
Healthful Eating Behaviors among Couples Contribute to Lower Gestational Weight Gain
 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Overview of the GLOWING Study
2.2. Assessment of Participant Demographics
2.3. Pregnant Persons’ and Non-Pregnant Partners’ Weight and Body Mass Index (BMI)
2.4. Gestational Weight Gain (GWG)
2.5. Pregnant Persons and Non-Pregnant Partners’ Eating Behaviors
2.6. Statistical Analyses and Power Analysis Calculations
3. Results
3.1. Overall Participant Demographics
3.2. Gestational Weight Gain
3.3. Parental Eating Inventory Eating Behaviors
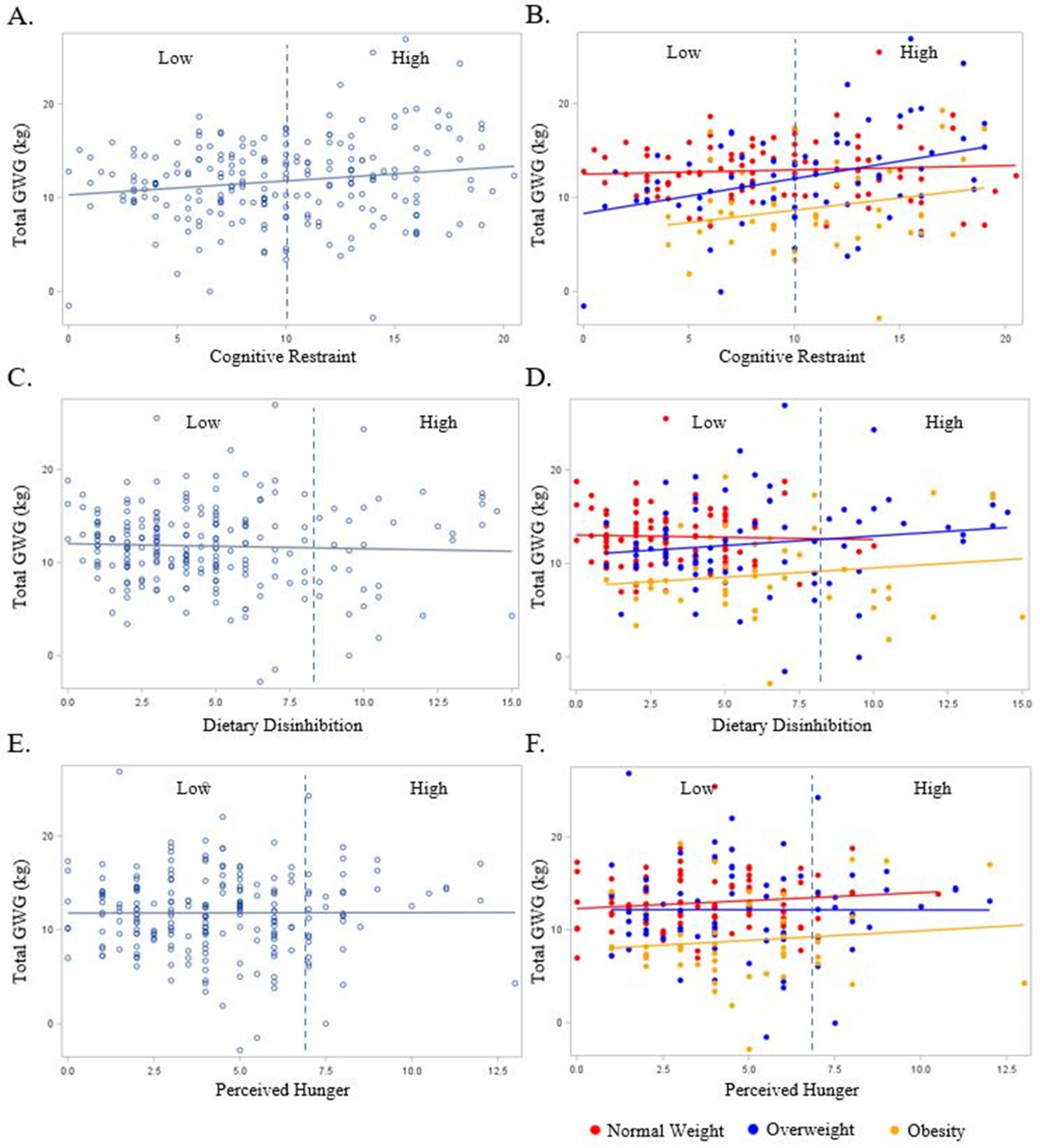
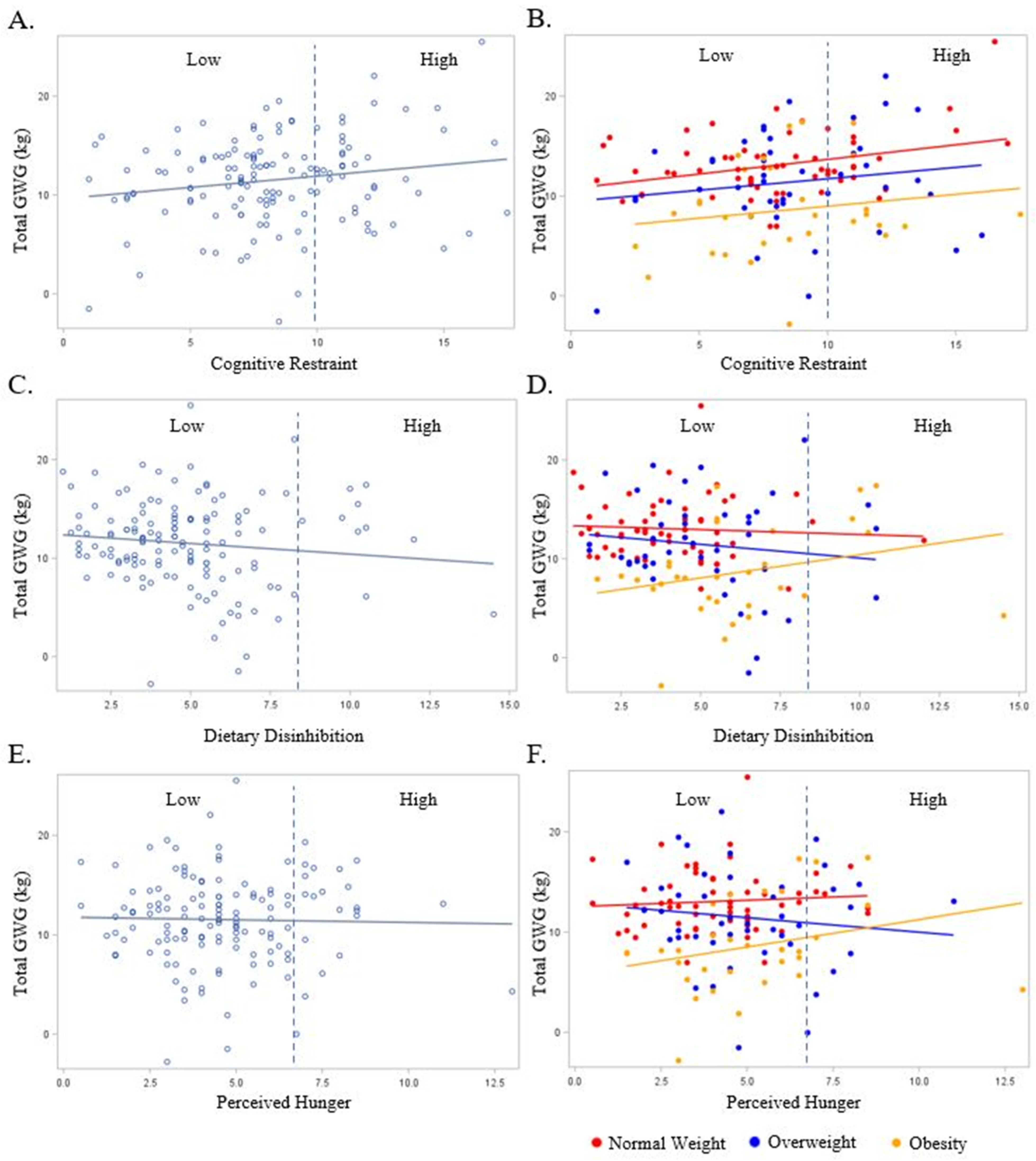
3.4. Relationships between the Pregnant Persons’ Eating Behaviors with GWG
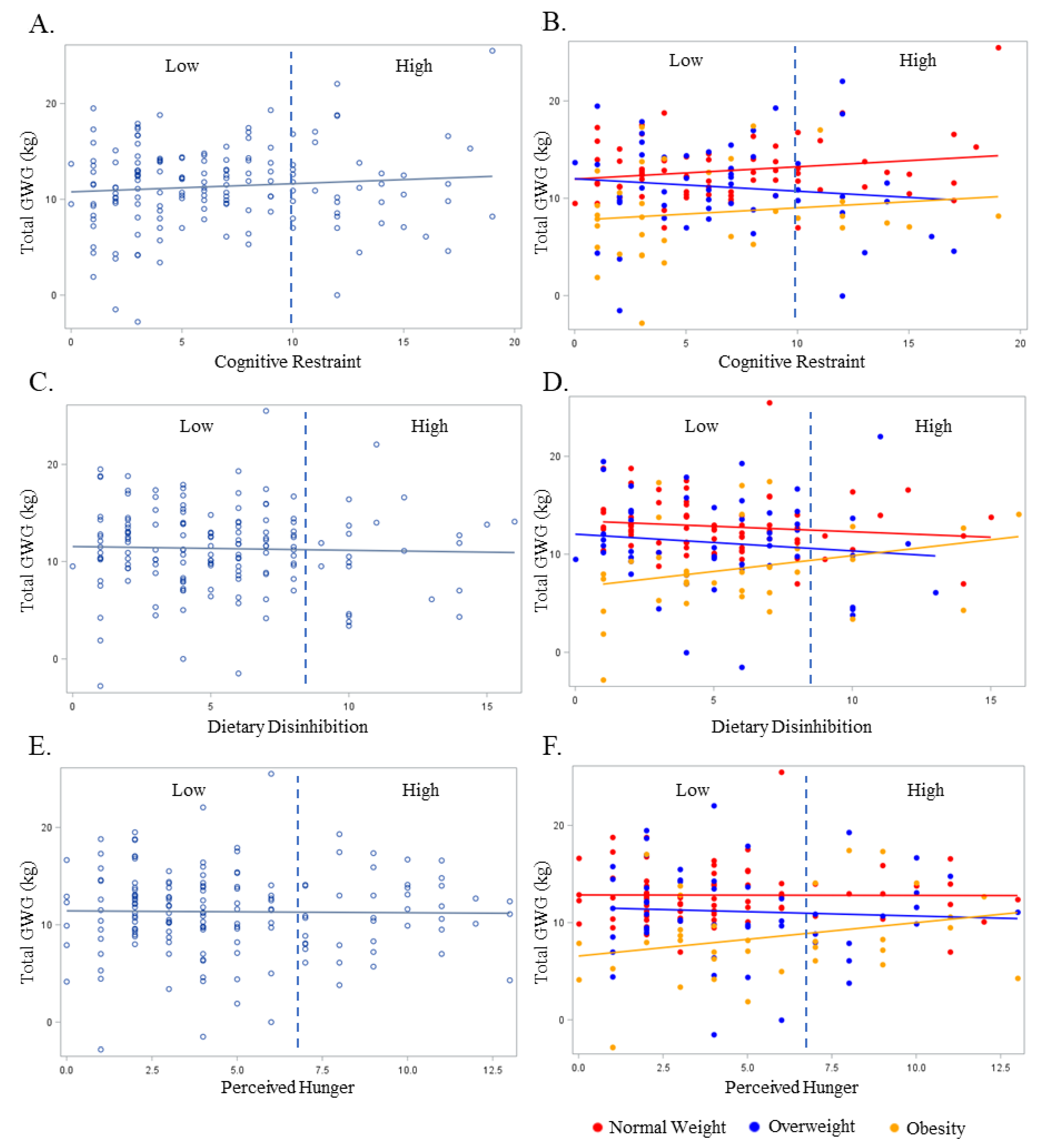
3.5. Relationships between Non-Pregnant Partners’ Eating Behaviors with GWG
3.6. Relationship between the Average Eating Behaviors of the Pregnant Persons and Non-Pregnant Partners with GWG
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hedderson, M.M.; Gunderson, E.P.; Ferrara, A. Gestational Weight Gain and Risk of Gestational Diabetes Mellitus. Obstet. Gynecol. 2010, 115, 597–604. [Google Scholar] [CrossRef]
- Gavard, J.A.; Artal, R. Gestational Weight Gain and Maternal and Neonatal Outcomes in Term Twin Pregnancies in Obese Women. Twin Res. Hum. Genet. 2014, 17, 127–133. [Google Scholar] [CrossRef]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain with Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Chiavaroli, V.; Hopkins, S.A.; Biggs, J.B.; Rodrigues, R.O.; Seneviratne, S.N.; Baldi, J.C.; McCowan, L.M.E.; Cutfield, W.S.; Hofman, P.L.; Derraik, J.G.B. The associations between maternal BMI and gestational weight gain and health outcomes in offspring at age 1 and 7 years. Sci. Rep. 2021, 11, 20865. [Google Scholar] [CrossRef]
- Rasmussen, K.; Yaktine, A.L.; US Institute of Medicine; National Research Council Committee to Reexamine IOM Pregnancy Weight Guidelines. Food and Nutrition Board, Board on Children, Youth and Families, Institute of Medicine, National Research Council. Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Kominiarek, M.A.; Peaceman, A.M. Gestational weight gain. Am. J. Obstet. Gynecol. 2017, 217, 642–651. [Google Scholar] [CrossRef]
- Force, U.P.S.T.; Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Krist, A.H.; et al. Behavioral Counseling Interventions for Healthy Weight and Weight Gain in Pregnancy. JAMA 2021, 325, 2087–2093. [Google Scholar] [CrossRef]
- Harrison, C.L.; Khomami, M.B.; Enticott, J.; Thangaratinam, S.; Rogozińska, E.; Teede, H.J. Key Components of Antenatal Lifestyle Interventions to Optimize Gestational Weight Gain. JAMA Netw. Open 2023, 6, e2318031. [Google Scholar] [CrossRef] [PubMed]
- Gilmore, L.A.; Ravussin, E.; Bray, G.A.; Han, H.; Redman, L.M. An objective estimate of energy intake during weight gain using the intake-balance method. Am. J. Clin. Nutr. 2014, 100, 806–812. [Google Scholar] [CrossRef] [PubMed]
- de Jersey, S.J.; Mallan, K.; Callaway, L.; Daniels, L.A.; Nicholson, J.M. A cross sectional comparison of predisposing, reinforcing and enabling factors for lifestyle health behaviours and weight gain in healthy and overweight pregnant women. Matern. Child Health J. 2016, 21, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Most, J.; Amant, M.S.; Hsia, D.S.; Altazan, A.D.; Thomas, D.M.; Gilmore, L.A.; Vallo, P.M.; Beyl, R.A.; Ravussin, E.; Redman, L.M. Evidence-based recommendations for energy intake in pregnant women with obesity. J. Clin. Investig. 2019, 129, 4682–4690. [Google Scholar] [CrossRef] [PubMed]
- Paulino, D.S.M.; Pinho-Pompeu, M.; Raikov, F.; Freitas-Jesus, J.V.; Machado, H.C.; Surita, F.G. The Role of Health-related Behaviors in Gestational Weight Gain among Women with Overweight and Obesity: A Cross-sectional Analysis. Rev. Bras. Hematol. Hemoter. 2020, 42, 316–324. [Google Scholar] [CrossRef]
- Vanhees, K.; Vonhögen, I.G.C.; van Schooten, F.J.; Godschalk, R.W.L. You are what you eat, and so are your children: The impact of micronutrients on the epigenetic programming of offspring. Cell. Mol. Life Sci. 2014, 71, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Vaiserman, A.M. Epigenetic programming by early-life stress: Evidence from human populations. Dev. Dyn. 2015, 244, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Toivonen, K.I.; Oinonen, K.A.; Duchene, K.M. Preconception health behaviours: A scoping review. Prev. Med. 2017, 96, 1–15. [Google Scholar] [CrossRef]
- Wang, Y.; Min, J.; Khuri, J.; Li, M. A systematic examination of the association between parental and child obesity across countries. Adv. Nutr. Int. Rev. J. 2017, 8, 436–448. [Google Scholar] [CrossRef] [PubMed]
- Kebbe, M.; Flanagan, E.W.; Sparks, J.R.; Redman, L.M. Eating behaviors and dietary patterns of women during pregnancy: Optimizing the universal ‘Teachable Moment’. Nutrients 2021, 13, 3298. [Google Scholar] [CrossRef] [PubMed]
- Clark, M.; Ogden, J. The impact of pregnancy on eating behaviour and aspects of weight concern. Int. J. Obes. 1999, 23, 18–24. [Google Scholar] [CrossRef]
- Lane, M.; Robker, R.L.; Robertson, S.A. Parenting from before conception. Science 2014, 345, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Eberle, C.; Kirchner, M. Paternale Programmierung: Präkonzeptionelle Risikofaktor in Bezug auf das Diabetes-Risiko der Nachkommen. Diabetologie Stoffwechsel 2019, 14, P-079. [Google Scholar]
- Eberle, C.; Kirchner, M.F.; Herden, R.; Stichling, S. Paternal metabolic and cardiovascular programming of their offspring: A systematic scoping review. PLoS ONE 2020, 15, e0244826. [Google Scholar] [CrossRef]
- Kasman, A.M.; Zhang, C.A.; Li, S.; Stevenson, D.K.; Shaw, G.M.; Eisenberg, M.L. Association of preconception paternal health on perinatal outcomes: Analysis of U.S. claims data. Fertil. Steril. 2020, 113, 947–954. [Google Scholar] [CrossRef]
- Dimofski, P.; Meyre, D.; Dreumont, N.; Leininger-Muller, B. Consequences of Paternal Nutrition on Offspring Health and Disease. Nutrients 2021, 13, 2818. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, M.d.S.; Perez, G.d.S.; Ferreira, L.d.J.D.; dos Santos, L.S.; Cordeiro, G.d.S.; Couto, R.D.; Medeiros, J.M.B. Paternal high-fat diet exposure induces adverse effects on offspring health: A systematic review of animal studies. Braz. Arch. Biol. Technol. 2021, 64, e21190123. [Google Scholar] [CrossRef]
- Hieronimus, B.; Ensenauer, R. Influence of maternal and paternal pre-conception overweight/obesity on offspring outcomes and strategies for prevention. Eur. J. Clin. Nutr. 2021, 75, 1735–1744. [Google Scholar] [CrossRef] [PubMed]
- Billah, M.; Khatiwada, S.; Morris, M.J.; Maloney, C.A. Effects of paternal overnutrition and interventions on future generations. Int. J. Obes. 2022, 46, 901–917. [Google Scholar] [CrossRef] [PubMed]
- Shi, Q.; Qi, K. Developmental origins of health and disease: Impact of paternal nutrition and lifestyle. Pediatr. Investig. 2023, 7, 111–131. [Google Scholar] [CrossRef] [PubMed]
- Bagherzadeh, R.; Gharibi, T.; Safavi, B.; Mohammadi, S.Z.; Karami, F.; Keshavarz, S. Pregnancy; an opportunity to return to a healthy lifestyle: A qualitative study. BMC Pregnancy Childbirth 2021, 21, 751. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Hays, N.P.; Roberts, S.B. Aspects of eating behaviors “Disinhibition” and “Restraint” are related to weight gain and BMI in women. Obesity 2008, 16, 52–58. [Google Scholar] [CrossRef]
- Tang, X.; Andres, A.; West, D.S.; Lou, X.; Krukowski, R.A. Eating behavior and weight gain during pregnancy. Eat. Behav. 2020, 36, 101364. [Google Scholar] [CrossRef]
- Slane, J.D.; Levine, M.D. Association of restraint and disinhibition to gestational weight gain among pregnant former smokers. Women’s Health Issues 2015, 25, 390–395. [Google Scholar] [CrossRef][Green Version]
- Waters, T.E.A.; Raby, K.L.; Ruiz, S.K.; Martin, J.; Roisman, G.I. Adult attachment representations and the quality of romantic and parent–child relationships: An examination of the contributions of coherence of discourse and secure base script knowledge. Dev. Psychol. 2018, 54, 2371–2381. [Google Scholar] [CrossRef]
- Sparks, J.R.; Phelan, S.; Drews, K.L.; Redman, L.M. The partner-an underutilized facilitator to support healthy gestational weight gain. BMC Pregnancy Childbirth 2023, 23, 446. [Google Scholar] [CrossRef]
- Rhodes, A.; Smith, A.D.; Llewellyn, C.H.; Croker, H. Investigating partner involvement in pregnancy and identifying barriers and facilitators to participating as a couple in a digital healthy eating and physical activity intervention. BMC Pregnancy Childbirth 2021, 21, 450. [Google Scholar] [CrossRef]
- Krukowski, R.A.; West, D.; DiCarlo, M.; Shankar, K.; Cleves, M.A.; Tedford, E.; Andres, A. A Behavioral Intervention to Reduce Excessive Gestational Weight Gain. Matern. Child Health J. 2016, 21, 485–491. [Google Scholar] [CrossRef]
- Diaz, E.C.; Cleves, M.A.; DiCarlo, M.; Sobik, S.R.; Ruebel, M.L.; Thakali, K.M.; Sims, C.R.; Dajani, N.K.; Krukowski, R.A.; Børsheim, E.; et al. Parental adiposity differentially associates with newborn body composition. Pediatr. Obes. 2020, 15, e12596. [Google Scholar] [CrossRef]
- Gilmore, L.A.; Redman, L.M. Weight gain in pregnancy and application of the 2009 IOM guidelines: Toward a uniform approach. Obesity 2015, 23, 507–511. [Google Scholar] [CrossRef]
- Most, J.; Dervis, S.; Haman, F.; Adamo, K.B.; Redman, L.M. Energy Intake Requirements in Pregnancy. Nutrients 2019, 11, 1812. [Google Scholar] [CrossRef] [PubMed]
- You, Z.; Shan, L.; Cheng, S.; Xia, Y.; Zhao, Y.; Zhang, H.; Zhao, Z. Dietary intake patterns during pregnancy and excessive gestational weight gain: A systematic review and meta-analysis. Food Funct. 2023, 14, 5910–5920. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F.; Clément, K.; Le Barzic, M.; Le Gall, A.; Guy-Grand, B.; Basdevant, A. The eating inventory and body adiposity from leanness to massive obesity: A study of 2509 adults. Obes. Res. 2004, 12, 2023–2030. [Google Scholar] [CrossRef] [PubMed]
- Heinonen, K. Strengthening Antenatal Care towards a Salutogenic Approach: A Meta-Ethnography. Int. J. Environ. Res. Public Health 2021, 18, 5168. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Shi, W.-X.; Parsons, J.; Forbes, A.; Kong, M.; Zhang, Y.-P.; Yang, H.; Forde, R. The effects of a couple-based gestational diabetes mellitus intervention on self-management and pregnancy outcomes: A randomised controlled trial. Diabetes Res. Clin. Pract. 2023, 205, 110947. [Google Scholar] [CrossRef]
- Meghea, C.I.; Brinzaniuc, A.; Sidor, A.; Chereches, R.M.; Mihu, D.; Iuhas, C.; Stamatian, F.; Caracostea, G.; Dascal, M.D.; Foley, K.; et al. A couples-focused intervention for smoking cessation during pregnancy: The study protocol of the Quit Together pilot randomized controlled trial. Tob. Prev. Cessat. 2018, 4, 17. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, M.E.; Roettger, M.E.; Jones, D.E.; Paul, I.M.; Kan, M.L. Effects of a psychosocial couple-based prevention program on adverse birth outcomes. Matern. Child Health J. 2015, 19, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Ngai, F.; Wong, P.W.; Chung, K.; Chau, P.; Hui, P. Effect of couple-based cognitive behavioural intervention on prevention of postnatal depression: Multisite randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, J.; Persson, L.-O.; Sjöström, L.; Sullivan, M. Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int. J. Obes. 2000, 24, 1715–1725. [Google Scholar] [CrossRef]
- Cappelleri, J.C.; Bushmakin, A.G.; Gerber, R.A.; Leidy, N.K.; Sexton, C.C.; Lowe, M.R.; Karlsson, J. Psychometric analysis of the Three-Factor Eating Questionnaire-R21: Results from a large diverse sample of obese and non-obese participants. Int. J. Obes. 2009, 33, 611–620. [Google Scholar] [CrossRef]
- Swartz, M.C.; Basen-Engquist, K.M.; Markham, C.; Lyons, E.J.; Cox, M.; Chandra, J.; Ater, J.L.; Askins, M.A.; Scheurer, M.E.; Lupo, P.J.; et al. Psychometric analysis of the three-factor eating questionnaire-R18V2 in adolescent and young adult-aged central nervous system tumor survivors. J. Adolesc. Young Adult Oncol. 2016, 5, 278–285. [Google Scholar] [CrossRef]
- Most, J.; Rebello, C.J.; Altazan, A.D.; Martin, C.K.; Amant, M.S.; Redman, L.M. Behavioral Determinants of Objectively Assessed Diet Quality in Obese Pregnancy. Nutrients 2019, 11, 1446. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pregnant Person (n = 218) | Non-Pregnant Partner (n = 157) | p-Value | |
|---|---|---|---|
| Age (Mean ± SD) | 30.3 ± 3.7 | 31.4 ± 4.1 | 0.07 |
| Body Mass Index (BMI; kg/m2; Mean ± SD) | 26.1 ± 4.3 | 28.5 ± 5.2 | <0.0001 |
| Normal Weight, N (%) | 99 (45.4) | 44 (28.0) | <0.0001 |
| Overweight, N (%) | 73 (33.5) | 62 (39.5) | |
| Obesity, N (%) | 46 (21.1) | 51 (35.5) | |
| Marital Status * | |||
| Married or Cohabiting, N (%) | 191 (87.6) | - | |
| Single, Divorced, or Unknown/Not Reported, N (%) | 27 (12.4) | - | |
| Race/Ethnicity | 0.68 | ||
| White/Caucasian, N (%) | 169 (77.5) | 129 (82.2) | |
| Black/African American, N (%) | 22 (10.1) | 16 (10.2) | |
| Asian or more than One Race, N (%) | 3 (1.4) | 0 (0.0) | |
| Unknown or Not Reported, N (%) | 24 (11.0) | 12 (7.6) | |
| Highest Education Completed | <0.001 | ||
| <College Graduate, N (%) | 120 (55.0) | 65 (41.4) | |
| ≥College Graduate, N (%) | 76 (34.9) | 73 (46.5) | |
| Unknown/Not Reported, N (%) | 22 (10.1) | 19 (12.1) | |
| Individual Income | 0.01 | ||
| <USD 40,000 USD, N (%) | 92 (42.2) | 50 (31.9) | |
| ≥USD 40,000 USD, N (%) | 70 (32.1) | 92 (58.6) | |
| Unknown/Not Reported, N (%) | 56 (25.7) | 15 (9.5) |
| Pregnant Person | Overall (218) | Normal Weight (99) | Overweight (73) | Obesity (46) |
|---|---|---|---|---|
| Gestational Weight Gain (Total; kg) | 11.8 ± 4.3 | 12.9 ± 3.0 * | 12.1 ± 4.9 * | 8.8 ± 4.5 |
| Inadequate, N (%) | 26 (12.0) | 14 (14.4) ‡ | 6 (8.2) | 6 (13.0) |
| Recommended, N (%) | 86 (39.4) | 49 (49.5) ‡ | 21 (28.8) | 16 (34.8) |
| Excess, N (%) | 106 (48.6) | 36 (36.1) ‡ | 46 (63.0) | 24 (52.2) |
| The Eating Inventory | ||||
| Cognitive Restraint, M ± SD | 9.8 ± 4.7 †† | 9.0 ± 4.8 ‡ | 10.3 ± 4.8 | 10.7 ± 4.1 |
| Low, N (%) | 124 (56.9) †† | 62 (62.6) ‡ | 38 (52.0) | 24 (52.2) |
| High, N (%) | 94 (43.1) †† | 37 (37.4) ‡ | 35 (48.0) | 22 (47.8) |
| Dietary Disinhibition, M ± SD | 4.8 ± 3.2 | 3.2 ± 2.0 ‡ | 6.0 ± 3.4 | 6.5 ± 3.5 |
| Low, N (%) | 187 (85.8) | 97 (98.0) ‡ | 56 (76.7) | 34 (73.9) |
| High, N (%) | 31 (14.2) | 2 (2.0) ‡ | 17 (23.3) | 12 (26.1) |
| Perceived Hunger, M ± SD | 4.4 ± 2.5 | 3.7 ± 2.1 ‡ | 5.0 ± 2.6 | 4.9 ± 2.6 |
| Low, N (%) | 193 (88.5) | 95 (96.0) ‡ | 58 (79.5 | 40 (87.0) |
| High, N (%) | 25 (11.5) | 4 (4.0) ‡ | 15 (20.5) | 6 (13.0) |
| Non-Pregnant Partner | Overall (157) | Normal Weight (72) | Overweight (51) | Obese (34) |
| The Eating Inventory | ||||
| Cognitive Restraint, M ± SD | 6.6 ± 4.6 †† | 6.8 ± 4.7 | 6.8 ± 4.2 | 5.8 ± 4.8 |
| Low, N (%) | 127 (80.9) †† | 59 (81.9) | 41 (80.4) | 27 (79.4) |
| High, N (%) | 30 (19.1) †† | 13 (18.1) | 10 (19.6) | 7 (20.6) |
| Dietary Disinhibition, M ± SD | 5.4 ± 3.4 | 5.3 ± 3.2 | 5.3 ± 3.3 | 5.8 ± 3.8 |
| Low, N (%) | 134 (85.4) | 63 (87.5) | 43 (84.3) | 28 (82.4) |
| High, N (%) | 23 (14.6) | 9 (12.5) | 8 (15.7) | 6 (17.6) |
| Perceived Hunger, M ± SD | 4.7 ± 3.2 | 4.3 ± 3.1 | 4.8 ± 3.1 | 5.6 ± 3.6 |
| Low, N (%) | 125 (79.6) | 61 (84.7) | 40 (78.4) | 24 (70.6) |
| High, N (%) | 32 (20.4) | 11 (15.3) | 11 (21.6) | 10 (29.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sparks, J.R.; Redman, L.M.; Drews, K.L.; Sims, C.R.; Krukowski, R.A.; Andres, A. Healthful Eating Behaviors among Couples Contribute to Lower Gestational Weight Gain. Nutrients 2024, 16, 822. https://doi.org/10.3390/nu16060822
Sparks JR, Redman LM, Drews KL, Sims CR, Krukowski RA, Andres A. Healthful Eating Behaviors among Couples Contribute to Lower Gestational Weight Gain. Nutrients. 2024; 16(6):822. https://doi.org/10.3390/nu16060822
Chicago/Turabian StyleSparks, Joshua R., Leanne M. Redman, Kimberly L. Drews, Clark R. Sims, Rebecca A. Krukowski, and Aline Andres. 2024. "Healthful Eating Behaviors among Couples Contribute to Lower Gestational Weight Gain" Nutrients 16, no. 6: 822. https://doi.org/10.3390/nu16060822
APA StyleSparks, J. R., Redman, L. M., Drews, K. L., Sims, C. R., Krukowski, R. A., & Andres, A. (2024). Healthful Eating Behaviors among Couples Contribute to Lower Gestational Weight Gain. Nutrients, 16(6), 822. https://doi.org/10.3390/nu16060822