
OptimalMe Program: A Mixed Method Investigation into the Engagement and Acceptability of a Preconception Digital Health Lifestyle Intervention with Individual Coaching for Women’s Health and Behaviour Change




{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methodology
2.1. Intervention Methodologies
2.1.1. Intervention Overview
2.1.2. Delivery and Implementation
2.2. Intervention Components
2.2.1. OptimalMe Digital Platform
2.2.2. Health and Behaviour Assessment for PCC
2.2.3. Educational Resources
2.2.4. Personalised Goal Setting and Progress Monitoring Tool
2.3. Data Collection and Evaluation Methodologies
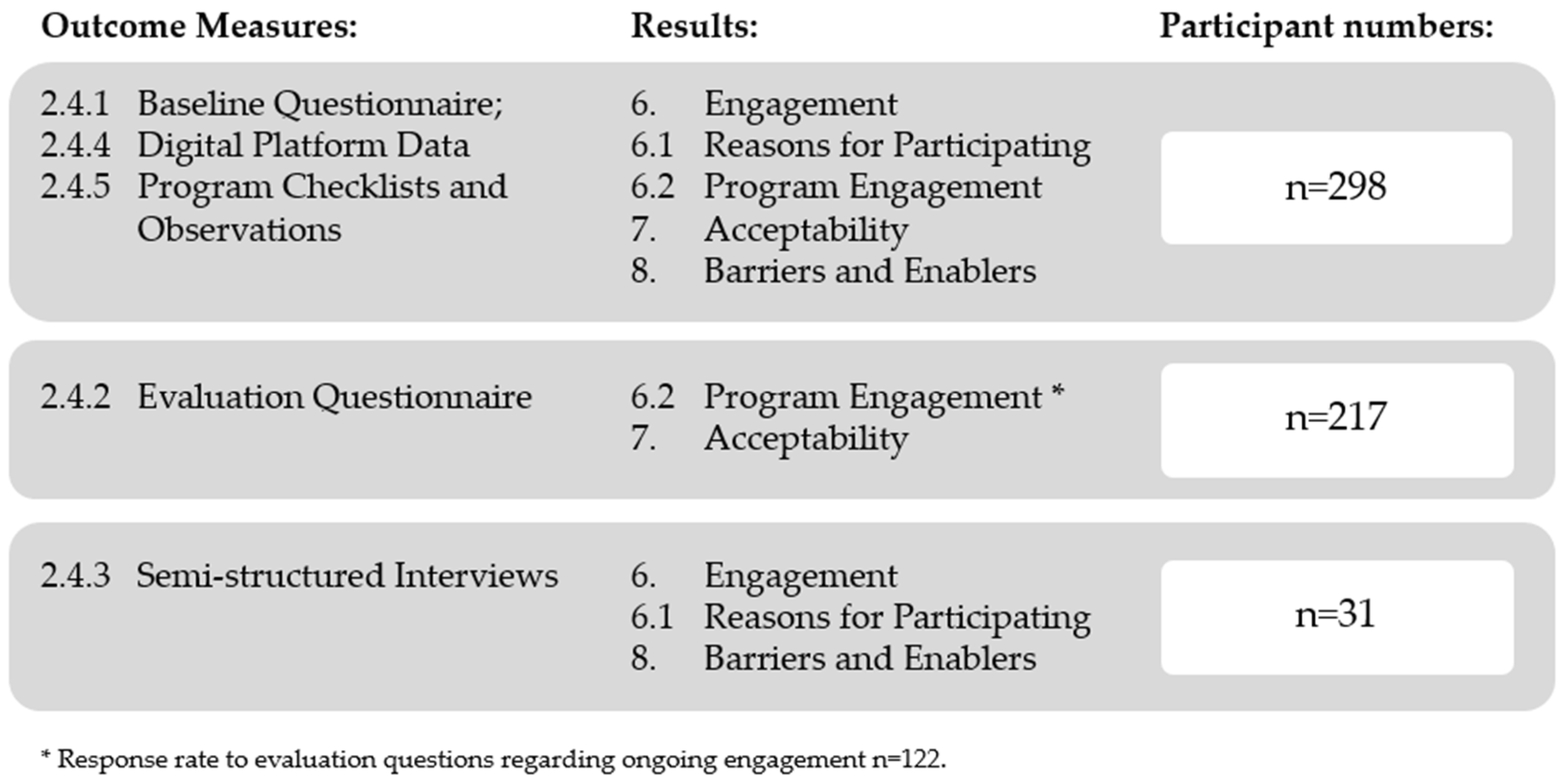
2.4. Outcome Measures
2.4.1. Baseline Questionnaire
2.4.2. Evaluation Questionnaires
2.4.3. Semi-Structured Interviews
2.4.4. Digital Platform Data
2.4.5. Program Checklists and Observations
3. Analyses
3.1. Quantitative
3.2. Qualitative
3.3. Triangulation
4. Ethics
5. Results
6. Engagement
6.1. Reasons for Participating
‘I was … just starting to explore the idea of trying to conceive and I was … thinking it was probably something that I didn’t have a lot of background knowledge in. I’ve had lots of friends who have had kids, so I’ve got their anecdotal information, but I was quite conscious of actually [personally] knowing very little about women’s health’.(OM312, Videoconferencing)
‘I thought it would be a good opportunity to learn something that I had no knowledge on; an area that I didn’t know much about and was just really keen to get as much info as I could on this journey’.(OM085, Telephone)
‘I just wanted to make sure I was the healthiest that I could be before I got pregnant [after the loss of our newborn]’.(OM182, Telephone)
‘I thought it would be a good chance—cos we’re looking at getting pregnant again—to get some healthy habits in place before or while on the journey to having another baby […] I’ve got three other kids’.(OM112, Telephone)
“‘The structure of [the factsheet] was good, because it had those true and false (quiz) questions at the start, where you can test your own knowledge. If I got one wrong, I was quite surprised myself, [and thought]’ okay maybe I can read into this a little bit more, why did I make that choice of that answer?”.(OM013, Videoconferencing)
6.2. Program Engagement
7. Acceptability
8. Barriers and Enablers
‘you’ve got to make sure the goals are achievable and reasonable […] you can so quickly be demotivated if you just don’t feel like you’re getting anywhere with your goals setting. So, I think going through it with someone else and talking strategies and sort of getting a check that each goal is sort of reasonable and achievable is really important’.(OM112, Telephone)
‘on the website, [it wasn’t] the biggest motivator for me; it was more talking to [the coach] and going through those goals, which is basically just a verbal version of that. But to have feedback from another person about what is a realistic goal and what’s not a realistic goal was really useful’.(OM331, Videoconferencing)
‘The first ones that I did were about increasing exercise and water intake. For those, it felt really easy to work out what would my goal be and realistic steps to achieve that goal. But if it was more specific, or a bit more niche, then it would probably be a bit more difficult, so I guess the broad stroke goals that all women would have are pretty easy to do, but some of them are more specific to each person and might be a bit more difficult’.(OM331, Videoconferencing)
‘some way of it popping up [goal reminders]. [Such as] it’s been, however long since you’ve started this goal, how are you finding you’re going, or […] something like that’.(OM227, Telephone)
‘if it was an app, you could have notification or things to say ‘have you checked your goal this week or something?’ Yeah, I don’t know little things like that [would encourage me to keep] logging on and checking in’.(OM182, Telephone)
‘there was probably [room for] improvement, in terms of it prompting you to go to the next section, […] it would be good if there was a bit of a like a workflow that would prompt you to say … instead of asking you to click it, it would almost just appear, so that you keep going [through the education content or tools]’.(OM202, Videoconferencing)
‘[I’d prefer a mobile app] because I don’t have to go on to a website [and] sign in; I just have to click on to an app, probably touch my finger for password protection and then I can just click, rather than get to a computer, go online and do it. Rather than just have something that’s in my pocket that I could be doing while I’m travelling to work’.(OM190, Telephone)
9. Discussion
10. Strengths and Limitations
11. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.A.J.M.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; et al. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Physical Activity; AIHW: Canberra, Australia, 2023. Available online: https://www.aihw.gov.au/reports/physical-activity/physical-activity (accessed on 12 January 2024).
- Australian Institute of Health and Welfare. Diet; AIHW: Canberra, Australia, 2023. Available online: https://www.aihw.gov.au/reports/food-nutrition/diet (accessed on 12 January 2024).
- Australian Institute of Health and Welfare. Overweight and Obesity; AIHW: Canberra, Australia, 2023. Available online: https://www.aihw.gov.au/reports/overweight-obesity/overweight-and-obesity/contents/overweight-and-obesity (accessed on 12 January 2024).
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Dorney, E.; Black, K.I. Preconception care. Aust. J. Gen. Pract. 2018, 47, 424–429. [Google Scholar] [CrossRef]
- Johnson, K.; Posner, S.F.; Biermann, J.; Cordero, J.F.; Atrash, H.K.; Parker, C.S.; Boulet, S.; Curtis, M.G. Recommendations to improve preconception health and Health Care—United States: Report of the CDC/ATSDR preconception care work group and the select panel on preconception care. Morb. Mortal. Wkly. Rep. 2006, 55, 1-CE-4. [Google Scholar]
- Chivers, B.R.; Boyle, J.A.; Lang, A.Y.; Teede, H.J.; Moran, L.J.; Harrison, C.L. Preconception health and lifestyle behaviours of women planning a pregnancy: A cross-sectional study. J. Clin. Med. 2020, 9, 1701. [Google Scholar] [CrossRef]
- Stephenson, J.; Patel, D.; Barrett, G.; Howden, B.; Copas, A.; Ojukwu, O.; Pandya, P.; Shawe, J. How do women prepare for pregnancy? Preconception experiences of women attending antenatal services and views of health professionals. PLoS ONE 2014, 9, e103085. [Google Scholar] [CrossRef]
- Khan, N.N.; Boyle, J.A.; Lang, A.Y.; Harrison, C.L. Preconception health attitudes and behaviours of women: A qualitative investigation. Nutrients 2019, 11, 1490. [Google Scholar] [CrossRef]
- Poels, M.; Koster, M.P.; Boeije, H.R.; Franx, A.; van Stel, H.F. Why do women not use preconception care? A systematic review on barriers and facilitators. Obstet. Gynecol. Surv. 2016, 71, 603–612. [Google Scholar] [CrossRef]
- Goossens, J.; De Roose, M.; Van Hecke, A.; Goemaes, R.; Verhaeghe, S.; Beeckman, D. Barriers and facilitators to the provision of preconception care by healthcare providers: A systematic review. Int. J. Nurs. Stud. 2018, 87, 113–130. [Google Scholar] [CrossRef]
- Nwolise, C.H.; Carey, N.; Shawe, J. Preconception care education for women with diabetes: A systematic review of conventional and digital health interventions. J. Med. Internet Res. 2016, 18, e5615. [Google Scholar] [CrossRef]
- Carter, J.; Sandall, J.; Shennan, A.H.; Tribe, R.M. Mobile phone apps for clinical decision support in pregnancy: A scoping review. BMC Med Inform. Decis. Mak. 2019, 19, 219. [Google Scholar] [CrossRef]
- Rhodes, A.; Smith, A.D.; Chadwick, P.; Croker, H.; Llewellyn, C.H. Exclusively digital health interventions targeting diet, physical activity, and weight gain in pregnant women: Systematic review and meta-analysis. JMIR Mhealth Uhealth 2020, 8, e18255. [Google Scholar] [CrossRef]
- Lee, M.; Lee, H.; Kim, Y.; Kim, J.; Cho, M.; Jang, J.; Jang, H. Mobile app-based health promotion programs: A systematic review of the literature. Int. J. Environ. Res. Public Health 2018, 15, 2838. [Google Scholar] [CrossRef]
- Kim, S.J.; Marsch, L.A.; Brunette, M.F.; Dallery, J. Harnessing Facebook for smoking reduction and cessation interventions: Facebook user engagement and social support predict smoking reduction. J. Med. Internet Res. 2017, 19, e168. [Google Scholar] [CrossRef]
- Gough, A.; Hunter, R.F.; Ajao, O.; Jurek, A.; McKeown, G.; Hong, J.; Barrett, E.; Ferguson, M.; McElwee, G.; McCarthy, M. Tweet for behavior change: Using social media for the dissemination of public health messages. JMIR Public Health Surveill. 2017, 3, e6313. [Google Scholar] [CrossRef]
- Roberts, A.L.; Fisher, A.; Smith, L.; Heinrich, M.; Potts, H.W. Digital health behaviour change interventions targeting physical activity and diet in cancer survivors: A systematic review and meta-analysis. J. Cancer Surviv. 2017, 11, 704–719. [Google Scholar] [CrossRef]
- Harrison, C.L.; Brammall, B.R.; Garad, R.; Teede, H. OptimalMe Intervention for Healthy Preconception, Pregnancy, and Postpartum Lifestyles: Protocol for a Randomized Controlled Implementation Effectiveness Feasibility Trial. JMIR Res. Protoc. 2022, 11, e33625. [Google Scholar] [CrossRef]
- Markland, D.; Ryan, R.M.; Tobin, V.J.; Rollnick, S. Motivational interviewing and self–determination theory. J. Soc. Clin. Psychol. 2005, 24, 811–831. [Google Scholar] [CrossRef]
- Brammall, B.R.; Garad, R.M.; Teede, H.J.; Harrison, C.L. Evaluating Preconception Health and Behaviour Change in Australian Women Planning a Pregnancy: The OptimalMe Program, a Digital Healthy Lifestyle Intervention with Remotely Delivered Coaching. Nutrients 2024, 16, 155. [Google Scholar] [CrossRef]
- Australian Dietary Guidelines Summary; National Health and Medical Research Council: Canberra, Australia, 2013.
- Department of Health and Aged Care Physical Activity and Exercise Guidelines for All Australians. For Adults (18 to 64 Years) 2021. Available online: https://www.health.gov.au/topics/physical-activity-and-exercise/physical-activity-and-exercise-guidelines-for-all-australians/for-adults-18-to-64-years (accessed on 12 January 2024).
- Bailey, R.R. Goal setting and action planning for health behavior change. Am. J. Lifestyle Med. 2019, 13, 615–618. [Google Scholar] [CrossRef]
- A Healthy Lifestyle—WHO Recommendations; World Health Organization: Geneva, Switzerland. 2010. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 15 January 2024).
- Kozica, S.; Lombard, C.B.; Ilic, D.; Ng, S.; Harrison, C.L.; Teede, H.J. Acceptability of delivery modes for lifestyle advice in a large scale randomised controlled obesity prevention trial. BMC Public Health 2015, 15, 699. [Google Scholar] [CrossRef]
- Strauss, A.; Corbin, J. Basics of Qualitative Research; Sage Publications: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- Beasley, T.M.; Schumacker, R.E. Multiple regression approach to analyzing contingency tables: Post hoc and planned comparison procedures. J. Exp. Educ. 1995, 64, 79–93. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- O’Cathain, A.; Murphy, E.; Nicholl, J. Three techniques for integrating data in mixed methods studies. BMJ 2010, 341, c4587. [Google Scholar] [CrossRef]
- Yardley, L.; Spring, B.J.; Riper, H.; Morrison, L.G.; Crane, D.H.; Curtis, K.; Merchant, G.C.; Naughton, F.; Blandford, A. Understanding and promoting effective engagement with digital behavior change interventions. Am. J. Prev. Med. 2016, 51, 833–842. [Google Scholar] [CrossRef]
- Couper, M.P.; Alexander, G.L.; Zhang, N.; Little, R.J.; Maddy, N.; Nowak, A.M.; McClure, J.B.; Calvi, J.J.; Rolnick, S.J.; Stopponi, A.M.; et al. Engagement and retention: Measuring breadth and depth of participant use of an online intervention. J. Med. Internet Res. 2010, 12, e1430. [Google Scholar] [CrossRef]
- Hommel, K.A.; Hente, E.; Herzer, M.; Ingerski, L.M.; Denson, L.A. Telehealth behavioral treatment for medication nonadherence: A pilot and feasibility study. Eur. J. Gastroenterol. Hepatol. 2013, 25, 469. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef]
- Chung, J.; Gardner, H.J. Temporal presence variation in immersive computer games. Int. J. Hum. Comput. Interact. 2012, 28, 511–529. [Google Scholar] [CrossRef]
- Michie, S.; Yardley, L.; West, R.; Patrick, K.; Greaves, F. Developing and evaluating digital interventions to promote behavior change in health and health care: Recommendations resulting from an international workshop. J. Med. Internet Res. 2017, 19, e232. [Google Scholar] [CrossRef]
- McGuire, A.M.; Seib, C.; Porter-Steele, J.; Anderson, D.J. The association between Web-based or face-to-face lifestyle interventions on the perceived benefits and barriers to exercise in midlife women: Three-Arm Equivalency Study. J. Med. Internet Res. 2019, 21, e10963. [Google Scholar] [CrossRef] [PubMed]
- Silberman, J.M.; Kaur, M.; Sletteland, J.; Venkatesan, A. Outcomes in a digital weight management intervention with one-on-one health coaching. PLoS ONE 2020, 15, e0232221. [Google Scholar] [CrossRef] [PubMed]
- Brammall, B.R.; Garad, R.M.; Boyle, A.J.; Hayman, M.J.; de Jersey, S.J.; Teede, H.J.; Hong, Q.V.; Carrandi, A.; Harrison, C.L. Assessing the Content and Quality of Digital Tools for Managing Gestational Weight Gain: Systematic Search and Evaluation. J. Med. Internet Res. 2022, 24, e37552. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brammall, B.R.; Garad, R.M.; Teede, H.J.; Baker, S.E.; Harrison, C.L. OptimalMe Program: A Mixed Method Investigation into the Engagement and Acceptability of a Preconception Digital Health Lifestyle Intervention with Individual Coaching for Women’s Health and Behaviour Change. Nutrients 2024, 16, 572. https://doi.org/10.3390/nu16050572
Brammall BR, Garad RM, Teede HJ, Baker SE, Harrison CL. OptimalMe Program: A Mixed Method Investigation into the Engagement and Acceptability of a Preconception Digital Health Lifestyle Intervention with Individual Coaching for Women’s Health and Behaviour Change. Nutrients. 2024; 16(5):572. https://doi.org/10.3390/nu16050572
Chicago/Turabian StyleBrammall, Bonnie R., Rhonda M. Garad, Helena J. Teede, Susanne E. Baker, and Cheryce L. Harrison. 2024. "OptimalMe Program: A Mixed Method Investigation into the Engagement and Acceptability of a Preconception Digital Health Lifestyle Intervention with Individual Coaching for Women’s Health and Behaviour Change" Nutrients 16, no. 5: 572. https://doi.org/10.3390/nu16050572
APA StyleBrammall, B. R., Garad, R. M., Teede, H. J., Baker, S. E., & Harrison, C. L. (2024). OptimalMe Program: A Mixed Method Investigation into the Engagement and Acceptability of a Preconception Digital Health Lifestyle Intervention with Individual Coaching for Women’s Health and Behaviour Change. Nutrients, 16(5), 572. https://doi.org/10.3390/nu16050572