
Opposing Effects of Nutritional Supply on Bone Health at Different Ages: Based on the National Health and Nutrition Examination Survey Database

Abstract
1. Introduction
2. Materials and Methods
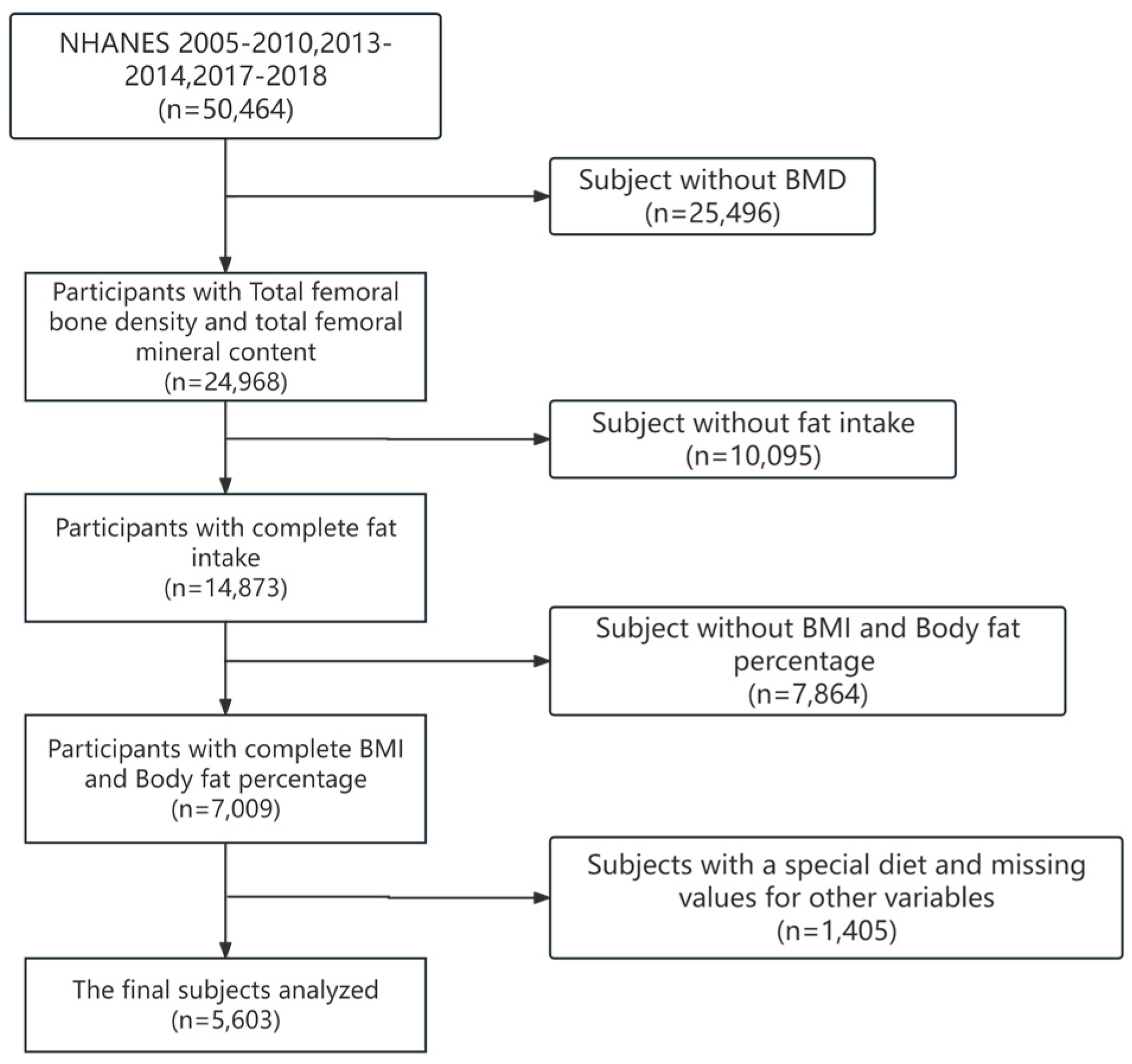
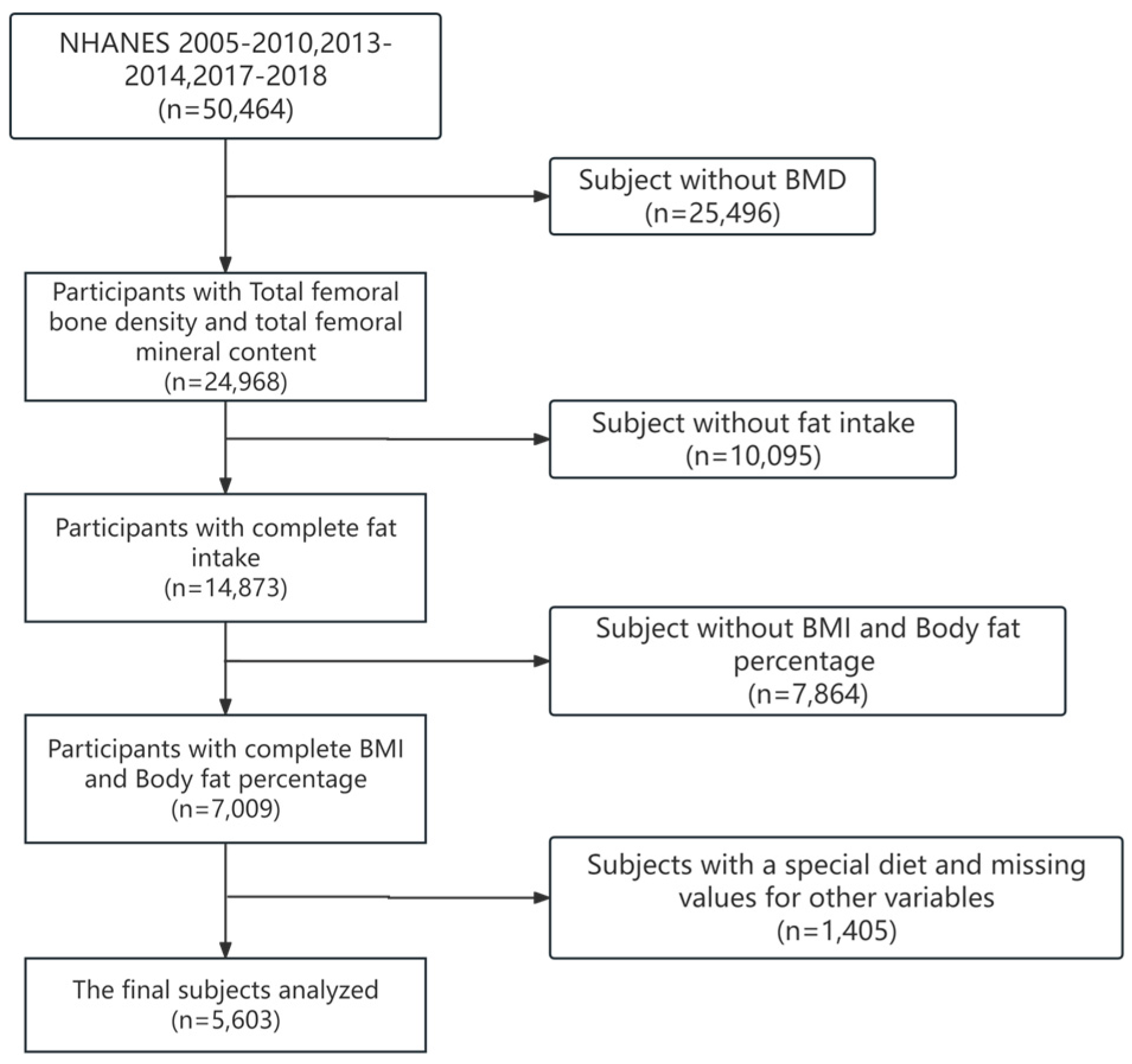
2.1. Data Sources
2.2. Evaluation of Dietary Data
2.3. Assessment of Bone Mineral Density
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Subjects
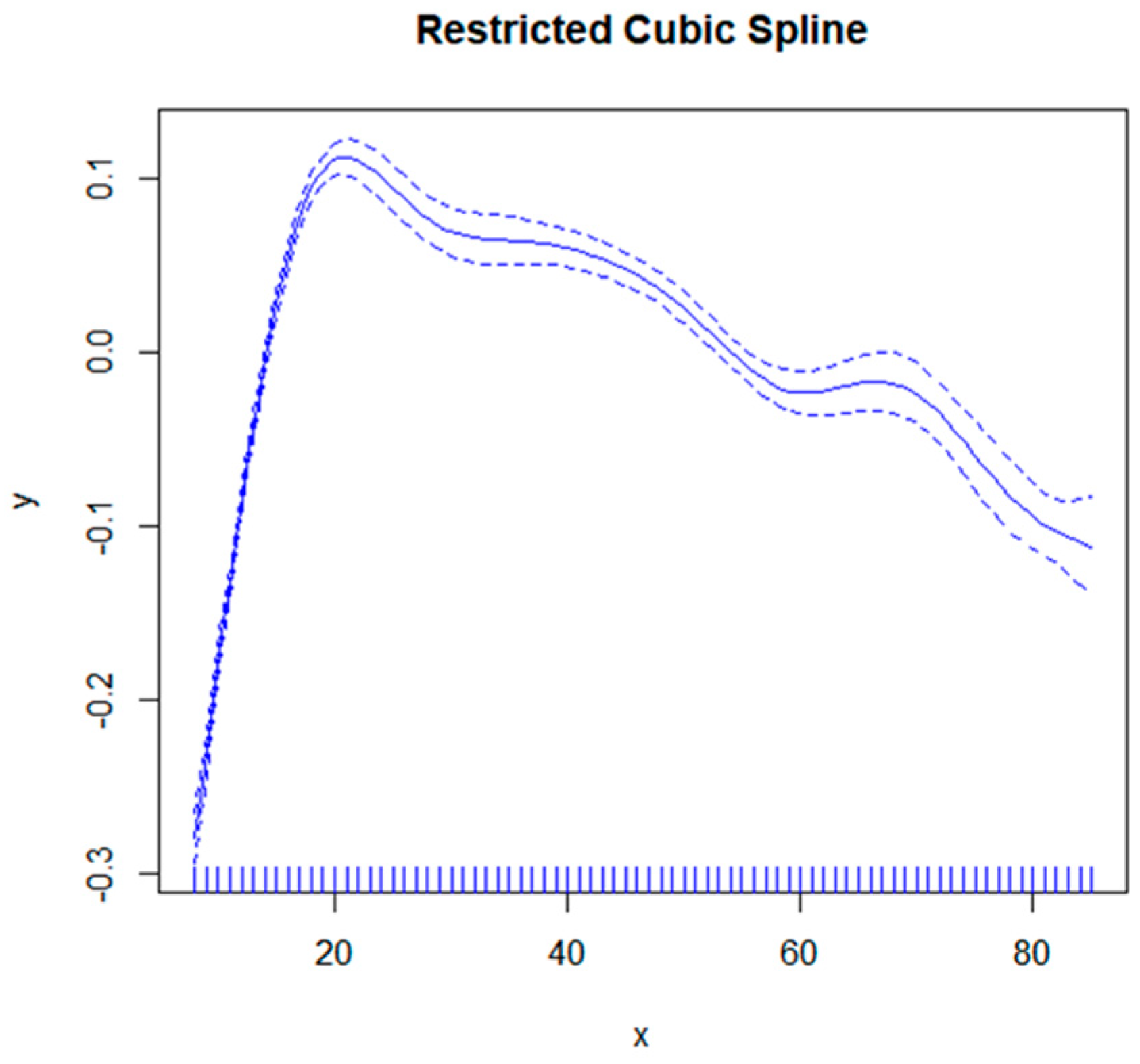
3.2. Correlation between Age and Bone Mineral Density
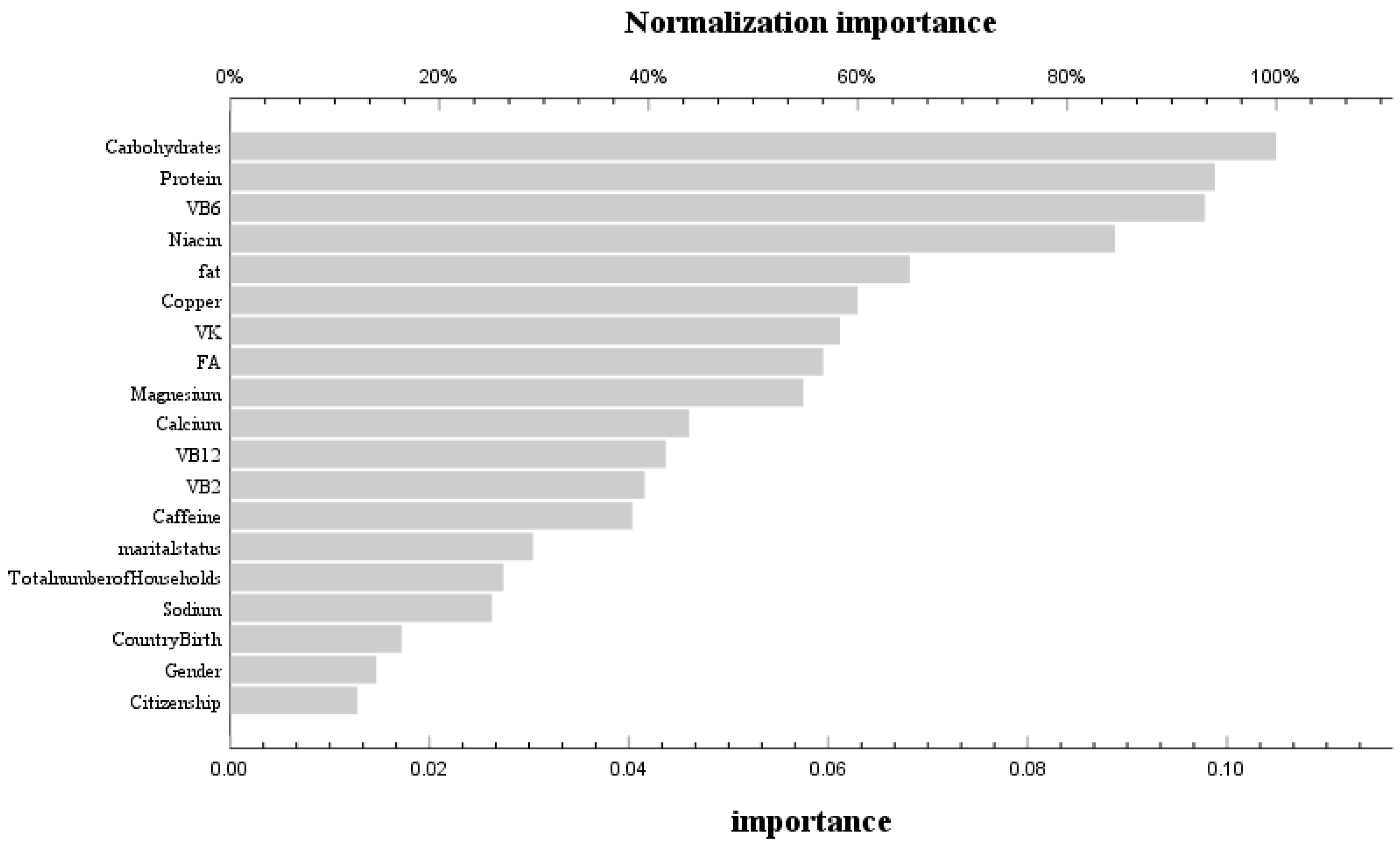
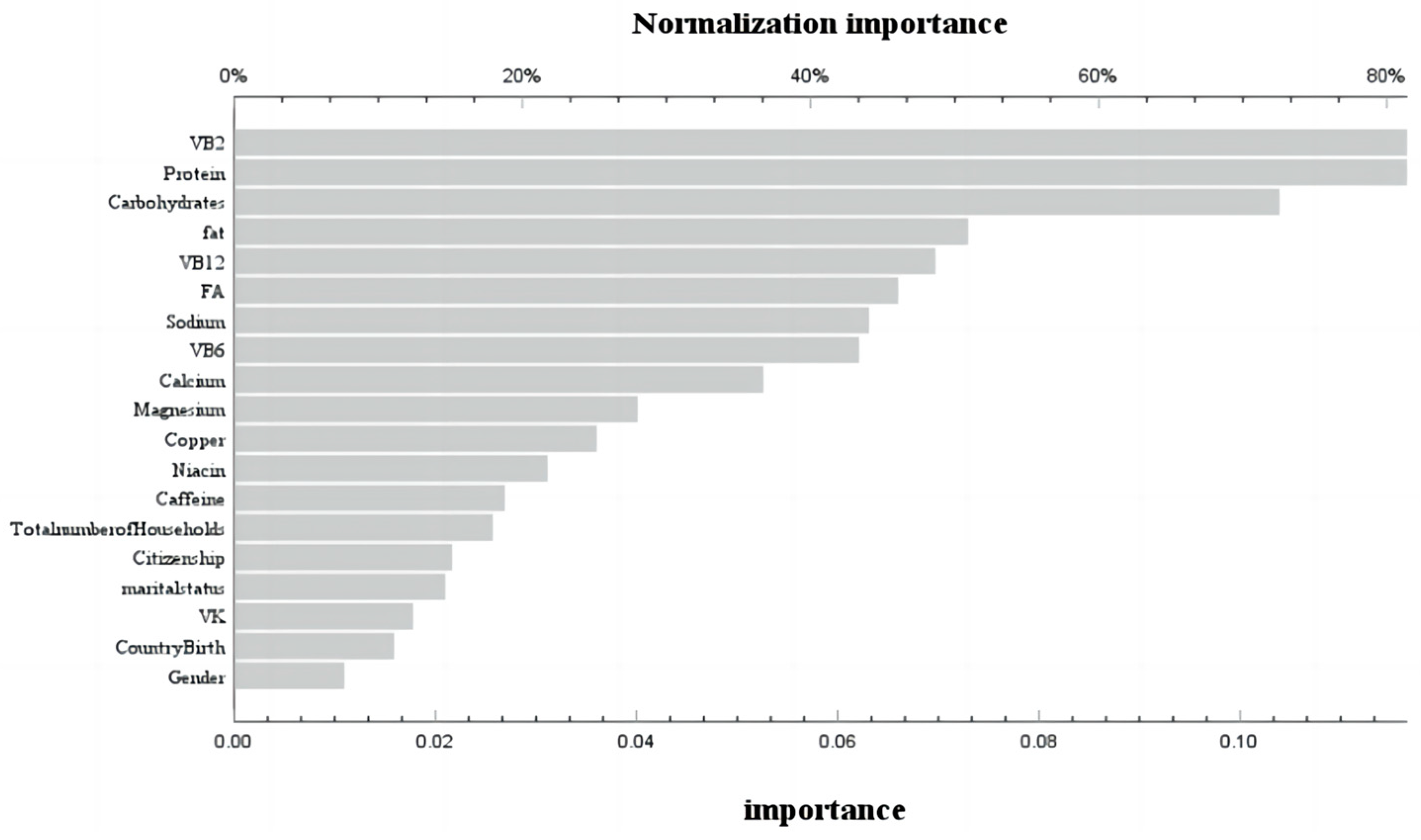
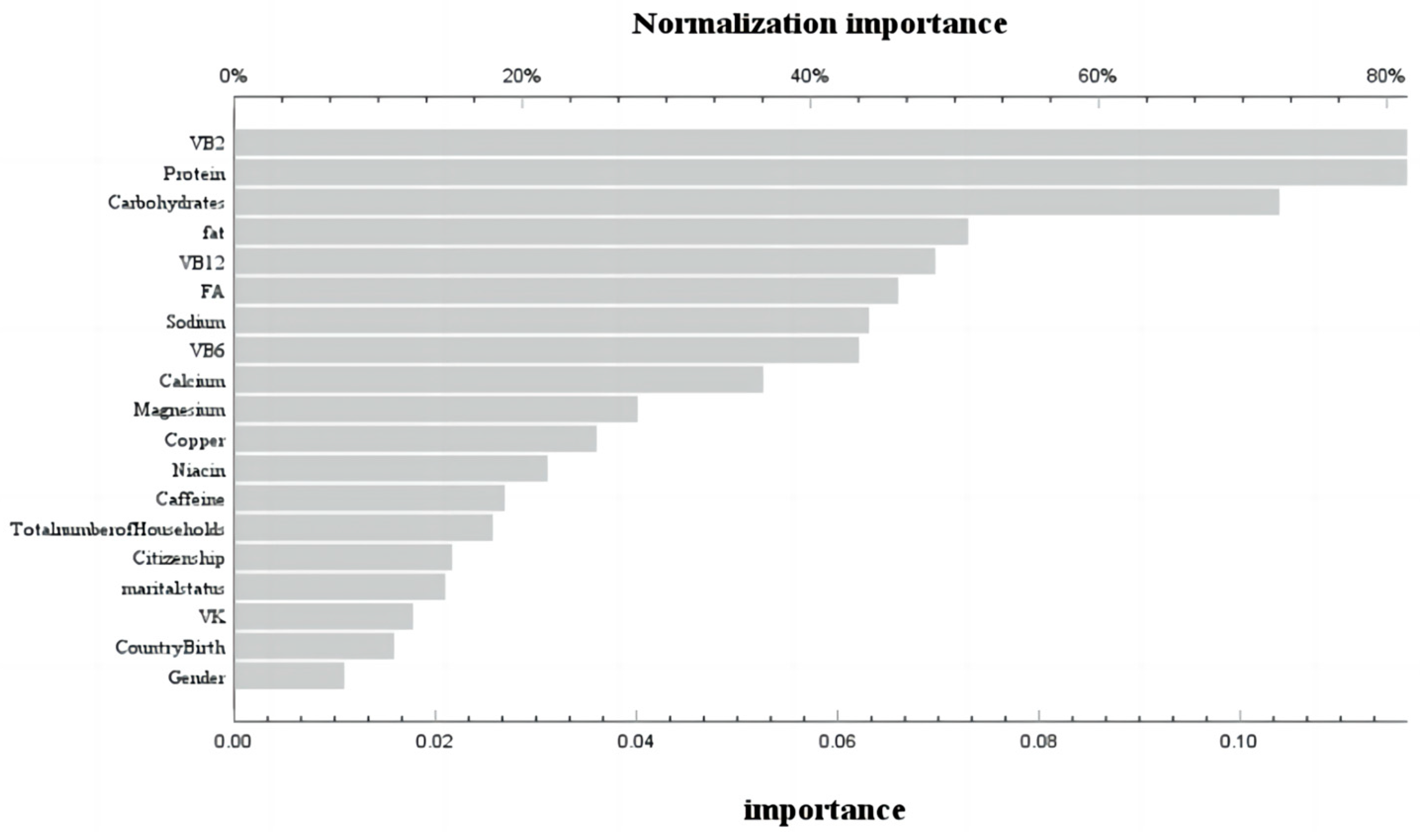
3.3. Machine Learning Using Neural Network Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ensrud, K.E.; Crandall, C.J. Osteoporosis. Ann. Intern. Med. 2017, 167, ITC17–ITC32. [Google Scholar] [CrossRef] [PubMed]
- Brown, C. Osteoporosis: Staying strong. Nature 2017, 550, S15–S17. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.A.; Chapurlat, R. Imminent fracture risk. Jt. Bone Spine 2021, 88, 105105. [Google Scholar] [CrossRef] [PubMed]
- Lane, N.E. Epidemiology, etiology, and diagnosis of osteoporosis. Am. J. Obstet. Gynecol. 2006, 194, S3–S11. [Google Scholar] [CrossRef]
- Mundy, G.R. Osteoporosis: Pathophysiology and non-pharmacological management. Best Pract. Res. Clin. Rheumatol. 2001, 15, 727–745. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.M.; Gordon, C.M.; Janz, K.F.; Kalkwarf, H.J.; Lappe, J.M.; Lewis, R.; O’Karma, M.; Wallace, T.C.; Zemel, B.S. Erratum to: The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: A systematic review and implementation recommendations. Osteoporos. Int. 2016, 27, 1387. [Google Scholar] [CrossRef]
- Rubio-Gutierrez, J.C.; Mendez-Hernandez, P.; Gueguen, Y.; Galichon, P.; Tamayo-Ortiz, M.; Haupt, K.; Medeiros, M.; Barbier, O.C. Overview of Traditional and Environmental Factors Related to Bone Health. Environ. Sci. Pollut. Res. 2022, 29, 31042–31058. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Xie, Y.; Wang, L.; Huang, G.; Cheng, Y.; Hou, D.; Liu, W.; Zhang, T.; Liu, J. The Association between Lead Exposure and Bone Mineral Density in Childhood and Adolescence: Results from NHANES 1999–2006 and 2011–2018. Nutrients 2022, 14, 1523. [Google Scholar] [CrossRef]
- Ho, S.C.; Chan, S.G.; Yi, Q.; Wong, E.; Leung, P.C. Soy intake and the maintenance of peak bone mass in Hong Kong Chinese women. J. Bone Miner. Res. 2001, 16, 1363–1369. [Google Scholar] [CrossRef]
- Savegnago, R.P.; Nunes, B.N.; Caetano, S.L.; Ferraudo, A.S.; Schmidt, G.S.; Ledur, M.C.; Munari, D.P. Comparison of logistic and neural network models to fit to the egg production curve of White Leghorn hens. Poult. Sci. 2011, 90, 705–711. [Google Scholar] [CrossRef]
- Warin, K.; Limprasert, W.; Suebnukarn, S.; Paipongna, T.; Jantana, P.; Vicharueang, S. Maxillofacial fracture detection and classification in computed tomography images using convolutional neural network-based models. Sci. Rep. 2023, 13, 3434. [Google Scholar] [CrossRef]
- Alanazi, R. Identification and Prediction of Chronic Diseases Using Machine Learning Approach. J. Healthc. Eng. 2022, 2022, 2826127. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Chen, Y.; He, Q.; Wang, X.; Liao, Y.; Liu, J.; Liu, Z.; Huang, J.; Song, T. Bone age assessment from articular surface and epiphysis using deep neural networks. Math. Biosci. Eng. 2023, 20, 13133–13148. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, C.M.; Moonga, B.S.; Kovach, J.S. Cadmium, follicle-stimulating hormone, and effects on bone in women age 42–60 years, NHANES III. Environ. Res. 2010, 110, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Melamed, M.L.; Abramowitz, M.K. Serum bicarbonate and bone mineral density in US adults. Am. J. Kidney Dis. 2015, 65, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Hassanabadi, N.; Berger, C.; Papaioannou, A.; Cheung, A.M.; Rahme, E.; Leslie, W.D.; Goltzman, D.; Morin, S.N. Variation in bone mineral density and fractures over 20 years among Canadians: A comparison of the Canadian Multicenter Osteoporosis Study and the Canadian Longitudinal Study on Aging. Osteoporos. Int. 2023, 34, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Zhao, K.; Zha, X.; Du, X.; Li, Y.; Chen, S.; Wu, Y.; Li, S.; Lu, Y.; Zhang, Y.; et al. Opportunistic Screening Using Low-Dose CT and the Prevalence of Osteoporosis in China: A Nationwide, Multicenter Study. J. Bone Miner. Res. 2021, 36, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Elhakeem, A.; Heron, J.; Tobias, J.H.; Lawlor, D.A. Physical Activity Throughout Adolescence and Peak Hip Strength in Young Adults. Jama Netw. Open 2020, 3, e2013463. [Google Scholar] [CrossRef] [PubMed]
- Seeman, E. Growth in bone mass and size--are racial and gender differences in bone mineral density more apparent than real? J. Clin. Endocrinol. Metab. 1998, 83, 1414–1419. [Google Scholar]
- Prynne, C.J.; Mishra, G.D.; O’Connell, M.A.; Muniz, G.; Laskey, M.A.; Yan, L.; Prentice, A.; Ginty, F. Fruit and vegetable intakes and bone mineral status: A cross sectional study in 5 age and sex cohorts. Am. J. Clin. Nutr. 2006, 83, 1420–1428. [Google Scholar] [CrossRef]
- Seijo, M.; Bonanno, M.N.; Bryk, G.; Zeni, C.M.; Pita, M.D.P.M.; Zeni, S.N. Does Vitamin D Insufficiency Influence Prebiotic Effect on Calcium Absorption and Bone Retention? Calcif. Tissue Int. 2022, 111, 300–312. [Google Scholar] [CrossRef]
- Martiniakova, M.; Babikova, M.; Mondockova, V.; Blahova, J.; Kovacova, V.; Omelka, R. The Role of Macronutrients, Micronutrients and Flavonoid Polyphenols in the Prevention and Treatment of Osteoporosis. Nutrients 2022, 14, 523. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsen, B.; Madsen, J.S.; Tofteng, C.L.; Stilgren, L.; Bladbjerg, E.M.; Kristensen, S.R.; Brixen, K.; Mosekilde, L. Are effects of MTHFR (C677T) genotype on BMD confined to women with low folate and riboflavin intake? Analysis of food records from the Danish osteoporosis prevention study. Bone 2005, 36, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Chaves, N.A.; Yano, C.L.; Paredes-Gamero, E.J.; Machado, D.; Justo, G.Z.; Peppelenbosch, M.P.; Ferreira, C.V. Riboflavin and photoproducts in MC3T3-E1 differentiation. Toxicol. In Vitro 2010, 24, 1911–1919. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.R.; Jacques, P.F.; Selhub, J.; Fredman, L.; Tucker, K.L.; Samelson, E.J.; Kiel, D.P.; Cupples, L.A.; Hannan, M.T. Plasma B vitamins, homocysteine, and their relation with bone loss and hip fracture in elderly men and women. J. Clin. Endocrinol. Metab. 2008, 93, 2206–2212. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.E.; Harland, B.F.; Ross, E.; Gautz, L.; Dunn, M.A. Effects of dietary aluminum and niacin on chick tibiae. Poult. Sci. 1992, 71, 1188–1195. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.E.; Qiu, X.L.; Gautz, L.D.; Ross, E. Changes in dimensions and mechanical properties of bone in chicks fed high levels of niacin. Food Chem. Toxicol. 1995, 33, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Tartara, A.; Fossari, F.; Vecchio, V.; Faliva, M.A.; Naso, M.; Perna, S.; Nichetti, M.; Peroni, G. Adequate Intake and Supplementation of B Vitamins, in Particular Folic Acid, can Play a Protective Role in Bone Health. Curr. Aging Sci. 2022, 15, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Tjaderhane, L.; Larmas, M. A high sucrose diet decreases the mechanical strength of bones in growing rats. J. Nutr. 1998, 128, 1807–1810. [Google Scholar] [CrossRef]
- Terada, M.; Inaba, M.; Yano, Y.; Hasuma, T.; Nishizawa, Y.; Morii, H.; Otani, S. Growth-inhibitory effect of a high glucose concentration on osteoblast-like cells. Bone 1998, 22, 17–23. [Google Scholar] [CrossRef]
- Douard, V.; Sabbagh, Y.; Lee, J.; Patel, C.; Kemp, F.W.; Bogden, J.D.; Lin, S.; Ferraris, R.P. Excessive fructose intake causes 1,25-(OH)(2)D(3)-dependent inhibition of intestinal and renal calcium transport in growing rats. Am. J. Physiol. Endocrinol. Metab. 2013, 304, E1303–E1313. [Google Scholar] [CrossRef]
- Zhang, Q.; Ma, G.; Greenfield, H.; Zhu, K.; Du, X.; Foo, L.H.; Hu, X.; Fraser, D.R. The association between dietary protein intake and bone mass accretion in pubertal girls with low calcium intakes. Br. J. Nutr. 2010, 103, 714–723. [Google Scholar] [CrossRef]
- Vatanparast, H.; Bailey, D.A.; Baxter-Jones, A.D.; Whiting, S.J. The effects of dietary protein on bone mineral mass in young adults may be modulated by adolescent calcium intake. J. Nutr. 2007, 137, 2674–2679. [Google Scholar] [CrossRef]
- Remer, T.; Manz, F.; Alexy, U.; Schoenau, E.; Wudy, S.A.; Shi, L. Long-term high urinary potential renal acid load and low nitrogen excretion predict reduced diaphyseal bone mass and bone size in children. J. Clin. Endocrinol. Metab. 2011, 96, 2861–2868. [Google Scholar] [CrossRef]
- Ekbote, V.H.; Khadilkar, A.V.; Chiplonkar, S.A.; Khadilkar, V.V. Determinants of bone mineral content and bone area in Indian preschool children. J. Bone Miner. Metab. 2011, 29, 334–341. [Google Scholar] [CrossRef]
- Fazeli, P.K.; Horowitz, M.C.; MacDougald, O.A.; Scheller, E.L.; Rodeheffer, M.S.; Rosen, C.J.; Klibanski, A. Marrow fat and bone--new perspectives. J. Clin. Endocrinol. Metab. 2013, 98, 935–945. [Google Scholar] [CrossRef]
- Gao, S.; Qian, X.; Huang, S.; Deng, W.; Li, Z.; Hu, Y. Association between macronutrients intake distribution and bone mineral density. Clin. Nutr. 2022, 41, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Felson, D.T.; Zhang, Y.; Hannan, M.T.; Anderson, J.J. Effects of weight and body mass index on bone mineral density in men and women: The Framingham study. J. Bone Miner. Res. 1993, 8, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Beier, E.; Sheu, T.; Zhang, H.; Zuscik, M.J.; Puzas, E.J.; Boyce, B.F.; Mooney, R.A.; Xing, L. High-fat diet causes bone loss in young mice by promoting osteoclastogenesis through alteration of the bone marrow environment. Calcif. Tissue Int. 2015, 96, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Rharass, T.; Lucas, S. Mechanisms In Endocrinology: Bone marrow adiposity and bone, a bad romance? Eur. J. Endocrinol. 2018, 179, R165–R182. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhang, Z.; Pei, L.; Zhang, X.; Li, B.; Meng, Y.; Zhou, X. How high-fat diet affects bone in mice: A systematic review and meta-analysis. Obes. Rev. 2022, 23, e13493. [Google Scholar] [CrossRef]
- Muruganandan, S.; Ionescu, A.M.; Sinal, C.J. At the Crossroads of the Adipocyte and Osteoclast Differentiation Programs: Future Therapeutic Perspectives. Int. J. Mol. Sci. 2020, 21, 2277. [Google Scholar] [CrossRef]
- Chen, X.; Wang, C.; Zhang, K.; Xie, Y.; Ji, X.; Huang, H.; Yu, X. Reduced femoral bone mass in both diet-induced and genetic hyperlipidemia mice. Bone 2016, 93, 104–112. [Google Scholar] [CrossRef]
- Deng, P.; Yuan, Q.; Cheng, Y.; Li, J.; Liu, Z.; Liu, Y.; Li, Y.; Su, T.; Wang, J.; Salvo, M.E.; et al. Loss of KDM4B exacerbates bone-fat imbalance and mesenchymal stromal cell exhaustion in skeletal aging. Cell Stem Cell 2021, 28, 1057–1073. [Google Scholar] [CrossRef] [PubMed]
- Fabiani, R.; Naldini, G.; Chiavarini, M. Dietary Patterns in Relation to Low Bone Mineral Density and Fracture Risk: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 219–236. [Google Scholar] [CrossRef] [PubMed]
- Orozco, P. Atherogenic lipid profile and elevated lipoprotein (a) are associated with lower bone mineral density in early postmenopausal overweight women. Eur. J. Epidemiol. 2004, 19, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Fu, F. Convolutional neural network model by deep learning and teaching robot in keyboard musical instrument teaching. PLoS ONE 2023, 18, e0293411. [Google Scholar] [CrossRef]
- Han, H.; Chen, S.; Wang, X.; Jin, J.; Li, X.; Li, Z. Association between muscle strength and mass and bone mineral density in the US general population: Data from NHANES 1999–2002. J. Orthop. Surg. Res. 2023, 18, 397. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Number of Subjects (n = 5603) | Statistic | p Value | |
|---|---|---|---|---|
| ≤20 | >20 | |||
| Gender | 2.565 | 0.109 | ||
| Male | 1100 | 1905 | ||
| Female | 1005 | 1593 | ||
| Country of Birth | 175.729 | <0.001 | ||
| Mexican Americans | 1856 | 2577 | ||
| Other Hispanic | 175 | 739 | ||
| Non-Hispanic white | 74 | 182 | ||
| Citizenship | 22.335 | <0.001 | ||
| Born or naturalized citizens | 1897 | 3006 | ||
| Non-US citizens | 208 | 487 | ||
| Others | 0 | 5 | ||
| Marital status | 2640.290 | <0.001 | ||
| Married | 11 | 2050 | ||
| Widowhood | 1 | 217 | ||
| Divorce | 0 | 430 | ||
| Separation | 8 | 108 | ||
| Never married | 1087 | 458 | ||
| Living with a partner | 33 | 234 | ||
| other | 965 | 1 | ||
| Total number of households | 1007.355 | <0.001 | ||
| 1 | 21 | 509 | ||
| 2 | 150 | 1028 | ||
| 3 | 348 | 708 | ||
| 4 | 572 | 562 | ||
| 5 | 505 | 377 | ||
| 6 | 265 | 160 | ||
| >6 | 244 | 154 | ||
| Annual household income | 383.878 | <0.001 | ||
| less than USD 20,000 | 449 | 629 | ||
| USD 20,000 to 44,999 | 636 | 1059 | ||
| USD 45,000 to 74,999 | 474 | 756 | ||
| More than USD 75,000 | 526 | 527 | ||
| others | 20 | 527 | ||
| Total femoral density(g/cm2) | 0.91 ± 0.18 | 0.96 ± 0.15 | 94.554 | <0.001 |
| Characteristics | Total Number of Subjects (n = 5603) | Statistic | p Value | |
|---|---|---|---|---|
| ≤20 | >20 | |||
| Energy (kcal) | 2262.71 ± 1082.29 | 2221.44 ± 1055.19 | −1.286 | 0.198 |
| Protein (g) | 79.16 ± 44.09 | 84.90 ± 47.08 | −4.843 | <0.01 |
| Carbohydrates (g) | 296.38 ± 147.61 | 266.60 ± 131.92 | −7.885 | <0.01 |
| Total fat (g) | 85.52 ± 46.55 | 83.56 ± 48.21 | −2.336 | 0.019 |
| Fat energy supply | 769.66 ± 418.91 | 752.04 ± 433.92 | −2.336 | 0.019 |
| The proportion of fat energy supply | 0.34 ± 0.08 | 0.33 ± 0.09 | −1.53 | <0.01 |
| Cholesterol (mg) | 256.61 ± 212.22 | 307.22 ± 251.91 | −7.341 | <0.01 |
| Vitamin E | 6.43 ± 4.80 | 7.95 ± 5.86 | −11.018 | <0.01 |
| Total folic acid (μg) | 398.83 ± 300.08 | 409.99 ± 248.63 | −4.312 | <0.01 |
| Vitamin B12 (μg) | 5.38 ± 5.01 | 5.50 ± 8.62 | −3.571 | <0.01 |
| Vitamin C (mg) | 93.72 ± 107.25 | 87.86 ± 102.63 | −1.108 | 0.268 |
| Vitamin K (μg) | 63.04 ± 80.98 | 106.32 ± 152.39 | −16.597 | <0.01 |
| Calcium (mg) | 984.85 ± 639.68 | 924.24 ± 594.45 | −3.308 | <0.01 |
| Phosphorus (mg) | 1303.05 ± 695.55 | 1376.44 ± 705.68 | −4.446 | <0.01 |
| Magnesium (mg) | 245.21 ± 130.73 | 307.18 ± 157.02 | −17.139 | <0.01 |
| Iron (mg) | 16.21 ± 9.85 | 15.63 ± 9.15 | −1.681 | 0.093 |
| Zinc (mg) | 11.88 ± 7.71 | 12.26 ± 12.86 | −0.408 | 0.683 |
| Selenium (μg) | 105.01 ± 60.74 | 116.62 ± 72.25 | −6.146 | <0.01 |
| Caffeine (mg) | 39.99 ± 72.38 | 176.02 ± 221.89 | −33.095 | <0.01 |
| Vitamin B2 (mg) | 2.15 ± 1.31 | 2.23 ± 1.33 | −2.425 | 0.015 |
| Vitamin B1(mg) | 1.69 ± 1.01 | 1.67 ± 1.01 | −0.758 | 0.448 |
| Niacin (mg) | 24.34 ± 15.14 | 26.11 ± 15.96 | −4.999 | 0.957 |
| Vitamin B6 (mg) | 1.86 ± 1.28 | 2.10 ± 1.40 | −7.146 | <0.01 |
| Age | Pearson’s Correlation | p Value |
|---|---|---|
| ≤20 years | 0.658 | <0.001 |
| >20 years | -0.307 | <0.001 |
| Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| b | p Value | OR | b | p Value | OR | b | p Value | OR | |
| ≤20 years | |||||||||
| Vitamin B2 | 0.021 | 0.65 | 1.021 | −0.098 | 0.163 | 0.906 | −0.349 | 0.075 | 0.705 |
| Vitamin B6 | 0.064 | 0.15 | 1.066 | 0.001 | 0.996 | 1.001 | −0.466 | 0.034 | 0.627 |
| Niacin | 0.006 | 0.093 | 1.006 | 0.012 | 0.181 | 1.012 | 0.061 | 0.004 | 1.062 |
| Vitamin B12 | 0.008 | 0.495 | 1.008 | 0 | 0.995 | 1 | 0 | 0.983 | 1 |
| Carbohydrates stage | |||||||||
| Appropriate | 0.251 | 0.422 | 0.818 | ||||||
| Low | −0.186 | 0.152 | 0.83 | 0.233 | 0.346 | 1.263 | 0.074 | 0.772 | 1.077 |
| High | −0.304 | 0.201 | 0.738 | 0.077 | 0.761 | 1.08 | −0.219 | 0.578 | 0.803 |
| Protein stage | |||||||||
| Appropriate | 0.188 | 0.221 | 0.082 | ||||||
| Low | −0.289 | 0.125 | 0.749 | 0.193 | 0.174 | 1.212 | −0.567 | 0.079 | 0.567 |
| High | −0.183 | 0.169 | 0.833 | −0.068 | 0.764 | 0.935 | −0.32 | 0.251 | 0.726 |
| HFD stage | |||||||||
| Appropriate | |||||||||
| High | 1.429 | 0.049 | 4.173 | 1.388 | 0.057 | 4.007 | 1.142 | 0.286 | 3.133 |
| >20 years | |||||||||
| Vitamin B2 | 0.024 | 0.478 | 1.025 | 0.142 | 0.007 | 1.153 | 0.253 | 0.002 | 1.288 |
| Vitamin B6 | −0.058 | 0.104 | 0.943 | −0.172 | 0.022 | 0.842 | −0.125 | 0.168 | 0.883 |
| Niacin | −0.003 | 0.288 | 0.997 | 0.004 | 0.584 | 1.004 | 0.003 | 0.765 | 1.003 |
| Vitamin B12 | −0.003 | 0.653 | 0.997 | −0.003 | 0.689 | 0.997 | −0.005 | 0.696 | 0.995 |
| Carbohydrates stage | |||||||||
| Appropriate | 0.031 | 0.057 | 0.068 | ||||||
| Low | −0.123 | 0.283 | 0.884 | −0.117 | 0.327 | 0.889 | −0.166 | 0.258 | 0.847 |
| High | 0.292 | 0.109 | 1.339 | 0.291 | 0.117 | 1.338 | 0.333 | 0.089 | 1.396 |
| Protein stage | |||||||||
| Appropriate | 0.077 | 0.356 | 0.529 | ||||||
| Low | 0.266 | 0.085 | 1.304 | 0.214 | 0.177 | 1.239 | 0.183 | 0.303 | 1.2 |
| High | −0.08 | 0.425 | 0.923 | −0.01 | 0.924 | 0.99 | −0.068 | 0.622 | 0.934 |
| HFD stage | |||||||||
| Appropriate | 1 | ||||||||
| High | −0.035 | 0.897 | 0.966 | −0.051 | 0.852 | 0.95 | −0.047 | 0.878 | 1.048 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, J.; Zhang, Y.; Yuan, Y.; Li, M.; Zhai, B.; Chen, J. Opposing Effects of Nutritional Supply on Bone Health at Different Ages: Based on the National Health and Nutrition Examination Survey Database. Nutrients 2024, 16, 758. https://doi.org/10.3390/nu16060758
Wei J, Zhang Y, Yuan Y, Li M, Zhai B, Chen J. Opposing Effects of Nutritional Supply on Bone Health at Different Ages: Based on the National Health and Nutrition Examination Survey Database. Nutrients. 2024; 16(6):758. https://doi.org/10.3390/nu16060758
Chicago/Turabian StyleWei, Jieqiong, Yaxi Zhang, Yuehan Yuan, Min Li, Bingfang Zhai, and Jihua Chen. 2024. "Opposing Effects of Nutritional Supply on Bone Health at Different Ages: Based on the National Health and Nutrition Examination Survey Database" Nutrients 16, no. 6: 758. https://doi.org/10.3390/nu16060758
APA StyleWei, J., Zhang, Y., Yuan, Y., Li, M., Zhai, B., & Chen, J. (2024). Opposing Effects of Nutritional Supply on Bone Health at Different Ages: Based on the National Health and Nutrition Examination Survey Database. Nutrients, 16(6), 758. https://doi.org/10.3390/nu16060758