
The Association of Vitamin D Receptor Polymorphisms with COVID-19 Severity
 , , , ,
, , , ,  , and
, and
Abstract
1. Introduction
2. Patients and Methods
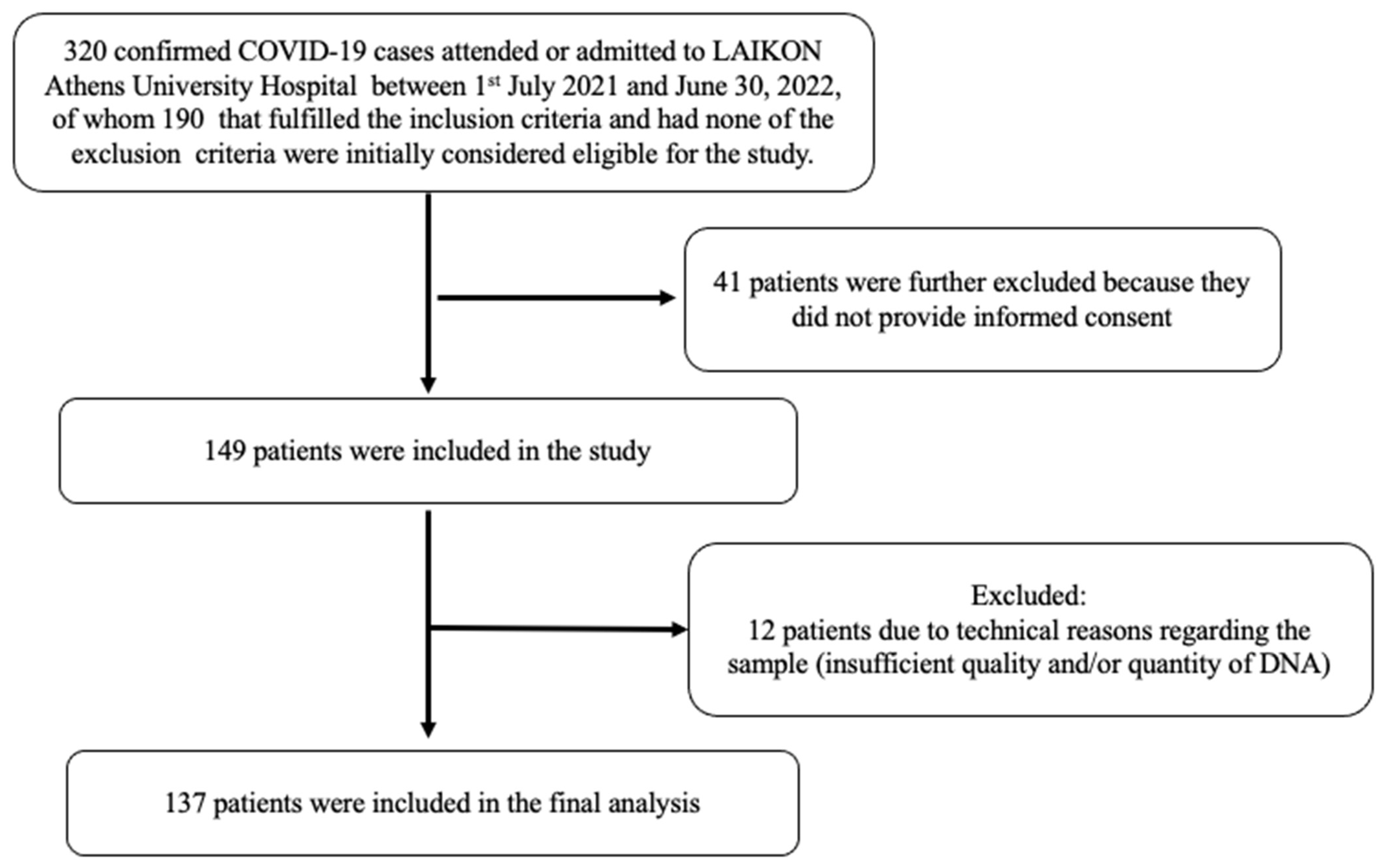
2.1. Participants
2.2. Sampling Procedure and Measurements
2.2.1. Biochemical Analyses
2.2.2. Genetic Analysis
2.3. Statistics
3. Results
Genetic Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsitsilonis, O.E.; Paraskevis, D.; Lianidou, E.; Terpos, E.; Akalestos, A.; Pierros, V.; Kostaki, E.G.; Kastritis, E.; Moutsatsou, P.; Politou, M.; et al. SARS-CoV-2 Infection Is Asymptomatic in Nearly Half of Adults with Robust Anti-Spike Protein Receptor-Binding Domain Antibody Response. Vaccines 2021, 9, 207. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Bassatne, A.; Basbous, M.; Chakhtoura, M.; El Zein, O.; Rahme, M.; El-Hajj Fuleihan, G. The link between COVID-19 and VItamin D (VIVID): A systematic review and meta-analysis. Metabolism 2021, 119, 154753. [Google Scholar] [CrossRef]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.C.; Silva, C.B.R.; Franco, A.S.; Macedo, M.B.; Dalmolin, H.H.H.; et al. Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients with Moderate to Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Alcala Diaz, J.F.; Lopez Miranda, J.; Bouillon, R.; Quesada Gomez, J.M. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef] [PubMed]
- Butler-Laporte, G.; Nakanishi, T.; Mooser, V.; Morrison, D.R.; Abdullah, T.; Adeleye, O.; Mamlouk, N.; Kimchi, N.; Afrasiabi, Z.; Rezk, N.; et al. Vitamin D and COVID-19 susceptibility and severity in the COVID-19 Host Genetics Initiative: A Mendelian randomization study. PLoS Med. 2021, 18, e1003605. [Google Scholar] [CrossRef]
- Amin, H.A.; Drenos, F. No evidence that vitamin D is able to prevent or affect the severity of COVID-19 in individuals with European ancestry: A Mendelian randomisation study of open data. BMJ Nutr. Prev. Health 2021, 4, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.J.; Baker, I.; Davey Smith, G. Meta-analysis of vitamin D receptor polymorphisms and pulmonary tuberculosis risk. Int. J. Tuberc. Lung Dis. 2005, 9, 1174–1177. [Google Scholar] [PubMed]
- Lee, Y.H.; Song, G.G. Vitamin D receptor gene FokI, TaqI, BsmI, and ApaI polymorphisms and susceptibility to pulmonary tuberculosis: A meta-analysis. Genet. Mol. Res. 2015, 14, 9118–9129. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.J.; Llewelyn, M.; Toossi, Z.; Patel, P.; Pasvol, G.; Lalvani, A.; Wright, D.; Latif, M.; Davidson, R.N. Influence of vitamin D deficiency and vitamin D receptor polymorphisms on tuberculosis among Gujarati Asians in west London: A case-control study. Lancet 2000, 355, 618–621. [Google Scholar] [CrossRef] [PubMed]
- McNally, J.D.; Sampson, M.; Matheson, L.A.; Hutton, B.; Little, J. Vitamin D receptor (VDR) polymorphisms and severe RSV bronchiolitis: A systematic review and meta-analysis. Pediatr. Pulmonol. 2014, 49, 790–799. [Google Scholar] [CrossRef]
- Abdollahzadeh, R.; Shushizadeh, M.H.; Barazandehrokh, M.; Choopani, S.; Azarnezhad, A.; Paknahad, S.; Pirhoushiaran, M.; Makani, S.Z.; Yeganeh, R.Z.; Al-Kateb, A.; et al. Association of Vitamin D receptor gene polymorphisms and clinical/severe outcomes of COVID-19 patients. Infect. Genet. Evol. 2021, 96, 105098. [Google Scholar] [CrossRef]
- Freitas, A.T.; Calhau, C.; Antunes, G.; Araujo, B.; Bandeira, M.; Barreira, S.; Bazenga, F.; Braz, S.; Caldeira, D.; Santos, S.C.R.; et al. Vitamin D-related polymorphisms and vitamin D levels as risk biomarkers of COVID-19 disease severity. Sci. Rep. 2021, 11, 20837. [Google Scholar] [CrossRef] [PubMed]
- Peralta, E.M.; Rosales, Y.Z.; Mesa, T.C.; González, E.N.S.; Pérez, Y.H.; de los Ángeles González Torres, M.; Balbuena, H.R.; Teruel, B.M. TaqI polymorphism of the VDR gene: Aspects related to the clinical behavior of COVID-19 in Cuban patients. Egypt. J. Med. Hum. Genet. 2021, 22, 83. [Google Scholar] [CrossRef]
- Apaydin, T.; Polat, H.; Dincer Yazan, C.; Ilgin, C.; Elbasan, O.; Dashdamirova, S.; Bayram, F.; Tukenmez Tigen, E.; Unlu, O.; Tekin, A.F.; et al. Effects of vitamin D receptor gene polymorphisms on the prognosis of COVID-19. Clin. Endocrinol. 2022, 96, 819–830. [Google Scholar] [CrossRef]
- Mamurova, B.; Akan, G.; Mogol, E.; Turgay, A.; Tuncel, G.; Evren, E.U.; Evren, H.; Suer, K.; Sanlidag, T.; Ergoren, M.C. Strong Association between Vitamin D Receptor Gene and Severe Acute Respiratory Syndrome coronavirus 2 Infectious Variants. Glob. Med. Genet. 2023, 10, 27–33. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of COVID-19: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020; pp. 13–15.
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef]
- Zacharioudaki, M.; Messaritakis, I.; Galanakis, E. Vitamin D receptor, vitamin D binding protein and CYP27B1 single nucleotide polymorphisms and susceptibility to viral infections in infants. Sci. Rep. 2021, 11, 13835. [Google Scholar] [CrossRef]
- Veldman, C.M.; Cantorna, M.T.; DeLuca, H.F. Expression of 1,25-dihydroxyvitamin D3 receptor in the immune system. Arch. Biochem. Biophys. 2000, 374, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Mora, J.R.; Iwata, M.; von Andrian, U.H. Vitamin effects on the immune system: Vitamins A and D take centre stage. Nat. Rev. Immunol. 2008, 8, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Laplana, M.; Royo, J.L.; Fibla, J. Vitamin D Receptor polymorphisms and risk of enveloped virus infection: A meta-analysis. Gene 2018, 678, 384–394. [Google Scholar] [CrossRef]
- Bellamy, R.; Hill, A.V. Genetic susceptibility to mycobacteria and other infectious pathogens in humans. Curr. Opin. Immunol. 1998, 10, 483–487. [Google Scholar] [CrossRef]
- Hustmyer, F.G.; DeLuca, H.F.; Peacock, M. ApaI, BsmI, EcoRV and TaqI polymorphisms at the human vitamin D receptor gene locus in Caucasians, blacks and Asians. Hum. Mol. Genet. 1993, 2, 487. [Google Scholar] [CrossRef]
- Roth, D.E.; Jones, A.B.; Prosser, C.; Robinson, J.L.; Vohra, S. Vitamin D receptor polymorphisms and the risk of acute lower respiratory tract infection in early childhood. J. Infect. Dis. 2008, 197, 676–680. [Google Scholar] [CrossRef]
- Cao, Y.; Wang, X.; Cao, Z.; Cheng, X. Association of Vitamin D receptor gene TaqI polymorphisms with tuberculosis susceptibility: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 10187–10203. [Google Scholar]
- Thakkinstian, A.; D’Este, C.; Attia, J. Haplotype analysis of VDR gene polymorphisms: A meta-analysis. Osteoporos. Int. 2004, 15, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Nejentsev, S.; Godfrey, L.; Snook, H.; Rance, H.; Nutland, S.; Walker, N.M.; Lam, A.C.; Guja, C.; Ionescu-Tirgoviste, C.; Undlien, D.E.; et al. Comparative high-resolution analysis of linkage disequilibrium and tag single nucleotide polymorphisms between populations in the vitamin D receptor gene. Hum. Mol. Genet. 2004, 13, 1633–1639. [Google Scholar] [CrossRef] [PubMed]
- Albu-Mohammed, W.H.M.; Anvari, E.; Fateh, A. Evaluating the Role of BglI rs739837 and TaqI rs731236 Polymorphisms in Vitamin D Receptor with SARS-CoV-2 Variants Mortality Rate. Genes 2022, 13, 2346. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameters | Controls (Group 1) n = 72 | Mild COVID-19 (Group 2) n = 51 | Severe COVID-19 (Group 3) n = 86 | p-Value All Groups | p-Value 1 vs. 2 | p-Value 1 vs. 3 | p-Value 2 vs. 3 |
|---|---|---|---|---|---|---|---|
| Gender (males), n (%) | 30 (41.7%) | 25 (49%) | 61 (70.9%) | 0.001 ǂ | 0.419 × | <0.001 × | 0.010 × |
| Age (years) | 56.0 ± 11.4 | 56.51 ± 16.6 | 60.5 ± 12.5 | 0.072 * | - | - | - |
| Weight (kg) | 81.76 ± 19.8 | 78.99 ± 15.2 | 84.33 ± 17.2 | 0.236 * | - | - | - |
| BMI (kg/m2) | 28.9 ± 5.4 | 27.6 ± 4.4 | 28.6 ± 6.4 | 0.429 * | - | - | - |
| Lymphocytes, n | 2200 (1760, 2615) | 1360 (705, 2250) | 900 (645, 1245) | <0.001 ^ | <0.001 † | <0.001 † | 0.003 † |
| WBC, n/μL | 7020 (6205, 8297.5) | 6215 (4650, 9245) | 6270 (4710, 9115) | 0.219 ^ | |||
| Serum 25(OH)D (ng/mL) | 28 (20.0, 33.7) | 25.20 (16.6, 37.0) | 23.05 (13.2, 30.0) | 0.120 ^ | |||
| Vitamin D status | 0.220 ǂ | ||||||
| Deficiency, n (%) | 1 (1.4) | 2 (4.0) | 5 (5.8) | ||||
| Inadequacy, n (%) | 12 (16.7) | 4 (7.8) | 17 (19.8) | ||||
| Sufficiency, n (%) | 59 (81.9) | 45 (88.2) | 64 (74.4) | ||||
| Hb (g/dL) | 13.7 ± 1.5 | 12.9 ± 2.1 | 13.3 ± 3.9 | 0.286 * | |||
| Serum Creatinine (mg/dL) | 0.84 ± 0.36 | 0.87 ± 0.4 | 1.5 ± 3.9 | 0.125 * | |||
| LDH (U/L) | 180.5 (153.8, 205.8) | 215 (179.8, 297.0) | 312.5 (222.8, 415.3) | <0.001 ^ | <0.001 † | <0.001 † | <0.001 † |
| Serum CRP (mg/L) | 2 (0.85, 4.6) | 9.2 (3, 45.4) | 43 (12.1, 91) | <0.001 ^ | <0.001 † | <0.001 † | <0.001 † |
| Ferritin (ng/mL) | 66.5 (35.0, 97.0) | 211.0 (54.3, 443.5) | 528.5 (260.3, 1110.3) | <0.001 ^ | <0.001 † | <0.001 † | <0.001 † |
| D-dimers (μg/mL) | 0.5 (0.3-0.6) | 0.6 (0.3, 1.4) | 0.9 (0.5, 3.7) | <0.001 | 0.065 † | <0.001 † | 0.020 † |
| HbA1c (%) | 6.3 (5.0, 12.7) | 6.1 (5.1, 7.9) | 7.6 (5.5, 12.7) | 0.012 ^ | 0.327 † | 0.005 † | 0.023 † |
| DM, n (%) | 22 (30.6) | 9 (17.6) | 18 (20.9) | 0.193 ǂ | - | - | |
| COPD, n (%) | 0 (0) | 2 (3.9) | 2 (2.3) | 0.273 ǂ | - | - | |
| Stroke n (%) | 0 (0) | 3 (5.9) | 4 (4.7) | 0.141 ǂ | |||
| CAD, n (%) | 8 (11.1) | 4 (7.8) | 5 (5.8) | 0.477 ǂ | |||
| Hypertension, n (%) | 22 (30.6) | 14 (27.5) | 30 (34.9) | 0.647 ǂ | |||
| Current smokers, n (%) | 13 (18.1) | 10 (19.6) | 8 (9.3) | 0.166 ǂ | |||
| SNP Genotypes | Controls/Mild Symptoms | Severe Symptoms | Analysis Model | OR (95%CI) | p-Value | HWE in Control Group (p-Value) |
|---|---|---|---|---|---|---|
| TT | 43 | 35 | Additive (TT vs. TC vs. CC) | 0.009 | 0.35 | |
| TC | 66 | 30 | ||||
| CC | 14 | 21 | ||||
| TT | 43 | 35 | Homozygous (CC vs. TT) | 1.84 (0.82–4.14) | 0.14 | |
| CC | 14 | 21 | ||||
| TT | 43 | 35 | Heterozygous (TC vs. TT) | 0.56 (0.3–1.04) | 0.07 | |
| TC | 66 | 30 | ||||
| TT | 43 | 35 | Dominant (TC + CC vs. TT) | 0.78 (0.44–1.38) | 0.4 | |
| TC + CC | 80 | 51 | ||||
| TC + TT | 109 | 65 | Recessive (CC vs. TC + TT) | 2.52 (1.2–5.29) | 0.01 | |
| CC | 14 | 21 | ||||
| T | 152 | 100 | Allelic (C vs. T) | 0.86 (0.58–1.28) | 0.45 | |
| C | 94 | 72 |
| Parameters | Univariable Analysis | Multivariable Analysis * | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| TaqI Recessive (CC vs. TC/TT) | 2.52 (1.2–5.29) | 0.01 | 3.234 (1.179–8.869) | 0.023 |
| Age (years) | 1.025 (1.003–1.047) | 0.024 | 1.028 (1.002–1.055) | 0.038 |
| Gender (female vs. male) | 0.331 (0.185–0.595) | <0.001 | 0.257 (0.123–0.537) | |
| Serum CRP levels (mg/dL) | 1.024 (1.014–1.34) | <0.001 | 1.021 (1.011–1.031) | <0.001 |
| Lymphocytes (k/μL) | 0.998 (0.998–0.999) | <0.001 | 0.998 (0.998–0.999) | <0.001 |
| LDH (U/L) | 1.012 (1.008–1.016) | <0.001 | 1.008 (1.003–1.013) | 0.001 |
| Ferritin (ng/mL) | 1.003 (1.002–1.005) | <0.001 | 1.003 (1.002–1.004) | <0.001 |
| D-dimers (μg/mL) | 1.004 (1.000–1.009) | 0.035 | 1.003 (0.999–1.007) | 0.087 |
| Serum 25(OH)D levels (ng/mL) | 0.970 (0.939–1.002) | 0.063 | - | |
| DM (yes vs. no) | 0.895 (0.643–1.248) | 0.514 | - | |
| CAD (yes vs. no) | 0.853 (0.355–2.049) | 0.722 | - | |
| COPD (yes vs. no) | 1.417 (0.196–10.258) | 0.730 | - | |
| Smoking (yes vs. no) | 0.534 (0.223–1.278) | 0.159 | - | |
| BMI (kg/m2) | 1.009 (0.960–1.060) | 0.725 | - | |
| Interaction between TaqI additive (TT vs. TC vs. CC) model and serum vitamin D levels | 0.967 (0.879–1.064) | 0.487 | - | |
| Interaction between TaqI recessive (CC vs TC/TT) model and serum vitamin D levels | 0.881 (0.739–1.049) | 0.154 | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tentolouris, N.; Achilla, C.; Anastasiou, I.A.; Eleftheriadou, I.; Tentolouris, A.; Basoulis, D.; Kosta, O.; Lambropoulos, A.; Yavropoulou, M.P.; Chatzikyriakidou, A.; et al. The Association of Vitamin D Receptor Polymorphisms with COVID-19 Severity. Nutrients 2024, 16, 727. https://doi.org/10.3390/nu16050727
Tentolouris N, Achilla C, Anastasiou IA, Eleftheriadou I, Tentolouris A, Basoulis D, Kosta O, Lambropoulos A, Yavropoulou MP, Chatzikyriakidou A, et al. The Association of Vitamin D Receptor Polymorphisms with COVID-19 Severity. Nutrients. 2024; 16(5):727. https://doi.org/10.3390/nu16050727
Chicago/Turabian StyleTentolouris, Nikolaos, Charoula Achilla, Ioanna A. Anastasiou, Ioanna Eleftheriadou, Anastasios Tentolouris, Dimitrios Basoulis, Ourania Kosta, Alexandros Lambropoulos, Maria P. Yavropoulou, Anthoula Chatzikyriakidou, and et al. 2024. "The Association of Vitamin D Receptor Polymorphisms with COVID-19 Severity" Nutrients 16, no. 5: 727. https://doi.org/10.3390/nu16050727
APA StyleTentolouris, N., Achilla, C., Anastasiou, I. A., Eleftheriadou, I., Tentolouris, A., Basoulis, D., Kosta, O., Lambropoulos, A., Yavropoulou, M. P., Chatzikyriakidou, A., & Jude, E. B. (2024). The Association of Vitamin D Receptor Polymorphisms with COVID-19 Severity. Nutrients, 16(5), 727. https://doi.org/10.3390/nu16050727