
Healthy Diet-Related Knowledge, Attitude, and Practice (KAP) and Related Socio-Demographic Characteristics among Middle-Aged and Older Adults: A Cross-Sectional Survey in Southwest China

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
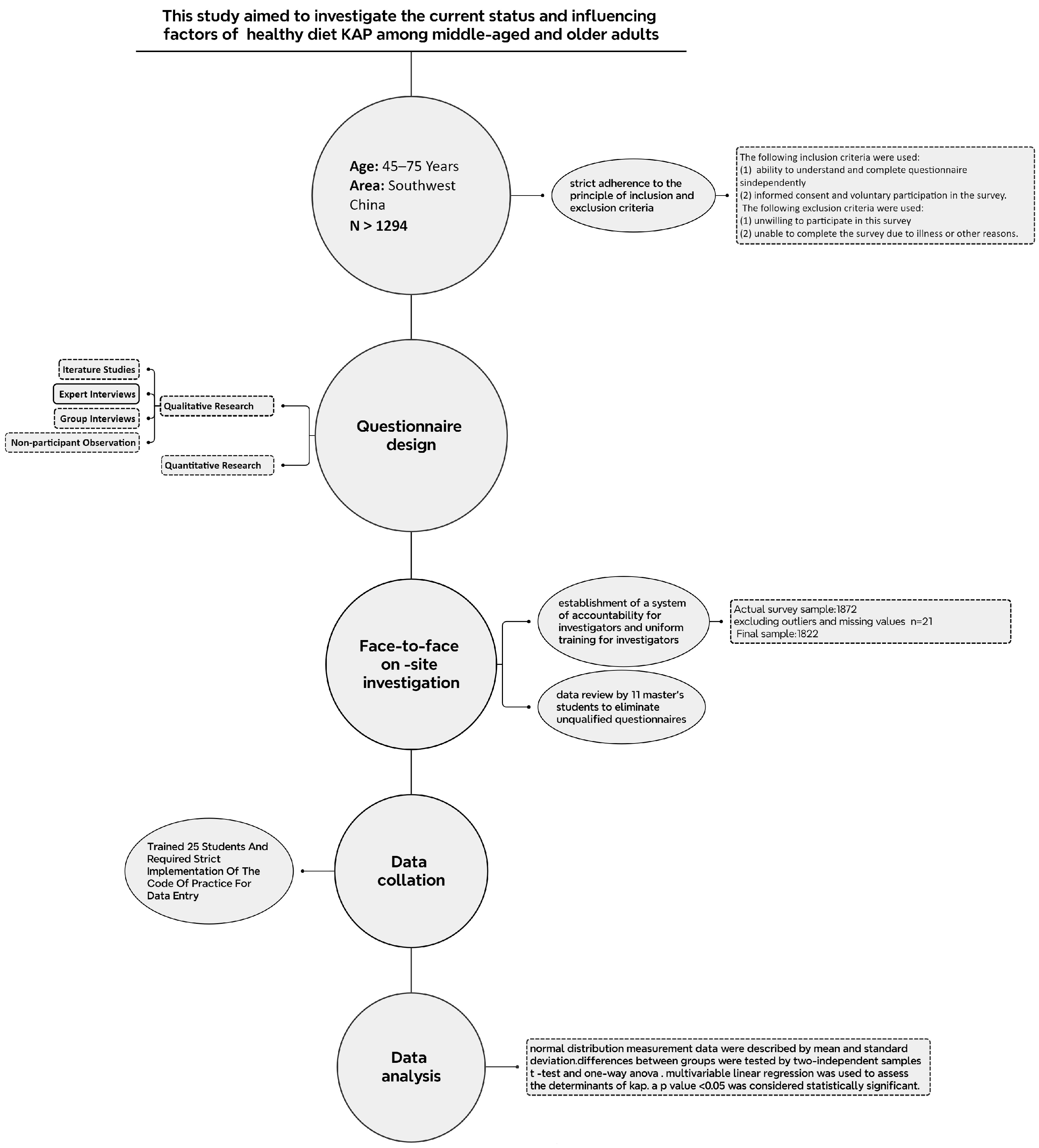
2.1. Schematic Representation of the Cross-Sectional Studies
2.2. Study Design and Sample
2.3. Inclusion and Exclusion Criteria
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Status of Healthy Diet-Related Knowledge, Attitudes, and Practices (KAP)
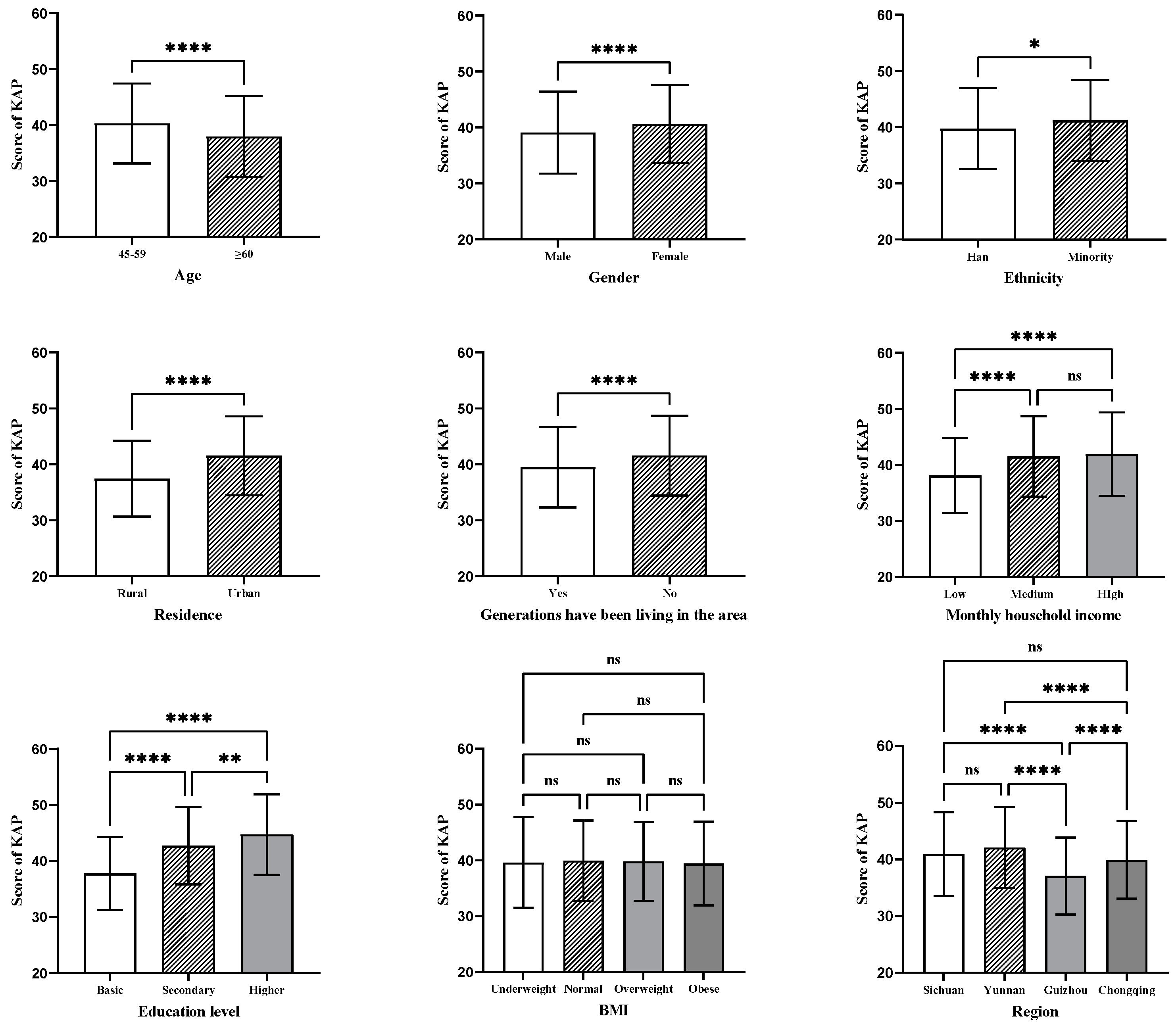
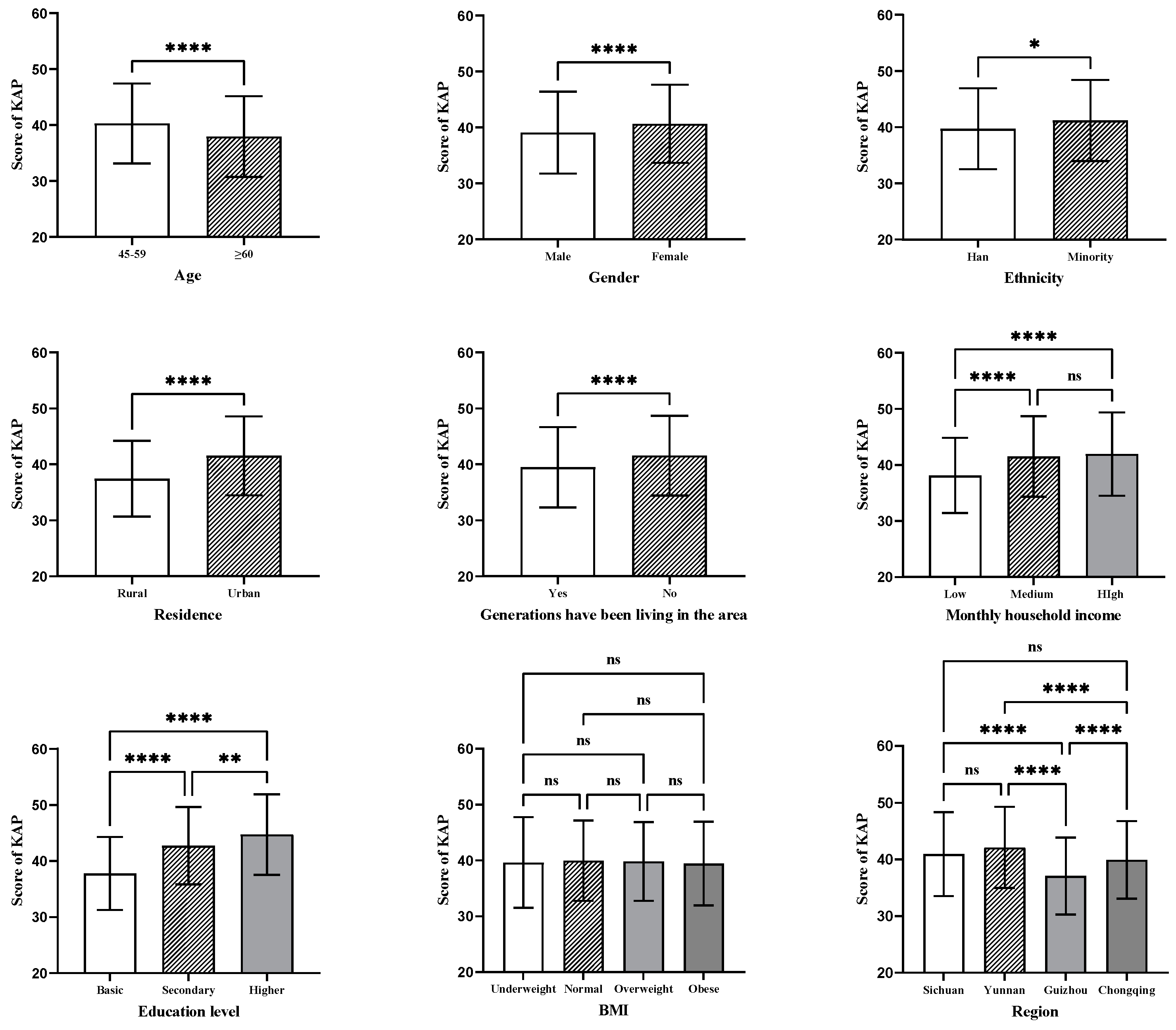
3.3. Univariate Analysis of Healthy Diet-Related Knowledge–Attitude–Practice (KAP)
3.4. Multiple Linear Regressions to Identify Factors Affecting the Healthy Diet KAP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Healthcare Access and Quality Collaborators. Assessing performance of the Healthcare Access and Quality Index, overall and by select age groups, for 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet Glob. Health 2022, 10, e1715–e1743. [Google Scholar] [CrossRef]
- Prince, M.J.; Wu, F.; Guo, Y.; Gutierrez Robledo, L.M.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Tatum, M. China’s population peak. Lancet 2022, 399, 509. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Strauss, J.A.; Hu, P.; Zhao, Y.; Crimmins, E.M. Links Between Mortality and Socioeconomic Characteristics, Disease Burden, and Biological and Physical Functioning in the Aging Chinese Population. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2022, 77, 365–377. [Google Scholar] [CrossRef]
- Puri, S.; Shaheen, M.; Grover, B. Nutrition and cognitive health: A life course approach. Front. Public Health 2023, 11, 1023907. [Google Scholar] [CrossRef]
- Miao, Y.-F.; Dong, X.-X.; Li, D.-L.; Zhang, T.; Wu, Y.; Pan, C.-W. Chronic conditions and depressive symptoms in middle-aged and older Chinese adults: Roles of perceived social support and area of residence. J. Affect. Disord. 2023, 340, 290–298. [Google Scholar] [CrossRef]
- Sharma, P.; Maurya, P.; Muhammad, T. Number of chronic conditions and associated functional limitations among older adults: Cross-sectional findings from the longitudinal aging study in India. BMC Geriatr. 2021, 21, 664. [Google Scholar] [CrossRef]
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Wang, M.Y.; Sung, H.C.; Liu, J.Y. Population Aging and Its Impact on Human Wellbeing in China. Front. Public Health 2022, 10, 883566. [Google Scholar] [CrossRef]
- Turner, A.; LaMonica, H.M.; Moroney, C.; O’Leary, F.; Naismith, S.L.; Flood, V.M. Knowledge, Attitudes, and Behaviours Concerning the Mediterranean Diet Among Older Adults in Australia. J. Community Health 2023, 48, 951–962. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Zhai, Z.; Yang, Y.; Lin, G.; Lin, W.; Wu, J.; Liu, X.; Zhang, S.; Zhou, Q.; Liu, H.; Hao, G. The hypertension and hyperlipidemia status among type 2 diabetic patients in the community and influencing factors analysis of glycemic control. Diabetol. Metab. Syndr. 2023, 15, 73. [Google Scholar] [CrossRef]
- Mohan, V.; Unnikrishnan, R.; Shobana, S.; Malavika, M.; Anjana, R.M.; Sudha, V. Are excess carbohydrates the main link to diabetes & its complications in Asians? Indian J. Med. Res. 2018, 148, 531–538. [Google Scholar]
- Traylor, D.A.; Gorissen, S.H.M.; Phillips, S.M. Perspective: Protein Requirements and Optimal Intakes in Aging: Are We Ready to Recommend More Than the Recommended Daily Allowance? Adv. Nutr. 2018, 9, 171–182. [Google Scholar] [CrossRef]
- Bojang, K.P.; Manchana, V. Nutrition and Healthy Aging: A Review. Curr. Nutr. Rep. 2023, 12, 369–375. [Google Scholar] [CrossRef]
- Aggarwal, M.; Devries, S.; Freeman, A.M.; Ostfeld, R.; Gaggin, H.; Taub, P.; Rzeszut, A.K.; Allen, K.; Conti, R.C. The Deficit of Nutrition Education of Physicians. Am. J. Med. 2018, 131, 339–345. [Google Scholar] [CrossRef]
- Zhang, Y.X.; Wang, Y.H.; Chen, Y.; Zhou, J.; Xu, L.A.; Xu, K.L.; Wang, N.; Fu, C.W.; Liu, T. Associations of Dietary Patterns and Risk of Hypertension in Southwest China: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 12378. [Google Scholar] [CrossRef]
- Huang, C.; Zhang, Y.; Liu, Y.; Liu, J.X.; Hu, Y.M.; Tang, W.W.; Wang, T.D.; Huang, X.B. Prevalence and related factors of abdominal obesity among urban adults aged 35 to 79 years in southwest China. Front. Public Health 2023, 11, 1117897. [Google Scholar] [CrossRef]
- Li, Y.; Teng, D.; Shi, X.; Qin, G.; Qin, Y.; Quan, H.; Shi, B.; Sun, H.; Ba, J.; Chen, B.; et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: National cross sectional study. BMJ 2020, 369, m997. [Google Scholar] [CrossRef]
- Ruan, Y.; Huang, Y.; Zhang, Q.; Qin, S.; Du, X.; Sun, Y. Association between dietary patterns and hypertension among Han and multi-ethnic population in southwest China. BMC Public Health 2018, 18, 1106. [Google Scholar] [CrossRef]
- Liu, T.; Yang, X.; Wu, Y.; Chen, M.; Yang, Y.; Chen, Y.; Wang, Y.; Zhou, J.; Xu, K.; Wang, N.; et al. Unhealthy Dietary Patterns Increased Risks of Incident Obesity: A Prospective Cohort Study in Southwest China. Diabetes Metab. Syndr. Obes. 2022, 15, 3111–3120. [Google Scholar] [CrossRef]
- Leng, G.; Adan, R.A.H.; Belot, M.; Brunstrom, J.M.; de Graaf, K.; Dickson, S.L.; Hare, T.; Maier, S.; Menzies, J.; Preissl, H.; et al. The determinants of food choice. Proc. Nutr. Soc. 2017, 76, 316–327. [Google Scholar] [CrossRef]
- Bettinghaus, E.P. Health promotion and the knowledge-attitude-behavior continuum. Prev. Med. 1986, 15, 475–491. [Google Scholar] [CrossRef]
- Zhang, Q.; Qin, G.H.; Liu, Z.T.; Li, Z.; Li, J.J.; Varma, D.S.; Wan, Q.Q.; Zhao, J.; Min, X.D.; Han, X.M.; et al. Dietary Balance Index-07 and the Risk of Anemia in Middle Aged and Elderly People in Southwest China: A Cross Sectional Study. Nutrients 2018, 10, 162. [Google Scholar] [CrossRef]
- Yang, Y.; He, D.; Wei, L.; Wang, S.; Chen, L.; Luo, M.; Mao, Z. Association between diet-related knowledge, attitudes, behaviors, and self-rated health in Chinese adult residents: A population-based study. BMC Public Health 2020, 20, 720. [Google Scholar] [CrossRef]
- Black, M.; Bowman, M. Nutrition and Healthy Aging. Clin. Geriatr. Med. 2020, 36, 655–669. [Google Scholar] [CrossRef]
- Hill, C.R.; Blekkenhorst, L.C.; Radavelli-Bagatini, S.; Sim, M.; Woodman, R.J.; Devine, A.; Shaw, J.E.; Hodgson, J.M.; Daly, R.M.; Lewis, J.R. Fruit and Vegetable Knowledge and Intake within an Australian Population: The AusDiab Study. Nutrients 2020, 12, 3628. [Google Scholar] [CrossRef]
- Laurenti, P.; De Meo, C.; Sacchini, D.; Spagnolo, A.G.; Moro, D.; Varacca, A.; Landi, F.; Manes-Gravina, E.; Sgadari, A.; Bernabei, R.; et al. Factors affecting safe and healthy diet in older adults in Italy: Results of a preliminary study performed in a community-dwelling sample. Public Health Nutr. 2020, 23, 432–438. [Google Scholar] [CrossRef]
- Ul Haq, I.; Mariyam, Z.; Li, M.; Huang, X.; Jiang, P.; Zeb, F.; Wu, X.; Feng, Q.; Zhou, M. A Comparative Study of Nutritional Status, Knowledge Attitude and Practices (KAP) and Dietary Intake between International and Chinese Students in Nanjing, China. Int. J. Environ. Res. Public Health 2018, 15, 1910. [Google Scholar] [CrossRef]
- Ding, C.; Qiu, Y.; Hao, L.; Hong, H.; Shan, F.; Yuan, F.; Chen, Z.; Gong, W.; Liu, A. [Dietary recommendation-related knowledge level of Chinese adults in 2021]. Wei Sheng Yan Jiu J. Hyg. Res. 2022, 51, 870–875. [Google Scholar]
- Zeng, Q.; He, Y.; Dong, S.; Zhao, X.; Chen, Z.; Song, Z.; Chang, G.; Yang, F.; Wang, Y. Optimal cut-off values of BMI, waist circumference and waist:height ratio for defining obesity in Chinese adults. Br. J. Nutr. 2014, 112, 1735–1744. [Google Scholar] [CrossRef]
- Sindhu, S.; Madaiah, M. Impact of educational intervention in promoting KAP of food label information to make healthier food choices among adolescents in Bangalore City. J. Fam. Med. Prim. Care 2023, 12, 1371–1378. [Google Scholar] [CrossRef]
- Haron, H.; Kamal, N.F.; Yahya, H.M.; Shahar, S. Knowledge, Attitude and Practice (KAP) of Malay Elderly on Salt Intake and Its Relationship With Blood Pressure. Front. Public Health 2020, 8, 559071. [Google Scholar] [CrossRef]
- Jeinie, M.H.B.; Guad, R.M.; Hetherington, M.M.; Gan, S.H.; Aung, Y.N.; Seng, W.Y.; Lin, C.L.S.; George, R.; Sawatan, W.; Nor, N.M.; et al. Comparison of Nutritional Knowledge, Attitudes and Practices between Urban and Rural Secondary School Students: A Cross-Sectional Study in Sabah, East Malaysia. Foods 2021, 10, 2037. [Google Scholar] [CrossRef]
- Choi, Y.J.; Crimmins, E.M.; Kim, J.K.; Ailshire, J.A. Food and nutrient intake and diet quality among older Americans. Public Health Nutr. 2021, 24, 1638–1647. [Google Scholar] [CrossRef]
- Xu, Z.W.; Chen, S.Z.; Guo, M.; Zhang, T.L.; Niu, X.X.; Zhou, Y.X.; Tan, J.L.; Wang, J. The impact of diet quality on cognitive ability of Chinese older adults: Evidence from the China Health and Nutrition Survey (CHNS). BMC Geriatr. 2024, 24, 55. [Google Scholar] [CrossRef]
- Liao, Y.; Yang, J. Status of nutrition labeling knowledge, attitude, and practice (KAP) of residents in the community and structural equation modeling analysis. Front. Nutr. 2023, 10, 1097562. [Google Scholar] [CrossRef]
- Żarnowski, A.; Jankowski, M.; Gujski, M. Nutrition Knowledge, Dietary Habits, and Food Labels Use-A Representative Cross-Sectional Survey among Adults in Poland. Int. J. Environ. Res. Public Health 2022, 19, 11364. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, J.; Ma, J.; Shi, W.; Wu, J. Comparison of Salt-Related Knowledge and Behaviors Status of WeChat Users between 2019 and 2020. Nutrients 2021, 13, 2141. [Google Scholar] [CrossRef]
- Milte, C.M.; Ball, K.; Crawford, D.; McNaughton, S.A. Diet quality and cognitive function in mid-aged and older men and women. BMC Geriatr. 2019, 19, 361. [Google Scholar] [CrossRef]
- Lee, J.; Allen, J. Gender Differences in Healthy and Unhealthy Food Consumption and Its Relationship with Depression in Young Adulthood. Community Ment. Health J. 2021, 57, 898–909. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; Vynckier, L.; Moreno, L.A.; Beghin, L.; de la, O.A.; Forsner, M.; Gonzalez-Gross, M.; Huybrechts, I.; Iguacel, I.; Kafatos, A.; et al. Mediation of psychosocial determinants in the relation between socio-economic status and adolescents’ diet quality. Eur. J. Nutr. 2018, 57, 951–963. [Google Scholar] [CrossRef] [PubMed]
- Mu, T.Y.; Xu, R.X.; Zhu, Q.Y.; Chen, L.S.; Dong, D.; Xu, J.Y.; Shen, C.Z. Diet-related knowledge, attitudes, and behaviors among young and middle-aged individuals with high-normal blood pressure: A cross-sectional study in China. Front. Public Health 2022, 10, 898457. [Google Scholar] [CrossRef]
- Van Hoa, H.; Giang, H.T.; Vu, P.T.; Van Tuyen, D.; Khue, P.M. Factors Associated with Health Literacy among the Elderly People in Vietnam. BioMed Res. Int. 2020, 2020, 3490635. [Google Scholar] [CrossRef]
- Pollard, C.M.; Pulker, C.E.; Meng, X.; Kerr, D.A.; Scott, J.A. Who Uses the Internet as a Source of Nutrition and Dietary Information? An Australian Population Perspective. J. Med. Internet Res. 2015, 17, e209. [Google Scholar] [CrossRef]
- Ma, L.; Xu, H.; Zhang, Z.; Li, L.; Lin, Z.; Qin, H. Nutrition knowledge, attitudes, and dietary practices among parents of children and adolescents in Weifang, China: A cross-sectional study. Prev. Med. Rep. 2023, 35, 102396. [Google Scholar] [CrossRef]
- Wang, S.J.; Wang, T.T.; Wang, J.B. Nutritional knowledge, attitudes and dietary behaviors of teachers and students in a medical college in Beijing and their influencing factors. Beijing Da Xue Xue Bao.Yi Xue Ban J. Peking Univ. Health Sci. 2020, 52, 881–885. [Google Scholar]
- Chen, S.; Deng, T.; Guo, L.; Han, H.; Lu, T.; Regan, Á.; Shan, L.C.; Tao, W.; Wall, P. A survey of Chinese consumers’ knowledge, beliefs and behavioural intentions regarding salt intake and salt reduction. Public Health Nutr. 2020, 23, 1450–1459. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, S.; Shi, M.; Wang, X.; Liu, H.; Guo, S.; Tan, L.; Yang, X.; Wu, X.; Hao, L. Awareness of nutrition and health knowledge and its influencing factors among Wuhan residents. Front. Public Health 2022, 10, 987755. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | n (%) | |
|---|---|---|
| Age | 45–59 | 1473 (81.2) |
| ≥60 | 343 (18.8) | |
| Gender | Male | 914 (50.2) |
| Female | 908 (49.8) | |
| Ethnicity | Han | 1670 (91.7) |
| Minority | 152 (8.3) | |
| Family residence | Rural | 750 (41.2) |
| Urban | 1072 (58.8) | |
| Generations have lived in the area | Yes | 1508 (81.8) |
| No | 314 (17.2) | |
| Education | Basic | 1122 (61.6) |
| Secondary | 550 (30.2) | |
| Higher | 150 (8.2) | |
| Monthly household income | Low | 950 (52.2) |
| Medium | 454 (24.9) | |
| High | 418 (22.9) | |
| BMI | Underweight | 70 (3.8) |
| Normal | 1024 (56.2) | |
| Overweight | 604 (33.2) | |
| Obese | 124 (6.8) | |
| Region | Guizhou | 441 (24.2) |
| Chongqing | 677 (37.2) | |
| Sichuan | 363 (19.9) | |
| Yunnan | 341 (18.7) | |
| Variables | Score of Knowledge | p-Value | Score of Attitude | p-Value | Score of Practice | p-Value | |
|---|---|---|---|---|---|---|---|
| Age a | 45–59 | 4.94 ± 3.01 | <0.001 * | 21.54 ± 4.13 | <0.001 * | 13.81 ± 2.86 | 0.162 |
| ≥60 | 4.30 ± 2.82 | 20.08 ± 4.19 | 13.57 ± 2.75 | ||||
| Gender a | Male | 4.63 ± 2.89 | 0.006 * | 21.11 ± 4.34 | 0.104 | 13.33 ± 2.92 | <0.001 * |
| Female | 5.01 ± 3.06 | 21.42 ± 4.00 | 14.19 ± 2.69 | ||||
| Ethnicity a | Han | 4.80 ± 2.97 | 0.435 | 21.19 ± 4.19 | 0.014 * | 13.73 ± 2.86 | 0.094 |
| Minority | 5.00 ± 3.19 | 22.06 ± 3.94 | 14.13 ± 2.66 | ||||
| Residence a | Rural | 3.96 ± 2.60 | <0.001 * | 20.32 ± 4.38 | <0.001 * | 13.17 ± 2.74 | <0.001 * |
| Urban | 5.42 ± 3.08 | 21.92 ± 3.89 | 14.18 ± 2.84 | ||||
| Generations have lived in the area a | Yes | 4.67 ± 2.94 | <0.001 * | 21.16 ± 4.21 | 0.021 * | 13.66 ± 2.83 | 0.001 * |
| No | 5.53 ± 3.11 | 21.76 ± 3.98 | 14.25 ± 2.84 | ||||
| Education level b | Basic | 3.97 ± 2.56 | <0.001 * | 20.39 ± 4.15 | <0.001 * | 13.41 ± 2.75 | <0.001 * |
| Secondary | 5.95 ± 3.06 | 22.48 ± 3.88 | 14.31 ± 2.86 | ||||
| Higher | 7.00 ± 3.14 | 23.34 ± 3.53 | 14.39 ± 3.07 | ||||
| Monthly household income b | Low | 4.12 ± 2.64 | <0.001 * | 20.45 ± 4.14 | <0.001 * | 13.56 ± 2.79 | 0.006 * |
| Medium | 5.44 ± 3.04 | 22.06 ± 4.01 | 13.99 ± 2.79 | ||||
| High | 5.73 ± 3.26 | 22.24 ± 4.08 | 13.98 ± 2.99 | ||||
| BMI b | Underweight | 5.31 ± 3.51 | 0.055 | 20.81 ± 4.61 | 0.474 | 13.49 ± 2.73 | 0.377 |
| Normal | 4.89 ± 2.99 | 21.34 ± 4.08 | 13.70 ± 2.85 | ||||
| Overweight | 4.73 ± 2.86 | 21.12 ± 4.26 | 13.92 ± 2.85 | ||||
| Obese | 4.23 ± 3.09 | 21.56 ± 4.29 | 13.65 ± 2.79 | ||||
| Region b | Guizhou | 3.57 ± 2.57 | <0.001 * | 20.31 ± 4.34 | <0.001 * | 13.19 ± 2.69 | <0.001 * |
| Chongqing | 5.01 ± 2.90 | 21.18 ± 4.09 | 13.72 ± 2.85 | ||||
| Sichuan | 5.32 ± 3.13 | 21.49 ± 4.22 | 14.13 ± 2.77 | ||||
| Yunnan | 5.52 ± 3.02 | 22.43 ± 3.78 | 14.18 ± 2.98 | ||||
| Variables | β | SE | Beta | t | p-Value |
|---|---|---|---|---|---|
| Age | |||||
| 45–59 (Ref) | |||||
| ≥60 | −1.333 | 0.387 | −0.072 | −3.446 | 0.001 * |
| Gender | |||||
| Male (Ref) | |||||
| Female | 1.808 | 0.302 | 0.125 | 5.983 | <0.001 * |
| Ethnicity | |||||
| Han (Ref) | |||||
| Minority | 1.083 | 0.557 | 0.042 | 1.943 | 0.052 |
| Residence | |||||
| Rural (Ref) | |||||
| Urban | 1.945 | 0.340 | 0.133 | 5.719 | <0.001 * |
| Generations have lived in the area | |||||
| Yes (Ref) | |||||
| No | 0.694 | 0.412 | 0.036 | 1.684 | 0.092 |
| Education level | |||||
| Basic (Ref) | |||||
| Secondary | 3.493 | 0.367 | 0.223 | 9.522 | <0.001 * |
| Higher | 4.830 | 0.613 | 0.184 | 7.875 | <0.001 * |
| Monthly household income | |||||
| Low (Ref) | |||||
| Medium | 1.330 | 0.386 | 0.080 | 3.443 | 0.001 * |
| High | 0.923 | 0.410 | 0.054 | 2.254 | 0.024 * |
| Region | |||||
| Guizhou (Ref) | |||||
| Chongqing | 2.259 | 0.399 | 0.151 | 5.661 | <0.001 * |
| Sichuan | 3.092 | 0.464 | 0.171 | 6.660 | <0.001 * |
| Yunnan | 3.153 | 0.475 | 0.171 | 6.640 | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, L.; Shi, Y.; Li, S.; Jiang, K.; Zhang, L.; Wen, Y.; Shi, Z.; Zhao, Y. Healthy Diet-Related Knowledge, Attitude, and Practice (KAP) and Related Socio-Demographic Characteristics among Middle-Aged and Older Adults: A Cross-Sectional Survey in Southwest China. Nutrients 2024, 16, 869. https://doi.org/10.3390/nu16060869
Fu L, Shi Y, Li S, Jiang K, Zhang L, Wen Y, Shi Z, Zhao Y. Healthy Diet-Related Knowledge, Attitude, and Practice (KAP) and Related Socio-Demographic Characteristics among Middle-Aged and Older Adults: A Cross-Sectional Survey in Southwest China. Nutrients. 2024; 16(6):869. https://doi.org/10.3390/nu16060869
Chicago/Turabian StyleFu, Lin, Ya Shi, Shengping Li, Ke Jiang, Laixi Zhang, Yaqi Wen, Zumin Shi, and Yong Zhao. 2024. "Healthy Diet-Related Knowledge, Attitude, and Practice (KAP) and Related Socio-Demographic Characteristics among Middle-Aged and Older Adults: A Cross-Sectional Survey in Southwest China" Nutrients 16, no. 6: 869. https://doi.org/10.3390/nu16060869
APA StyleFu, L., Shi, Y., Li, S., Jiang, K., Zhang, L., Wen, Y., Shi, Z., & Zhao, Y. (2024). Healthy Diet-Related Knowledge, Attitude, and Practice (KAP) and Related Socio-Demographic Characteristics among Middle-Aged and Older Adults: A Cross-Sectional Survey in Southwest China. Nutrients, 16(6), 869. https://doi.org/10.3390/nu16060869