
Vitamin D Supplementation and Recurrence of Benign Paroxysmal Positional Vertigo


Abstract
1. Introduction
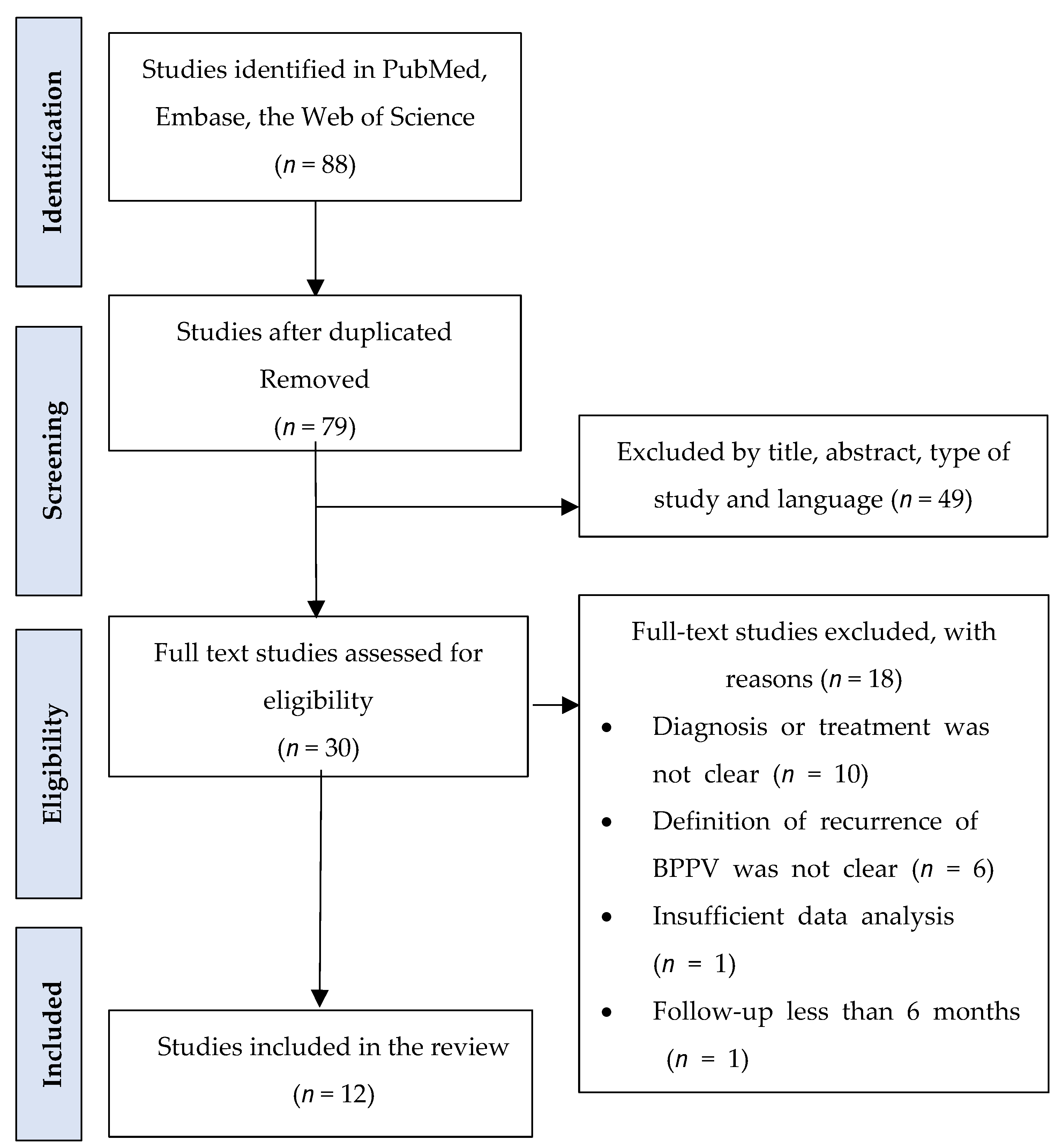
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Baloh, R.W.; Honrubia, V.; Jacobson, K. Benign positional vertigo: Clinical and oculographic features in 240 cases. Neurology 1987, 37, 371–378. [Google Scholar] [CrossRef]
- Neuhauser, H.K. Epidemiology of vertigo. Curr. Opin. Neurol. 2007, 20, 40–46. [Google Scholar] [CrossRef]
- Neuhauser, H.K.; von Brevern, M.; Radtke, A. Epidemiology of vestibular vertigo: A neurotologic survey of the general population. Neurology 2005, 65, 898–904. [Google Scholar] [CrossRef]
- von Brevern, M.; Radtke, A.; Lezius, F. Epidemiology of benign paroxysmal positional vertigo: A population based study. J. Neurol. Neurosurg. Psychiatry 2007, 78, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Sfakianaki, I.; Binos, P.; Karkos, P. Risk factors for recurrence of benign paroxysmal positional vertigo. a clinical review. J. Clin. Med. 2021, 10, 4372. [Google Scholar] [CrossRef]
- Li, J.C.; Li, C.J.; Epley, J. Cost-effective management of benign positional vertigo using canalith repositioning. Otolaryngol. Head Neck Surg. 2000, 122, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Benecke, H.; Agus, S.; Kuessner, D. The burden and impact of vertigo: Findings from the REVERT patient registry. Front. Neurol. 2013, 4, 136. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, N.; Gubbels, S.P.; Schwartz, S.R. Clinical practice guideline: Benign paroxysmal positional vertigo (Update). Otolaryngol. Head Neck Surg. 2017, 156, S1–S47. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.H.; Kim, J.S.; Shin, J.W. Decreased serum vitamin D in idiopathic benign paroxysmal positional vertigo. J. Neurol. 2013, 260, 832–838. [Google Scholar] [CrossRef]
- Bűki, B.; Ecker, M.; Jűnger, H. Vitamin D deficiency and benign paroxysmal positioning vertigo. Med. Hypotheses 2013, 80, 201–204. [Google Scholar] [CrossRef]
- Talaat, H.S.; Abuhadied, G.; Talaat, A.S. Low bone mineral density and vitamin D deficiency in patients with benign positional paroxysmal vertigo. Eur. Arch. Otorhinolaryngol. 2015, 272, 2249–2253. [Google Scholar] [CrossRef]
- Rhim, G.I. Serum vitamin D and recurrent benign paroxysmal positional vertigo. Laryngoscope Investig. Otolaryngol. 2016, 1, 150–153. [Google Scholar] [CrossRef]
- Yang, Z.; Li, J.; Zhu, Z. Effect of vitamin D supplementation on benign paroxysmal positional vertigo recurrence: A meta-analysis. Sci. Prog. 2021, 104, 1–14. [Google Scholar] [CrossRef]
- Jeong, S.H.; Lee, S.U.; Kim, J.S. Prevention of recurrent benign paroxysmal positional vertigo with vitamin D supplementation: A meta-analysis. J. Neurol. 2022, 269, 619–626. [Google Scholar] [CrossRef]
- Hong, X.; Christ-Franco, M.; Moher, D. Vitamin D supplementation for benign paroxysmal positional vertigo: A systematic review. Otol. Neurotol. 2022, 43, e704–e711. [Google Scholar] [CrossRef]
- Talaat, H.S.; Kabel, A.-M.H.; Khaliel, L.H. Reduction of recurrence rate of benign paroxysmal positional vertigo by treatment of severe vitamin D deficiency. Auris Nasus Larynx 2016, 43, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Sheikhzadeh, M.; Lotfi, Y.; Mousavi, A. The effect of serum vitamin D normalization in preventing recurrences of benign paroxysmal positional vertigo: A case-control study. Casp. J. Intern. Med. 2016, 7, 173–177. [Google Scholar]
- Califano, L.; Salafa, F.; Melillo, M.G. Is hypovitaminosis D a risk factor for either the onset or the recurrence of benign paroxysmal positional vertigo? Front. ORL 2019, 10, 27–37. [Google Scholar]
- Pecci, R.; Mandalà, M.; Marcari, A. Vitamin D insufficiency/deficiency in patients with recurrent benign paroxysmal positional vertigo. J. Int. Adv. Otol. 2022, 18, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, J.M.; Leonardo, J.C.H.; Niembro, J.K.I. Therapeutic effect of the correction of vitamin D deficiency in patients with benign paroxysmal positional vertigo. a randomized clinical trial. Int. Arch. Otorhinolaryngol. 2022, 26, e666–e670. [Google Scholar]
- Libonati, G.A.; Leone, A.; Martellucci, S. Prevention of recurrent benign paroxysmal positional vertigo: The role of combined supplementation with vitamin D and antioxidants. Audiol. Res. 2022, 12, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Bazoni, J.A.; Ciquinato, D.S.; Marquez, A.d.S. Hypovitaminosis D, low bone mineral density, and diabetes mellitus as probable risk factors for benign paroxysmal positional vertigo in the elderly. Int. Arch. Otorhinolaryngol. 2020, 24, e272–e277. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.J.; Goutham, M.K.; Bhat, V.S. Association of serum calcium and vitamin D with benign paroxysmal positional vertigo. Int. Arch. Otorhinolaryngol. 2022, 26, e365–e369. [Google Scholar] [CrossRef] [PubMed]
- Resuli, A.S.; Bedir, A.; Özgür, A. The relationship between benign paroxysmal positional vertigo and vitamin D. Cureus 2022, 14, e26068. [Google Scholar]
- Cobb, L.H.; Bailey, V.O.; Liu, Y.F. Relationship of vitamin D levels with clinical presentation and recurrence of BPPV in a Southeastern United States institution. Auris Nasus Larynx 2023, 50, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.Y.; Wang, Y.J.; Li, J.L. Low vitamin D and uric acid status in patients with benign paroxysmal positional vertigo. Sci. Prog. 2023, 106, 1–9. [Google Scholar] [CrossRef]
- Sarsitthithum, K.; Wisupagan, T.; Kiatthanabumrung, S. The association between serum vitamin D levels and benign paroxysmal positional vertigo. Ear Nose Throat J. 2023, 102, 473–477. [Google Scholar] [CrossRef]
- Shin, H.I.; Park, Y.; Lee, H.J. Correlation between serum vitamin D level and benign paroxysmal positional vertigo recurrence. Auris Nasus Larynx 2023, 50, 700–707. [Google Scholar] [CrossRef]
- Jeong, S.H.; Kim, J.S.; Kim, H.J. Prevention of benign paroxysmal positional vertigo with vitamin D supplementation. Neurology 2020, 95, e1117–e1125. [Google Scholar] [CrossRef]
- Rhim, G.I. Effect of vitamin D injection in recurrent benign paroxysmal positional vertigo with vitamin D deficiency. Int. Arch. Otorhinolaryngol. 2020, 24, e423–e428. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Valcour, A.; Blocki, F.; Hawkins, D.M. Effects of age and serum 25-OH-vitamin D on serum parathyroid hormone levels. J. Clin. Endocrinol. Metab. 2012, 97, 3989–3995. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R. Comparative analysis of nutritional guidelines for vitamin D. Nat. Rev. Endocrinol. 2017, 13, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Cui, A.; Zhang, T.; Xiao, P. Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: A pooled analysis of 7.9 million participants. Front. Nutr. 2023, 10, 1070808. [Google Scholar] [CrossRef]
- Hilger, J.; Friedel, A.; Herr, R. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [CrossRef]
- AlGarni, M.A.; Mirza, A.A.; Althobaiti, A.A. Association of benign paroxysmal positional vertigo with vitamin D deficiency: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2018, 275, 2705–2711. [Google Scholar] [CrossRef]
- Yang, B.; Lu, Y.; Xing, D. Association between serum vitamin D levels and benign paroxysmal positional vertigo: A systematic review and meta-analysis of observational studies. Eur. Arch. Otorhinolaryngol. 2020, 277, 169–177. [Google Scholar] [CrossRef]
- Goldschagg, N.; Teupser, D.; Feil, K. No evidence for a specific vitamin D deficit in benign paroxysmal positional vertigo. Eur. J. Neurol. 2021, 28, 3182–3186. [Google Scholar] [CrossRef]
- Büki, B.; Jünger, H.; Zhang, Y. The price of immune responses and the role of vitamin D in the inner ear. Otol. Neurotol. 2019, 40, 701–709. [Google Scholar] [CrossRef]
- Nakada, T.; Sugiura, S.; Uchida, Y. Difference in serum levels of vitamin D between canalolithiasis and cupulolithiasis of the horizontal semicircular canal in benign paroxysmal positional vertigo. Front. Neurol. 2019, 10, 176. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.; Cade, J.; Dawson, J. Empirically derived dietary patterns in UK adults are associated with sociodemographic characteristics, lifestyle, and diet quality. Nutrients 2018, 10, 177. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | Country | Age (Year) | Case/ Control | Vit. D in Case a | Vit. D in Control a | Vit. D in Non-Re Current a | Vit. D in Recurrent a | p-Value |
|---|---|---|---|---|---|---|---|---|
| Bazoni (2020) [22] | Brazil | 68.7 | 17/92 | 27.8 | 23.8 | NA | NA | 0.260 |
| Thomas (2021) [23] | India | 44.4 | 49/49 | 21.3 | 17.6 | NA | NA | 0.243 |
| Resuli (2022) [24] | Turkey | 44 | 258/100 | 18.8 | 30.7 | NA | NA | 0.000 |
| Pecci (2022) [19] | Italy | 62 | 26/24 | 20.2 | 23.7 | NA | NA | 0.160 |
| Cobb (2023) [25] | USA | 66.2 | 173/5962 | 31.4 | 26.0 | 37.6 | 29.0 | 0.012 b |
| Ren (2023) [26] | China | 60 | 182/182 | 17.1 | 19.2 | NA | NA | 0.328 |
| Sarsitthithum (2023) [27] | Thailand | 60.5 | 69/68 | 21.5 | 26.3 | 21.0 | 21.9 | 0.313 b |
| Shin (2023) [28] | Korea | 48 | 332/NA | 14.7 | NA | 12.9 | 19.2 | 0.001 b |
| Author (Year) | Population | Intervention | Case/ Control | Follow Up (Months) | Vitamin D before Treatment a | Vitamin D after Treatment a | Outcomes |
|---|---|---|---|---|---|---|---|
| Rhim (2020) [30] | BPPV with vitamin D lower than 10 ng/mL | 3 to 4 injections totaling 200,000 IU of vitamin D3 within the first year | 24/50 | 24 | 6.06 | 31.1 | No significant differences |
| Jeong (2020) [29] | BPPV with vitamin D lower than 20 ng/mL | vitamin D 400 IU and 500 mg of calcium carbonate twice a day for 1 year | 448/512 | 12 | 13.3 | 24.2 | Proportion of patients with recurrence was lower in the intervention than in the observation group (37.8 vs. 46.7%, p = 0.005) |
| Sánchez (2022) [20] | BPPV with vitamin D lower than 30 ng/mL | oral cholecalciferol 16,000 UI once a week during 8–10 weeks | 35 | 6–13 | 18.5 | 26.2 | Intervention group had a decreased recurrence of vertigo (p = 0.017) |
| Pecci (2022) [19] | BPPV with vitamin D lower than 30 ng/mL | oral cholecalciferol 25,000–50,000 IU once a week for 4 weeks, then 7000 IU once a week for 2 months | 26/24 | 4–8 | 20.18 | 28.1 | 5/16 patients (31.25%) had only 1 recurrence (average number of relapses/patient: 0.31, p = 0.0003) |
| Libonati (2022) [21] | BPPV with vitamin D lower than 30 ng/mL | vitamin D3 800 IU daily for 6 months | 128 | 6 | 18.2 | 36.9 | A significant reduction in BPPV relapses compared to the baseline was observed (p < 0.0001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rhim, G.; Kim, M.-J. Vitamin D Supplementation and Recurrence of Benign Paroxysmal Positional Vertigo. Nutrients 2024, 16, 689. https://doi.org/10.3390/nu16050689
Rhim G, Kim M-J. Vitamin D Supplementation and Recurrence of Benign Paroxysmal Positional Vertigo. Nutrients. 2024; 16(5):689. https://doi.org/10.3390/nu16050689
Chicago/Turabian StyleRhim, Guil, and Moon-Jung Kim. 2024. "Vitamin D Supplementation and Recurrence of Benign Paroxysmal Positional Vertigo" Nutrients 16, no. 5: 689. https://doi.org/10.3390/nu16050689
APA StyleRhim, G., & Kim, M.-J. (2024). Vitamin D Supplementation and Recurrence of Benign Paroxysmal Positional Vertigo. Nutrients, 16(5), 689. https://doi.org/10.3390/nu16050689