7) | 79 (6.5) | ||
| Child’s race | ||||
| Black or African American | 14 (2.5) | 0.851 | 42 (5.9) | 0.538 |
| White | 29 (2.2) | 71 (5.4) | ||
| All other | 8 (2.0) | 28 (6.9) | ||
| Child’s ethnicity | ||||
| Hispanic or Latino | 38 (3.8) | <0.001 | 85 (8.7) | <0.001 |
| Not Hispanic or Latino | 14 (1.1) | 60 (4.1) | ||
| Child’s birth weight | ||||
| Low | 3 (1.8) | 0.859 | 12 (6.7) | 0.763 |
| Normal | 49 (2.3) | 133 (5.9) | ||
| High | 1 (3.3) | 1 (3.3) | ||
| Maternal marital status | ||||
| Married | 15 (2.0) | 0.569 | 37 (4.8) | 0.106 |
| Not married | 38 (2.4) | 109 (6.4) | ||
| Maternal timing of WIC enrollment | ||||
| 1st trimester | 18 (2.3) | 0.593 | 47 (5.9) | 0.798 |
| 2nd trimester | 18 (1.9) | 54 (5.5) | ||
| 3rd trimester | 11 (3.2) | 22 (6.0) | ||
| Postnatal | 6 (2.2) | 23 (7.1) | ||
| Maternal BMI at screening | ||||
| Normal or underweight | 25 (2.4) | 0.953 | 74 (7.0) | 0.133 |
| Overweight | 13 (2.3) | 33 (4.8) | ||
| Obese | 15 (2.2) | 39 (5.4) | ||
| Maternal age of enrollment | ||||
| 16–19 years | 5 (2.0) | 0.886 | 19 (7.4) | 0.562 |
| 20–25 years | 23 (2.4) | 58 (5.9) | ||
| 26 years or older | 25 (2.2) | 69 (5.6) | ||
| Maternal highest education | ||||
| 9th grade or less | 7 (3.1) | <0.001 | 19 (8.4) | <0.001 |
| 10th or 11th grade | 6 (1.8) | 18 (5.4) | ||
| 12th Grade | 11 (1.3) | 41 (4.5) | ||
| More than 12th grade | 29 (3.3) | 68 (6.9) | ||
| Maternal nativity status | ||||
| Mother born in U.S. | 31 (1.8) | 0.017 | 90 (4.9) | <0.001 |
| Mother not born in U.S. | 22 (3.5) | 55 (8.7) | ||
| Maternal food security score | ||||
| High or marginal food security | 23 (1.9) | 0.273 | 66 (5.3) | 0.425 |
| Low food security | 22 (3.0) | 53 (6.7) | ||
| Very low food security | 8 (2.0) | 27 (6.2) | ||
| Maternal poverty status | ||||
| 75% of poverty guideline or below | 35 (2.4) | 0.296 | 104 (6.7) | 0.098 |
| Above 75% but no more than 130% | 16 (2.5) | 33 (4.9) | ||
| Above 130% of poverty guideline | 2 (0.9) | 9 (3.9) | ||
| Maternal cohabitation status | ||||
| Mother living with father of the baby | 32 (2.5) | 0.503 | 72 (5.4) | 0.244 |
| Mother not living with father of the baby | 21 (2.1) | 74 (6.5) | ||
| Maternal breastfeeding duration | ||||
| No breastfeeding or 0 m | 6 (1.6) | 0.387 | 18 (4.2) | 0.045 |
| Greater than 0 m but ≤ 3 m | 23 (2.1) | 66 (5.9) | ||
| Greater than 3 m but ≤ 6 m | 9 (3.5) | 14 (4.9) | ||
| Greater than 6 m | 14 (2.7) | 47 (8.3) | ||
| Maternal nutrition education | ||||
| Received training on formula only | 12 (2.8) | 0.265 | 23 (5.2) | 0.170 |
| Received training on cereal only | 4 (1.8) | 22 (9.0) | ||
| Received training on both | 25 (2.1) | 74 (5.9) | ||
| Received training on neither | 8 (1.9) | 26 (5.7) | ||
| Not applicable | 4 (6.0) | 1 (1.8) | ||
| Maternal benefit program non-WIC | ||||
| Did not participate in any programs | 9 (2.3) | 0.943 | 22 (6.0) | 0.076 |
| Participates in SNAP and other programs | 25 (2.2) | 85 (6.9) | ||
| Participates in programs other than SNAP | 19 (2.4) | 39 (4.5) |
| Nutritional Outcomes | Dried Bean at 11 m | Dried Bean at 24 m | ||||
|---|---|---|---|---|---|---|
| No Consumption (n = 2202) | Consumption (n = 114) | p-Value | No Consumption (n = 2193) | Consumption (n = 241) | p-Value | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Energy (Kcal) | 907.01 ± 330.97 | 975.05 ± 340.89 | 0.033 | 1326.18 ± 326.31 | 1264.35 ± 316.82 | 0.005 |
| Protein (g) | 24.04 ± 12.93 | 28.79 ± 15.40 | <0.001 | 51.85 ± 13.42 | 51.97 ± 12.84 | 0.896 |
| Protein intake (% of energy) | 10.3 ± 3.3 | 11.4 ± 3.3 | 0.001 | 15.8 ± 2.5 | 16.7 ± 2.5 | <0.001 |
| Carbohydrate (g) | 122.50 ± 47.64 | 128.26 ± 47.96 | 0.209 | 176.14 ± 43.00 | 170.85 ± 45.38 | 0.072 |
| Carbohydrate intake (% of energy) | 54.1 ± 8.0 | 52.6 ± 7.3 | 0.048 | 53.5 ± 5.7 | 54.2 ± 5.7 | 0.052 |
| Total fat (g) | 36.51 ± 14.78 | 39.61 ± 14.62 | 0.029 | 47.77 ± 14.31 | 42.87 ± 13.06 | <0.001 |
| Fat intake (% of energy) | 36.4 ± 7.0 | 36.9 ± 6.6 | 0.438 | 32.3 ± 4.7 | 30.5 ± 5.1 | <0.001 |
| Fiber (g) | 6.05 ± 4.05 | 8.34 ± 5.00 | <0.001 | 10.38 ± 3.35 | 11.56 ± 3.37 | <0.001 |
| Iron (mg) | 18.00 ± 13.84 | 15.38 ± 13.18 | 0.048 | 11.78 ± 3.31 | 11.52 ± 3.27 | 0.255 |
| Potassium (mg) | 1251.84 ± 487.74 | 1357.65 ± 552.37 | 0.025 | 1967.00 ± 435.80 | 2036.85 ± 428.88 | 0.018 |
| Folate (mcg) | 154.39 ± 93.84 | 202.49 ± 119.73 | <0.001 | 307.21 ± 115.34 | 323.62 ± 116.28 | 0.036 |
| Vitamin D (mcg) | 8.02 ± 5.26 | 6.76 ± 4.47 | 0.012 | 8.18 ± 3.09 | 8.44 ± 2.97 | 0.216 |
| Magnesium (mg) | 121.07 ± 60.36 | 137.62 ± 66.77 | 0.005 | 189.16 ± 40.66 | 195.93 ± 38.68 | 0.014 |
| Nutritional Outcomes | Chili at 11 m | Chili at 24 m | ||||
|---|---|---|---|---|---|---|
| No Consumption (n = 2263) | Consumption (n = 53) | p-Value | No Consumption (n = 2292) | Consumption (n = 142) | p-Value | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Energy (Kcal) | 907.01 ± 329.87 | 1053.67 ± 379.44 | 0.002 | 1318.46 ± 325.74 | 1345.89 ± 327.65 | 0.330 |
| Protein (g) | 24.12 ± 12.97 | 30.72 ± 16.65 | <0.001 | 51.80 ± 13.34 | 52.77 ± 13.75 | 0.401 |
| Protein intake (% of energy) | 10.4 ± 3.3 | 11.3 ± 3.0 | 0.045 | 15.9 ± 2.5 | 15.8 ± 2.3 | 0.691 |
| Carbohydrate (g) | 122.34 ± 47.51 | 141.77 ± 50.31 | 0.003 | 175.21 ± 43.27 | 182.14 ± 42.74 | 0.064 |
| Carbohydrate intake (% of energy) | 54.0 ± 7.9 | 54.2 ± 7.6 | 0.891 | 53.5 ± 5.7 | 54.5 ± 5.3 | 0.038 |
| Total fat (g) | 36.55 ± 14.69 | 41.40 ± 18.11 | 0.018 | 47.34 ± 14.29 | 46.44 ± 13.86 | 0.468 |
| Fat intake (% of energy) | 36.5 ± 7.0 | 35.4 ± 7.1 | 0.281 | 32.2 ± 4.8 | 30.9 ± 4.6 | 0.003 |
| Fiber (g) | 6.10 ± 4.04 | 9.03 ± 6.38 | <0.001 | 10.40 ± 3.31 | 12.01 ± 4.00 | <0.001 |
| Iron (mg) | 17.87 ± 13.82 | 18.19 ± 14.16 | 0.868 | 11.74 ± 3.33 | 12.01 ± 3.01 | 0.348 |
| Potassium (mg) | 1252.10 ± 489.83 | 1468.23 ± 521.25 | 0.002 | 1967.01 ± 431.80 | 2085.47 ± 479.91 | 0.002 |
| Folate (mcg) | 155.59 ± 94.33 | 206.89 ± 137.76 | <0.001 | 307.76 ± 115.53 | 326.10 ± 114.26 | 0.066 |
| Vitamin D (mcg) | 7.96 ± 5.24 | 8.04 ± 5.08 | 0.910 | 8.21 ± 3.08 | 8.15 ± 2.99 | 0.807 |
| Magnesium (mg) | 121.24 ± 60.16 | 149.47 ± 79.13 | 0.001 | 188.99 ± 40.00 | 203.39 ± 46.10 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choudhary, D.; Rideout, T.C.; Millen, A.E.; Wen, X. Bean Consumption during Childhood Is Associated with Improved Nutritional Outcomes in the First Two Years of Life. Nutrients 2024, 16, 1120. https://doi.org/10.3390/nu16081120
Choudhary D, Rideout TC, Millen AE, Wen X. Bean Consumption during Childhood Is Associated with Improved Nutritional Outcomes in the First Two Years of Life. Nutrients. 2024; 16(8):1120. https://doi.org/10.3390/nu16081120
Chicago/Turabian StyleChoudhary, Divya, Todd C. Rideout, Amy E. Millen, and Xiaozhong Wen. 2024. "Bean Consumption during Childhood Is Associated with Improved Nutritional Outcomes in the First Two Years of Life" Nutrients 16, no. 8: 1120. https://doi.org/10.3390/nu16081120
APA StyleChoudhary, D., Rideout, T. C., Millen, A. E., & Wen, X. (2024). Bean Consumption during Childhood Is Associated with Improved Nutritional Outcomes in the First Two Years of Life. Nutrients, 16(8), 1120. https://doi.org/10.3390/nu16081120