
Association between Controlling Nutritional Status (CONUT) Score and Body Composition, Inflammation and Frailty in Hospitalized Elderly Patients
 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Biochemical Analysis and Data Collection
2.3. Multidimensional Assessment
2.3.1. Nutritional Status and CONUT Score
2.3.2. Cognitive and Functional Status
2.4. Anthropometric and Body Composition Assessment
2.5. Statistical Analysis
3. Results
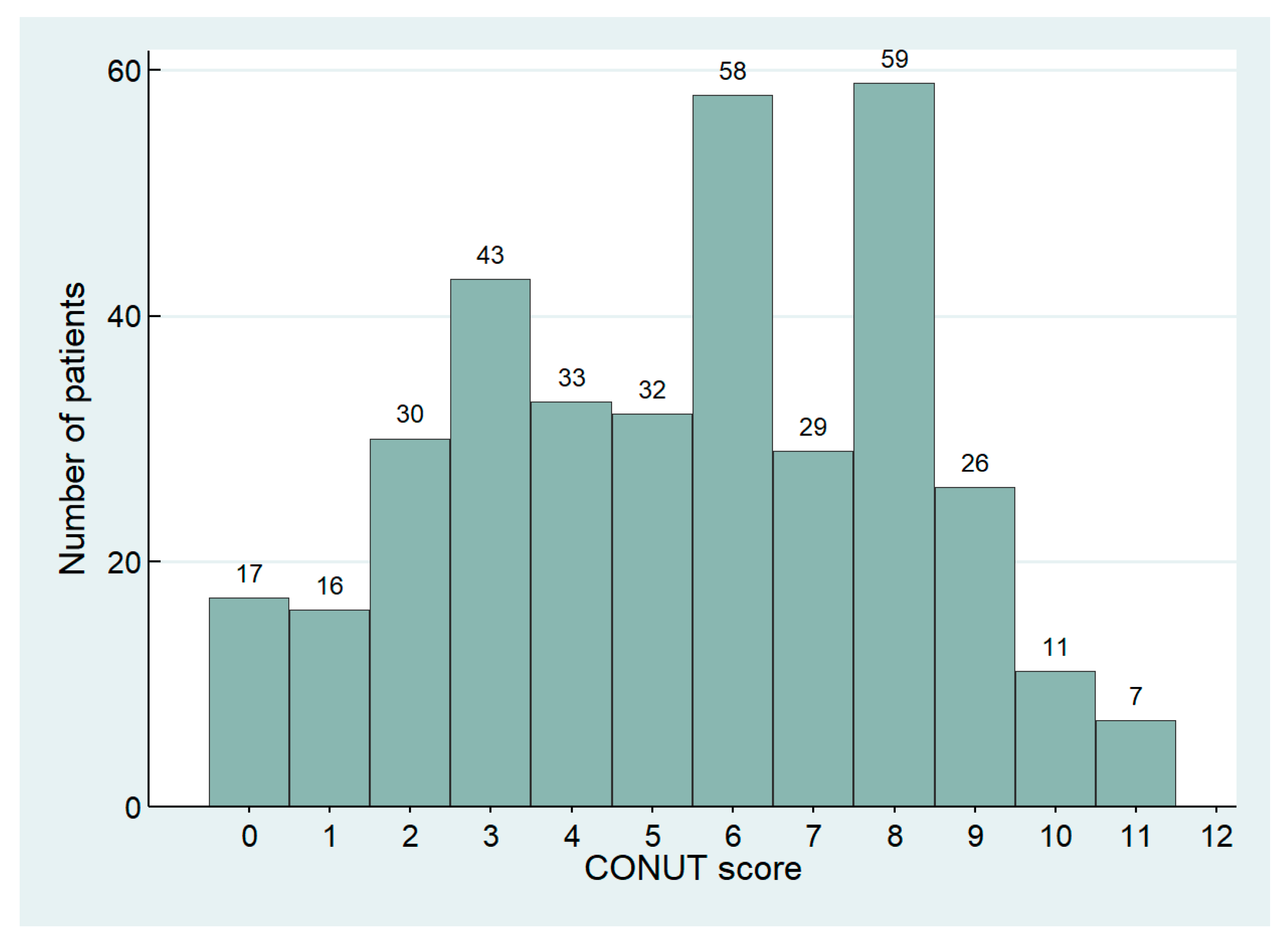
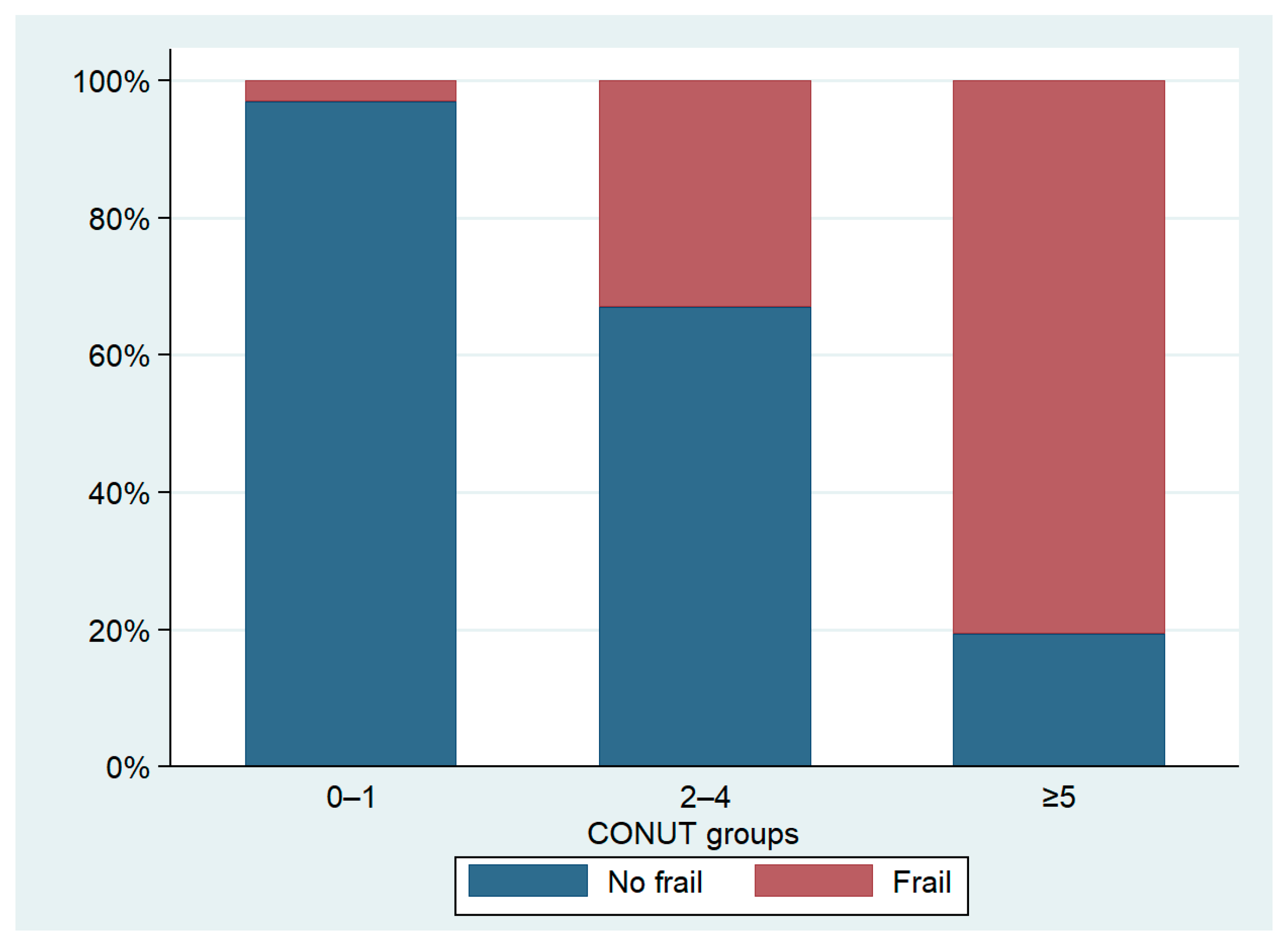
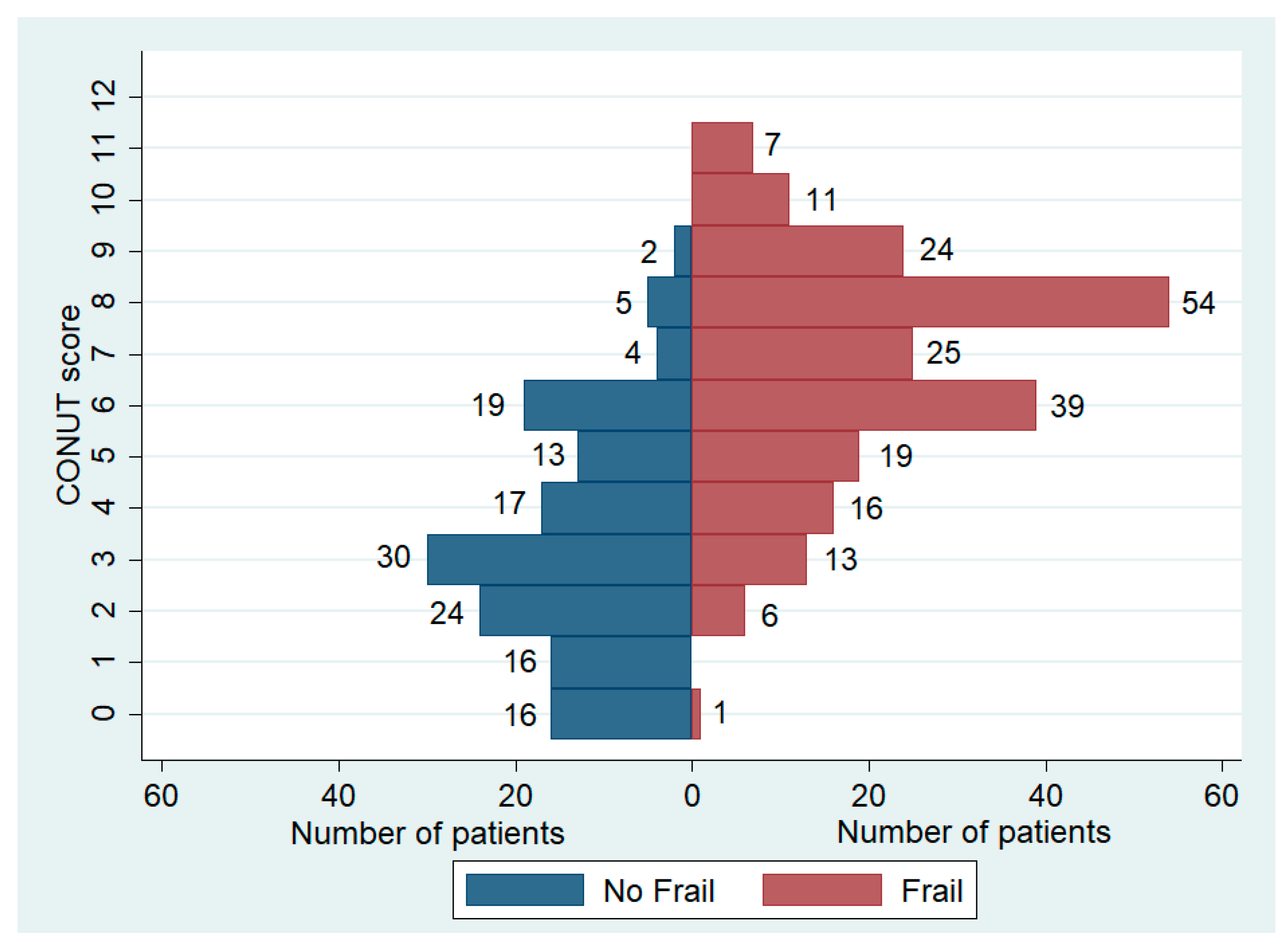
3.1. CONUT Score, Multidimensional Evaluation and Prevalence of Frailty
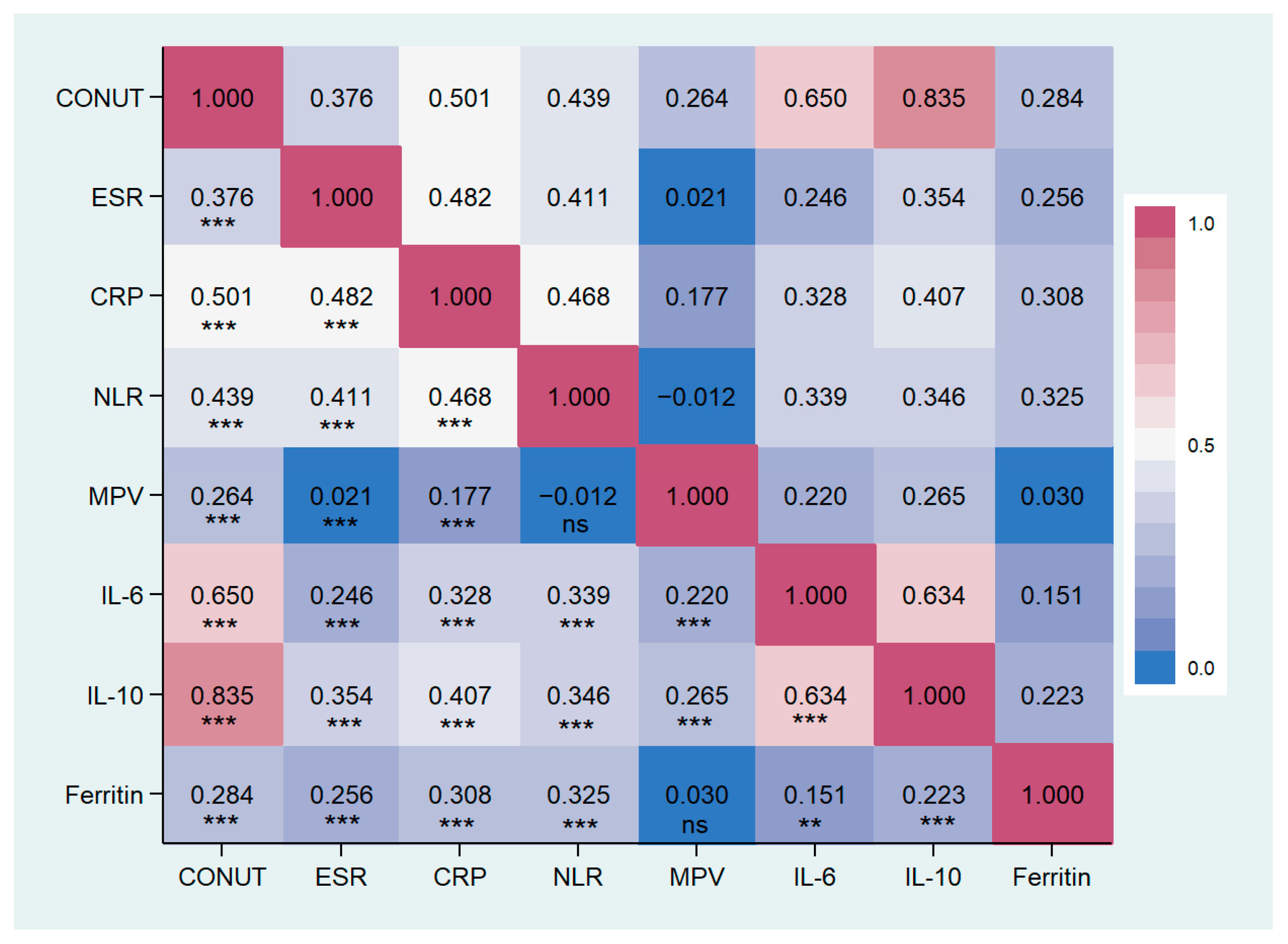
3.2. CONUT Score and Inflammatory Markers
3.3. CONUT Score, Anthropometric Measures, and Body Composition
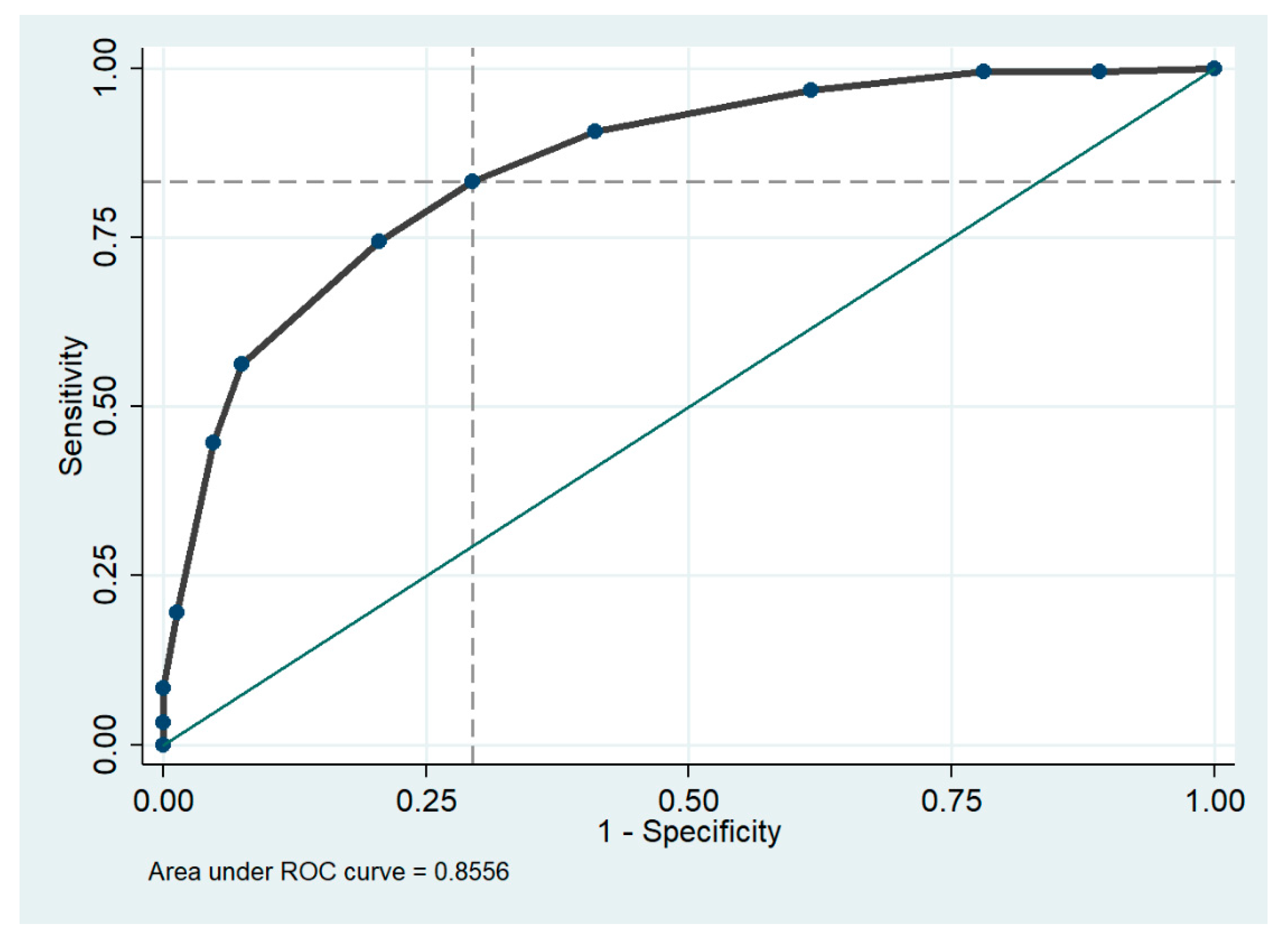
3.4. CONUT Score as Predictor of Frailty
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Norman, K.; Haß, U.; Pirlich, M. Malnutrition in Older Adults—Recent Advances and Remaining Challenges. Nutrients 2021, 13, 2764. [Google Scholar] [CrossRef]
- Saunders, J.; Smith, T. Malnutrition: Causes and consequences. Clin. Med. 2010, 10, 624–627. [Google Scholar] [CrossRef]
- Miano, N.; Di Marco, M.; Alaimo, S.; Coppolino, G.; L’Episcopo, G.; Leggio, S.; Scicali, R.; Piro, S.; Purrello, F.; Di Pino, A.; et al. Controlling Nutritional Status (CONUT) Score as a Potential Prognostic Indicator of In-Hospital Mortality, Sepsis and Length of Stay in an Internal Medicine Department. Nutrients 2023, 15, 1554. [Google Scholar] [CrossRef]
- Muresan, B.T.; Núñez-Abad, M.; Artero, A.; Rios Rios, J.; Cunquero-Tomás, A.J.; Iranzo, V.; Garrido, J.; Jiménez-Portilla, A.; Camps Herrero, C.; Sánchez Juan, C.J. Relation of Malnutrition and Nosocomical Infections in Cancer Patients in Hospital: An Observational Study. J. Nutr. Metab. 2022, 2022, 5232480. [Google Scholar] [CrossRef]
- Rinninella, E.; Borriello, R.; D’Angelo, M.; Galasso, T.; Cintoni, M.; Raoul, P.; Impagnatiello, M.; Annicchiarico, B.E.; Gasbarrini, A.; Mele, M.C. COntrolling NUTritional Status (CONUT) as Predictive Score of Hospital Length of Stay (LOS) and Mortality: A Prospective Cohort Study in an Internal Medicine and Gastroenterology Unit in Italy. Nutrients 2023, 15, 1472. [Google Scholar] [CrossRef]
- Rajendran, P.; Chen, Y.; Chen, Y.; Chung, L.; Tamilselvi, S.; Shen, C.; Day, C.H.; Chen, R.; Viswanadha, V.P.; Kuo, W.; et al. The multifaceted link between inflammation and human diseases. J. Cell. Physiol. 2018, 233, 6458–6471. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Bosco, N.; Bourdet-Sicard, R.; Capuron, L.; Delzenne, N.; Doré, J.; Franceschi, C.; Lehtinen, M.J.; Recker, T.; Salvioli, S.; et al. Health relevance of the modification of low grade inflammation in ageing (inflammageing) and the role of nutrition. Ageing Res. Rev. 2017, 40, 95–119. [Google Scholar] [CrossRef] [PubMed]
- Bellanti, F.; Romano, A.D.; Lo Buglio, A.; Castriotta, V.; Guglielmi, G.; Greco, A.; Serviddio, G.; Vendemiale, G. Oxidative stress is increased in sarcopenia and associated with cardiovascular disease risk in sarcopenic obesity. Maturitas 2018, 109, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Mądra-Gackowska, K.; Szewczyk-Golec, K.; Gackowski, M.; Woźniak, A.; Kędziora-Kornatowska, K. Evaluation of Selected Parameters of Oxidative Stress and Adipokine Levels in Hospitalized Older Patients with Diverse Nutritional Status. Antioxidants 2023, 12, 569. [Google Scholar] [CrossRef]
- Dalleau, S.; Baradat, M.; Guéraud, F.; Huc, L. Cell death and diseases related to oxidative stress:4-hydroxynonenal (HNE) in the balance. Cell Death Differ. 2013, 20, 1615–1630. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, M.C.; Clemens, D.L.; Duryee, M.J.; Sarmiento, C.; Chiou, A.; Hunter, C.D.; Tian, J.; Klassen, L.W.; O’Dell, J.R.; Thiele, G.M.; et al. Direct antioxidant properties of methotrexate: Inhibition of malondialdehyde-acetaldehyde-protein adduct formation and superoxide scavenging. Redox Biol. 2017, 13, 588–593. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, T.; Li, J.; Xia, M.; Li, Y.; Wang, X.; Liu, C.; Zheng, T.; Chen, R.; Kan, D.; et al. Oxidative Stress and 4-hydroxy-2-nonenal (4-HNE): Implications in the Pathogenesis and Treatment of Aging-related Diseases. J. Immunol. Res. 2022, 2022, 2233906. [Google Scholar] [CrossRef]
- Ciancarelli, I.; Morone, G.; Iosa, M.; Cerasa, A.; Calabrò, R.S.; Iolascon, G.; Gimigliano, F.; Tonin, P.; Tozzi Ciancarelli, M.G. Influence of Oxidative Stress and Inflammation on Nutritional Status and Neural Plasticity: New Perspectives on Post-Stroke Neurorehabilitative Outcome. Nutrients 2022, 15, 108. [Google Scholar] [CrossRef]
- Stumpf, F.; Keller, B.; Gressies, C.; Schuetz, P. Inflammation and Nutrition: Friend or Foe? Nutrients 2023, 15, 1159. [Google Scholar] [CrossRef]
- Antuña, E.; Cachán-Vega, C.; Bermejo-Millo, J.C.; Potes, Y.; Caballero, B.; Vega-Naredo, I.; Coto-Montes, A.; Garcia-Gonzalez, C. Inflammaging: Implications in Sarcopenia. Int. J. Mol. Sci. 2022, 23, 15039. [Google Scholar] [CrossRef]
- Padilha de Lima, A.; Macedo Rogero, M.; Araujo Viel, T.; Garay-Malpartida, H.M.; Aprahamian, I.; Lima Ribeiro, S.M. Interplay between Inflammaging, Frailty and Nutrition in COVID-19: Preventive and Adjuvant Treatment Perspectives. J. Nutr. Health Aging 2022, 26, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Lo Buglio, A.; Bellanti, F.; Serviddio, G.; Vendemiale, G. Impact of Nutritional Status on Muscle Architecture in Elderly Patients Hospitalized in Internal Medicine Wards. J. Nutr. Health Aging 2020, 24, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Wennberg, A.M.; Ebeling, M.; Ek, S.; Meyer, A.; Ding, M.; Talbäck, M.; Modig, K. Trends in Frailty Between 1990 and 2020 in Sweden Among 75-, 85-, and 95-Year-Old Women and Men: A Nationwide Study from Sweden. J. Gerontol. Ser. A 2023, 78, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Osatnik, J.; Matarrese, A.; Leone, B.; Cesar, G.; Kleinert, M.; Sosa, F.; Roberti, J.; Ivulich, D. Frailty and clinical outcomes in critically ill patients with cancer: A cohort study. J. Geriatr. Oncol. 2022, 13, 1156–1161. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.; Ueno, R.; Afroz, A.; Billah, B.; Tiruvoipati, R.; Subramaniam, A. Association between frailty and clinical outcomes in surgical patients admitted to intensive care units: A systematic review and meta-analysis. Br. J. Anaesth. 2022, 128, 258–271. [Google Scholar] [CrossRef]
- Cortes, R.; Bennasar-Veny, M.; Castro-Sanchez, E.; Fresneda, S.; de Pedro-Gomez, J.; Yañez, A. Nutrition screening tools for risk of malnutrition among hospitalized patients. Medicine 2020, 99, e22601. [Google Scholar] [CrossRef]
- Aloy dos Santos, T.; Luft, V.C.; Souza, G.C.; de Albuquerque Santos, Z.; Keller Jochims, A.M.; Carnevale de Almeida, J. Malnutrition screening tool and malnutrition universal screening tool as a predictors of prolonged hospital stay and hospital mortality: A cohort study. Clin. Nutr. ESPEN 2023, 54, 430–435. [Google Scholar] [CrossRef]
- Bellanti, F.; Lo Buglio, A.; Quiete, S.; Vendemiale, G. Malnutrition in Hospitalized Old Patients: Screening and Diagnosis, Clinical Outcomes, and Management. Nutrients 2022, 14, 910. [Google Scholar] [CrossRef]
- Soysal, P.; Veronese, N.; Arik, F.; Kalan, U.; Smith, L.; ISIK, A.T. Mini Nutritional Assessment Scale-Short Form can be useful for frailty screening in older adults. Clin. Interv. Aging 2019, 14, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Sharma, Y.; Avina, P.; Ross, E.; Horwood, C.; Hakendorf, P.; Thompson, C. Validity of the Malnutrition Universal Screening Tool for Evaluation of Frailty Status in Older Hospitalised Patients. Gerontol. Geriatr. Med. 2022, 8, 233372142211078. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, A.D.; van der Windt, D.A.; Riley, R.D.; Abrams, K.; Moons, K.G.M.; Steyerberg, E.W.; Schroter, S.; Sauerbrei, W.; Altman, D.G.; Hemingway, H. Prognosis research strategy (PROGRESS) 4: Stratified medicine research. BMJ 2013, 346, e5793. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Moons, K.G.M.; van der Windt, D.A.; Hayden, J.A.; Perel, P.; Schroter, S.; Riley, R.D.; Hemingway, H.; Altman, D.G. Prognosis Research Strategy (PROGRESS) 3: Prognostic Model Research. PLoS Med. 2013, 10, e1001381. [Google Scholar] [CrossRef]
- Özkan, A.E.; Koca, N.; Tekeli, A.H. Assessment of nutritional status and clinical outcomes: A comprehensive retrospective analysis of critically ill patients. Medicine 2023, 102, e36018. [Google Scholar] [CrossRef] [PubMed]
- Zanetti, M.; Marzaro, G.; De Colle, P.; Toigo, G.; Bianchini, D.; Nastri, M.; Suriano, C.; Barazzoni, R.; Sanson, G. Predictors of short- and long-term mortality among acutely admitted older patients: Role of inflammation and frailty. Aging Clin. Exp. Res. 2022, 34, 409–418. [Google Scholar] [CrossRef]
- Li, Q.; Shang, N.; Gao, Q.; Yang, L.; Guo, S. Computed tomography-based body composition is associated with adverse clinical outcomes among older patients with sepsis in the emergency department. Eur. Geriatr. Med. 2023, 14, 353–361. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.P.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Sun, X.; Luo, L.; Zhao, X.; Ye, P. Controlling Nutritional Status (CONUT) score as a predictor of all-cause mortality in elderly hypertensive patients: A prospective follow-up study. BMJ Open 2017, 7, e015649. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.; Guigoz, Y.; Garry, P.J.; Nourhashemi, F.; Bennahum, D.; Lauque, S.; Albarede, J.-L. The mini nutritional assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999, 15, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Power, L.; Mullally, D.; Gibney, E.R.; Clarke, M.; Visser, M.; Volkert, D.; Bardon, L.; de van der Schueren, M.A.E.; Corish, C.A. A review of the validity of malnutrition screening tools used in older adults in community and healthcare settings—A MaNuEL study. Clin. Nutr. ESPEN 2018, 24, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Akpom, C.A. A Measure of Primary Sociobiological Functions. Int. J. Health Serv. 1976, 6, 493–508. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Lesher, E.L.; Berryhill, J.S. Validation of the geriatric depression scale-short form among inpatients. J. Clin. Psychol. 1994, 50, 256–260. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Bioelectrical impedance analysis in body composition measurement: National Institutes of Health Technology Assessment Conference Statement. Am. J. Clin. Nutr. 1996, 64, 524S–532S. [CrossRef]
- Gallagher Allred, C.R.; Coble Voss, A.; Finn, S.C.; McCamish, M.A. Malnutrition and Clinical Outcomes. J. Am. Diet. Assoc. 1996, 96, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, A.J.; Buitrago, G.; Rodríguez, N.; Gómez, G.; Sulo, S.; Gómez, C.; Partridge, J.; Misas, J.; Dennis, R.; Alba, M.J.; et al. Clinical and economic outcomes associated with malnutrition in hospitalized patients. Clin. Nutr. 2019, 38, 1310–1316. [Google Scholar] [CrossRef]
- O’Shea, E.; Trawley, S.; Manning, E.; Barrett, A.; Browne, V.; Timmons, S. Malnutrition in hospitalised older adults: A multicentre observational study of prevalence, associations and outcomes. J. Nutr. Health Aging 2017, 21, 830–836. [Google Scholar] [CrossRef]
- Hiesmayr, M.; Tarantino, S.; Moick, S.; Laviano, A.; Sulz, I.; Mouhieddine, M.; Schuh, C.; Volkert, D.; Simon, J.; Schindler, K. Hospital Malnutrition, a Call for Political Action: A Public Health and NutritionDay Perspective. J. Clin. Med. 2019, 8, 2048. [Google Scholar] [CrossRef]
- Zugasti Murillo, A.; Petrina-Jáuregui, M.E.; Ripa-Ciáurriz, C.; Sánchez Sánchez, R.; Villazón-González, F.; González-Díaz Faes, Á.; Fernández-López, C.; Calles-Romero, L.; Martín-Palmero, Á.; Riestra-Fernández, M.; et al. SeDREno study—Prevalence of hospital malnutrition according to GLIM criteria, ten years after the PREDyCES study. Nutr. Hosp. 2021, 38, 1016–1025. [Google Scholar] [CrossRef]
- Skeie, E.; Sygnestveit, K.; Nilsen, R.M.; Harthug, S.; Koch, A.M.; Tangvik, R.J. Prevalence of patients “at risk of malnutrition” and nutritional routines among surgical and non-surgical patients at a large university hospital during the years 2008–2018. Clin. Nutr. 2021, 40, 4738–4744. [Google Scholar] [CrossRef] [PubMed]
- Castel, H.; Shahar, D.; Harman-Boehm, I. Gender Differences in Factors Associated with Nutritional Status of Older Medical Patients. J. Am. Coll. Nutr. 2006, 25, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Formiga, F.; Ferrer, A.; de Ulíbarri Pérez, J.I.; Badia, T.; Montero, A.; Soldevila, L.; Moreno, R.; Corbella, X. Detecting malnutrition and predicting mortality in the Spanish oldest old: Utility of the Controlling Nutritional Status (CONUT) score compared with the Mini Nutritional Assessment (MNA) score. Eur. Geriatr. Med. 2016, 7, 566–570. [Google Scholar] [CrossRef]
- Cabré, M.; Ferreiro, C.; Arus, M.; Roca, M.; Palomera, E.; Serra-Prat, M. Evaluation of CONUT for Clinical Malnutrition Detection and Short-Term Prognostic Assessment in Hospitalized Elderly People. J. Nutr. Health Aging 2015, 19, 729–733. [Google Scholar] [CrossRef]
- Uemura, Y.; Shibata, R.; Miyagaki, Y.; Takemoto, K.; Ishikawa, S.; Murohara, T.; Watarai, M. A Comparative Study of Three Nutritional Risk/Screening Indices for Predicting Cardiac Events and Physical Functioning Among Patients with Acute Heart Failure. Int. Heart J. 2022, 63, 21–809. [Google Scholar] [CrossRef]
- Yamaura, T.; Arizumi, F.; Maruo, K.; Kishima, K.; Yoshie, N.; Kusukawa, T.; Imamura, F.; Tachibana, T. The Impact of Controlling Nutritional Status (CONUT) score on functional prognosis in hospitalized elderly patients with acute osteoporotic vertebral fractures. BMC Geriatr. 2022, 22, 1002. [Google Scholar] [CrossRef]
- Takagi, K.; Takahashi, H.; Miura, T.; Yamagiwa, K.; Kawase, K.; Muramatsu-Maekawa, Y.; Koie, T.; Mizuno, M. Prognostic Value of the Controlling Nutritional Status (CONUT) Score in Patients at Dialysis Initiation. Nutrients 2022, 14, 2317. [Google Scholar] [CrossRef]
- Xiao, Q.; Li, X.; Duan, B.; Li, X.; Liu, S.; Xu, B.; Shi, S.; Zhang, J.; Qin, H.; Duan, X.; et al. Clinical significance of controlling nutritional status score (CONUT) in evaluating outcome of postoperative patients with gastric cancer. Sci. Rep. 2022, 12, 93. [Google Scholar] [CrossRef]
- Bornæs, O.; Andersen, A.L.; Houlind, M.B.; Kallemose, T.; Tavenier, J.; Aharaz, A.; Nielsen, R.L.; Jørgensen, L.M.; Beck, A.M.; Andersen, O.; et al. Mild Cognitive Impairment Is Associated with Poorer Nutritional Status on Hospital Admission and after Discharge in Acutely Hospitalized Older Patients. Geriatrics 2022, 7, 95. [Google Scholar] [CrossRef]
- Ramsey, K.A.; Meskers, C.G.M.; Trappenburg, M.C.; Verlaan, S.; Reijnierse, E.M.; Whittaker, A.C.; Maier, A.B. Malnutrition is associated with dynamic physical performance. Aging Clin. Exp. Res. 2020, 32, 1085–1092. [Google Scholar] [CrossRef]
- Hettiarachchi, J.; Reijnierse, E.M.; Soh, C.H.; Agius, B.; Fetterplace, K.; Lim, W.K.; Maier, A.B. Malnutrition is associated with poor trajectories of activities of daily living in geriatric rehabilitation inpatients: RESORT. Mech. Ageing Dev. 2021, 197, 111500. [Google Scholar] [CrossRef]
- Flood, A.; Chung, A.; Parker, H.; Kearns, V.; O’Sullivan, T.A. The use of hand grip strength as a predictor of nutrition status in hospital patients. Clin. Nutr. 2014, 33, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Fogg, C.; Griffiths, P.; Meredith, P.; Bridges, J. Hospital outcomes of older people with cognitive impairment: An integrative review. Int. J. Geriatr. Psychiatry 2018, 33, 1177–1197. [Google Scholar] [CrossRef]
- Verweij, N.M.; Schiphorst, A.H.W.; Pronk, A.; van den Bos, F.; Hamaker, M.E. Physical performance measures for predicting outcome in cancer patients: A systematic review. Acta Oncol. 2016, 55, 1386–1391. [Google Scholar] [CrossRef] [PubMed]
- Jenab, Y.; Hosseini, K.; Esmaeili, Z.; Tofighi, S.; Ariannejad, H.; Sotoudeh, H. Prediction of in-hospital adverse clinical outcomes in patients with pulmonary thromboembolism, machine learning based models. Front. Cardiovasc. Med. 2023, 10, 1087702. [Google Scholar] [CrossRef]
- Islam, M.Z.; Disu, T.R.; Farjana, S.; Rahman, M.M. Malnutrition and other risk factors of geriatric depression: A community-based comparative cross-sectional study in older adults in rural Bangladesh. BMC Geriatr. 2021, 21, 572. [Google Scholar] [CrossRef]
- Yildirim, D. Relationship between the depression levels and nutritional statuses of advanced stage cancer patients. Palliat. Support. Care 2021, 20, 1–8. [Google Scholar] [CrossRef]
- Hao, R.; Qi, X.; Xia, X.; Wang, L.; Li, X. Malnutrition on admission increases the in-hospital mortality and length of stay in elder adults with acute ischemic stroke. J. Clin. Lab. Anal. 2022, 36, e24132. [Google Scholar] [CrossRef]
- Gu, M.; Wang, J.; Xiao, L.; Chen, X.; Wang, M.; Huang, Q.; Zhou, J.; Sun, W. Malnutrition and poststroke depression in patients with ischemic stroke. J. Affect. Disord. 2023, 334, 113–120. [Google Scholar] [CrossRef]
- Hickson, M. Malnutrition and ageing. Postgrad. Med. J. 2006, 82, 2–8. [Google Scholar] [CrossRef]
- Buglio, A.L.; Bellanti, F.; Capurso, C.; Paglia, A.; Vendemiale, G. Adherence to Mediterranean Diet, Malnutrition, Length of Stay and Mortality in Elderly Patients Hospitalized in Internal Medicine Wards. Nutrients 2019, 11, 790. [Google Scholar] [CrossRef]
- Shizgal, H.M. The effect of malnutrition on body composition. Surg. Gynecol. Obstet. 1981, 152, 22–26. [Google Scholar] [PubMed]
- Landi, F.; Camprubi-Robles, M.; Bear, D.E.; Cederholm, T.; Malafarina, V.; Welch, A.A.; Cruz-Jentoft, A.J. Muscle loss: The new malnutrition challenge in clinical practice. Clin. Nutr. 2019, 38, 2113–2120. [Google Scholar] [CrossRef] [PubMed]
- Amarya, S.; Singh, K.; Sabharwal, M. Changes during aging and their association with malnutrition. J. Clin. Gerontol. Geriatr. 2015, 6, 78–84. [Google Scholar] [CrossRef]
- Kaluźniak-Szymanowska, A.; Krzymińska-Siemaszko, R.; Deskur-Śmielecka, E.; Lewandowicz, M.; Kaczmarek, B.; Wieczorowska-Tobis, K. Malnutrition, Sarcopenia, and Malnutrition-Sarcopenia Syndrome in Older Adults with COPD. Nutrients 2021, 14, 44. [Google Scholar] [CrossRef]
- Kramer, C.S.; Groenendijk, I.; Beers, S.; Wijnen, H.H.; van de Rest, O.; de Groot, L.C. The Association between Malnutrition and Physical Performance in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Curr. Dev. Nutr. 2022, 6, nzac007. [Google Scholar] [CrossRef] [PubMed]
- Serafini, E.; Marzetti, E.C.R. Nutritional approach to sarcopenia. J. Gerontol. Geriatr. 2019, 67, 52–61. [Google Scholar]
- Meza-Valderrama, D.; Marco, E.; Dávalos-Yerovi, V.; Muns, M.D.; Tejero-Sánchez, M.; Duarte, E.; Sánchez-Rodríguez, D. Sarcopenia, Malnutrition, and Cachexia: Adapting Definitions and Terminology of Nutritional Disorders in Older People with Cancer. Nutrients 2021, 13, 761. [Google Scholar] [CrossRef]
- Wilson, D.; Jackson, T.; Sapey, E.; Lord, J.M. Frailty and sarcopenia: The potential role of an aged immune system. Ageing Res. Rev. 2017, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Li, X.; Lin, X.; Ju, Y.; Leng, J. The correlation between nutrition and frailty and the receiver operating characteristic curve of different nutritional indexes for frailty. BMC Geriatr. 2021, 21, 619. [Google Scholar] [CrossRef] [PubMed]
- Norazman, C.W.; Adznam, S.N.; Jamaluddin, R. Malnutrition as Key Predictor of Physical Frailty among Malaysian Older Adults. Nutrients 2020, 12, 1713. [Google Scholar] [CrossRef]
- Soysal, P.; Stubbs, B.; Lucato, P.; Luchini, C.; Solmi, M.; Peluso, R.; Sergi, G.; Isik, A.T.; Manzato, E.; Maggi, S.; et al. Inflammation and frailty in the elderly: A systematic review and meta-analysis. Ageing Res. Rev. 2016, 31, 1–8. [Google Scholar] [CrossRef]
- Fatyga, P.; Pac, A.; Fedyk-Łukasik, M.; Grodzicki, T.; Skalska, A. The relationship between malnutrition risk and inflammatory biomarkers in outpatient geriatric population. Eur. Geriatr. Med. 2020, 11, 383–391. [Google Scholar] [CrossRef]
- Keller, U. Nutritional Laboratory Markers in Malnutrition. J. Clin. Med. 2019, 8, 775. [Google Scholar] [CrossRef]
- Tan, C.S.Y.; Read, J.A.; Phan, V.H.; Beale, P.J.; Peat, J.K.; Clarke, S.J. The relationship between nutritional status, inflammatory markers and survival in patients with advanced cancer: A prospective cohort study. Support. Care Cancer 2015, 23, 385–391. [Google Scholar] [CrossRef]
- Monk, J.M.; Steevels, T.A.M.; Hillyer, L.M.; Woodward, B. Constitutive, but Not Challenge-Induced, Interleukin-10 Production Is Robust in Acute Pre-Pubescent Protein and Energy Deficits: New Support for the Tolerance Hypothesis of Malnutrition-Associated Immune Depression Based on Cytokine Production in vivo. Int. J. Environ. Res. Public Health 2011, 8, 117–135. [Google Scholar] [CrossRef]
- Villani, R.; Cavallone, F.; Romano, A.D.; Bellanti, F.; Serviddio, G. Two-Dimensional Shear Wave Elastography versus Transient Elastography: A Non-Invasive Comparison for the Assessment of Liver Fibrosis in Patients with Chronic Hepatitis C. Diagnostics 2020, 10, 313. [Google Scholar] [CrossRef]
- Chen, L.; Deng, H.; Cui, H.; Fang, J.; Zuo, Z.; Deng, J.; Li, Y.; Wang, X.; Zhao, L. Inflammatory responses and inflammation-associated diseases in organs. Oncotarget 2018, 9, 7204–7218. [Google Scholar] [CrossRef]
- Romano, A.D.; Lo Buglio, A.; Bellanti, F.; Villani, R.; Serviddio, G.; Vendemiale, G. Diagnostic reliability of the procalcitonin serum marker in septic frail patient. Aging Clin. Exp. Res. 2019, 31, 727–732. [Google Scholar] [CrossRef]
- Pourhassan, M.; Cederholm, T.; Trampisch, U.; Volkert, D.; Wirth, R. Inflammation as a diagnostic criterion in the GLIM definition of malnutrition—What CRP-threshold relates to reduced food intake in older patients with acute disease? Eur. J. Clin. Nutr. 2022, 76, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Li, M.; Chang, M.; Liu, R.; Qiu, J.; Wang, K.; Deng, C.; Shen, Y.; Zhu, J.; Wang, W.; et al. Inflammation: Roles in Skeletal Muscle Atrophy. Antioxidants 2022, 11, 1686. [Google Scholar] [CrossRef]
- Dalle, S.; Rossmeislova, L.; Koppo, K. The Role of Inflammation in Age-Related Sarcopenia. Front. Physiol. 2017, 8, 1045. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Lee, J.; Jung, Y.S.; Kwon, W.Y.; Oh, D.K.; Park, M.H.; Lim, C.-M.; Lee, S.-M. Preexisting Clinical Frailty Is Associated with Worse Clinical Outcomes in Patients with Sepsis. Crit. Care Med. 2022, 50, 780–790. [Google Scholar] [CrossRef] [PubMed]
- Boucher, E.L.; Gan, J.M.; Rothwell, P.M.; Shepperd, S.; Pendlebury, S.T. Prevalence and outcomes of frailty in unplanned hospital admissions: A systematic review and meta-analysis of hospital-wide and general (internal) medicine cohorts. eClinicalMedicine 2023, 59, 101947. [Google Scholar] [CrossRef]
- Guerra, R.S.; Fonseca, I.; Sousa, A.S.; Jesus, A.; Pichel, F.; Amaral, T.F. ESPEN diagnostic criteria for malnutrition—A validation study in hospitalized patients. Clin. Nutr. 2017, 36, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Visvanathan, R.; Piantadosi, C.; Chapman, I. Use of the Mini Nutritional assessment to detect frailty in hospitalised older people. J. Nutr. Health Aging 2012, 16, 764–767. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nutritional Status | ||||
|---|---|---|---|---|
| Variables | Normal | Light | Moderate | Severe |
| Albumin (g/dL) Score | ≥3.5 0 | 3.0–3.49 2 | 2.5–2.9 4 | <2.5 6 |
| Total lymphocyte (/mm3) Score | >1600 0 | 1200–1599 1 | 800–1199 2 | <800 3 |
| Total cholesterol (mg/dL) Score | >180 0 | 140–180 1 | 100–139 2 | <100 3 |
| Screening total score | 0–1 | 2–4 | 5–8 | 9–12 |
| Normal (Score 0–1) n. 33 (9.1%) | Mild (Score 2–4) n. 106 (29.4%) | Moderate/Severe (Score ≥ 5) n. 222 (61.5%) | p Value | |
|---|---|---|---|---|
| Age, years | 74.1 ± 7.2 | 76.9 ± 7.7 | 81.1 ± 7.8 | <0.001 |
| Genre F, n (%) | 19 (57.6) | 62 (58.5) | 134 (60.4) | 0.922 |
| Comorbities, ≥3 | 12 (36.4) | 47 (44.3) | 103 (46.4) | 0.553 |
| Haemoglobin, g/dL | 13.5 ± 1.5 | 12.1 ± 2.0 | 10.9 ± 1.8 | <0.001 |
| WBC, n/mm3 | 6900 [5800–9225] | 7130 [5350–8790] | 7400 [5000–11,090] | 0.918 |
| Neutrophils, n/mm3 | 4319 [3247–5638] | 4613 [3445–6381] | 5639 [3368–8940] | 0.021 |
| Lymphocytes, n/mm3 | 1991 [1687–2449] | 1473 [1065–2160] | 981 [730–1370] | <0.001 |
| Platelet, 103/mm3 | 202 [181–242] | 193 [136–245] | 189 [126–236] | 0.249 |
| Glucose, mg/dL | 100 [89–120] | 107 [88–141] | 107 [82–139] | 0.598 |
| Albumin, g/dL | 4.0 ± 0.4 | 3.4 ± 0.4 | 2.8 ± 0.4 | <0.001 |
| Creatinine, mg/dL | 0.85 [0.70–1.07] | 0.94 [0.77–1.27] | 1.06 [0.80–1.49] | 0.015 |
| Total cholesterol, mg/dL | 185 [172–215] | 164 [144–189] | 125 [105–147] | <0.001 |
| LDL, mg/dL | 113 [105–127] | 98 [86–126] | 78 [60–96] | <0.001 |
| HDL, mg/dL | 49 [42–62] | 45 [34–55] | 33 [25–40] | <0.001 |
| Triglycerides, mg/dL | 131 [77–171] | 106 [87–149] | 103 [73–142] | 0.182 |
| ESR, mm/h | 9.0 [4.5–63.0] | 30.0 [7.0–76.7] | 66.0 [40.0–88.2] | <0.001 |
| CRP, ng/mL | 2.9 [1.3–4.5] | 7.0 [3.7–10.0] | 20.9 [12.4–43.7] | <0.001 |
| NLR | 1.3 [1.2–4.5] | 2.2 [1.6–3.5] | 5.4 [3.7–7.1] | <0.001 |
| MPV, fL | 10.1 ± 0.9 | 11.1 ± 1.2 | 11.7 ± 1.4 | <0.001 |
| Ferritin, ng/mL | 87 [29–158] | 98 [35–207] | 182 [57–435] | <0.001 |
| IL1α, pg/mL | 0.8 [0.4–1.2] | 0.6 [0.3–1.0] | 0.7 [0.3–1.0] | 0.258 |
| IL1β, pg/mL | 0.1 [0.0–0.3] | 0.7 [0.3–0.9] | 0.5 [0.3–0.8] | 0.390 |
| IL2, U/mL | 0.2 [0.1–0.7] | 0.6 [0.3–1.0] | 0.4 [0.2–0.6] | 0.683 |
| IL6, pg/mL | 2.3 [1.0–2.9] | 5.1 [2.9–12.6] | 18.6 [14.2–19.8] | <0.001 |
| IL8, pg | 67.5 [39.7–123.4] | 104.1 [56.4–125.0] | 121.6 [92.8–194.3] | 0.754 |
| IL10, pg/mL | 0.5 [0.3–0.6] | 1.26 [0.9–1.7] | 2.2 [1.7–3.0] | <0.001 |
| TNFα, pg/mL | 3.3 [3.2–3.7] | 3.6 [2.3–6.6] | 3.7 [2.6–4.9] | 0.236 |
| EGF, pg/mL | 16.0 [9.7–28.9] | 11.4 [7.6–13.2] | 8.7 [7.1–13.8] | 0.079 |
| VEGF, pg | 196.2 [124.3–349.2] | 169.0 [128.4–299.3] | 220.0 [161.0–295.6] | 0.944 |
| INFγ, pg/mL | 0.9 [0.3–0.9] | 0.9 [0.5–4.8] | 0.7 [0.1–0.9] | 0.514 |
| Normal (Score 0–1) n. 33 (9.1%) | Mild (Score 2–4) n. 106 (29.4%) | Moderate/Severe (Score ≥ 5) n. 222 (61.5%) | p Value | |
|---|---|---|---|---|
| MNA, score | 25.1 ± 2.1 | 21.9 ± 4.2 | 17.4 ± 4.4 | <0.001 |
| MMSE, score | 23.9 ± 3.8 | 22.2 ± 7.6 | 17.9 ± 8.7 | <0.001 |
| ADL, score | 5 [4–6] | 6 [5–6] | 4 [2–6] | <0.001 |
| IADL, score | 7 [6–7] | 7 [4–8] | 3 [1–5] | <0.001 |
| Barthel, score | 95 [85–95] | 90 [60–95] | 70 [45–90] | <0.001 |
| GDS-SF, score | 1 [1–3] | 3 [1–6] | 5 [3–7] | <0.001 |
| Frail, n (%) | 1 (3.0) | 35 (33.0) | 179 (80.6) | <0.001 |
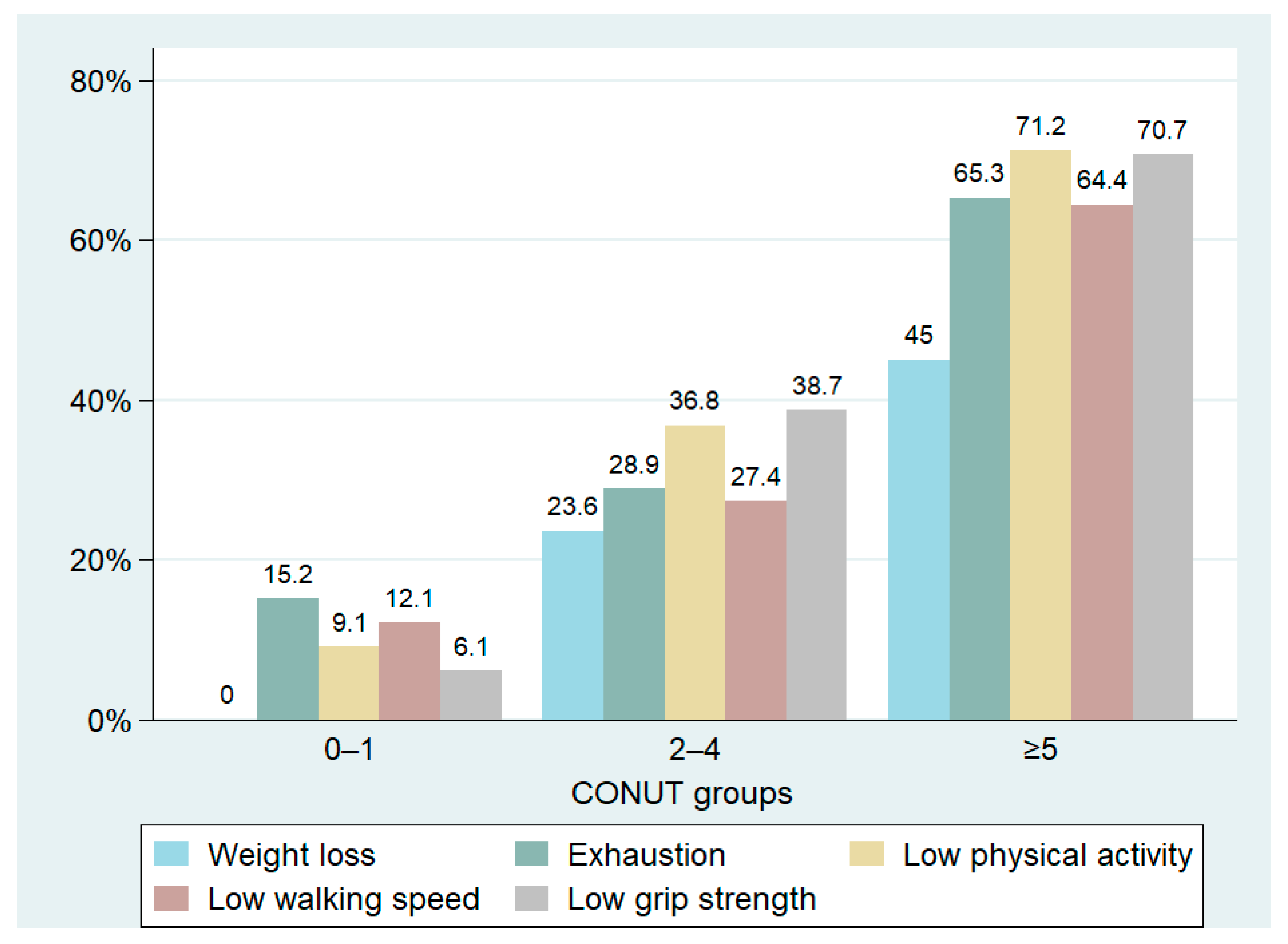
| Fried’s score items | ||||
| Weight loss, n (%) | 0 (0.0%) | 25 (23.6%) | 100 (45.0%) | <0.001 |
| Exhaustion, n (%) | 5 (15.2%) | 20 (18.9%) | 145 (65.3%) | <0.001 |
| Low physical activity, n (%) | 3 (9.1%) | 39 (36.8%) | 158 (71.2%) | <0.001 |
| Low walking speed, n (%) | 4 (12.1%) | 29 (27.4%) | 143 (64.4%) | <0.001 |
| Low grip strength, n (%) | 2 (6.1%) | 41 (38.7%) | 157 (70.7%) | <0.001 |
| r | p Value | |
|---|---|---|
| ESR, mm/h | 0.376 | <0.001 |
| CRP, ng/mL | 0.501 | <0.001 |
| NLR | 0.439 | <0.001 |
| MPV, fL | 0.264 | <0.001 |
| IL-6, pg/mL | 0.650 | <0.001 |
| IL-10, pg/mL | 0.835 | <0.001 |
| Ferritin, ng/mL | 0.284 | <0.001 |
| MNA, score | −0.493 | <0.001 |
| MMSE, score | −0.263 | <0.001 |
| ADL, score | −0.356 | <0.001 |
| IADL, score | −0.510 | <0.001 |
| Barthel, score | −0.325 | <0.001 |
| GDS-SF, score | 0.278 | <0.001 |
| FM, % | 0.420 | <0.001 |
| FFM, % | −0.420 | <0.001 |
| MM, % | −0.235 | <0.001 |
| Normal (Score 0–1) n. 33 (9.1%) | Mild (Score 2–4) n. 106 (29.4%) | Moderate/Severe (Score ≥ 5) n. 222 (61.5%) | p Value | |
|---|---|---|---|---|
| BMI, kg/m2 | 28.0 [24.8–31.4] | 27. 0 [24.7–30.9] | 25.1 [22.6–29.1] | <0.001 |
| Arm circumference, cm | 28.9 ± 3.5 | 27.9 ± 5.2 | 25.1 ± 4.7 | <0.001 |
| Thigh circumference, cm | 52.9 ± 8.6 | 44.0 ± 7.5 | 39.8 ± 7.4 | <0.001 |
| Waist circumference, cm | 101.8 ± 14.3 | 105.7 ± 17.8 | 99.6 ± 13.9 | 0.003 |
| Calf circumference, cm | 34.5 ± 3.7 | 31.5 ± 5.5 | 29.4 ± 5.6 | <0.001 |
| FM, % | 32.4 [26.8–36.5] | 34.1 [30.2–43.6] | 42.4 [39.2–46.1] | <0.001 |
| FFM, %, | 67.6 [63.4–73.2] | 65.9 [56.4–69.8] | 57.6 [53.9–60.8] | <0.001 |
| MM, % | 34.0 [29.3–39.2] | 30.6 [25.5–35.3] | 28.3 [24.3–33.3] | <0.001 |
| TBW, % | 54.5 [50.6–59.3] | 51.2 [45.1–56.0] | 51.8 [45.5–58.2] | 0.188 |
| ECW, % | 50.1 [46.2–55.7] | 51.4 [46.4–56.7] | 51.7 [47.5–58.6] | 0.519 |
| ICW, % | 49.9 [44.2–53.7] | 48.6 [43.3–53.6] | 48.2 [41.4–52.5] | 0.519 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Buglio, A.; Bellanti, F.; Carmignano, D.F.P.; Serviddio, G.; Vendemiale, G. Association between Controlling Nutritional Status (CONUT) Score and Body Composition, Inflammation and Frailty in Hospitalized Elderly Patients. Nutrients 2024, 16, 576. https://doi.org/10.3390/nu16050576
Lo Buglio A, Bellanti F, Carmignano DFP, Serviddio G, Vendemiale G. Association between Controlling Nutritional Status (CONUT) Score and Body Composition, Inflammation and Frailty in Hospitalized Elderly Patients. Nutrients. 2024; 16(5):576. https://doi.org/10.3390/nu16050576
Chicago/Turabian StyleLo Buglio, Aurelio, Francesco Bellanti, Daniela Francesca Pia Carmignano, Gaetano Serviddio, and Gianluigi Vendemiale. 2024. "Association between Controlling Nutritional Status (CONUT) Score and Body Composition, Inflammation and Frailty in Hospitalized Elderly Patients" Nutrients 16, no. 5: 576. https://doi.org/10.3390/nu16050576
APA StyleLo Buglio, A., Bellanti, F., Carmignano, D. F. P., Serviddio, G., & Vendemiale, G. (2024). Association between Controlling Nutritional Status (CONUT) Score and Body Composition, Inflammation and Frailty in Hospitalized Elderly Patients. Nutrients, 16(5), 576. https://doi.org/10.3390/nu16050576