
Cardiovascular Disease Risk in Individuals Following Plant-Based Dietary Patterns Compared to Regular Meat-Eaters


 and
and 
Abstract
1. Introduction
2. Materials and Methods
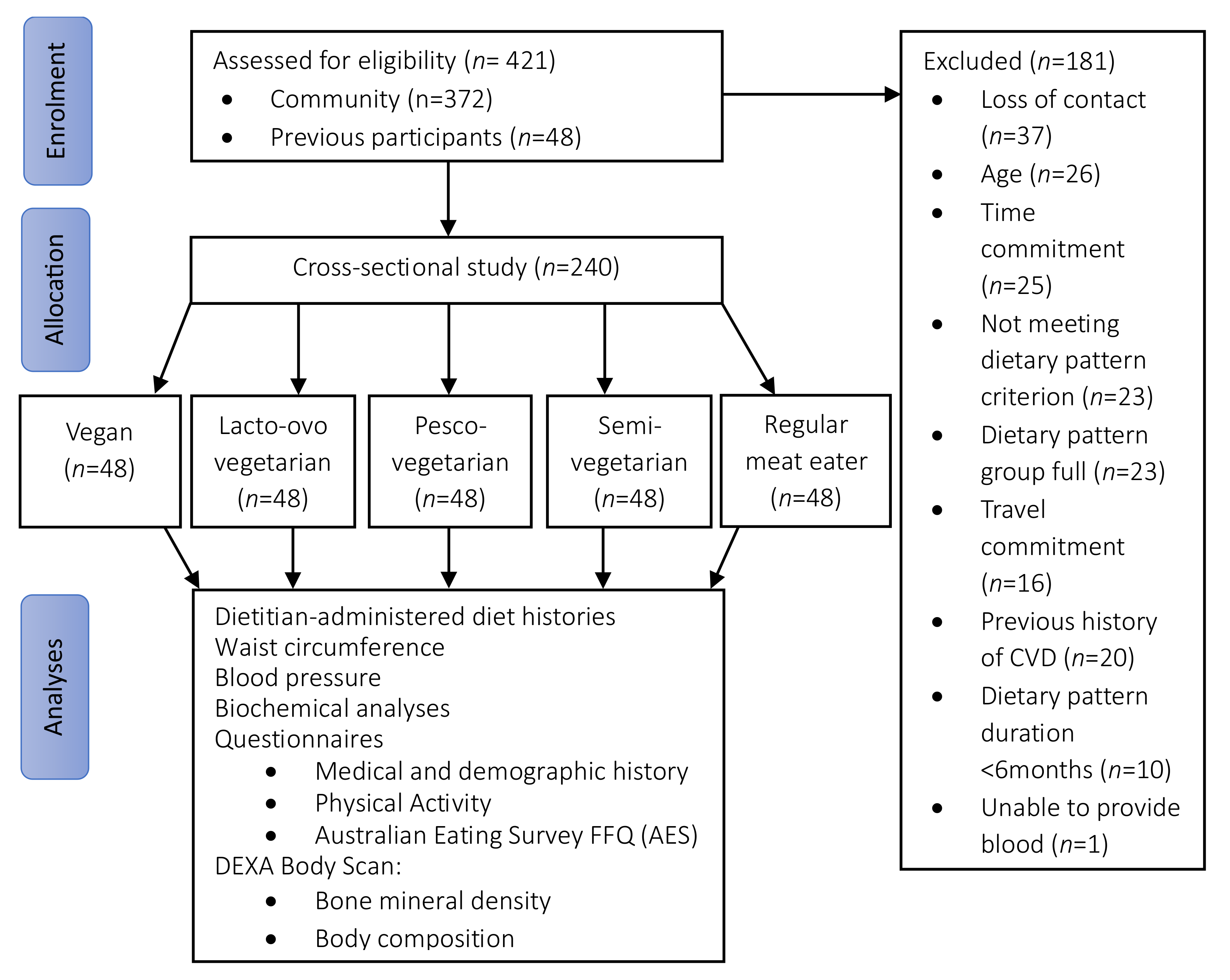
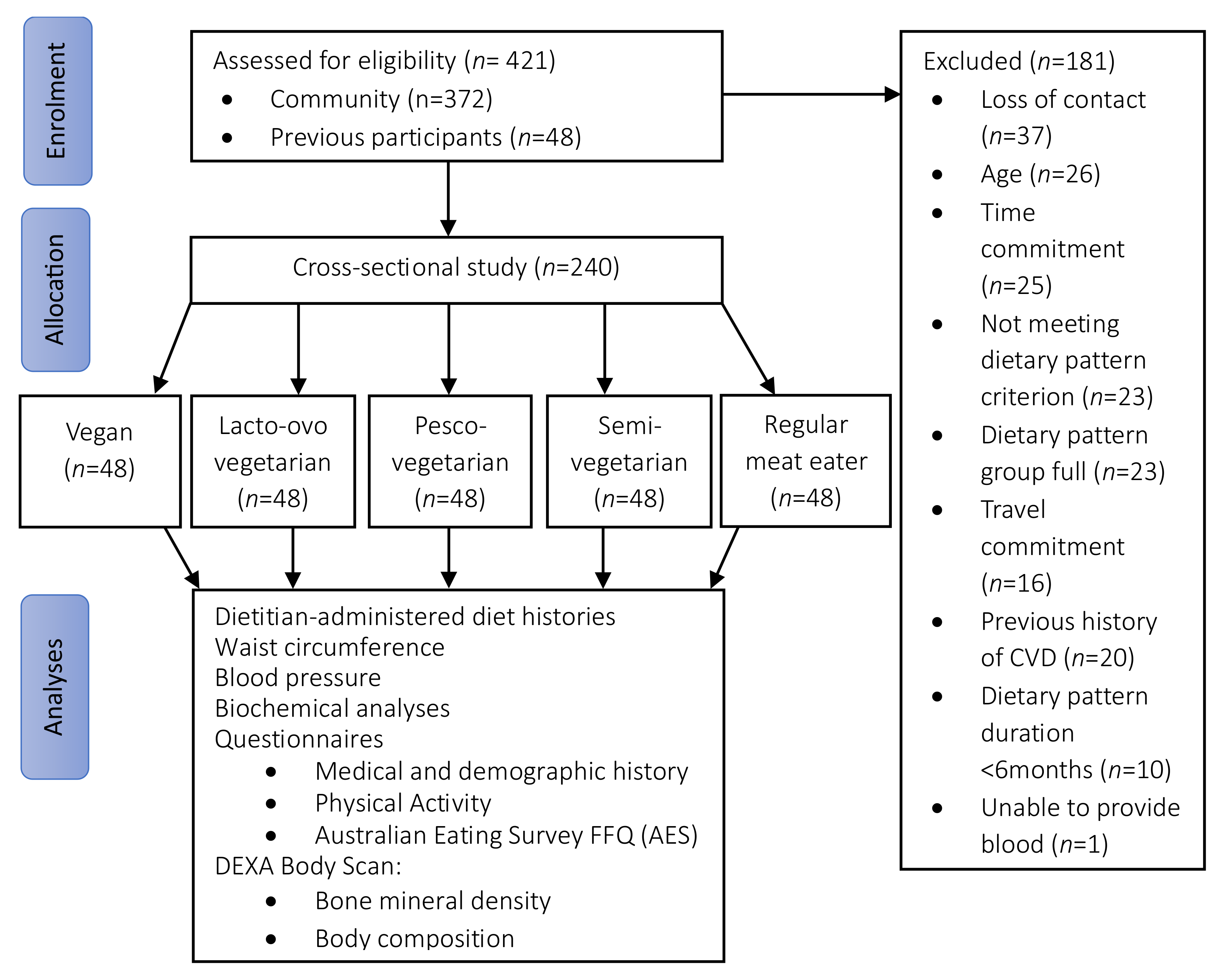
2.1. Study Population
2.2. Study Regime
2.3. Dietary Assessment
2.4. Cardiovascular Disease Risk Outcome Assessment
2.5. Covariates and Mediators
2.6. Statistical Analyses
2.7. Subgroup Analyses
3. Results
3.1. Characteristics of the Study Population
3.2. Characteristics across Dietary Pattern Groups
3.3. Cardiometabolic Disease Risk Factors
3.4. Quantitative Dietary Intake
3.5. Qualitative Dietary Intake and Diet Quality
3.6. Dietary Patterns and Predicted 5-Year and 10-Year Risks of Cardiovascular Disease
3.7. Association between CVD Risk and Frequency of Meat and Fish Intake
3.8. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roy Morgan Research. The Slow but Steady Rise of Vegetarianism in Australia: Roy Morgan; 2016. Available online: https://www.roymorgan.com/findings/the-slow-but-steady-rise-of-vegetarianism-in-australia (accessed on 30 June 2023).
- Raven, P. How Many Britons will Attempt a Vegan Diet and Lifestyle in January 2023?: YouGov UK; 2023. Available online: https://yougov.co.uk/topics/society/articles-reports/2022/12/29/how-many-britons-will-attempt-vegan-diet-and-lifes (accessed on 30 June 2023).
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef] [PubMed]
- Austin, G.; Ferguson, J.J.A.; Garg, M.L. Effects of Plant-Based Diets on Weight Status in Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2021, 13, 4099. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.Y.; Huang, C.C.; Hu, F.B.; Chavarro, J.E. Vegetarian Diets and Weight Reduction: A Meta-Analysis of Randomized Controlled Trials. J. Gen. Int. Med. 2016, 31, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Baleato, C.L.; Ferguson, J.J.A.; Oldmeadow, C.; Mishra, G.D.; Garg, M.L. Plant-Based Dietary Patterns versus Meat Consumption and Prevalence of Impaired Glucose Intolerance and Diabetes Mellitus: A Cross-Sectional Study in Australian Women. Nutrients 2022, 14, 4152. [Google Scholar] [CrossRef] [PubMed]
- Corrin, T.; Papadopoulos, A. Understanding the attitudes and perceptions of vegetarian and plant-based diets to shape future health promotion programs. Appetite 2017, 109, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Lea, E.; Worsley, A. Benefits and barriers to the consumption of a vegetarian diet in Australia. Public Health Nutr. 2003, 6, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Plant-Based Diets Are Associated with a Lower Risk of Incident Cardiovascular Disease, Cardiovascular Disease Mortality, and All-Cause Mortality in a General Population of Middle-Aged Adults. J. Am. Heart Assoc. 2019, 8, e012865. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Castro-Barquero, S.; Estruch, R.; Sacanella, E. Nutrition and Cardiovascular Health. Int. J. Mol. Sci. 2018, 19, 3988. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Larson, N.; Steffen, L.M.; Schreiner, P.J.; Gallaher, D.D.; Duprez, D.A.; Shikany, J.M.; Rana, J.S.; Jacobs, D.R., Jr. Plant-Centered Diet and Risk of Incident Cardiovascular Disease During Young to Middle Adulthood. J. Am. Heart Assoc. 2021, 10, e020718. [Google Scholar] [CrossRef]
- Jafari, S.; Hezaveh, E.; Jalilpiran, Y.; Jayedi, A.; Wong, A.; Safaiyan, A.; Barzegar, A. Plant-based diets and risk of disease mortality: A systematic review and meta-analysis of cohort studies. Crit. Rev. Food Sci. Nutr. 2022, 62, 7760–7772. [Google Scholar] [CrossRef]
- Mihrshahi, S.; Ding, D.; Gale, J.; Allman-Farinelli, M.; Banks, E.; Bauman, A.E. Vegetarian diet and all-cause mortality: Evidence from a large population-based Australian cohort-the 45 and Up Study. Prev. Med. 2017, 97, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.Y.N.; Appleby, P.N.; Bradbury, K.E.; Perez-Cornago, A.; Travis, R.C.; Clarke, R.; Key, T.J. Risks of ischaemic heart disease and stroke in meat eaters, fish eaters, and vegetarians over 18 years of follow-up: Results from the prospective EPIC-Oxford study. BMJ 2019, 366, l4897. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans 2020–2025. Available online: https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf (accessed on 8 July 2021).
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- Ferguson, J.J.A.; Oldmeadow, C.; Mishra, G.D.; Garg, M.L. Plant-based dietary patterns are associated with lower body weight, BMI and waist circumference in older Australian women. Public Health Nutr. 2022, 25, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Nutrition, Physical Activity & Obesity (NAO); Office for Prevention & Control of NCDs (MOS). Plant-based Diets and Their Impact on Health, Sustainability and the Environment: A Review of the Evidence; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Ferguson, J.J.A.; Austin, G.; Oldmeadow, C.; Garg, M.L. Plant-Based Dietary Patterns and Cardiovascular Disease Risk in Australians: Protocol for a Cross-Sectional Study. Nutrients 2023, 15, 2850. [Google Scholar] [CrossRef] [PubMed]
- EatForHealth. Australian Guide to Healthy Eating: Australian Goverment National Health and Medical Researcg Council. 2013. Available online: https://www.eatforhealth.gov.au/guidelines/australian-guide-healthy-eating (accessed on 23 October 2023).
- Collins, C.E.; Boggess, M.M.; Watson, J.F.; Guest, M.; Duncanson, K.; Pezdirc, K.; Rollo, M.; Hutchesson, M.J.; Burrows, T.L. Reproducibility and comparative validity of a food frequency questionnaire for Australian adults. Clin. Nutr. 2014, 33, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Shrier, I.; Platt, R.W. Reducing bias through directed acyclic graphs. BMC Med. Res. Methodol. 2008, 8, 70. [Google Scholar] [CrossRef]
- Australian Chronic Disease Prevention Alliance (ACDPA). Australian Absolute Cardiovascular Disease Risk Calculator 2012. Available online: https://www.cvdcheck.org.au/ (accessed on 20 October 2023).
- National Vascular Disease Prevention Alliance. Guidelines for the Management of Absolute Cardiovascular Disease Risk; Stroke Foundation: Melbourne, Australia, 2012. [Google Scholar]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef]
- Lu, Y.; Hajifathalian, K.; Ezzati, M.; Woodward, M.; Rimm, E.B.; Danaei, G. Metabolic mediators of the effects of body-mass index, overweight, and obesity on coronary heart disease and stroke: A pooled analysis of 97 prospective cohorts with 1·8 million participants. Lancet 2014, 383, 970–983. [Google Scholar] [PubMed]
- Australian Government National Health and Medical Research Council. Australian Guidelines to Reduce Health Risks from Drinking Alcohol Canberra; National Health & Medical Research Council: Canberra, Australia, 2009. [Google Scholar]
- Alcohol Guidlines: Dietitians Australia. 2013. Available online: https://www.eatforhealth.gov.au/ (accessed on 8 July 2023).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Body Mass Index (BMI) and Waist Measurement: Australian Goverment, Department of Health and Aged Care. 2021. Available online: https://www.health.gov.au/topics/overweight-and-obesity/bmi-and-waist (accessed on 9 September 2023).
- So, J.H.; Lee, J.K.; Shin Jy Park, W. Risk of Cardiovascular Disease Using Framingham Risk Score in Korean Cancer Survivors. Korean J. Fam. Med. 2016, 37, 235–241. [Google Scholar] [CrossRef]
- Imai, K.; Keele, L.; Tingley, D. A general approach to causal mediation analysis. Psychol. Methods 2010, 15, 309–334. [Google Scholar] [CrossRef] [PubMed]
- Dybvik, J.S.; Svendsen, M.; Aune, D. Vegetarian and vegan diets and the risk of cardiovascular disease, ischemic heart disease and stroke: A systematic review and meta-analysis of prospective cohort studies. Eur. J. Nutr. 2023, 62, 51–69. [Google Scholar] [CrossRef] [PubMed]
- Quek, J.; Lim, G.; Lim, W.H.; Ng, C.H.; So, W.Z.; Toh, J.; Pan, X.H.; Chin, Y.H.; Muthiah, M.D.; Chan, S.P.; et al. The Association of Plant-Based Diet with Cardiovascular Disease and Mortality: A Meta-Analysis and Systematic Review of Prospect Cohort Studies. Front. Cardiovasc. Med. 2021, 8, 756810. [Google Scholar] [CrossRef] [PubMed]
- Gan, Z.H.; Cheong, H.C.; Tu, Y.K.; Kuo, P.H. Association between Plant-Based Dietary Patterns and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Nutrients 2021, 13, 3952. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Yang, B.; Zheng, J.; Li, G.; Wahlqvist, M.L.; Li, D. Cardiovascular disease mortality and cancer incidence in vegetarians: A meta-analysis and systematic review. Ann. Nutr. Metab. 2012, 60, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Petrea, R.E.; Beiser, A.S.; Seshadri, S.; Kelly-Hayes, M.; Kase, C.S.; Wolf, P.A. Gender differences in stroke incidence and poststroke disability in the Framingham heart study. Stroke 2009, 40, 1032–1037. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, G.; Tartarone, A.; Lerose, R.; Lalinga, A.V.; Capobianco, A.M. Cardiovascular risk of smoking and benefits of smoking cessation. J. Thorac. Dis. 2020, 12, 3866–3876. [Google Scholar] [CrossRef] [PubMed]
- Threapleton, D.E.; Greenwood, D.C.; Evans, C.E.L.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Cade, J.E.; Gale, C.P.; Burley, V.J. Dietary fibre intake and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ Br. Med. J. 2013, 347, f6879. [Google Scholar] [CrossRef]
- Australian Government NHaMRC. Nutrient Reference Values: Australian Goverment 2006. Available online: https://www.eatforhealth.gov.au/nutrient-reference-values/nutrients/ (accessed on 18 September 2023).
- de Souza, R.J.; Mente, A.; Maroleanu, A.; Cozma, A.I.; Ha, V.; Kishibe, T.; Uleryk, E.; Schunemann, H.; Beyene, J.; Anand, S.S. Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: Systematic review and meta-analysis of observational studies. BMJ 2015, 351, h3978. [Google Scholar] [CrossRef]
- Hooper, L.; Martin, N.; Jimoh, O.F.; Kirk, C.; Foster, E.; Abdelhamid, A.S. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst. Rev. 2020, 5, Cd011737. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferré, M.; Babio, N.; Martínez-González, M.A.; Corella, D.; Ros, E.; Martín-Peláez, S.; Estruch, R.; Aros, F.; Gomez-Garcia, E.; Fiol, M.; et al. Dietary fat intake and risk of cardiovascular disease and all-cause mortality in a population at high risk of cardiovascular disease. Am. J. Clin. Nutr. 2015, 102, 1563–1573. [Google Scholar] [CrossRef] [PubMed]
- Ander, B.P.; Dupasquier, C.M.; Prociuk, M.A.; Pierce, G.N. Polyunsaturated fatty acids and their effects on cardiovascular disease. Exp. Clin. Cardiol. 2003, 8, 164–172. [Google Scholar] [PubMed]
- Ferguson, J.J.A.; Dias, C.B.; Garg, M.L. Omega-3 Polyunsaturated Fatty Acids and Hyperlipidaemias. In Omega-3 Fatty Acids: Keys to Nutritional Health; Hegde, M.V., Zanwar, A.A., Adekar, S.P., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 67–78. [Google Scholar]
- Wang, T.; Kroeger, C.M.; Cassidy, S.; Mitra, S.; Ribeiro, R.V.; Jose, S.; Masedunskas, A.; Senior, A.M.; Fontana, L. Vegetarian Dietary Patterns and Cardiometabolic Risk in People with or at High Risk of Cardiovascular Disease: A Systematic Review and Meta-analysis. JAMA Netw. Open 2023, 6, e2325658. [Google Scholar] [CrossRef]
- Koch, C.A.; Kjeldsen, E.W.; Frikke-Schmidt, R. Vegetarian or vegan diets and blood lipids: A meta-analysis of randomized trials. Eur. Heart J. 2023, 44, 2609–2622. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Barnard, N.D.; Levin, S.M.; Watanabe, M. Vegetarian diets and glycemic control in diabetes: A systematic review and meta-analysis. Cardiovasc. Diagn. Ther. 2014, 4, 373–382. [Google Scholar] [PubMed]
- McMacken, M.; Shah, S. A plant-based diet for the prevention and treatment of type 2 diabetes. J. Geriatr. Cardiol. 2017, 14, 342–354. [Google Scholar] [PubMed]
- Shi, W.; Huang, X.; Schooling, C.M.; Zhao, J.V. Red meat consumption, cardiovascular diseases, and diabetes: A systematic review and meta-analysis. Eur. Heart J. 2023, 44, 2626–2635. [Google Scholar] [CrossRef]
- Foundation, H. Meat & Heart Healthy Eatin: Dietary Position Statement: The Australian Heart Foundation; 2019. Available online: www.heartfoundation.org.au (accessed on 16 August 2023).
- Nohr, E.A.; Liew, Z. How to investigate and adjust for selection bias in cohort studies. Acta Obstet. Gynecol. Scand. 2018, 97, 407–416. [Google Scholar] [CrossRef]

{kind=link}
| Times per Week Consumed | Vegan | Lacto-Ovo Vegetarian | Pesco-Vegetarian | Semi-Vegetarian | Regular Meat-Eater |
|---|---|---|---|---|---|
| Red meats | 0 | 0 | 0 | 0 or <2 | 0 or ≥7 |
| White meat/poultry | 0 | 0 | 0 | 0 or <2 | 0 or ≥7 |
| Processed/cured meats | 0 | 0 | 0 | 0 or <2 | 0 or ≥7 |
| Seafood/fish | 0 | 0 | ≥1 | 0 or <2 | 0 or ≥7 |
| Total of above categories | 0 | 0 | ≥1 | 1 to ≤2 | ≥7 |
| Usual eating habits: | |||||
| Animal-based dairy | 0 | Yes | n/a | n/a | n/a |
| Eggs | 0 | Yes | n/a | n/a | n/a |
| Total Sample (n = 240) | Vegan (n = 48) | Lacto-Ovo Vegetarian (n = 48) | Pesco-Vegetarian (n = 48) | Semi-Vegetarian (n = 48) | Regular Meat-Eater (n = 48) | p | |
|---|---|---|---|---|---|---|---|
| Women | 186 (77.5%) | 34 (70.0%) | 36 (75.0%) | 39 (81.3%) | 40 (83.3%) | 37 (77.1%) | 0.625 |
| Age (yrs) | 53.8 ± 10.3 | 47.8 ± 10.0 a | 53.7 ± 10.0 b | 55.8 ± 11.0 b | 55.2 ± 8.7 b | 56.5 ± 9.7 b | <0.001 |
| Ethnicity | |||||||
| Oceanian | 110 (45.8%) | 23 (47.9%) | 20 (41.7%) | 21 (43.8%) | 19 (39.6%) | 27 (56.3%) | 0.514 |
| European 1 | 66 (27.5%) | 15 (31.3%) | 14 (29.2%) | 10 (20.8%) | 14 (29.2%) | 13 (27.1%) | 0.809 |
| Other 1 | 64 (25.7%) | 10 (20.9%) | 14 (29.1%) | 17 (35.4%) | 15 (31.3%) | 8 (16.7%) | 0.238 |
| Height (cm) | 167.8 ± 9.1 | 170.1 ± 9.5 | 168.4 ± 10.2 | 167.2 ± 7.8 | 165.3 ± 9.7 | 168 ± 7.7 | 0.120 |
| Weight (kg) | 69.1 ± 13.3 | 70.4 ± 13.5 | 69.9 ± 13.4 | 67.6 ± 11.4 | 66.5 ± 14.4 | 71.25 ± 13.5 | 0.358 |
| Overweight or obese | 100 (41.7%) | 17 (35.4%) | 23 (48.0%) | 20 (41.7%) | 16 (33.3%) | 24 (50.0%) | 0.375 |
| Higher education | 42 (88.3%) | 42 (87.5%) | 41 (85.4%) | 44 (91.7%) | 41 (85.4%) | 44 (91.7%) | 0.767 |
| Retired/not working | 62 (25.8%) | 4 (8.3%) | 11 (22.9%) | 16 (33.3%) | 17 (35.4%) | 14 (29.2%) | 0.010 |
| Physical Activity (MET) | 5424 ± 5243 | 5775 ± 4036 | 6984 ± 8783 | 4909 ± 4101 | 4393 ± 3534 | 5060 ± 3600 | 0.143 |
| Current Smoker | 15 (6.3%) | 5 (10.4%) | 3 (6.3%) | 1 (2.1%) | 3 (6.3%) | 3 (6.3%) | 0.617 |
| Family History of CVD | 111 (46.3%) | 19 (39.6%) | 23 (47.9%) | 27 (56.3%) | 21 (43.8%) | 21 (43.8%) | 0.894 |
| Dietary pattern duration (yrs) | 16.5 ± 1.2 | 6.8 ± 7.7 a | 16.7 ± 14.1 b | 15.6 ± 14.7 a,b | 11.2 ± 13.8 a,b | 32.1 ± 24.7 c | <0.001 |
| Alcohol intake 2 | |||||||
| >4 drinks per month 2 | 50 (20.8%) | 8 (16.7%) | 11 (22.9%) | 12 (25.0%) | 10 (20.8%) | 9 (18.8%) | 0.917 |
| <2 alcohol free days/wk | 20 (8.3%) | 0 | 6 (12.5%) | 6 (12.5%) | 1 (2.1%) | 7 (14.6%) | 0.005 |
| Medication and Supplement use (%) 3 | |||||||
| HRT 4 | 21 (8.8) | 2 (4.2) | 5 (10.4) | 5 (10.4) | 4 (8.3) | 5 (10.4) | 0.724 |
| OHA | 2 (0.8) | 0 | 0 | 0 | 1 (2.1) | 1 (2.1) | 1.000 |
| Antihypertensive | 15 (6.3) | 1 (2.1) | 3 (6.3) | 6 (12.5) | 1 (2.1) | 4 (8.3) | 0.199 |
| Lipid lowering agent | 8 (3.3) | 0 | 1 (2.1) | 2 (4.2) | 3 (6.3) | 2 (4.2) | 0.653 |
| N-3 PUFA 5 | 27 (11.3) | 3 (6.3) | 7 (14.5) | 4 (8.3) | 2 (4.2) | 11 (22.9) | 0.035 |
| EPA/DHA | 24 (10.0) | 2 (4.2) | 5 (10.4) | 4 (8.3) | 2 (4.2) | 11 (22.9) | 0.025 |
| ALA | 3 (1.3) | 1 (2.1) | 2 (4.2) | 0 | 0 | 0 | 0.514 |
| Vitamin D | 70 (29.2) | 14 (29.2) | 16 (33.3) | 19 (39.6) | 12 (25.0) | 9 (18.8) | 0.349 |
| Variables (mmol/L) | Total Sample (n = 240) | Vegan (n = 48) | Lacto-Ovo Vegetarian (n = 48) | Pesco-Vegetarian (n = 48) | Semi-Vegetarian (n = 48) | Regular Meat-Eater (n = 48) | p |
|---|---|---|---|---|---|---|---|
| Hypertension 1 | 11 (4.6%) | 0 | 3 (6.3%) | 3 (6.3%) | 1 (2.1%) | 4 (8.3%) | 0.261 |
| T2D 1 | 2 (0.8%) | 0 | 0 | 0 | 1 (2.1%) | 1 (2.1%) | 1.000 |
| Hyperlipidaemia 1 | 9 (3.8%) | 1 (2.1%) | 2 (4.2%) | 2 (4.2%) | 2 (4.2%) | 1 (4.2%) | 0.910 |
| SBP (mm Hg) | 116.0 ± 14.7 | 114.6 ± 12.3 | 116.5 ± 14.6 | 114.5 ± 15.4 | 115.3 ± 12.2 | 119.0 ± 19.0 | 0.576 |
| DBP (mm Hg) | 72.2 ± 9.5 | 71.1 ± 9.6 | 72.4 ± 8.6 | 71.0 ± 9.1 | 72.5 ± 8.6 | 74.1 ± 11.3 | 0.534 |
| Total cholesterol | 5.2 ± 1.0 | 4.6 ± 0.9 a | 5.4 ± 1.1 b | 5.5 ± 1.0 b | 5.2 ± 0.7 b | 5.5 ± 0.8 b | <0.001 |
| LDL-C | 3.2 ± 0.8 | 2.7 ± 0.7 a | 3.3 ± 0.9 b | 3.4 ± 0.8 b | 3.1 ± 0.7 a,b | 3.4 ± 0.7 b | <0.001 |
| HDL-C | 1.6 ± 0.4 | 1.4 ± 0.3 | 1.6 ± 0.4 | 1.7 ± 0.4 | 1.6 ± 0.4 | 1.6 ± 0.4 | 0.070 |
| Non-HDL-C | 3.7 ± 0.9 | 3.2 ± 0.8 a | 3.8 ± 1.0 b | 3.8 ± 0.9 b | 3.6 ± 0.8 a,b | 3.9 ± 0.8 b | <0.001 |
| TG | 1.1 ± 0.6 | 1.1 ± 0.5 | 1.2 ± 0.6 | 1.0 ± 0.1 | 1.1 ± 0.6 | 1.1 ± 0.5 | 0.439 |
| FBG | 4.7 ± 0.7 | 4.5 ± 0.5 a | 4.6 ± 0.6 a,b | 4.8 ± 0.6 a,b | 4.8 ± 1.0 a,b | 4.9 ± 0.8 b | 0.034 |
| LFTs (U/L) 2 ALT AST GGT | 23.8 ± 12.7 26.1 ± 11.7 19.8 ± 15.1 | 25 ± 13.0 26.9 ± 7.9 19.3 ± 20.5 | 25.3 ± 20.6 28.2 ± 23.1 19.6 ± 13.0 | 22.5 ± 7.8 24.7 ± 5.4 18.2 ± 8.4 | 21.6 ± 7.3 24.6 ± 5.4 18.0 ± 7.8 | 24.8 ± 9.8 26.1 ± 5.9 23.8 ± 20.3 | 0.493 0.487 0.325 |
| Nutrient/Food Component (per/Day) | Total Sample (n = 240) | Vegan (n = 48) | Lacto-ovo Vegetarian (n = 48) | Pesco-Vegetarian (n = 48) | Semi-Vegetarian (n = 48) | Regular Meat-Eater (n = 48) | p |
|---|---|---|---|---|---|---|---|
| Quantitative data | |||||||
| Energy (kJ) | 9957 ± 2712 | 9784 ± 3254 | 9709.3 ± 3325 | 9013 ± 2284 | 9631 ± 2501 | 9491 ± 2304 | 0.506 |
| Protein (%) 1 | 16.4% ± 4.1 | 15.4% ± 3.6 a,b | 14.8% ± 4.2 a | 16.8% ± 3.2 b | 15.4% ± 2.8 a,b | 19.8% ± 4.5 c | <0.001 |
| Carbohydrate (%) 1 | 40.2% ± 9.4 | 43.9% ± 8.4 a | 41.3% ± 8.9 a,b | 37.9% ± 8.9 b,c | 42.3% ± 8.7 a,b | 35.8% ± 9.9 c | <0.001 |
| Total fat (%) 1 | 37.3% ± 8.1 | 35.2% ± 8.4 | 38.2% ± 8.4 | 38.6% ± 7.8 | 36.5% ± 7.1 | 33.2% ± 14.6 | 0.227 |
| Saturated (g) | 28.6 ± 13.2 | 23.3 ± 11.2 a | 28.4 ± 13.9 a,b | 27.8 ± 13.3 a,b | 30.4 ± 11.1 a,b | 33.2 ± 14.6 b | 0.003 |
| Trans fats (g) | 1.0 ± 0.6 | 0.5 ± 0.7 a | 0.8 ± 0.5 a | 1.0 ± 0.6 b | 1.0 ± 0.6 b | 1.2 ± 0.6 b | <0.001 |
| MUFAs (g) | 38.7 ± 15.1 | 37.0 ± 15.6 | 40.1 ± 15.8 | 39.9 ± 16.1 | 37.7 ± 14.6 | 39.1 ± 13.9 | 0.835 |
| PUFAs (g) | 20.1 ± 10.3 | 25.8 ± 13.6 a | 21.2 ± 10.0 a,b | 18.3 ± 7.4 b | 18.8 ± 9.8 b | 15.8 ± 6.8 b | <0.001 |
| Cholesterol (mg) | 143.1 ± 136.5 | 33.6 ± 92.1 a | 98.2 ± 120.8 a,c | 157.9 ± 108.2 b | 155.7 ± 110.6 b,c | 270.2 ± 128.6 d | <0.001 |
| Dietary fibre (g) | 45.3 ± 20.8 | 58.0 ± 18.8 a | 50.4 ± 29.7 a | 41.5 ± 13.6 b,c | 44.3 ± 16.9 b | 32.5 ± 11.0 c | <0.001 |
| Alcohol (g) | 5.2 ± 10.1 | 1.8 ± 4.3 a | 3.5 ± 7.1 a | 7.2 ± 12.0 a,b | 4.1 ± 7.8 a,b | 9.4 ± 14.4 b | 0.001 |
| Qualitative data | |||||||
| Vegetables | 5.9 ± 2.4 | 6.3 ± 2.5 | 6.2 ± 2.6 | 5.9 ± 2.1 | 5.9 ± 2.1 | 5.0 ± 2.6 | 0.081 |
| Grains | 2.7 ± 1.3 | 2.7 ± 1.1 | 2.6 ± 1.3 | 2.8 ± 1.5 | 2.7 ± 1.3 | 2.6 ± 1.5 | 0.907 |
| Fruit | 3.1 ± 1.7 | 3.8 ± 2.1 a | 3.0 ± 1.3 a,b | 3.0 ± 1.6 a,b | 3.1 ± 1.5 a,b | 2.7 ± 1.6 b | 0.015 |
| Protein-rich foods 2 | 1.9 ± 0.9 | 1.5 ± 0.7 a | 1.3 ± 0.5 a | 2.0 ± 0.6 b | 2.0 ± 1.0 a,b | 2.7 ± 0.7 c | <0.001 |
| Meats/seafood 2 | 0.6 ± 0.8 | 0.0 ± 0.0 a | 0.0 ± 0.0 a | 0.6 ± 0.4 b | 0.6 ± 0.7 a,d | 1.7 ± 0.6 c | <0.001 |
| Legumes/nuts | 1.1 ± 0.6 | 1.5 ± 0.7 a | 1.1 ± 0.5 b | 1.1 ± 0.5 b | 1.0 ± 0.5 b | 0.6 ± 0.5 c | <0.001 |
| Dairy 2 | 1.6 ± 1.3 | 0.0 ± 0.0 a | 1.6 ± 1.5 b | 1.8 ± 1.0 b | 1.7 ± 1.3 b | 2.0 ± 1.4 b | <0.001 |
| Discretionary 3 choices | 1.7 ± 1.2 | 1.3 ± 1.0 a | 1.6 ± 1.1 a | 1.6 ± 1.1 a | 1.8 ± 1.2 a,b | 2.3 ± 1.5 b | 0.002 |
| Comparisons to RME | 5-Year CVD Risk Score 1 | 10-Year CVD Risk Score 2 | ||
|---|---|---|---|---|
| Model | Crude | Adjusted | Crude | Adjusted |
| Vegan | ||||
| β | −2.40 * | −0.98 | −3.20 * | −0.87 |
| SE | 0.88 | 0.58 | 1.20 | 0.57 |
| 95% CI | −4.12, −0.67 | −2.11, 0.15 | −5.55, −0.85 | −1.20, 0.25 |
| Laco-ovo vegetarian diet | ||||
| β | −0.67 | −0.17 | −0.95 | −0.15 |
| SE | 0.93 | 0.68 | 1.31 | 0.68 |
| 95% CI | −2.48, 1.15 | −1.50, 1.16 | −3.51, 1.61 | −1.48, 1.18 |
| Pesco-vegetarian diet | ||||
| β | −0.65 | −0.14 | −0.47 | 0.37 |
| SE | 1.02 | 0.66 | 1.45 | 0.76 |
| 95% CI | −2.65, 1.36 | −1.43, 1.14 | −3.30, 2.37 | −1.11, 1.85 |
| Semi-vegetarian diet | ||||
| β | −1.25 | −0.69 | −1.55 | −0.53 |
| SE | 0.91 | 0.56 | 1.27 | 0.72 |
| 95% CI | −3.05, 0.55 | −1.79, 0.41 | 4.04, 0.94 | −1.94, 0.88 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Austin, G.; Ferguson, J.J.A.; Eslick, S.; Oldmeadow, C.; Wood, L.G.; Garg, M.L. Cardiovascular Disease Risk in Individuals Following Plant-Based Dietary Patterns Compared to Regular Meat-Eaters. Nutrients 2024, 16, 1063. https://doi.org/10.3390/nu16071063
Austin G, Ferguson JJA, Eslick S, Oldmeadow C, Wood LG, Garg ML. Cardiovascular Disease Risk in Individuals Following Plant-Based Dietary Patterns Compared to Regular Meat-Eaters. Nutrients. 2024; 16(7):1063. https://doi.org/10.3390/nu16071063
Chicago/Turabian StyleAustin, Grace, Jessica J. A. Ferguson, Shaun Eslick, Christopher Oldmeadow, Lisa G. Wood, and Manohar L. Garg. 2024. "Cardiovascular Disease Risk in Individuals Following Plant-Based Dietary Patterns Compared to Regular Meat-Eaters" Nutrients 16, no. 7: 1063. https://doi.org/10.3390/nu16071063
APA StyleAustin, G., Ferguson, J. J. A., Eslick, S., Oldmeadow, C., Wood, L. G., & Garg, M. L. (2024). Cardiovascular Disease Risk in Individuals Following Plant-Based Dietary Patterns Compared to Regular Meat-Eaters. Nutrients, 16(7), 1063. https://doi.org/10.3390/nu16071063