
Barriers to Adopting a Plant-Based Diet in High-Income Countries: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources/Search Strategy
2.2. Eligibility Criteria
- Study population: included human adults aged 18 to 65 years old. Studies were excluded if participants had diabetes, cardiovascular disease, high blood pressure, or obesity.
- Study setting: studies set in HICs were included, whereas those set in low- and middle-income countries (LMICs) were excluded. These were excluded due to large discrepancies in dietary patterns in middle-income countries. For example, on average, high-income countries consume too much meat and dairy. However, in middle-income countries, there is a much wider variation in dietary patterns. For example, many in Latin America consume high amounts of meat, whilst others (often in Asia) consume less. Therefore, including these countries would have likely introduced too much heterogeneity into the results; however, it would be useful to examine these countries and their different barriers in the future.
- Exposure: studies that included a perceived barrier to adopting a PBD were included. An example is a financial barrier. Studies that included PBDs were used, and these could be diets considered flexitarian or plant-forward but exclude exclusively plant-based/vegan diets. This type of diet was excluded as evidence on sustainable and healthy diets, including the EAT-Lancet Commission, recommends shifts to diets low in animal-source foods as being attainable for large parts of the population rather than diets where these foods are completely absent.
- Outcome: due to the nature of this review, defined outcomes were not a necessary part of the inclusion and exclusion criteria.
- Study design: all study designs were eligible; these included qualitative, mixed methods, and quantitative studies, both observational and experimental.
- Year: studies conducted before 2000 were excluded; any studies that fit all other eligibility criteria conducted after 2000 were included. The cut-off point for analysis of studies was May 2022.
- Type of publication: publications that were reviewed and not from the original publication source, such as systematic reviews and grey literature, were excluded.
- Language: Studies were only included if they were written in English.
- Studies with a focus on only meat alternatives were excluded.
2.3. Screening
2.4. Data Extraction and Analysis
2.5. Quality Assessment
3. Results
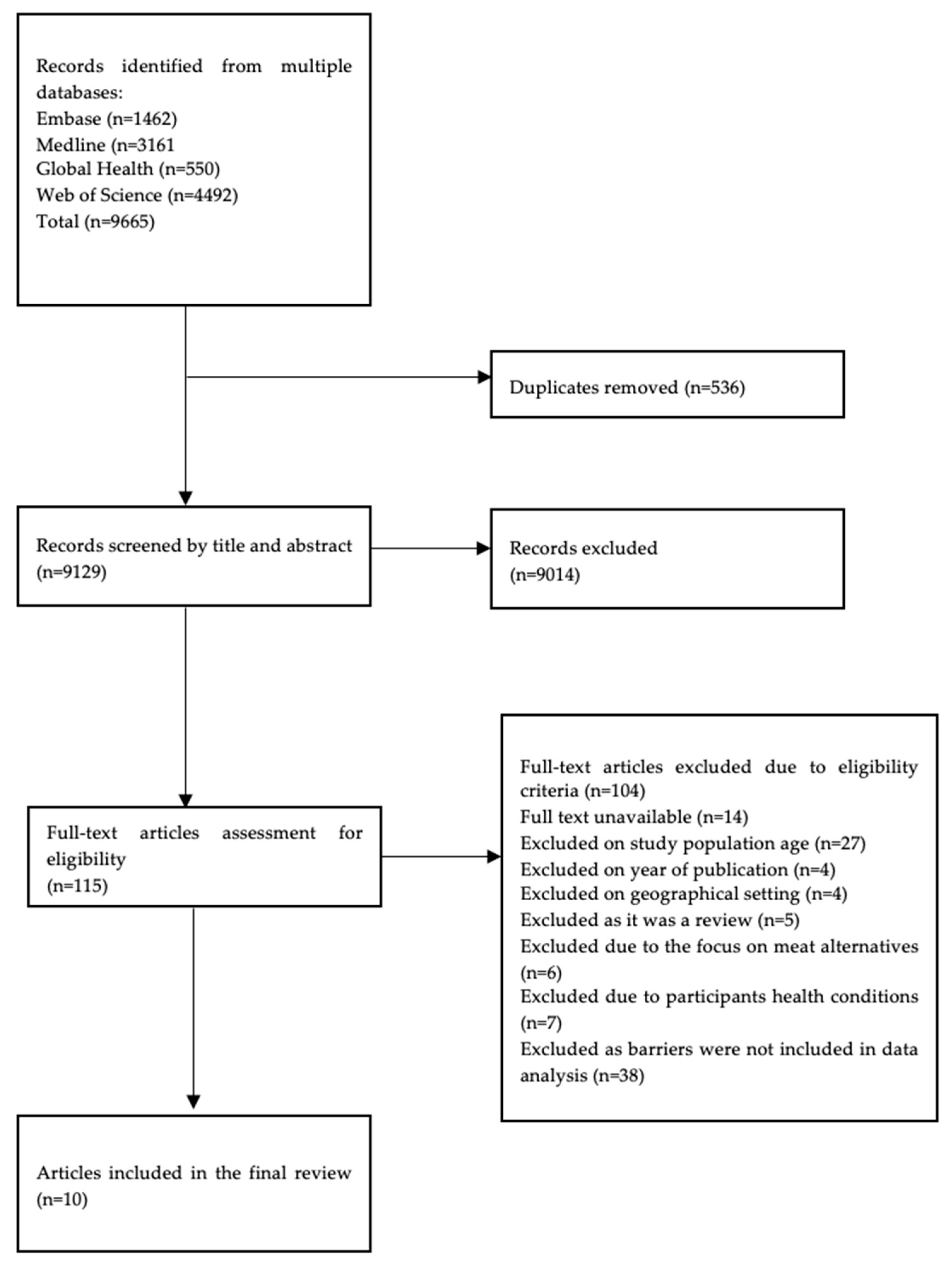
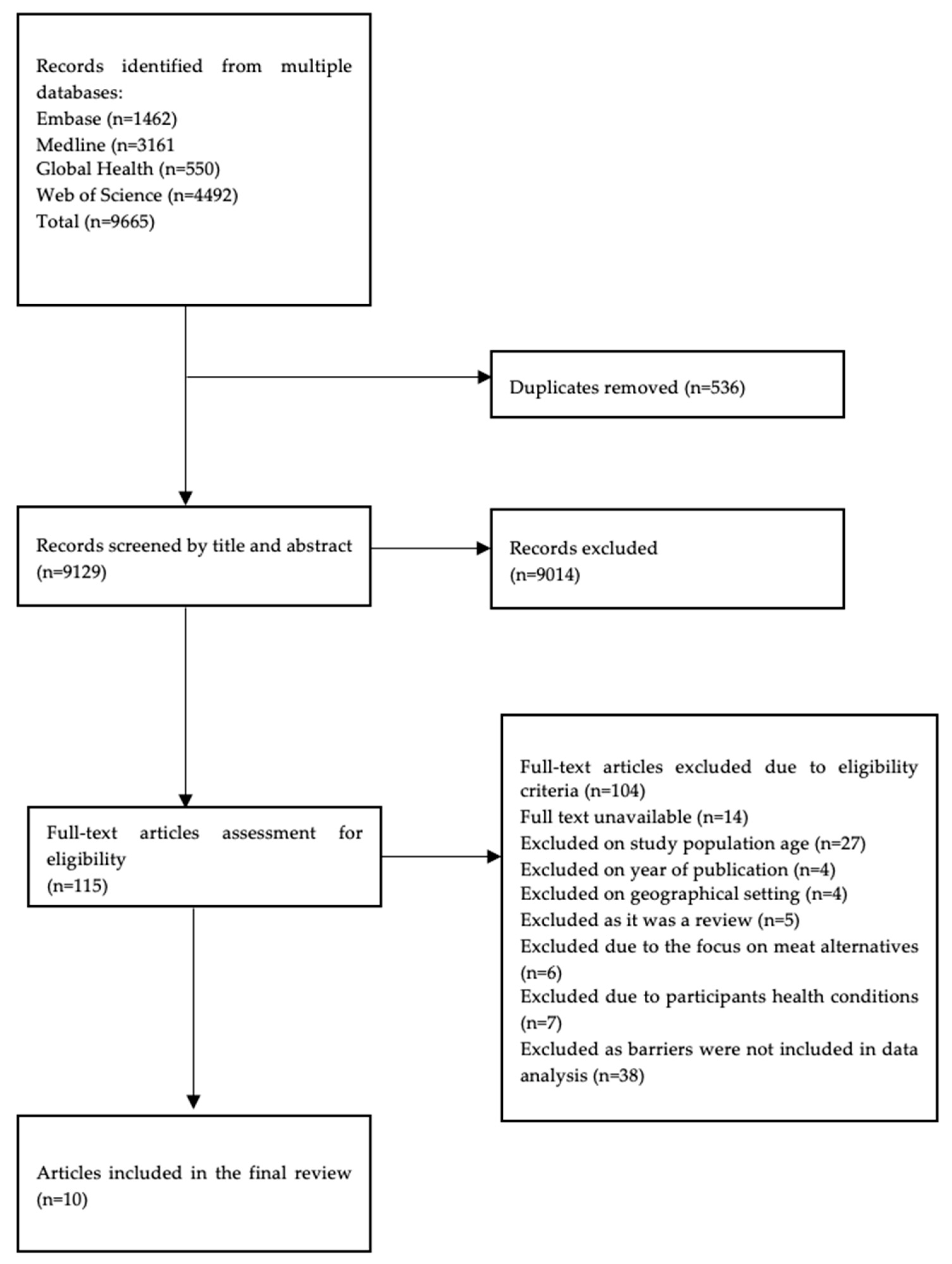
3.1. Study Selection
3.2. Study Characteristics
3.3. Results of Individual Studies
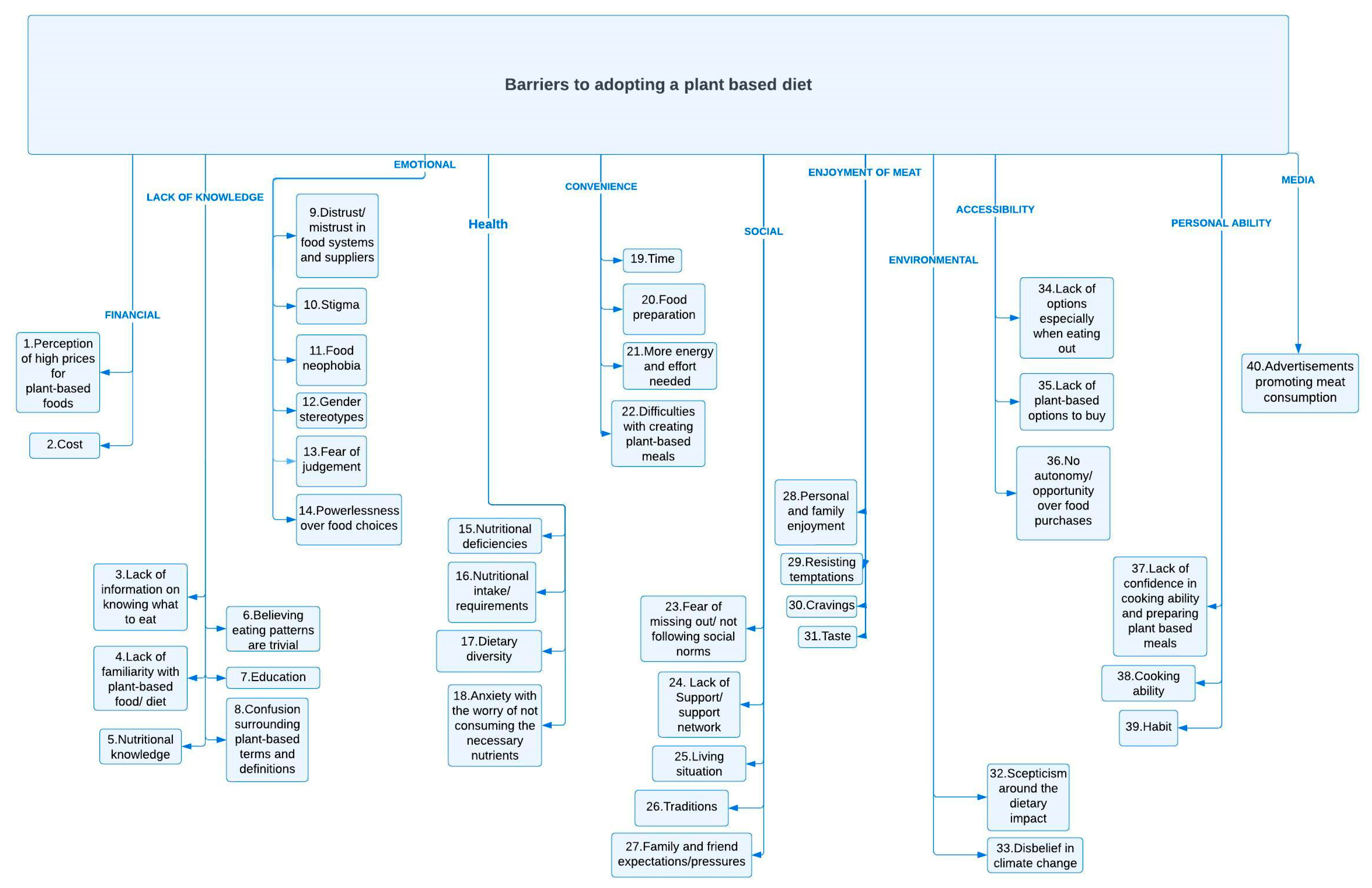
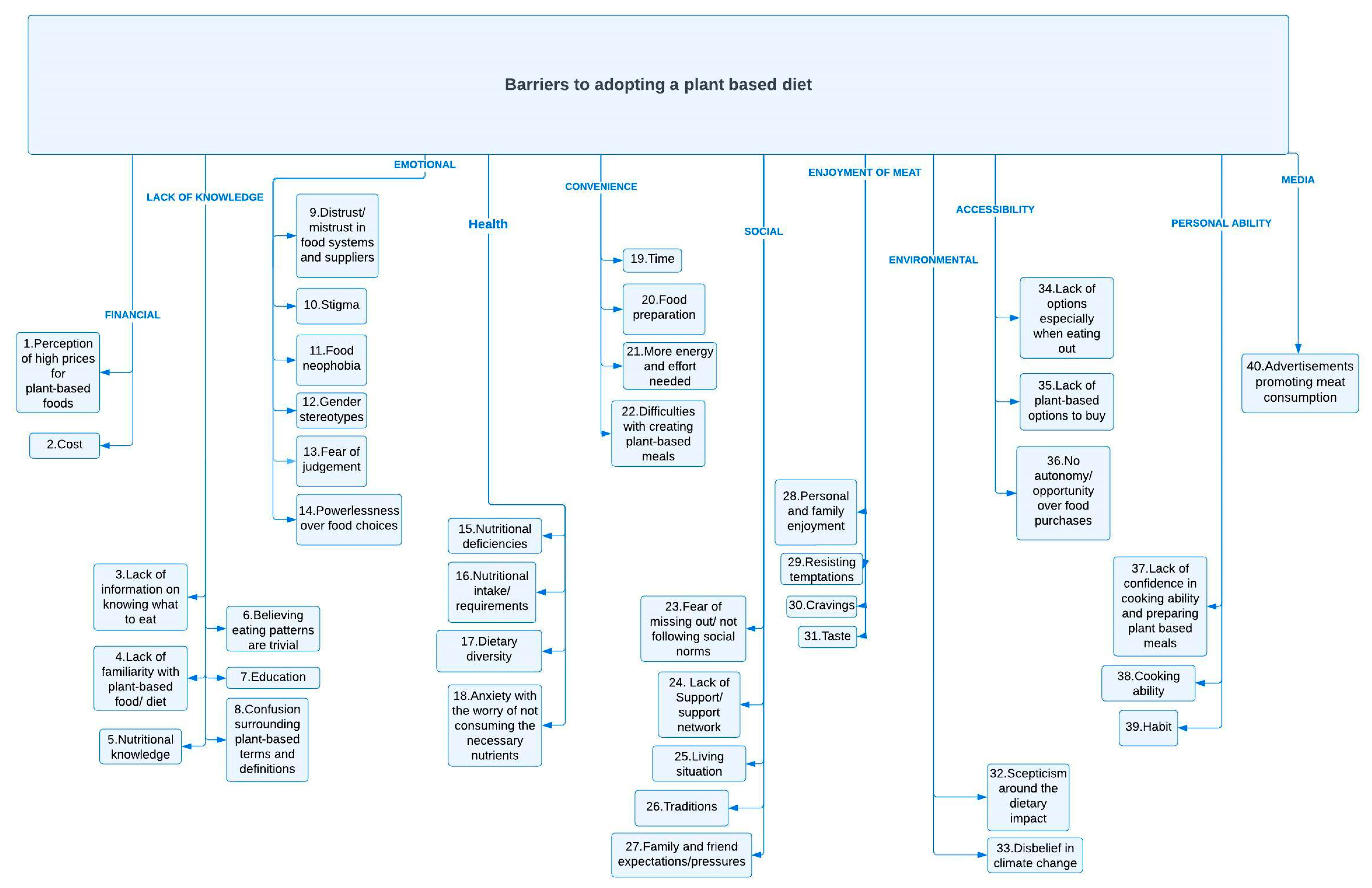
3.4. Synthesised Results
3.4.1. Financial
3.4.2. Lack of Knowledge
3.4.3. Emotional
3.4.4. Health
3.4.5. Convenience
3.4.6. Social
3.4.7. Enjoyment of Meat
3.4.8. Environmental
3.4.9. Accessibility
3.4.10. Personal Ability
3.4.11. Media
3.5. Quality Appraisal
3.5.1. Risk of Bias Assessment Results
3.5.2. Certainty Assessment Results
4. Discussion
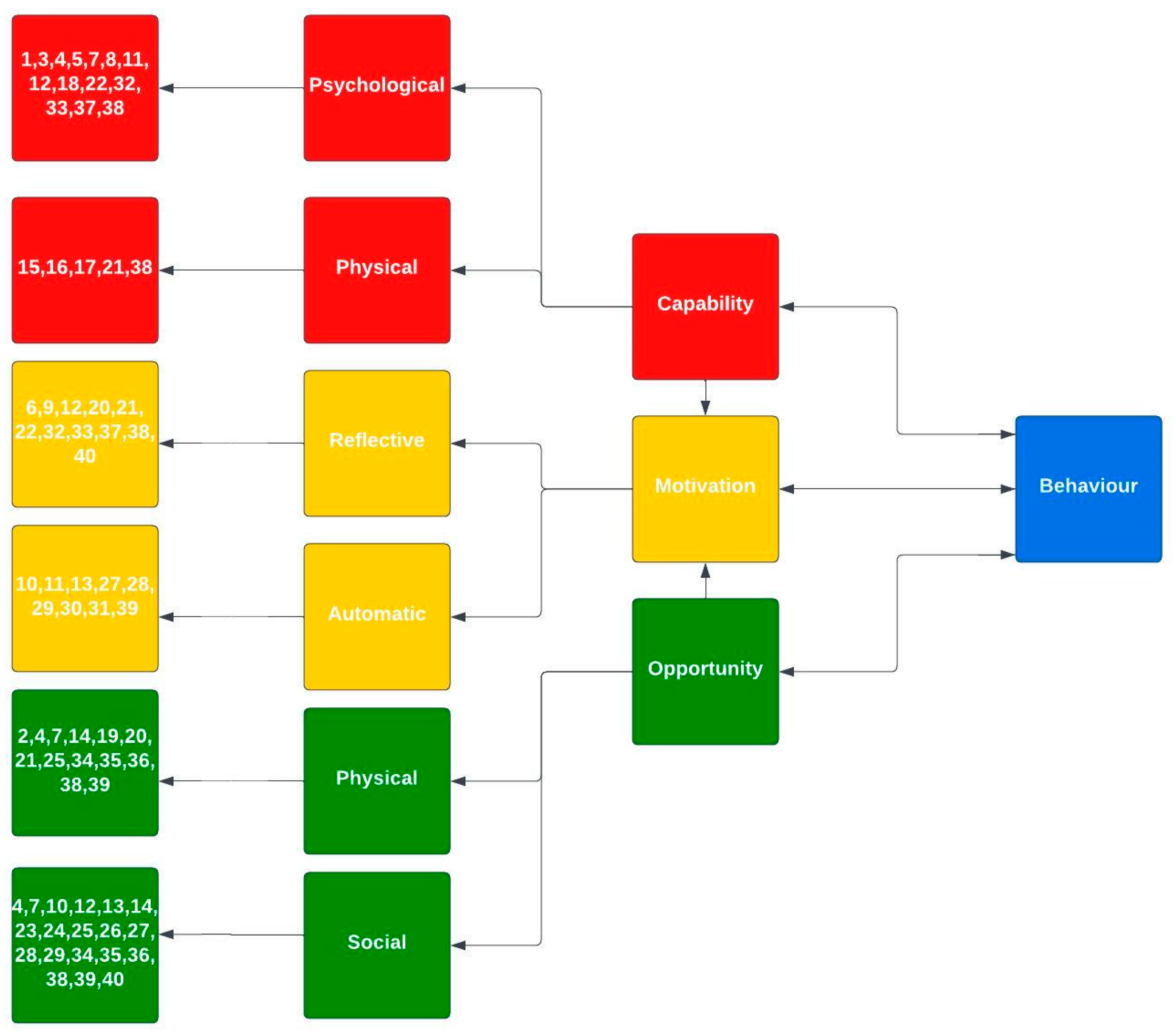
4.1. Summary of Key Findings
4.2. Interpretation of Results in the Context of Previous Research
4.3. Strengths and Limitations
4.3.1. Strengths
4.3.2. Limitations
4.4. Recommendations on How to Overcome the Most Important Barriers
4.5. Implications for Policy
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Department of Economic and Social Affairs. The Partnership Platform [Internet]. United Nations. 2022. Available online: https://sdgs.un.org/partnerships (accessed on 6 June 2022).
- Langyan, S.; Yadava, P.; Khan, F.N.; Dar, Z.A.; Singh, R.; Kumar, A. Sustaining protein nutrition through plant-based foods. Front. Nutr. 2022, 8, 772573. [Google Scholar] [CrossRef]
- Lynch, H.; Johnston, C.; Wharton, C. Plant-based diets: Considerations for environmental impact, protein quality, and exercise performance. Nutrients 2018, 10, 1841. [Google Scholar] [CrossRef]
- Department of Economic and Social Affairs. The 17 Goals|Sustainable Development [Internet]. United Nations. 2019. Available online: https://sdgs.un.org/goals (accessed on 6 June 2022).
- United Nations. For a Livable Climate: Net-Zero Commitments must Be Backed by Credible Action, United Nations. Available online: https://www.un.org/en/climatechange/net-zero-coalition (accessed on 2 March 2024).
- Meinshausen, M.; Lewis, J.; McGlade, C.; Gutschow, J.; Nicholls, Z.; Burdon, R.; Cozzi, L.; Hackman, B. Realisation of paris agreement pledges may limit warming just below 2 °C. Nature 2022, 604, 304–309. [Google Scholar] [CrossRef]
- Leahy, S.; Clark, H.; Reisinger, A. Challenges and prospects for agricultural greenhouse gas mitigation pathways consistent with the Paris Agreement. Front. Sustain. Food Syst. 2020, 4, 69. [Google Scholar] [CrossRef]
- Stewart, C.; Piernas, C.; Cook, B.; Jebb, S. Trends in UK meat consumption: Analysis of data from Years 1–11 (2008–2009 to 2018–2019) of the National Diet and Nutrition Survey Rolling Programme. Lancet Planet. Health 2021, 5, e699–e708. [Google Scholar] [CrossRef]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the anthropocene: The EAT–Lancet commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Causes of Climate Change, Climate Action. 2020. Available online: https://ec.europa.eu/clima/climate-change/causes-climate-change_en (accessed on 20 June 2022).
- Springmann, M.; Clark, M.A.; Rayner, M.; Scarborough, P.; Webb, P. The global and regional costs of healthy and sustainable dietary patterns: A modelling study. Lancet Planet. Health 2021, 5, e797–e807. [Google Scholar] [CrossRef]
- British Nutrition Foundation. Plant-Based Diets. Putting It into Practice. 2019. Available online: https://www.nutrition.org.uk/putting-it-into-practice/plant-based-diets/plant-based-diets/ (accessed on 21 June 2022).
- Eat Forum. The Planetary Health Diet, EAT. 2021. Available online: https://eatforum.org/eat-lancet-commission/the-planetary-health-diet-and-you/ (accessed on 25 June 2023).
- Alae-Carew, C.; Green, R.; Stewart, C.; Cook, B.; Dangour, A.D.; Scheelbeek, P.F.D. The role of plant-based alternative foods in sustainable and healthy food systems: Consumption trends in the UK. Sci. Total Environ. 2022, 807, 151041. [Google Scholar] [CrossRef] [PubMed]
- Frances Lee, M.; Eather, R.; Best, T. Plant-based dietary quality and depressive symptoms in Australian vegans and vegetarians: A cross-sectional study. BMJ Nutr. Prev. Health 2021, 4, e000332. Available online: https://nutrition.bmj.com/content/bmjnph/early/2021/10/20/bmjnph-2021-000332.full.pdf?with-ds=yes (accessed on 25 June 2023).
- Clem, J.; Barthel, B. A Look at Plant-Based Diets. Mo Med. 2021, 118, 233–238. [Google Scholar] [PubMed]
- Stoll-Kleemann, S.; Schmidt, U.J. Reducing meat consumption in developed and transition countries to counter climate change and Biodiversity Loss: A review of influence factors. Reg. Environ. Chang. 2016, 17, 1261–1277. [Google Scholar] [CrossRef]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Plant-based diets are associated with a lower risk of incident cardiovascular disease, cardiovascular disease mortality, and all-cause mortality in a general population of middle-aged adults. J. Am. Heart Assoc. 2019, 8, e012865. [Google Scholar] [CrossRef]
- Appleby, P.N.; Davey, G.K.; Key, T.J. Hypertension and blood pressure among meat eaters, fish eaters, vegetarians and vegans in EPIC–Oxford. Public Health Nutr. 2002, 5, 645–654. [Google Scholar] [CrossRef]
- Romanos-Nanclares, A.; Willett, W.C.; Rosner, B.A.; Collins, L.C.; Hu, F.B.; Toledo, E.; Eliassen, H. Healthful and unhealthful plant-based diets and risk of breast cancer in U.S. women: Results from the nurses’ health studies. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1921–1931. [Google Scholar] [CrossRef] [PubMed]
- Loeb, S.; Fu, B.C.; Bauer, S.R.; Pernar, C.H.; Chan, J.M.; Van Blarigan, E.L.; Giovannucci, E.L.; Kenfield, S.A.; Mucci, L.A. Association of Plant-based Diet index with prostate cancer risk. Am. J. Clin. Nutr. 2021, 115, 662–670. [Google Scholar] [CrossRef]
- Fung, T.T.; Brown, L.S. Dietary patterns and the risk of colorectal cancer. Curr. Nutr. Rep. 2012, 2, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Medawar, E.; Huhn, S.; Villringer, A.; Veronica Witte, A. The effects of plant-based diets on the body and the brain: A systematic review. Transl. Psychiatry 2019, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Plant-Based Diets and Their Impact on Health, Sustainability and the Environment: A Review of the Evidence: WHO European Office for the Prevention and Control of Noncommunicable Diseases. Regional Office for Europe. 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/349086/WHO-EURO-2021-4007-43766-61591-eng.pdf (accessed on 25 June 2022).
- Tomova, A.; Bukovsky, I.; Rembert, E.; Yonas, W.; Alwarith, J.; Barnard, N.D.; Kahleova, H. The effects of vegetarian and vegan diets on gut microbiota. Front. Nutr. 2019, 6, 47. [Google Scholar] [CrossRef]
- Rauma, A.L.; Mykkänen, H. Antioxidant status in vegetarians versus omnivores. Nutrition 2000, 16, 111–119. [Google Scholar] [CrossRef]
- Bryant, C.J. We can’ t keep meating like this: Attitudes towards vegetarian and vegan diets in the United Kingdom. Sustainability 2019, 11, 6844. [Google Scholar] [CrossRef]
- Alcorta, A.; Porta, A.; Tárrega, A.; Alvarez, M.D.; Vaquero, M.P. Foods for plant-based diets: Challenges and innovations. Foods 2021, 10, 293. [Google Scholar] [CrossRef] [PubMed]
- Michel, F.; Hartmann, C.; Siegrist, M. Consumers’ associations, perceptions and acceptance of meat and plant-based meat alternatives. Food Qual. Prefer. 2021, 87, 104063. [Google Scholar] [CrossRef]
- Lea, E.J.; Crawford, D.; Worsley, A. Consumers’ readiness to eat a plant-based diet. Eur. J. Clin. Nutr. 2006, 60, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- West, R.; Michie, S. Achieving Behaviour Change, Assist Publishing Service, Public Health England. 2020. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/933328/UFG_National_Guide_v04.00__1___1_.pdf (accessed on 26 June 2022).
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel, Understanding the Wheel—The Behaviour Change Wheel Book—A Guide to Designing Interventions. 2022. Available online: http://www.behaviourchangewheel.com/about-wheel (accessed on 26 June 2022).
- Fehér, A.; Gazdecki, M.; Véha, M.; Szakály, M.; Szakály, Z. A comprehensive review of the benefits of and the barriers to the switch to a plant-based diet. Sustainability 2020, 12, 4136. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP (Qualitative) Checklist. [Online]. 2018. Available online: https://casp-uk.b-cdn.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf (accessed on 1 July 2022).
- Center for Evidence Based Management. Critical Appraisal Checklist for Cross-Sectional Study. 2014. Available online: https://www.cebma.org (accessed on 1 July 2022).
- Appendix F Quality Appraisal Checklist—Quantitative Intervention Studies. Methods for the Development of NICE Public Health Guidance (Third Edition). 2012. Available online: https://www.nice.org.uk/process/pmg4/chapter/appendix-f-quality-appraisal-checklist-quantitative-intervention-studies#ftn.footnote_12 (accessed on 1 July 2022).
- Barr, S.I.; Chapman, G.E. Perceptions and practices of self-defined current vegetarian, former vegetarian, and Non-vegetarian Women. J. Am. Diet. Assoc. 2002, 102, 354–360. [Google Scholar] [CrossRef]
- Faber, I.; Castellanos-Feijoó, N.A.; Van de Sompel, L.; Davydova, A.; Perez-Cueto, F.J.A. Attitudes and knowledge towards plant-based diets of young adults across four European countries. exploratory survey. Appetite 2020, 145, 104498. [Google Scholar] [CrossRef]
- Kemper, J.A. Motivations, barriers, and strategies for meat reduction at different family lifecycle stages. Appetite 2020, 150, 104644. [Google Scholar] [CrossRef]
- Kemper, J.A.; White, S.K. Young adults’ experiences with flexitarianism: The 4Cs. Appetite 2021, 160, 105073. [Google Scholar] [CrossRef]
- Lea, E.J.; Crawford, D.; Worsley, A. Public views of the benefits and barriers to the consumption of a plant-based diet. Eur. J. Clin. Nutr. 2006, 60, 828–837. [Google Scholar] [CrossRef]
- Lim, T.J.; Okine, R.N.; Kershaw, J.C. Health- or environment-focused text messages as a potential strategy to increase plant-based eating among young adults: An exploratory study. Foods 2021, 10, 3147. [Google Scholar] [CrossRef]
- Macdiarmid, J.I.; Douglas, F.; Campbell, J. Eating like there’ s no tomorrow: Public awareness of the environmental impact of food and reluctance to eat less meat as part of a sustainable diet. Appetite 2016, 96, 487–493. [Google Scholar] [CrossRef]
- Mäkiniemi, J.-P.; Vainio, A. Barriers to climate-friendly food choices among young adults in Finland. Appetite 2014, 74, 12–19. [Google Scholar] [CrossRef]
- Markowski, K.L.; Roxburgh, S. “If I became a vegan, my family and friends would hate me”: Anticipating vegan stigma as a barrier to plant-based diets. Appetite 2019, 135, 1–9. [Google Scholar] [CrossRef]
- Von Essen, E. Young adults’ transition to a plant-based diet as a psychosomatic process: A psychoanalytically informed perspective. Appetite 2021, 157, 105003. [Google Scholar] [CrossRef] [PubMed]
- Lea, E.; Worsley, A. The factors associated with the belief that vegetarian diets provide health benefits. Asia Pac. J. Clin. Nutr. 2003, 12, 296–303. [Google Scholar] [PubMed]
- Lea, E.; Worsley, A. Influences on meat consumption in Australia. Appetite 2001, 36, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2021, 14, 29. [Google Scholar] [CrossRef]
- Hielkema, M.H.; Lund, T.B. Reducing meat consumption in meat-loving denmark: Exploring willingness, behavior, barriers and drivers. Food Qual. Prefer. 2021, 93, 104257. [Google Scholar] [CrossRef]
- Ensaff, H.; Coan, S.; Sahota, P.; Braybrook, D.; Akter, H.; McLeod, H. Adolescents’ Food Choice and the Place of Plant-Based Foods. Nutrients 2015, 7, 4619–4637. [Google Scholar] [CrossRef]
- Lourenco, C.; Nunes-Galbes, N.; Borgheresi, R.; Cezarino, L.; Martins, F.; Liboni, L. Psychological Barriers to Sustainable Dietary Patterns: Findings from Meat Intake Behaviour. Sustainability 2022, 14, 2199. [Google Scholar] [CrossRef]
- Graça, J.; Calheiros, M.; Oliveira, A. Attached to meat? (Un)Willingness and intentions to adopt a more plant-based diet. Appetite 2015, 95, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Perez-Cueto, F.J.A.; Rini, L.; Faber, I.; Rasmussen, M.A.; Bechtold, K.B.; Schouteten, J.J.; Steur, H.D. How barriers towards plant-based food consumption differ according to dietary lifestyle: Findings from a consumer survey in 10 EU countries. Int. J. Gastron. Food Sci. 2022, 29, 100587. [Google Scholar] [CrossRef]
- Eakman, T.; Metallinos-Katsaras, E. What are the predictors, motivators, and barriers to reducing meat and following a more plant-based diet? Curr. Dev. Nutr. 2022, 6, 481. [Google Scholar] [CrossRef]
- Graça, J.; Godinho, C.A.; Truninger, M. Reducing meat consumption and following plant-based diets: Current evidence and future directions to inform integrated transitions. Trends Food Sci. Amp Technol. 2019, 91, 380–390. [Google Scholar] [CrossRef]
- Szczebyło, A.; Rejman, K.; Halicka, E.; Laskowski, W. Towards more sustainable diets—Attitudes, opportunities and barriers to fostering pulse consumption in Polish cities. Nutrients 2020, 12, 1589. [Google Scholar] [CrossRef]
- Fresán, U.; Errendal, S.; Craig, W. Influence of the Socio-Cultural Environment and External Factors in Following Plant-Based Diets. Sustainability 2020, 12, 9093. [Google Scholar] [CrossRef]
- Kenyon, P.; Barker, M. Attitudes towards meat-eating in vegetarian and non-vegetarian teenage girls in England—An ethnographic approach. Appetite 1998, 30, 185–198. [Google Scholar] [CrossRef]
- Glandz, K.; Basil, M.; Malibach, E.; Goldberg, J.; Snyder, D. Why americans eat what they do. J. Am. Diet. Assoc. 1998, 98, 1118–1126. [Google Scholar] [CrossRef]
- Hirvonen, K.; Bai, Y.; Headey, D.; William, A. Affordability of the EAT–Lancet reference diet: A global analysis. Lancet Glob. Health 2020, 8, e59–e66. [Google Scholar] [CrossRef]
- Willett, W.; Rockstrom, J.; Lang, T.; Vermuelen, S.; Garnett, T.; Tilman, D.; Fanzo, J.; Hawkes, C.; Zurayk, R.; Rivera, J.; et al. Healthy Diets from Sustainable Food Systems Food Planet Health, Eat Forum. 2019. Available online: https://eatforum.org/content/uploads/2019/07/EAT-Lancet_Commission_Summary_Report.pdf (accessed on 22 June 2019).
- Kunst, J.; Hohle, S. Meat eaters by dissociation: How we present, prepare and talk about meat increases willingness to eat meat by reducing empathy and disgust. Appetite 2016, 105, 758–774. [Google Scholar] [CrossRef] [PubMed]
- Ellithorpe, M.; Zeldes, G.; Hall, E.; Chavez, M.; Takahashi, B.; Bleakley, A.; Plasencia, J. I’ m Lovin’ It: How Fast Food Advertising Influences Meat-Eating Preferences. J. Health Commun. 2022, 27, 141–151. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Author, Title, and Year | Study Geographical Setting | Study Population Sample Size, Age, Sex, and Social Position | Study Design | Study Outcome | Data Analysis Method |
|---|---|---|---|---|---|
| Barr and Chapman. Perceptions and practices of self-defined current vegetarian, former vegetarian, and non-vegetarian women (2002) [38]. | Canada | Total n = 193. Vegetarian n = 90; former vegetarian n = 35; non- vegetarian n = 68. Age: 18–50-year-olds. Females: n = 193. University graduates: 49.7%; students: 40.1%; employed: 73.2%. | Mixed methods. Cross-sectional survey; qualitative interviews with a subsample. | Dietary intake patterns and dietary change; Perception of meat and dairy products. | Group comparisons: One-way ANOVA. Continuous variables: Post hoc testing. Categorical variables: Chi-squared. |
| Faber, Castellanos-Feijoo, Van de Sompel, Davydova and Perez-Cueto. Attitudes and knowledge towards plant-based diets of young adults across four European countries (exploratory survey) (2020) [39]. | Belgium, Denmark, the Netherlands, and Spain | Total n = 438. Belgium n = 110; Denmark n = 119; Netherlands n = 116; Spain n = 93. Age: 18–30 years. Females: 56–82% across countries. Males comprise 18–44% of the population overall across countries. | Quantitative cross-sectional study. | Awareness of plant-based diets- perception and attitudes; The appeal of diet terminology. | Differences among countries: Pearson’ s Chi-squared test. Proportions: Fisher’ s exact test. Continuous variables: Kruskal–Wallis test. To test the association between knowledge and attitudes towards PB, vegan, and vegetarian diet terms. Adjusted for age, sex, etc.: logical regression. |
| Kemper. Motivations, barriers, and strategies for meat reduction at different family lifecycle stages (2020) [40]. | New Zealand | Total n = 36. Age: 18–60 years. Females: n = 32. Males: n = 4. | Qualitative research with the use of focus group interviews. | Motivations; Barriers; Strategies; Meat reduction. | Thematic analysis. |
| Kemper and White. Young adults’ experiences with flexitarianism: The 4Cs (2021) [41]. | New Zealand | Total n = 23. Age: 18–35 years. Females: n = 17. Males: n = 6. Students: 100%. | Qualitative research with an exploratory approach using semi-structured interviews. | Lived experiences; Motivations; Strategies; Barriers; Meat reduction and transition to a flexitarian diet. | Thematic analysis. |
| Lea, Crawford, and Worsley. Public views of the benefits and barriers to the consumption of a plant-based diet (2006) [42]. | Australia | Total n = 415. Age: 20–65 years. Females: 59.4%. Males: 40.6%. Employed full-time: 31.5%; employed part-time: 17.8%; unemployed: 2%. | Quantitative cross-sectional survey study design. | Perception and attitudes towards dietary intake/change; Barriers; Benefits. | Frequency of responses: Pearson’ s Chi-squared test (adjusted by sex, age, and university education). |
| Lim, Okine, and Kershaw. Health- or environment-focused text messages as a potential strategy to increase plant-based eating among young adults: an exploratory study (2021) [43]. | The United States of America | Total n = 159. Age: 18–26 years. Females: n = 107. Males: n = 49. Other: n = 3. | Quantitative 8-week text message pre- and post-intervention. | Dietary beliefs, intentions, behaviour, and intake. | Participant’ s characteristics group comparisons: Chi-squared test. Explore the effect of the interventions on dietary predictors, intentions, and behaviours: Paired samples t-test, from baseline and post-intervention answers. Differences between group intervention: Independent samples t-test. |
| Macdiarmid, Douglas, and Campbell. Eating like there’ s no tomorrow: public awareness of the environmental impact of food and reluctance to eat less meat as part of a sustainable diet (2016) [44]. | Scotland | Total n = 83. Age: 25–56 years. Females: n = 43. Males: n = 40. | Qualitative research with the use of focus group interviews. | Public awareness; Public willingness to make dietary changes; Meat reduction. | Thematic analysis. Exploring deprivation, sex or urban/rural differences in attitudes towards reducing meat consumption: Framework analysis. |
| Makiniemi and Vainio. Barriers to climate-friendly food choices among young adults in Finland (2014) [45]. | Finland | Total n = 350. Mean age: 24. Females: n = 280. Males: n = 70. Students: 100%. | Quantitative cross-sectional, questionnaire study. | Perception and attitudes, and barriers toward dietary intake/change. | Differences in men and women for perceived barriers: t-test. The impact of perceived barriers on climate-friendly food choices: multiple regression analysis. The impact of perceived barriers on climate-friendly food choices: multiple regression analysis. |
| Markowski and Roxburgh. “If I became a vegan, my family and friends would hate me:” Anticipating vegan stigma as a barrier to plant-based diets (2019) [46]. | The United States of America | Total n = 34. Females: n = 26. Males: n = 8. Students: 100%. | Qualitative interviews with the use of focus groups. | Individual perceptions; Stigmatisation; Barriers; Meat consumption. | Coding of transcripts. |
| Von Essen. Young adults’ transition to a plant-based diet as a psychosomatic process: A psychoanalytically informed perspective (2021) [47]. | Sweden | Total n = 9. Age: 18–35 years. | Qualitative semi-structured interviews. | Individual perceptions; Dietary transition; Challenges. | Descriptive phenomenological psychological method. |
| Barrier Identified | References of the Studies That Included Each Barrier |
|---|---|
| Financial | |
| 1. Perception of high prices for plant-based foods; | 40, 45 |
| 2. Cost. | 40 |
| Lack of knowledge | |
| 3. Lack of information on knowing what to eat; | 39, 40, 42, 45, 46 |
| 4. Lack of familiarity with plant-based foods/diets; | 39, 40, 43, 46 |
| 5. Nutritional knowledge; | 38, 40, 44, 47 |
| 6. Believing eating patterns are trivial; | 44 |
| 7. Education; | 40, 42 |
| 8. Confusion surrounding the terms and definitions of plant-based diets. | 39, 41, 44, 46 |
| Emotional | |
| 9. Distrust/mistrust in food systems and suppliers; | 40, 44, 45 |
| 10. Stigma; | 39, 41, 46 |
| 11. Food neophobia; | 42 |
| 12. Gender stereotypes; | 40, 42 |
| 13. Fear of judgement; | 41, 46 |
| 14. Powerlessness over food choices. | 41, 44, 45, 47 |
| Health | |
| 15. Nutritional deficiencies; | 38, 42, 47 |
| 16. Nutritional intake/requirements; | 38, 40, 41, 42, 46, 47 |
| 17. Dietary diversity; | 38, 41 |
| 18. Anxiety with the worry of not consuming the necessary nutrients. | 38, 47 |
| Convenience | |
| 19. Time; | 38, 40, 41, 45 |
| 20. Food preparation; | 38, 40 |
| 21. More energy and effort needed; | 40 |
| 22. Difficulties with creating plant-based meals. | 38, 40 |
| Social | |
| 23. Fear of missing out/not following social norms; | 41, 45, 46 |
| 24. Lack of support/a support network; | 38, 46 |
| 25. Living situation; | 38, 41 |
| 26. Traditions; | 44 |
| 27. Family and friend expectations and pressures. | 38, 40, 46 |
| Enjoyment of meat | |
| 28. Personal and family enjoyment; | 38, 39, 40 |
| 29. Resisting temptations; | 46 |
| 30. Cravings; | 40, 41, 44 |
| 31. Taste. | 38, 41, 42 |
| Environmental | |
| 32. Scepticisms around the dietary impact; | 44, 45 |
| 33. Disbelief in climate change. | 44 |
| Accessibility | |
| 34. Lack of options, especially when eating out; | 41, 44, 46 |
| 35. Lack of plant-based options to buy; | 41, 45 |
| 36. No autonomy/opportunity over food purchases. | 38, 41, 42, 47 |
| Personal ability | |
| 37. Lack of confidence in cooking ability and preparing plant-based meals; | 41 |
| 38. Cooking ability; | 38, 41 |
| 39. Habit. | 40, 42, 44, 45, 47 |
| Media | |
| 40. Advertisements promoting meat consumption. | 40 |
| Study | Score | Grading |
|---|---|---|
| Kemper (2020) [40]. | 9 | High |
| Kemper and White (2021) [41] . | 9 | High |
| Macdiarmid, Douglas, and Campbell (2016) [44]. | 9 | High |
| Markowski and Roxburgh (2019) [46]. | 7 | Moderate |
| Essen (2021) [47]. | 7 | Moderate |
| Barr and Chapman (2002) [38]. | 6 | Moderate |
| Faber, Castellanos-Feijoo, Sompel, Davydova, and Perez-Cueto (2020) [39]. | 9 | High |
| Lea, Crawford, and Worsley (2006) [42]. | 8 | High |
| Makiniemi and Vainio (2014) [45]. | 5 | Low |
| Lim, Okine, and Kershaw (2021) [43]. | + | Moderate |
| Barriers Identified | Level of Certainty | Times Mentioned |
|---|---|---|
| 1. Perception of high prices for plant-based foods | Moderate | 40, 45 |
| 2. Cost | Low | 40 |
| 3. Lack of information on knowing what to eat | Moderate | 39, 40, 42, 45, 46 |
| 4. Lack of familiarity with plant-based foods/diets | Moderate | 39, 40, 43, 46 |
| 5. Nutritional knowledge | Moderate | 38, 40, 44, 47 |
| 6. Believing eating patterns are trivial | Low | 44 |
| 7. Education | Moderate | 40, 42 |
| 8. Confusion surrounding the term and definitions of plant-based diets | Moderate | 39, 41, 44, 46 |
| 9. Distrust/mistrust in food systems and suppliers | Moderate | 40, 44, 45 |
| 10. Stigma | Moderate | 39, 41, 46 |
| 11. Food neophobia | Low | 42 |
| 12. Gender stereotypes | Moderate | 40, 42 |
| 13. Fear of judgement | Moderate | 41, 46 |
| 14. Powerlessness over food choices | Moderate | 41, 44, 45, 47 |
| 15. Nutritional deficiencies | Moderate | 38, 42, 47 |
| 16. Nutritional intake/requirements | High | 38, 40, 41, 42, 46, 47 |
| 17. Dietary diversity | Moderate | 38, 41 |
| 18. Anxiety with the worry of not consuming the necessary nutrients | Moderate | 38, 47 |
| 19. Time | Moderate | 38, 40, 41, 45 |
| 20. Food preparation | Moderate | 38, 40 |
| 21. More energy and effort needed | Low | 40 |
| 22. Difficulties with creating plant-based meals | Moderate | 38, 40 |
| 23. Fear of missing out/not following social norms | Moderate | 41, 45, 46 |
| 24. Lack of support/a support network | Moderate | 38, 46 |
| 25. Living situation | Moderate | 38, 41 |
| 26. Traditions | Low | 44 |
| 27. Family and friend expectations and pressures | Moderate | 38, 40, 46 |
| 28. Personal and family enjoyment | Moderate | 38, 39, 40 |
| 29. Resisting temptations | Low | 46 |
| 30. Cravings | Moderate | 40, 41, 44 |
| 31. Taste | Moderate | 38, 41, 42 |
| 32. Scepticisms around the dietary impact | Moderate | 44, 45 |
| 33. Disbelief in climate change | Low | 44 |
| 34. Lack of options, especially when eating out | Moderate | 41, 44, 46 |
| 35. Lack of plant-based options to buy | Moderate | 41, 45 |
| 36. No autonomy/opportunity over food purchases | Moderate | 38, 41, 42, 47 |
| 37. Lack of confidence in cooking ability and preparing plant-based meals | Low | 41 |
| 38. Cooking ability | Moderate | 38, 41 |
| 39. Habit | Moderate | 40, 42, 44, 45, 47 |
| 40. Advertisements promoting meat consumption | Low | 40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rickerby, A.; Green, R. Barriers to Adopting a Plant-Based Diet in High-Income Countries: A Systematic Review. Nutrients 2024, 16, 823. https://doi.org/10.3390/nu16060823
Rickerby A, Green R. Barriers to Adopting a Plant-Based Diet in High-Income Countries: A Systematic Review. Nutrients. 2024; 16(6):823. https://doi.org/10.3390/nu16060823
Chicago/Turabian StyleRickerby, Alice, and Rosemary Green. 2024. "Barriers to Adopting a Plant-Based Diet in High-Income Countries: A Systematic Review" Nutrients 16, no. 6: 823. https://doi.org/10.3390/nu16060823
APA StyleRickerby, A., & Green, R. (2024). Barriers to Adopting a Plant-Based Diet in High-Income Countries: A Systematic Review. Nutrients, 16(6), 823. https://doi.org/10.3390/nu16060823