
Nutrition-Related Knowledge, Attitudes, Practices, and Anemia Status of Lactating Mothers in Bukavu, Democratic Republic of the Congo—A Cross-Sectional Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
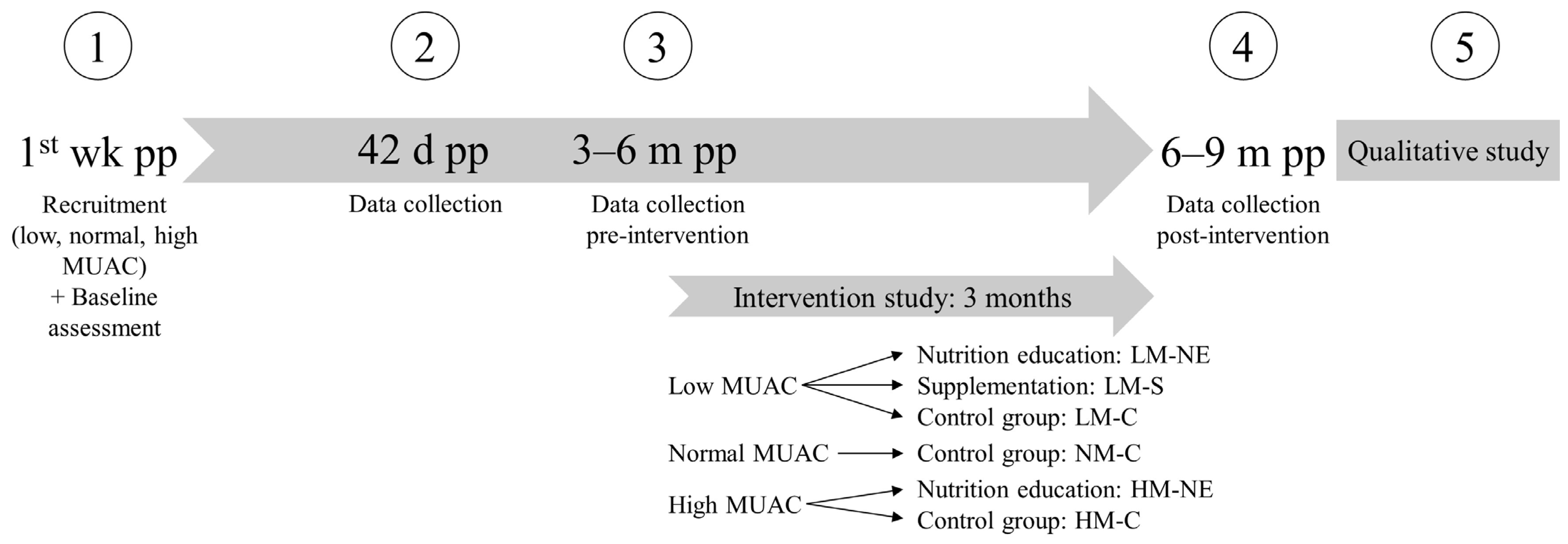
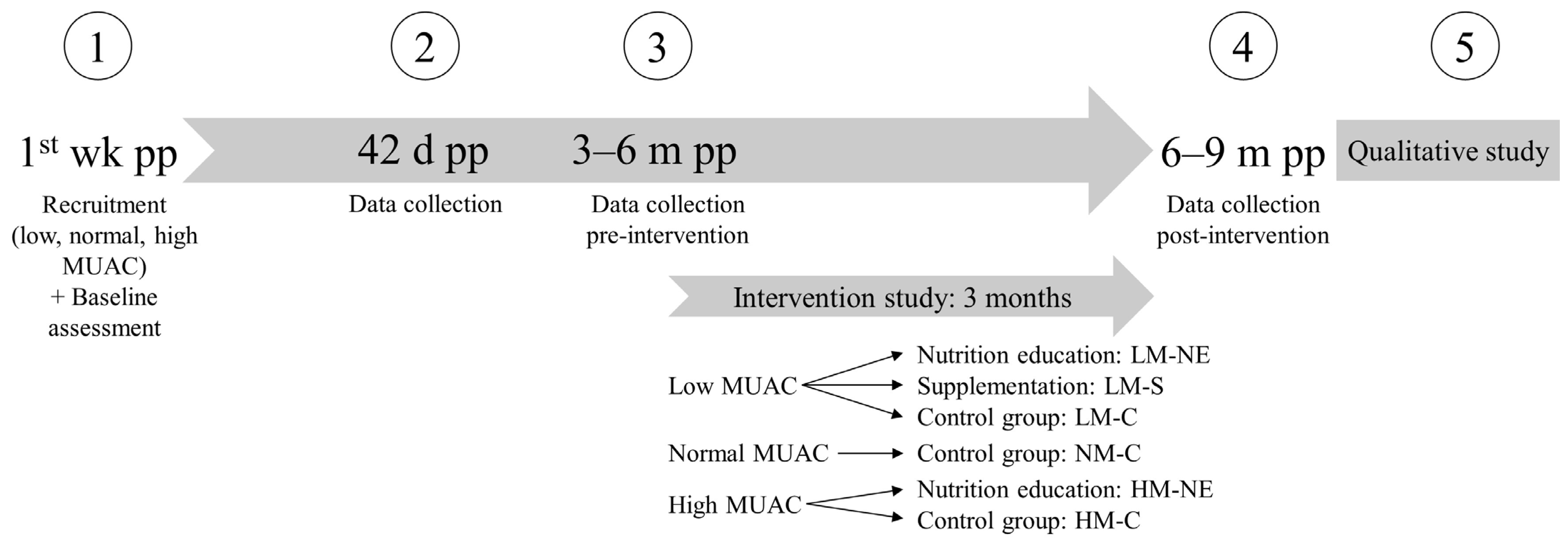
2.1. Study Design and Setting
2.2. Study Participants
2.3. Outcomes
2.3.1. Nutritional Knowledge, Attitudes, and Practice
2.3.2. Dietary Intake: 24 h Dietary Recalls
2.3.3. Anthropometrics and Hemoglobin
2.4. Sample Size and Statistics
3. Results
3.1. Nutritional Knowledge and Practice
3.2. Reasons for Dietary Choices and Attitudes towards Nutrition
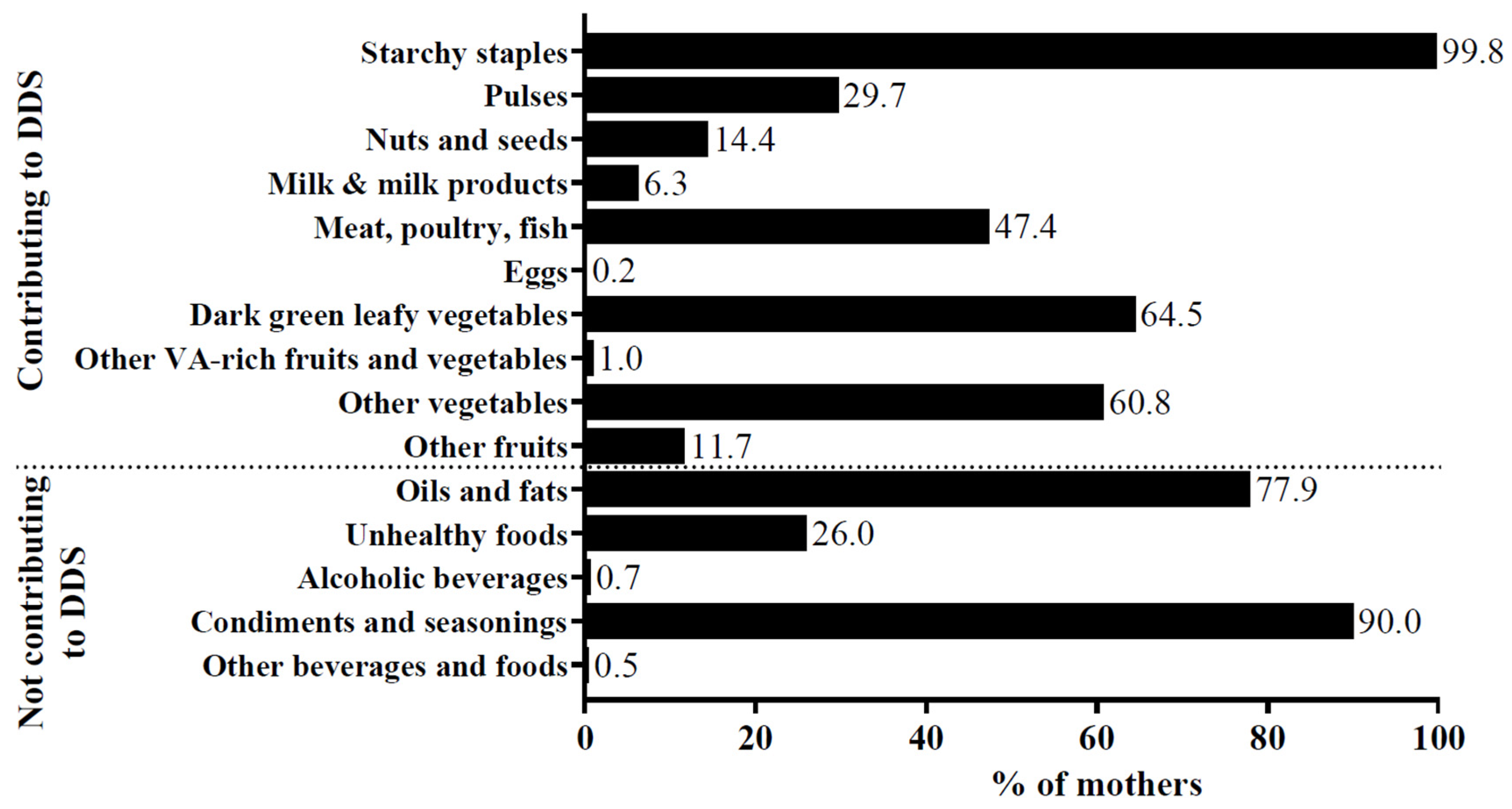
3.3. Dietary Intake
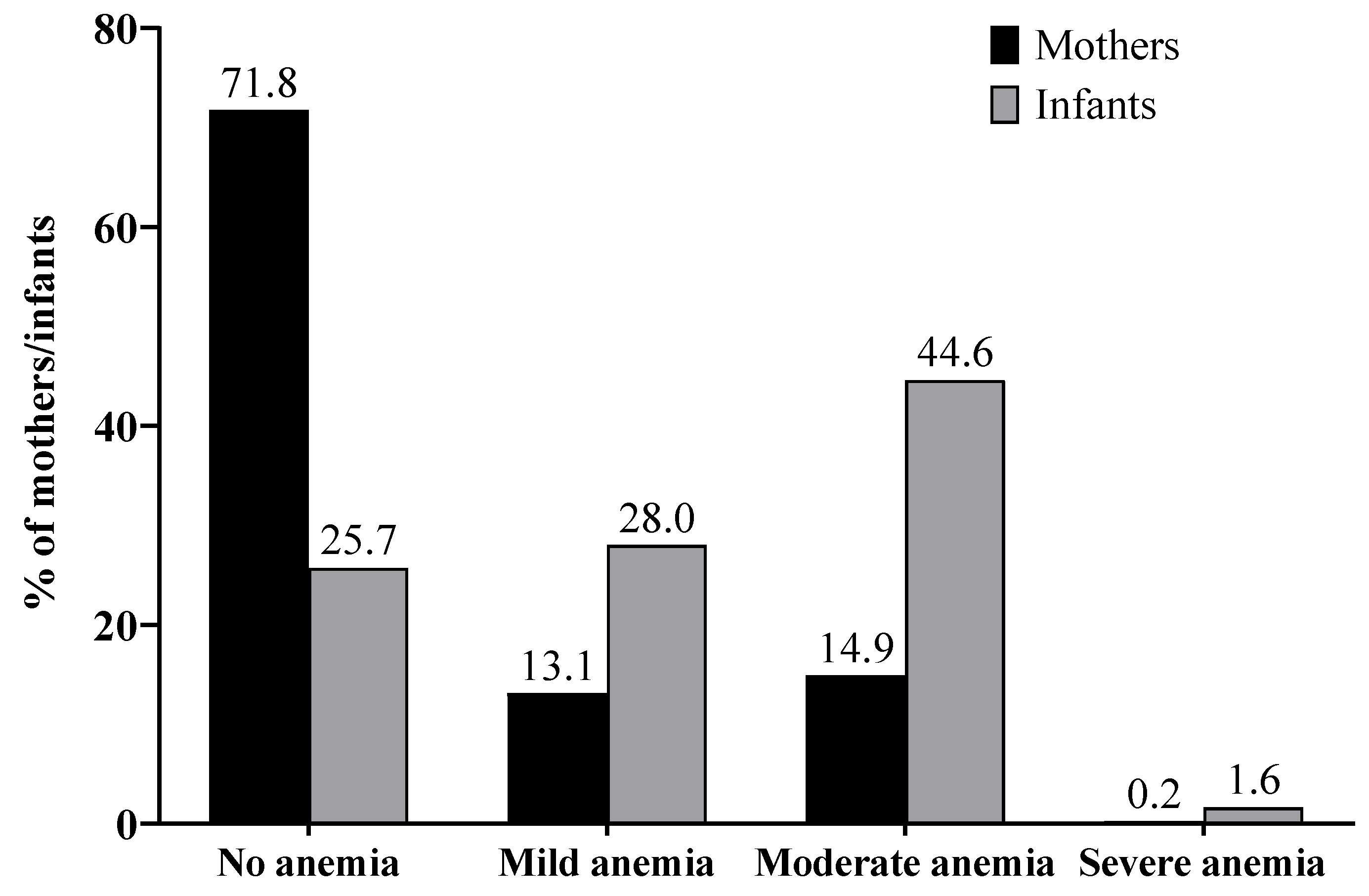
3.4. Hemoglobin and Anemia
3.5. Relationship of Nutritional Knowledge, Practice, Dietary Intake, and Hemoglobin Concentration
4. Discussion
4.1. Nutritional Knowledge
4.2. Dietary Intake
4.3. Anemia Status
4.4. Relationship of Nutritional and Socio-Demographic Factors
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Contento, I.R. Nutrition Education: Linking Research, Theory, and Practice. Asia Pac. J. Clin. Nutr. 2008, 17 (Suppl. 1), 176–179. [Google Scholar] [PubMed]
- Fautsch Macías, Y.; Glasauer, P. KAP Manual: Guidelines for Assessing Nutrition-Related Knowledge, Attitudes and Practices; Food and Agriculture Organization of the United Nations: Rome, Italy, 2014. [Google Scholar]
- Cusick, S.; Georgieff, M.K. The First 1,000 Days of Life: The Brain’s Window of Opportunity. Available online: https://www.unicef-irc.org/article/958-the-first-1000-days-of-life-the-brains-window-of-opportunity.html (accessed on 27 June 2019).
- Martorell, R. Improved Nutrition in the First 1000 Days and Adult Human Capital and Health. Am. J. Hum. Biol. 2017, 29, e22952. [Google Scholar] [CrossRef]
- Dror, D.K.; Allen, L.H. Overview of Nutrients in Human Milk. Adv. Nutr. 2018, 9, 278S–294S. [Google Scholar] [CrossRef] [PubMed]
- Chilot, D.; Aragaw, F.M.; Belay, D.G.; Asratie, M.H.; Bicha, M.M.; Alem, A.Z. Anaemia among Lactating and Non-Lactating Women in Low-Income and Middle-Income Countries: A Comparative Cross-Sectional Study. BMJ Open 2023, 13, e069851. [Google Scholar] [CrossRef]
- Kibret, K.T.; Chojenta, C.; D’Arcy, E.; Loxton, D. Spatial Distribution and Determinant Factors of Anaemia among Women of Reproductive Age in Ethiopia: A Multilevel and Spatial Analysis. BMJ Open 2019, 9, e027276. [Google Scholar] [CrossRef] [PubMed]
- MPSMRM; MSP; ICF International. Enquête Démographique et de Santé En République Démocratique Du Congo 2013–2014; Ministère du Plan et Suivi de la Mise en oeuvre de la Révolution de la Modernité, Ministère de la Santé Publique, ICF International: Rockville, MD, USA, 2014. [Google Scholar]
- Bahati, Y.L.; Delanghe, J.; Balaluka, G.B.; Philippé, J. Exploration of the Relationship between Anemia and Iron and Zinc Deficiencies in Children under 5 Years of Age Living in the Malaria Endemic Area of South Kivu/Democratic Republic of Congo. Ann. Hematol. 2022, 101, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Bahizire, E.; Tugirimana, P.L.; Dramaix, M.; Zozo, D.; Bahati, M.; Mwale, A.; Meuris, S.; Donnen, P. Malaria Is More Prevalent Than Iron Deficiency among Anemic Pregnant Women at the First Antenatal Visit in Rural South Kivu. Am. J. Trop. Med. Hyg. 2017, 97, 1551–1560. [Google Scholar] [CrossRef]
- Harvey-Leeson, S.; Karakochuk, C.D.; Hawes, M.; Tugirimana, P.L.; Bahizire, E.; Akilimali, P.Z.; Michaux, K.D.; Lynd, L.D.; Whitfield, K.C.; Moursi, M.; et al. Anemia and Micronutrient Status of Women of Childbearing Age and Children 6–59 Months in the Democratic Republic of the Congo. Nutrients 2016, 8, 98. [Google Scholar] [CrossRef]
- Moumin, N.A.; Angel, M.D.; Karakochuk, C.D.; Michaux, K.D.; Moursi, M.; Sawadogo, K.A.A.; Foley, J.; Hawes, M.D.; Whitfield, K.C.; Tugirimana, P.L.; et al. Micronutrient Intake and Prevalence of Micronutrient Inadequacy among Women (15–49 y) and Children (6–59 Mo) in South Kivu and Kongo Central, Democratic Republic of the Congo (DRC). PLoS ONE 2020, 15, e0223393. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef]
- Beitze, D.E.; Kavira Malengera, C.; Barhwamire Kabesha, T.; Frank, J.; Scherbaum, V. Disparities in Health and Nutrition between Semi-Urban and Rural Mothers and Birth Outcomes of Their Newborns in Bukavu, DR Congo: A Baseline Assessment. Prim. Health Care Res. Dev. 2023, 24, e61. [Google Scholar] [CrossRef]
- Perumal, N.; Cole, D.C.; Ouédraogo, H.Z.; Sindi, K.; Loechl, C.; Low, J.; Levin, C.; Kiria, C.; Kurji, J.; Oyunga, M. Health and Nutrition Knowledge, Attitudes and Practices of Pregnant Women Attending and Not-Attending ANC Clinics in Western Kenya: A Cross-Sectional Analysis. BMC Pregnancy Childbirth 2013, 13, 146. [Google Scholar] [CrossRef]
- Oh, H.-K.; Kang, S.; Cho, S.-H.; Ju, Y.; Faye, D. Factors Influencing Nutritional Practices among Mothers in Dakar, Senegal. PLoS ONE 2019, 14, e0211787. [Google Scholar] [CrossRef] [PubMed]
- Torheim, L.E.; Ouattara, F.; Diarra, M.M.; Thiam, F.D.; Barikmo, I.; Hatløy, A.; Oshaug, A. Nutrient Adequacy and Dietary Diversity in Rural Mali: Association and Determinants. Eur. J. Clin. Nutr. 2004, 58, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Tusa, B.S.; Weldesenbet, A.B.; Bahiru, N.; Enyew, D.B. Magnitudes of Anemia and Its Determinant Factors Among Lactating Mothers in East African Countries: Using the Generalized Mixed-Effect Model. Front Nutr. 2021, 8, 667466. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. UNICEF Conceptual Framework on Maternal and Child Nutrition; United Nations Children’s Fund, Nutrition and Child Development Section, Programme Group: New York, NY, USA, 2021. [Google Scholar]
- UNICEF Improving Child Nutrition. The Achievable Imperative for Global Progress; United Nations Children’s Fund: New York, NY, USA, 2013. [Google Scholar]
- Balarajan, Y.; Ramakrishnan, U.; Ozaltin, E.; Shankar, A.H.; Subramanian, S.V. Anaemia in Low-Income and Middle-Income Countries. Lancet 2011, 378, 2123–2135. [Google Scholar] [CrossRef]
- Bloem, M.W.; de Pee, S.; Darnton-Hill, I. New Issues in Developing Effective Approaches for the Prevention and Control of Vitamin A Deficiency. Food Nutr. Bull. 1998, 19, 137–148. [Google Scholar] [CrossRef]
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the US Department of Agriculture 5-Step Multiple-Pass Method in Assessing Food Intake in Obese and Nonobese Women. Am. J. Clin. Nutr. 2003, 77, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Lukmanji, Z.; Hertzmark, E.; Mlingi, N.; Assey, V.; Ndossi, G.; Fawzi, W. Tanzania Food Composition Tables; Muhimbili University of Health and Allied Sciences (MUHAS): Dar es Salaam, Tanzania; Tanzania Food and Nutrition Centre (TFNC): Dar es Salaam, Tanzania; Harvard School of Public Health (HSPH): Boston, MA, USA, 2008. [Google Scholar]
- Mwai, J.; Kimani, A.; Mbelenga, E.; Charrondiere, U.R.; Grande, F.; Rittenschober, D.; Vincent, A.; Murugu, D. Kenya Food Composition Tables 2018; FAO: Rome, Italy; Government of Kenya: Nairobi, Kenya, 2018.
- Vincent, A.; Grande, F.; Compaoré, E.; Amponsah Annor, G.; Addy, P.A.; Aburime, L.C.; Ahmed, D.; Bih Loh, A.M.; Dahdouh Cabia, S.; Deflache, N.; et al. FAO/INFOODS Food Composition Table for Western Africa (2019) User Guide & Condensed Food Composition Table/Table de Composition Des Aliments FAO/INFOODS Pour l’Afrique de l’Ouest (2019) Guide d’utilisation & Table de Composition Des Aliments Condensée; FAO: Rome, Italy, 2020. [Google Scholar]
- FAO. Minimum Dietary Diversity for Women: An Updated Guide to Measurement—From Collection to Action; FAO: Rome, Italy, 2021; ISBN 978-92-5-133993-0. [Google Scholar]
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011.
- Safiri, S.; Kolahi, A.-A.; Noori, M.; Nejadghaderi, S.A.; Karamzad, N.; Bragazzi, N.L.; Sullman, M.J.M.; Abdollahi, M.; Collins, G.S.; Kaufman, J.S.; et al. Burden of Anemia and Its Underlying Causes in 204 Countries and Territories, 1990–2019: Results from the Global Burden of Disease Study 2019. J. Hematol. Oncol. 2021, 14, 185. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.C., Jr. Sample Size Calculation for Two Independent Groups: A Useful Rule of Thumb. Proc. Singap. Healthc. 2011, 20, 138–140. [Google Scholar] [CrossRef]
- Krafft, A.; Perewusnyk, G.; Hanseler, E.; Quack, K.; Huch, R.; Breymann, C. Effect of Postpartum Iron Supplementation on Red Cell and Iron Parameters in Non-Anaemic Iron-Deficient Women: A Randomised Placebo-Controlled Study. BJOG 2005, 112, 445–450. [Google Scholar] [CrossRef]
- Bundala, N.; Kinabo, J.; Jumbe, T.; Bonatti, M.; Rybak, C.; Sieber, S. Gaps in Knowledge and Practice on Dietary Consumption among Rural Farming Households; a Call for Nutrition Education Training in Tanzania. Int. J. Food Sci. Nutr. 2020, 71, 341–351. [Google Scholar] [CrossRef]
- Nguyen, P.H.; Avula, R.; Ruel, M.T.; Saha, K.K.; Ali, D.; Tran, L.M.; Frongillo, E.A.; Menon, P.; Rawat, R. Maternal and Child Dietary Diversity Are Associated in Bangladesh, Vietnam, and Ethiopia. J. Nutr. 2013, 143, 1176–1183. [Google Scholar] [CrossRef]
- Oduor, F.O.; Boedecker, J.; Kennedy, G.; Mituki-Mungiria, D.; Termote, C. Caregivers’ Nutritional Knowledge and Attitudes Mediate Seasonal Shifts in Children’s Diets. Matern Child Nutr. 2019, 15, e12633. [Google Scholar] [CrossRef]
- Christian, A.K.; Marquis, G.S.; Colecraft, E.K.; Lartey, A.; Sakyi-Dawson, O.; Ahunu, B.K.; Butler, L.M. Caregivers’ Nutrition Knowledge and Attitudes Are Associated with Household Food Diversity and Children’s Animal Source Food Intake across Different Agro-Ecological Zones in Ghana. Br. J. Nutr. 2016, 115, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Aserese, A.D.; Atenafu, A.; Sisay, M.; Sorrie, M.B.; Yirdaw, B.W.; Zegeye, M.K. Adequate Vitamin A Rich Food Consumption and Associated Factors among Lactating Mothers Visiting Child Immunization and Post-Natal Clinic at Health Institutions in Gondar Town, Northwest Ethiopia. PLoS ONE 2020, 15, e0239308. [Google Scholar] [CrossRef] [PubMed]
- Nankumbi, J.; Grant, F.K.E.; Sibeko, L.; Mercado, E.; Kwikiriza, N.; Heck, S.; Cordeiro, L.S. Predictors of Vitamin A Rich Food Consumption among Women Living in Households Growing Orange-Fleshed Sweetpotatoes in Selected Regions in Uganda. Front. Public Health 2023, 10, 880166. [Google Scholar] [CrossRef] [PubMed]
- Nana, A.; Zema, T. Dietary Practices and Associated Factors during Pregnancy in Northwestern Ethiopia. BMC Pregnancy Childbirth 2018, 18, 183. [Google Scholar] [CrossRef] [PubMed]
- Maykondo, B.K.; Horwood, C.; Haskins, L.; Mapumulo, S.; Mapatano, M.A.; Kilola, B.M.; Mokanisa, M.B.; Hatloy, A.; John, V.M.; Bitadi, P.M.B.W. A Qualitative Study to Explore Dietary Knowledge, Beliefs, and Practices among Pregnant Women in a Rural Health Zone in the Democratic Republic of Congo. J. Health Popul. Nutr. 2022, 41, 51. [Google Scholar] [CrossRef]
- Getacher, L.; Egata, G.; Alemayehu, T.; Bante, A.; Molla, A. Minimum Dietary Diversity and Associated Factors among Lactating Mothers in Ataye District, North Shoa Zone, Central Ethiopia: A Community-Based Cross-Sectional Study. J. Nutr. Metab. 2020, 2020, 1823697. [Google Scholar] [CrossRef]
- Guja, T.; Melaku, Y.; Andarge, E. Concordance of Mother-Child (6–23 Months) Dietary Diversity and Its Associated Factors in Kucha District, Gamo Zone, Southern Ethiopia: A Community-Based Cross-Sectional Study. J. Nutr. Metab. 2021, 2021, 8819846. [Google Scholar] [CrossRef]
- Marinda, P.A.; Genschick, S.; Khayeka-Wandabwa, C.; Kiwanuka-Lubinda, R.; Thilsted, S.H. Dietary Diversity Determinants and Contribution of Fish to Maternal and Under-Five Nutritional Status in Zambia. PLoS ONE 2018, 13, e0204009. [Google Scholar] [CrossRef]
- Teferi, T.; Endalk, G.; Ayenew, G.M.; Fentahun, N. Inadequate Dietary Diversity Practices and Associated Factors among Postpartum Mothers in Gambella Town, Southwest Ethiopia. Sci. Rep. 2023, 13, 7252. [Google Scholar] [CrossRef]
- Bitew, Z.W.; Alemu, A.; Ayele, E.G.; Worku, T. Dietary Diversity and Practice of Pregnant and Lactating Women in Ethiopia: A Systematic Review and Meta-Analysis. Food Sci. Nutr. 2021, 9, 2686–2702. [Google Scholar] [CrossRef] [PubMed]
- Gitagia, M.W.; Ramkat, R.C.; Mituki, D.M.; Termote, C.; Covic, N.; Cheserek, M.J. Determinants of Dietary Diversity among Women of Reproductive Age in Two Different Agro-Ecological Zones of Rongai Sub-County, Nakuru, Kenya. Food Nutr. Res. 2019, 63, 1553. [Google Scholar] [CrossRef] [PubMed]
- Ochieng, J.; Afari-Sefa, V.; Lukumay, P.J.; Dubois, T. Determinants of Dietary Diversity and the Potential Role of Men in Improving Household Nutrition in Tanzania. PLoS ONE 2017, 12, e0189022. [Google Scholar] [CrossRef] [PubMed]
- Seid, A.; Cherie, H.A. Dietary Diversity, Nutritional Status and Associated Factors among Lactating Mothers Visiting Government Health Facilities at Dessie Town, Amhara Region, Ethiopia. PLoS ONE 2022, 17, e0263957. [Google Scholar] [CrossRef] [PubMed]
- Weldehaweria, N.B.; Misgina, K.H.; Weldu, M.G.; Gebregiorgis, Y.S.; Gebrezgi, B.H.; Zewdie, S.W.; Ngusse, H.A.; Gebrewa, H.G.; Alemu, W. Dietary Diversity and Related Factors among Lactating Women Visiting Public Health Facilities in Aksum Town, Tigray, Northern Ethiopia. BMC Nutr. 2016, 2, 38. [Google Scholar] [CrossRef]
- Kang, Y.; Hurley, K.M.; Ruel-Bergeron, J.; Monclus, A.B.; Oemcke, R.; Wu, L.S.F.; Mitra, M.; Phuka, J.; Klemm, R.; West, K.P.; et al. Household Food Insecurity Is Associated with Low Dietary Diversity among Pregnant and Lactating Women in Rural Malawi. Public Health Nutr. 2019, 22, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Alaofè, H.; Burney, J.; Naylor, R.; Taren, D. Prevalence of Anaemia, Deficiencies of Iron and Vitamin A and Their Determinants in Rural Women and Young Children: A Cross-Sectional Study in Kalalé District of Northern Benin. Public Health Nutr. 2017, 20, 1203–1213. [Google Scholar] [CrossRef]
- Franz, C.M.A.P.; Huch, M.; Mathara, J.M.; Abriouel, H.; Benomar, N.; Reid, G.; Galvez, A.; Holzapfel, W.H. African Fermented Foods and Probiotics. Int. J. Food Microbiol. 2014, 190, 84–96. [Google Scholar] [CrossRef]
- Mashau, M.E.; Maliwichi, L.L.; Jideani, A.I.O. Non-Alcoholic Fermentation of Maize (Zea mays) in Sub-Saharan Africa. Fermentation 2021, 7, 158. [Google Scholar] [CrossRef]
- Nout, M.J.R. Rich Nutrition from the Poorest—Cereal Fermentations in Africa and Asia. Food Microbiol. 2009, 26, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Kemdirim, O.C.; Chukwu, O.A.; Achinewhu, S.C. Effect of Traditional Processing of Cassava on the Cyanide Content of Gari and Cassava Flour. Plant Food Hum. Nutr. 1995, 48, 335–339. [Google Scholar] [CrossRef]
- Tesema, G.A.; Worku, M.G.; Tessema, Z.T.; Teshale, A.B.; Alem, A.Z.; Yeshaw, Y.; Alamneh, T.S.; Liyew, A.M. Prevalence and Determinants of Severity Levels of Anemia among Children Aged 6–59 Months in Sub-Saharan Africa: A Multilevel Ordinal Logistic Regression Analysis. PLoS ONE 2021, 16, e0249978. [Google Scholar] [CrossRef]
- Aderoba, A.K.; Iribhogbe, O.I.; Olagbuji, B.N.; Olokor, O.E.; Ojide, C.K.; Ande, A.B. Prevalence of Helminth Infestation during Pregnancy and Its Association with Maternal Anemia and Low Birth Weight. Int. J. Gynaecol. Obstet. 2015, 129, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, C.M.; Suchdev, P.S. Anemia Epidemiology, Pathophysiology, and Etiology in Low- and Middle-Income Countries. Ann. N. Y. Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef]
- Maketa, V.; Mavoko, H.M.; da Luz, R.I.; Zanga, J.; Lubiba, J.; Kalonji, A.; Lutumba, P.; Van Geertruyden, J.-P. The Relationship between Plasmodium Infection, Anaemia and Nutritional Status in Asymptomatic Children Aged under Five Years Living in Stable Transmission Zones in Kinshasa, Democratic Republic of Congo. Malar. J. 2015, 14, 83. [Google Scholar] [CrossRef] [PubMed]
- Matangila, J.R.; Doua, J.Y.; Linsuke, S.; Madinga, J.; da Luz, R.I.; Van Geertruyden, J.-P.; Lutumba, P. Malaria, Schistosomiasis and Soil Transmitted Helminth Burden and Their Correlation with Anemia in Children Attending Primary Schools in Kinshasa, Democratic Republic of Congo. PLoS ONE 2014, 9, e110789. [Google Scholar] [CrossRef]
- Mikobi, T.M.; Lukusa Tshilobo, P.; Aloni, M.N.; Mvumbi Lelo, G.; Akilimali, P.Z.; Muyembe-Tamfum, J.J.; Race, V.; Matthijs, G.; Mbuyi Mwamba, J.M. Correlation between the Lactate Dehydrogenase Levels with Laboratory Variables in the Clinical Severity of Sickle Cell Anemia in Congolese Patients. PLoS ONE 2015, 10, e0123568. [Google Scholar] [CrossRef]
- Tshilolo, L.; Aissi, L.M.; Lukusa, D.; Kinsiama, C.; Wembonyama, S.; Gulbis, B.; Vertongen, F. Neonatal Screening for Sickle Cell Anaemia in the Democratic Republic of the Congo: Experience from a Pioneer Project on 31 204 Newborns. J. Clin. Pathol. 2009, 62, 35–38. [Google Scholar] [CrossRef]
- Agyei, E.A.; Afrifa, S.K.; Munkaila, A.; Gaa, P.K.; Kuugbee, E.D.; Mogre, V. Income Level but Not Nutrition Knowledge Is Associated with Dietary Diversity of Rural Pregnant Women from Northern Ghana. J. Nutr. Metab. 2021, 2021, 5581445. [Google Scholar] [CrossRef]
- Dearden, K.A.; Bishwakarma, R.; Crookston, B.T.; Masau, B.T.; Mulokozi, G.I. Health Facility-Based Counselling and Community Outreach Are Associated with Maternal Dietary Practices in a Cross-Sectional Study from Tanzania. BMC Nutr. 2021, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Demilew, Y.M.; Alene, G.D.; Belachew, T. Dietary Practices and Associated Factors among Pregnant Women in West Gojjam Zone, Northwest Ethiopia. BMC Pregnancy Childbirth 2020, 20, 18. [Google Scholar] [CrossRef] [PubMed]
- Shumayla, S.; Irfan, E.M.; Kathuria, N.; Rathi, S.K.; Srivastava, S.; Mehra, S. Minimum Dietary Diversity and Associated Factors among Lactating Mothers in Haryana, India: A Community Based Cross-Sectional Study. BMC Pediatr. 2022, 22, 525. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, V.; Paudel, R.; Sunuwar, D.R.; Lyman, A.L.T.; Manohar, S.; Amatya, A. Factors Associated with Dietary Diversity among Pregnant Women in the Western Hill Region of Nepal: A Community Based Cross-Sectional Study. PLoS ONE 2021, 16, e0247085. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Roces, R.E.D.; Ladines-Llave, C.; Tuliao, M.T.R.; Kamau, M.W.; Yamada, C.; Tanaka, Y.; Shimazawa, K.; Iwamoto, S.; Matsuo, H. Dietary Intake Quality Is Affected by Knowledge and Dietary Intake Frequency among Pregnant Women in Muntinlupa, Philippines: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 12306. [Google Scholar] [CrossRef] [PubMed]
- Spronk, I.; Kullen, C.; Burdon, C.; O’Connor, H. Relationship between Nutrition Knowledge and Dietary Intake. Br. J. Nutr. 2014, 111, 1713–1726. [Google Scholar] [CrossRef] [PubMed]
- Amugsi, D.A.; Mittelmark, M.B.; Oduro, A. Association between Maternal and Child Dietary Diversity: An Analysis of the Ghana Demographic and Health Survey. PLoS ONE 2015, 10, e0136748. [Google Scholar] [CrossRef] [PubMed]
- WHO; FAO. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; Joint FAO/WHO Expert Consultation on Human Vitamin and Mineral Requirements (1998: Bangkok, Thailand); World Health Organization, Food and Agriculture Organization of the United Nations: Geneva, Switzerland; Rome, Italy, 2004.
- Henjum, S.; Torheim, L.E.; Thorne-Lyman, A.L.; Chandyo, R.; Fawzi, W.W.; Shrestha, P.S.; Strand, T.A. Low Dietary Diversity and Micronutrient Adequacy among Lactating Women in a Peri-Urban Area of Nepal. Public Health Nutr. 2015, 18, 3201–3210. [Google Scholar] [CrossRef]
- Martin-Prevel, Y.; Arimond, M.; Allemand, P.; Wiesmann, D.; Ballard, T.J.; Deitchler, M.; Dop, M.C.; Kennedy, G.; Lartey, A.; Lee, W.T.K.; et al. Development of a Dichotomous Indicator for Population-Level Assessment of Dietary Diversity in Women of Reproductive Age. Curr. Dev. Nutr. 2017, 1, cdn.117.001701. [Google Scholar] [CrossRef] [PubMed]
- Wemakor, A. Prevalence and Determinants of Anaemia in Pregnant Women Receiving Antenatal Care at a Tertiary Referral Hospital in Northern Ghana. BMC Pregnancy Childbirth 2019, 19, 495. [Google Scholar] [CrossRef] [PubMed]
- Wemakor, A.; Ziyaaba, A.; Yiripuo, F. Risk Factors of Anaemia among Postpartum Women in Bolgatanga Municipality, Ghana. BMC Nutr. 2022, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Agbozo, F.; Abubakari, A.; Der, J.; Jahn, A. Maternal Dietary Intakes, Red Blood Cell Indices and Risk for Anemia in the First, Second and Third Trimesters of Pregnancy and at Predelivery. Nutrients 2020, 12, 777. [Google Scholar] [CrossRef] [PubMed]
- Saaka, M.; Oladele, J.; Larbi, A.; Hoeschle-Zeledon, I. Dietary Diversity Is Not Associated with Haematological Status of Pregnant Women Resident in Rural Areas of Northern Ghana. J. Nutr. Metab. 2017, 2017, 8497892. [Google Scholar] [CrossRef] [PubMed]
- Lebso, M.; Anato, A.; Loha, E. Prevalence of Anemia and Associated Factors among Pregnant Women in Southern Ethiopia: A Community Based Cross-Sectional Study. PLoS ONE 2017, 12, e0188783. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Talegawkar, S.A.; Sedlander, E.; DiPietro, L.; Parida, M.; Ganjoo, R.; Aluc, A.; Rimal, R. Dietary Diversity and Its Associations with Anemia among Women of Reproductive Age in Rural Odisha, India. Ecol. Food Nutr. 2022, 61, 304–318. [Google Scholar] [CrossRef] [PubMed]
- Charlton, K.E.; Brewitt, P.; Bourne, L.T. Sources and Credibility of Nutrition Information among Black Urban South African Women, with a Focus on Messages Related to Obesity. Public Health Nutr. 2004, 7, 801–811. [Google Scholar] [CrossRef]
- Birungi, A.; Koita, Y.; Roopnaraine, T.; Matsiko, E.; Umugwaneza, M. Behavioural Drivers of Suboptimal Maternal and Child Feeding Practices in Rwanda: An Anthropological Study. Matern Child Nutr. 2023, 19, e13420. [Google Scholar] [CrossRef]
- Liguori, J.; Pradeilles, R.; Laar, A.; Zotor, F.; Tandoh, A.; Klomegah, S.; Osei-Kwasi, H.A.; Le Port, A.; Bricas, N.; Aryeetey, R.; et al. Individual-Level Drivers of Dietary Behaviour in Adolescents and Women through the Reproductive Life Course in Urban Ghana: A Photovoice Study. Matern Child Nutr. 2022, 18, e13412. [Google Scholar] [CrossRef]
- Kibr, G.; Mulugeta, A.; Bosha, T. Socio-Economic Variables Associated with Motivational Barriers of Food Choice among Lactating Women from Central Ethiopia: A Cross-Sectional Study. Ecol. Food Nutr. 2021, 60, 276–303. [Google Scholar] [CrossRef] [PubMed]
- FAO. FAOSTAT: Democratic Republic of the Congo. Available online: https://www.fao.org/faostat/en/#country/250 (accessed on 10 July 2023).
- Masuku, S.K.S.; Lan, S.-J.J. Nutritional Knowledge, Attitude, and Practices among Pregnant and Lactating Women Living with HIV in the Manzini Region of Swaziland. J. Health Popul. Nutr. 2014, 32, 261–269. [Google Scholar] [PubMed]
- Azene, A.G.; Aragaw, A.M.; Wubetie, H.T.; Wassie, G.T.; Tsegaye, G.W.; Derebe, M.A.; Mitiku, H.D. Dietary Diversity among Pregnant Women and Associated Factors in Ethiopia: Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0251906. [Google Scholar] [CrossRef] [PubMed]
- Heim, A.; Paksi, A. Low Dietary Diversity and Its Influencing Factors among a San Group in Namibia. BMC Res. Notes 2019, 12, 365. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Chen, X.; Liu, Z.; Varma, D.S.; Wan, R.; Zhao, S. Diet Diversity and Nutritional Status among Adults in Southwest China. PLoS ONE 2017, 12, e0172406. [Google Scholar] [CrossRef]
- Wondmeneh, T.G. Dietary Diversity Practice and Its Influencing Factors among Pregnant Women in Afar Region of Ethiopia: Mixed Method Study. BMC Pregnancy Childbirth 2022, 22, 291. [Google Scholar] [CrossRef]
- Kikafunda, J.K.; Lukwago, F.B.; Turyashemererwa, F. Anaemia and Associated Factors among Under-Fives and Their Mothers in Bushenyi District, Western Uganda. Public Health Nutr. 2009, 12, 2302–2308. [Google Scholar] [CrossRef]
- Sunguya, B.F.; Ge, Y.; Mlunde, L.; Mpembeni, R.; Leyna, G.; Huang, J. High Burden of Anemia among Pregnant Women in Tanzania: A Call to Address Its Determinants. Nutr. J. 2021, 20, 65. [Google Scholar] [CrossRef]
- Liyew, A.M.; Teshale, A.B. Individual and Community Level Factors Associated with Anemia among Lactating Mothers in Ethiopia Using Data from Ethiopian Demographic and Health Survey, 2016; a Multilevel Analysis. BMC Public Health 2020, 20, 775. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| K-Score Three Food Group Model | K-Score Malnutrition | K-Score Iron + Anemia | K-Score Vitamin A + Vitamin A Deficiency (VAD) | P-Score Iron |
|---|---|---|---|---|
| Can state at least 1 of the 3 types of food * | Can state a definition of malnutrition | Can state a sign/symptom of anemia | Can state a sign/symptom of VAD | Consumption of animal foods ≥ 1×/week |
| Can state an energy-giving food | Can state a consequence of malnutrition | Can state a consequence of iron deficiency in children | Consumption of green leafy vegetables ≥ 3×/week | |
| Can state a constructive food | Can state a cause of malnutrition | Can state a cause of anemia | Can state a cause of VAD | Consumption of fruits with a meal |
| Can state a protective food | Can state a preventive measure for malnutrition | Can state a preventive measure for anemia | Can state a preventive measure for VAD | Consumption of coffee/tea only outside a meal |
| Can state an iron-rich food | Can state a vitamin A-rich food | Fermentation of flour | ||
| Can state a method increasing iron bioavailability | Roasting of grains | |||
| Can state a drink reducing iron bioavailability |
| Variables a,b | % (n) | Score |
|---|---|---|
| K-Score three food group model (n = 438) | 0.36 ± 0.35 0.25 (0.00, 0.75) | |
| Knows at least one of the 3 types of food (n = 435) | 41.1 (179) | |
| Knows an energy-giving food (n = 437) | 39.1 (171) | |
| Knows a constructive food (n = 439) | 33.7 (148) | |
| Knows a protective food (n = 436) | 29.4 (128) | |
| K-Score malnutrition (n = 441) | 0.77 ± 0.33 1.00 (0.50, 1.00) | |
| Can define malnutrition (n = 436) | 70.6 (308) | |
| Knows a consequence/symptom of malnutrition (n = 441) | 85.9 (379) | |
| Knows a cause of malnutrition (n = 441) | 79.1 (349) | |
| Knows a measure to prevent malnutrition (n = 439) | 70.8 (311) | |
| K-Score iron + anemia (n = 428) | 0.24 ± 0.31 0.00 (0.00, 0.50) | |
| Knows a sign/symptom of anemia (n = 438) c | 27.2 (119) | |
| Knows a consequence of iron-deficient nutrition in children (n = 438) | 23.3 (102) | |
| Knows a cause of anemia (n = 440) | 33.0 (145) | |
| Knows a measure to prevent anemia (n = 440) | 32.5 (143) | |
| Knows an iron-rich food (n = 439) | 32.3 (142) | |
| Knows a food/method increasing iron bioavailability (n = 438) | 7.8 (34) | |
| Knows a drink decreasing iron bioavailability (n = 434) | 4.1 (18) | |
| K-Score vitamin A + vitamin A deficiency (n = 435) | 0.33 ± 0.40 0.00 (0.00, 0.75) | |
| Knows a sign/symptom of vitamin A deficiency (n = 438) c | 22.4 (98) | |
| Knows a cause of vitamin A deficiency (n = 439) | 35.8 (157) | |
| Knows a measure to prevent of vitamin A deficiency (n = 439) | 30.1 (132) | |
| Knows a vitamin A-rich food (n = 437) | 34.3 (150) | |
| K-Score total (n = 439) | 0.41 ± 0.24 0.39 (0.24, 0.56) | |
| P-Score iron (n = 425) | 0.43 ± 0.14 0.50 (0.33, 0.50) | |
| Eats fruits with a meal (n = 441) | 78.5 (346) | |
| Does not drink coffee/tea with a meal (n = 440) | 31.1 (137) | |
| Practices fermentation of flour (n = 421) | 1.0 (4) | |
| Practices roasting of flour (n = 441) | 2.9 (13) | |
| Eats animal foods at least once per week (n = 425) | 76.7 (326) | |
| Eats green leafy vegetables at least 3× per week (n = 442) | 73.3 (324) |
| Variables a,b | % (n) |
|---|---|
| Reasons for food choice (n = 442) c | |
| Taste | 68.1 (301) |
| Appearance | 42.5 (188) |
| Good for Health | 29.0 (128) |
| Availability | 25.6 (113) |
| Price | 12.2 (54) |
| Do not select | 0.9 (4) |
| Availability/affordability | 0.5 (2) |
| Diversified meal | 0.5 (2) |
| According to plans | 0.2 (1) |
| Do not know | 1.8 (8) |
| No answer | 0.7 (3) |
| Reasons for food diversification (n = 441) c | |
| Taste | 49.9 (220) |
| Good for health | 40.4 (178) |
| Appearance | 39.5 (174) |
| Availability | 33.8 (149) |
| Price | 10.0 (44) |
| For balancing, diversifying | 0.7 (3) |
| For satisfaction | 0.5 (2) |
| Habit | 0.2 (1) |
| Insufficient meal without | 0.2 (1) |
| Do not know | 2.7 (12) |
| No answer | 0.7 (3) |
| Variables | K-Score 3 FG Model | K-Score Malnutrition | K-Score Iron + Anemia | K-Score Vitamin A + VAD | K-Score Total | P-Score Iron | Dietary Diversity Score | Maternal Hb | Infant Hb | |
|---|---|---|---|---|---|---|---|---|---|---|
| K-Score malnutrition | τ | 0.292 | ||||||||
| p-value b | <0.001 | |||||||||
| n a | 437 | |||||||||
| K-Score iron + anemia | τ | 0.313 | 0.231 | |||||||
| p-value b | <0.001 | <0.001 | ||||||||
| n a | 424 | 427 | ||||||||
| K-Score vitamin A + VAD | τ | 0.256 | 0.185 | 0.301 | ||||||
| p-value b | <0.001 | <0.001 | <0.001 | |||||||
| n a | 430 | 433 | 420 | |||||||
| K-Score total | τ | 0.562 | 0.523 | 0.615 | 0.496 | |||||
| p-value b | <0.001 | <0.001 | <0.001 | <0.001 | ||||||
| n a | 437 | 439 | 425 | 431 | ||||||
| P-Score iron | τ | 0.023 | −0.004 | −0.028 | −0.093 | −0.030 | ||||
| p-value b | 0.575 | 0.931 | 0.492 | 0.027 | 0.425 | |||||
| n a | 421 | 424 | 413 | 417 | 422 | |||||
| Dietary Diversity Score | τ | 0.080 | 0.055 | 0.025 | −0.091 | 0.039 | −0.011 | |||
| p-value b | 0.052 | 0.186 | 0.552 | 0.029 | 0.303 | 0.791 | ||||
| n a | 405 | 408 | 396 | 403 | 406 | 393 | ||||
| Maternal Hb | τ | 0.053 | 0.090 | 0.086 | 0.066 | 0.095 | 0.085 | −0.009 | ||
| p-value b | 0.140 | 0.015 | 0.018 | 0.073 | 0.004 | 0.023 | 0.814 | |||
| n a | 430 | 433 | 420 | 427 | 431 | 419 | 404 | |||
| Infant Hb | τ | 0.001 | 0.003 | 0.001 | 0.007 | 0.003 | 0.001 | 0.012 | 0.027 | |
| p-value b | 0.971 | 0.938 | 0.987 | 0.846 | 0.939 | 0.986 | 0.749 | 0.419 | ||
| n a | 433 | 436 | 423 | 430 | 434 | 421 | 409 | 433 | ||
| Maternal MUAC | τ | 0.034 | 0.001 | −0.007 | −0.028 | 0.004 | 0.001 | 0.121 | 0.057 | 0.059 |
| p-value b | 0.334 | 0.987 | 0.848 | 0.439 | 0.897 | 0.972 | 0.001 | 0.081 | 0.069 | |
| n a | 437 | 440 | 427 | 434 | 438 | 424 | 410 | 436 | 439 | |
| Maternal age | τ | −0.009 | −0.006 | −0.020 | 0.000 | −0.005 | −0.055 | 0.047 | −0.059 | 0.021 |
| p-value b | 0.803 | 0.864 | 0.592 | 0.996 | 0.880 | 0.148 | 0.218 | 0.079 | 0.531 | |
| n a | 427 | 430 | 419 | 424 | 428 | 415 | 400 | 425 | 428 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beitze, D.E.; Kavira Malengera, C.; Barhwamire Kabesha, T.; Scherbaum, V. Nutrition-Related Knowledge, Attitudes, Practices, and Anemia Status of Lactating Mothers in Bukavu, Democratic Republic of the Congo—A Cross-Sectional Analysis. Nutrients 2024, 16, 870. https://doi.org/10.3390/nu16060870
Beitze DE, Kavira Malengera C, Barhwamire Kabesha T, Scherbaum V. Nutrition-Related Knowledge, Attitudes, Practices, and Anemia Status of Lactating Mothers in Bukavu, Democratic Republic of the Congo—A Cross-Sectional Analysis. Nutrients. 2024; 16(6):870. https://doi.org/10.3390/nu16060870
Chicago/Turabian StyleBeitze, Damaris Elisabeth, Céline Kavira Malengera, Theophile Barhwamire Kabesha, and Veronika Scherbaum. 2024. "Nutrition-Related Knowledge, Attitudes, Practices, and Anemia Status of Lactating Mothers in Bukavu, Democratic Republic of the Congo—A Cross-Sectional Analysis" Nutrients 16, no. 6: 870. https://doi.org/10.3390/nu16060870
APA StyleBeitze, D. E., Kavira Malengera, C., Barhwamire Kabesha, T., & Scherbaum, V. (2024). Nutrition-Related Knowledge, Attitudes, Practices, and Anemia Status of Lactating Mothers in Bukavu, Democratic Republic of the Congo—A Cross-Sectional Analysis. Nutrients, 16(6), 870. https://doi.org/10.3390/nu16060870