
Superior Mesenteric Artery Syndrome in Anorexia Nervosa: A Case Report and a Systematic Revision of the Literature

 ,
,
Abstract
1. Introduction
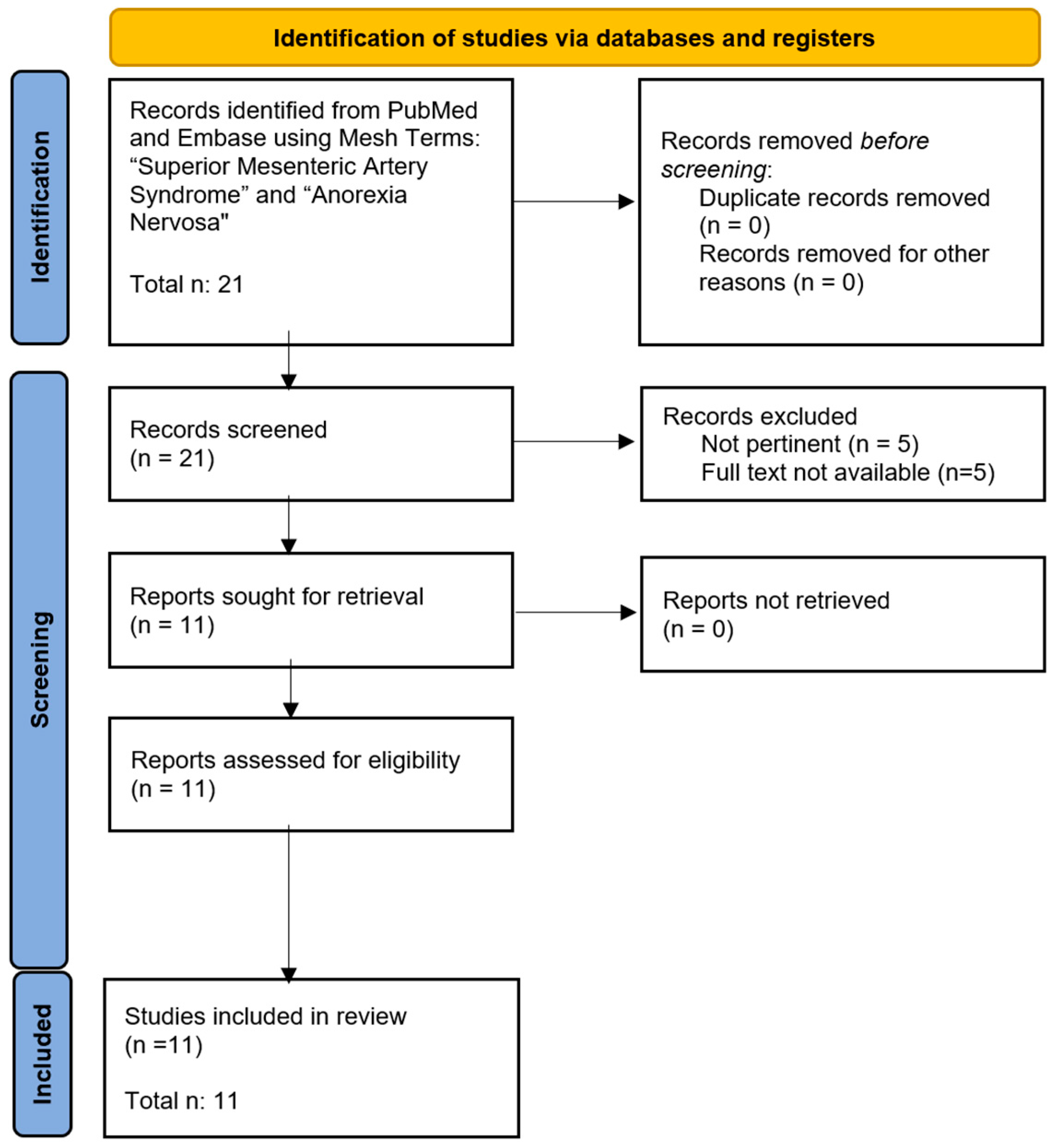
2. Materials and Methods
- Full-length articles or reviews of children and adolescents up to 18 years old.
- Full description of the clinical case/cases.
- Not pertinent to the field of study.
- Involving adults (>18 years).
- Not presenting a clinical description of the patient.
3. Results
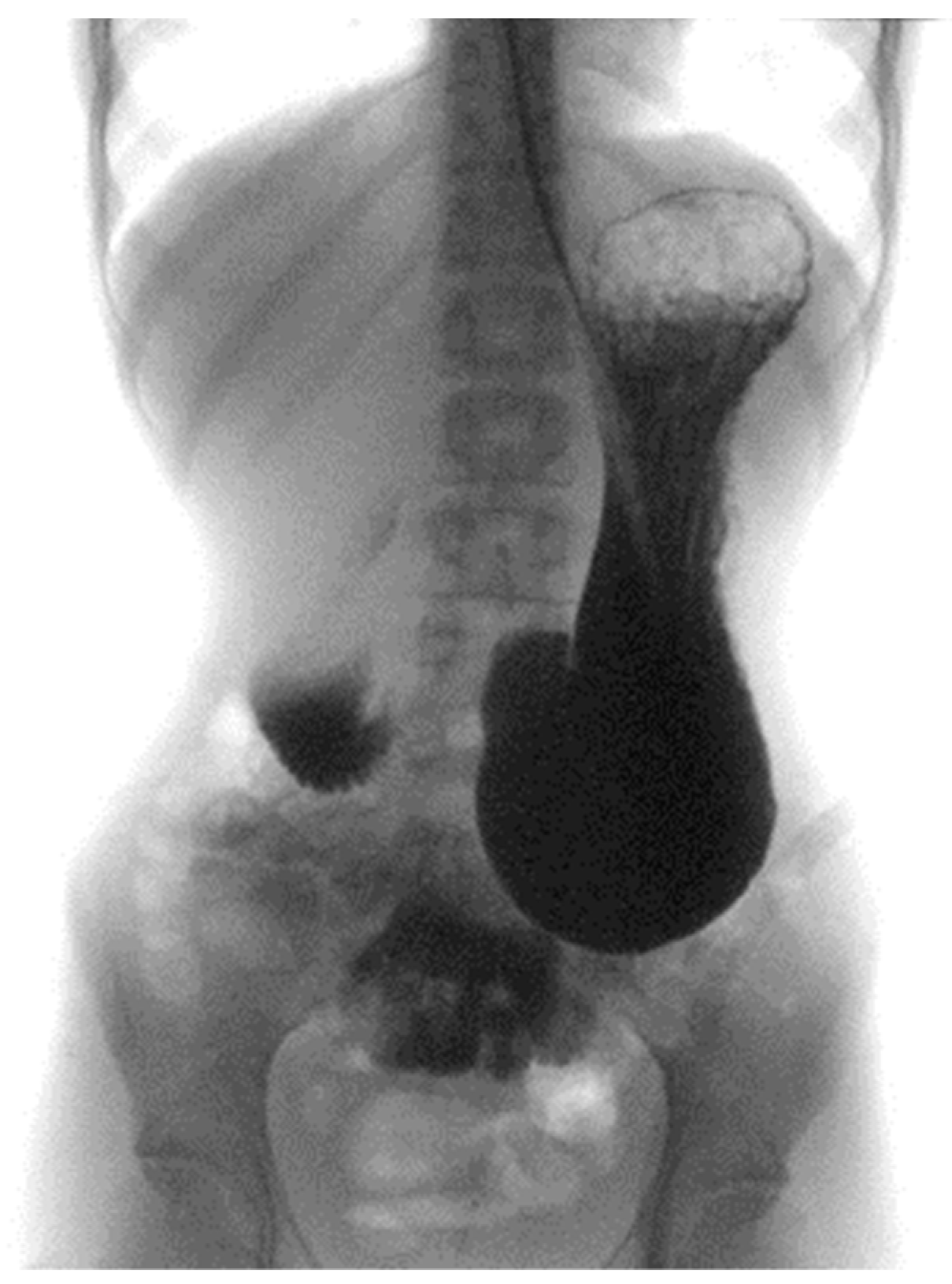
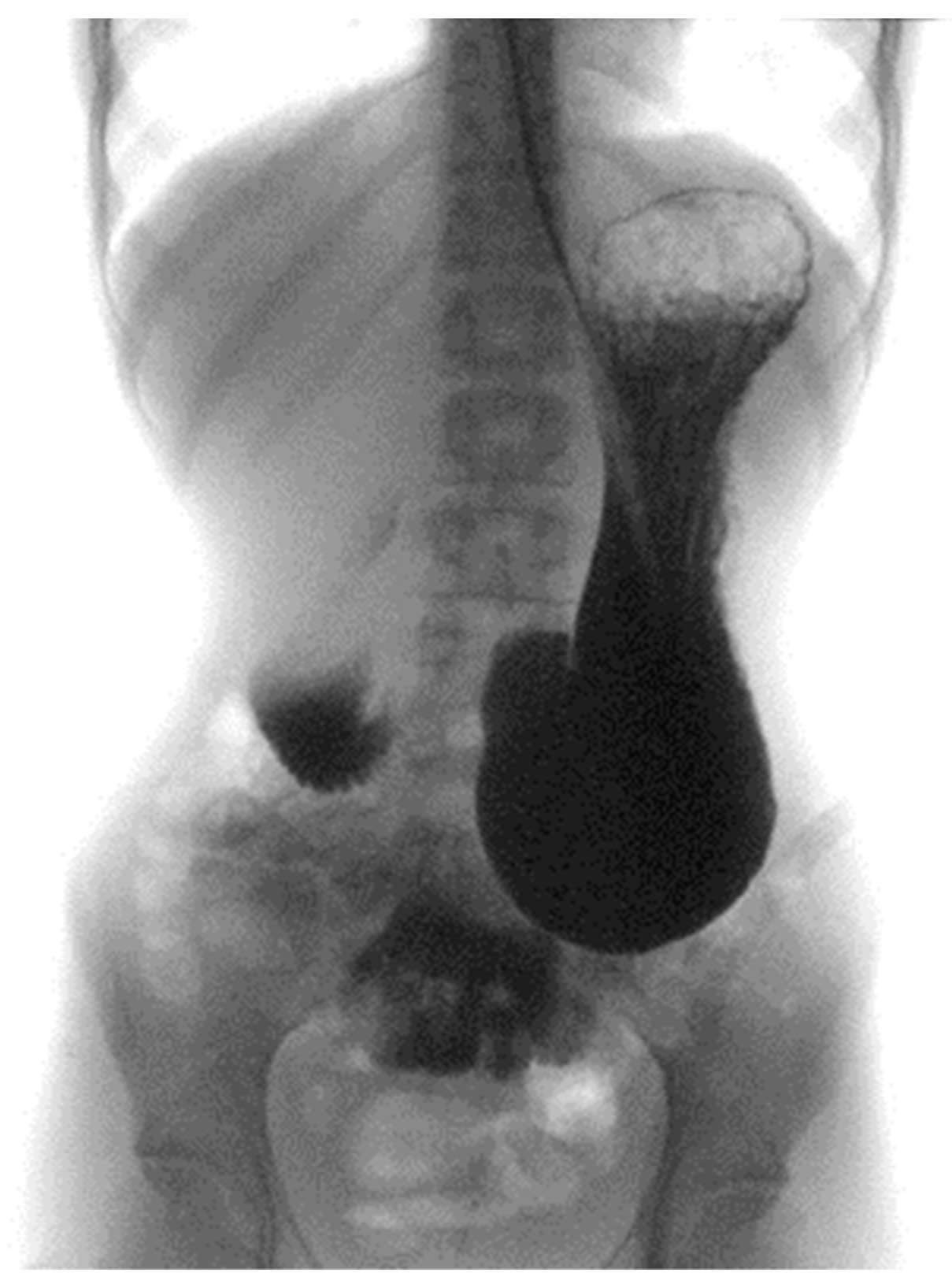
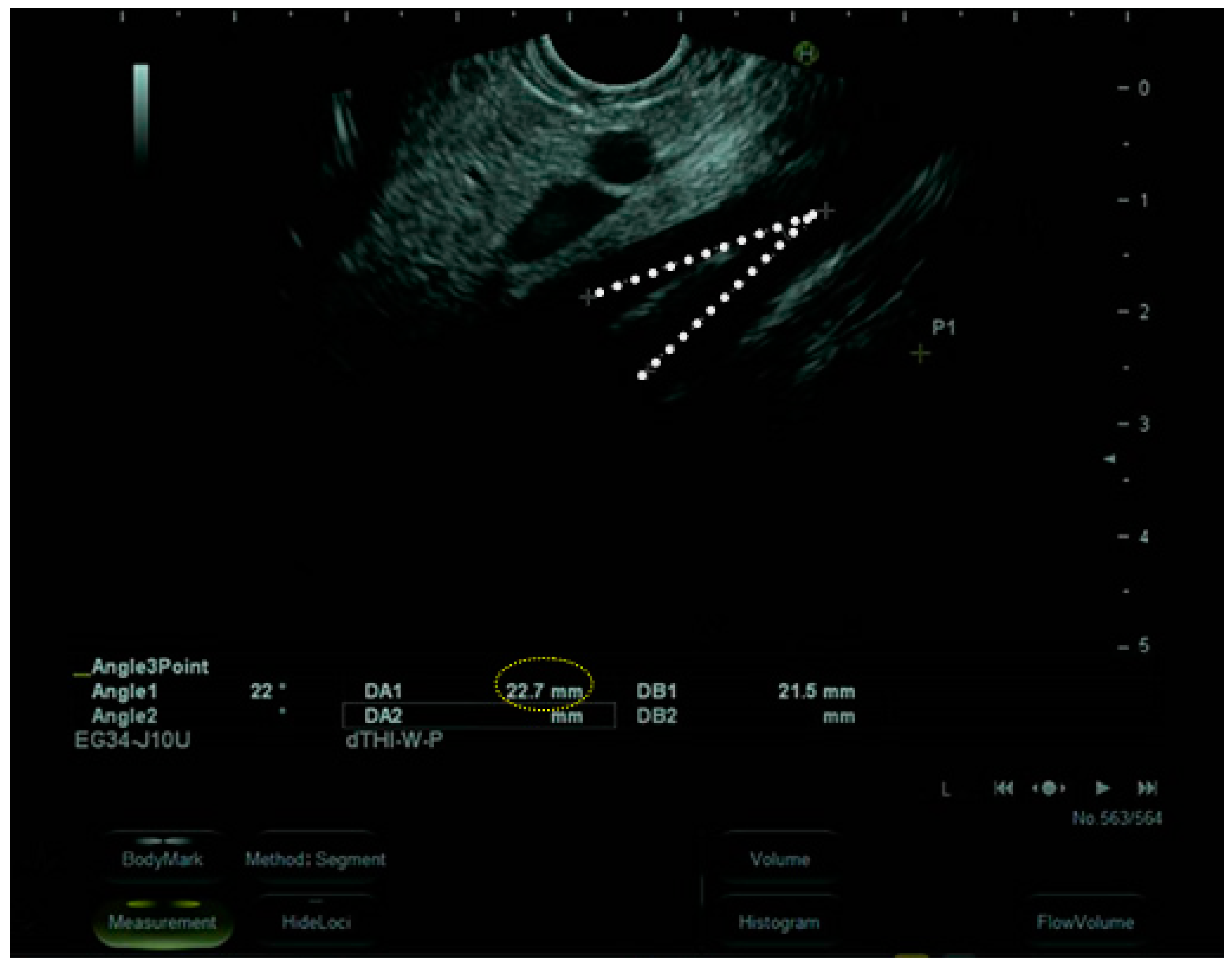
3.1. Case Report
3.2. Literature Review
3.2.1. Patient Demography
3.2.2. Complications
3.2.3. Treatment
3.2.4. Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hines, J.R.; Gore, R.M.; Ballantyne, G.H. Superior mesenteric artery syndrome. Diagnostic criteria and therapeutic approaches. Am. J. Surg. 1984, 148, 630–632. [Google Scholar] [CrossRef] [PubMed]
- Wayne, E.R.; Burrington, J.D. Duodenal obstruction by the superior mesenteric artery in children. Surgery 1972, 72, 762–768. [Google Scholar] [PubMed]
- Neri, S.; Signorelli, S.S.; Mondati, E.; Pulvirenti, D.; Campanile, E.; Di Pino, L.; Scuderi, M.; Giustolisi, N.; Di Prima, P.; Mauceri, B.; et al. Ultrasound imaging in the diagnosis of superior mesenteric artery syndrome. J. Intern. Med. 2005, 257, 346–351. [Google Scholar] [CrossRef]
- Trovato, C.M.; Capriati, T.; Bolasco, G.; Campana, C.; Papa, V.; Mazzoli, B.; Zanna, V.; Marchili, M.R.; Basso, M.S.; Maggiore, G.; et al. Five-Year Inpatient Management of Teenagers with Anorexia Nervosa: Focus on Nutritional Issues. J. Pediatr. Gastroenterol. Nutr. 2022, 74, 674–680. [Google Scholar] [CrossRef]
- Osegueda de Rodríguez, E.J.; Hernández-Villegas, A.C.; Serralde-Zúñiga, A.E.; Reyes-Ramírez, A.L.D.C. The two sides of superior mesenteric artery syndrome treatment: Conservative or surgical management? Nutr. Hosp. 2017, 34, 997–1000. [Google Scholar] [PubMed]
- Gwee, K.; Teh, A.; Huang, C. Acute superior mesenteric artery syndrome and pancreatitis in anorexia nervosa. Australas. Psychiatry Bull. R. Aust. New Zealand Coll. Psychiatr. 2010, 18, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Bloomberg, L.; Hoscheit, M.; Hendler, S.; Abegunde, A.T. Superior Mesenteric Artery Syndrome in an Adolescent Female with Anorexia Nervosa. Clin. Med. Res. 2010, 21, 46–48. [Google Scholar] [CrossRef]
- Elbadaway, M.H. Chronic superior mesenteric artery syndrome in anorexia nervosa. Br. J. Psychiatry 1992, 160, 552–554. [Google Scholar] [CrossRef]
- Sours, J.A.; Vorhaus, L.J. Superior mesenteric artery syndrome in anorexia nervosa: A case report. Am. J. Psychiatry 1981, 138, 519–520. [Google Scholar]
- Lee, C.W.; Park, M.I.; Park, S.J.; Moon, W.; Kim, H.H.; Kim, B.J.; Shim, I.K.; Park, S.S. A case of superior mesenteric artery syndrome caused by anorexia nervosa. Korean J. Gastroenterol. 2011, 58, 280–283. [Google Scholar] [CrossRef]
- Froese, A.P.; Szmuilowicz, J.; Bailey, J.D. The superior-mesenteric-artery syndrome: Cause or complication of anorexia nervosa? Can. Psychiatr. Assoc. J. 1978, 23, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Stheneur, C.; Rey, C.; Pariente, D.; Alvin, P. Dilatation aiguë de l’estomac avec pince mésentérique chez une jeune fille anorexique [Acute gastric dilatation with superior mesenteric artery syndrome in a young girl with anorexia nervosa]. Arch. Pediatr. Organe Off. Soc. Fr. Pediatr. 1995, 2, 973–976. [Google Scholar]
- Kim, T.; Kim, H.U.; Song, H.J. A case of gastric emphysema in anorexia nervosa presenting as acute gastric distension. Korean J. Gastroenterol. 2012, 60, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Verhoef, P.A.; Rampal, A. Unique challenges for appropriate management of a 16-year-old girl with superior mesenteric artery syndrome as a result of anorexia nervosa: A case report. J. Med. Case Rep. 2009, 3, 127. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, Y.; Kitamura, Y.; Wada, N.; Okinaga, K. Nihon Shokakibyo Gakkai zasshi. Jpn. J. Gastro-Enterol. 1985, 82, 2829–2833. [Google Scholar]
- Khan, H.; Al-Jabbari, E.; Shroff, N.; Barghash, M.; Shestopalov, A.; Bhargava, P. Coexistence of superior mesenteric artery syndrome and Nutcracker phenomenon. Radiol. Case Rep. 2022, 17, 1927–1930. [Google Scholar] [CrossRef] [PubMed]
- Diab, S.; Hayek, F. Combined Superior Mesenteric Artery Syndrome and Nutcracker Syndrome in a Young Patient: A Case Report and Review of the Literature. Am. J. Case Rep. 2020, 21, e922619. [Google Scholar] [CrossRef]
- Heidbreder, R. Co-occurring superior mesenteric artery syndrome and nutcracker syndrome requiring Roux-en-Y duodenojejunostomy and left renal vein transposition: A case report and review of the literature. J. Med. Case Rep. 2018, 12, 214. [Google Scholar] [CrossRef]
- Biank, V.; Werlin, S. Superior mesenteric artery syndrome in children: A 20-year experience. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 522–525. [Google Scholar] [CrossRef]
- Van Horne, N.; Jackson, J.P. Superior mesenteric artery syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Lee, T.H.; Lee, J.S.; Jo, Y.; Park, K.S.; Cheon, J.H.; Kim, Y.S.; Jang, J.Y.; Kang, Y.W. Superior mesenteric artery syndrome: Where do we stand today? J. Gastrointest. Surg. 2012, 16, 2203–2211. [Google Scholar] [CrossRef]
- Hall, N.Y.; Hetti Pathirannahalage, D.M.; Mihalopoulos, C.; Austin, S.B.; Le, L. Global Prevalence of Adolescent Use of Nonprescription Weight-Loss Products: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2024, 7, e2350940. [Google Scholar] [CrossRef] [PubMed]
- Neale, J.; Hudson, L.D. Anorexia nervosa in adolescents. Br. J. Hosp. Med. 2020, 81, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Jordaan, G.P.; Muller, A.; Greeff, M.; Stein, D.J. Eating disorder and superior mesenteric artery syndrome. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 1211. [Google Scholar] [CrossRef] [PubMed]
- Kornmehl, P.; Weizman, Z.; Liss, Z.; Bar-Ziv, J.; Joseph, A. Superior mesenteric artery syndrome presenting as an anorexia nervosa-like illness. J. Adolesc. Health Care Off. Publ. Soc. Adolesc. Med. 1988, 9, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.A.; Smith, M.S. Anorexia in a 14-year-old girl: Why won’t she eat? J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2006, 39, 936–938. [Google Scholar] [CrossRef] [PubMed]
- Civan, H.A.; Gülcü, D.; Erkan, T.; Çokuğraş, F.Ç.; Kutlu, T. Wilkie’s syndrome admitted for acute abdomen: A case presentation. Turk Pediatri Ars. 2018, 53, 193–196. [Google Scholar] [CrossRef]
- Frongia, G.; Schenk, J.P.; Schaible, A.; Sauer, P.; Mehrabi, A.; Günther, P. Food fear, quick satiety and vomiting in a 16 years old girl: It’s bulimia, or maybe not…? A case report of Wilkie’s syndrome (superior mesenteric artery syndrome). Int. J. Surg. Case Rep. 2019, 65, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Rehman, A.; Shah, J.; Naeem, A.; Naim, F. Wasting away–superior mesenteric artery syndrome in a young girl–a case report. J. Postgrad. Med. Inst. 2022, 36, 266–268. [Google Scholar]
- Peeters, E. Minimal Invasive Treatment of Wilkie’s Syndrome. J. Pediatr. Gastroenterol. Nutr. 2023, 76 (Suppl. S1), 1188. [Google Scholar]
- Rao, H.R.; Barron, M.A.; Biswas, A.; Branson, H.M.; Mitton, G.D.; Naqvi, A. Malnutrition in a child with T-cell ALL leading to superior mesenteric artery syndrome and Wernicke’s encephalopathy. Pediatr. Blood Cancer 2022, 69, e29651. [Google Scholar] [CrossRef]
- Raff, L.; Cole, E.; Phillips, L.; Raff, E. Food Insecurity Leading to Superior Mesenteric Artery Syndrome Managed Successfully with Endoscopic Gastrojejunostomy Stent. Am. J. Case Rep. 2023, 24, e939420. [Google Scholar] [CrossRef]
- Okamoto, T.; Sato, T.; Sasaki, Y. Superior mesenteric artery syndrome in a healthy active adolescent. BMJ Case Rep. 2019, 12, e228758. [Google Scholar] [CrossRef] [PubMed]
- Kogawa, K.; Kusama, Y. Superior mesenteric artery syndrome in a healthy adolescent. BMJ Case Rep. 2017, 2017, bcr2017220609. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Nagraj, S.; Chaube, R. Renal tubular acidosis and superior mesenteric artery syndrome. BMJ Case Rep. 2010, 2010, bcr0420091792. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.; Choudhary, A. Severe malnutrition causing superior mesenteric artery syndrome in an adolescent with Triple A syndrome. J. Pediatr. Endocrinol. Metab. JPEM 2016, 29, 1221–1224. [Google Scholar] [CrossRef] [PubMed]
- Bakker, M.E.; van Delft, R.; Vaessens, N.A.; Rosias, P.R. Superior mesenteric artery syndrome in a 15-year-old boy during Ramadan. Eur. J. Pediatr. 2014, 173, 1619–1621. [Google Scholar] [CrossRef] [PubMed]
- Yazdani, S.; Bloomberg, Z.; Klauber, R.; Meresh, E. Avoidant restrictive food intake disorder emerging during COVID-19 pandemic resulting in superior mesenteric artery syndrome. Eat. Weight. Disord. EWD 2022, 27, 2943–2945. [Google Scholar] [CrossRef]
- Riera, D.C.; Phalen, J.A. Superior mesenteric artery syndrome in a patient with autism spectrum disorder: Case report and review of the literature. J. Autism Dev. Disord. 2013, 43, 244–246. [Google Scholar] [CrossRef]
- Geskey, J.M.; Erdman, H.J.; Bramley, H.P.; Williams, R.J.; Shaffer, M.L. Superior mesenteric artery syndrome in intellectually disabled children. Pediatr. Emerg. Care 2012, 28, 351–353. [Google Scholar] [CrossRef]
- Russell, E.A.; Braverman, R.M.; Vasudevan, S.A.; Patel, B. A Traumatic Quinceañera: Acute Superior Mesenteric Artery Syndrome in an Adolescent Girl. Pediatr. Emerg. Care 2021, 37, e203–e205. [Google Scholar] [CrossRef]
- Welsch, T.; Büchler, M.W.; Kienle, P. Recalling superior mesenteric artery syndrome. Dig. Surg. 2007, 24, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Mangla, J.C. Superior mesenteric artery compression syndrome. Am. J. Gastroenterol. 1978, 70, 141. [Google Scholar] [PubMed]
- Lippl, F.; Hannig, C.; Weiss, W.; Allescher, H.D.; Classen, M.; Kurjak, M. Superior mesenteric artery syndrome: Diagnosis and treatment from the gastroenterologist’s view. J. Gastroenterol. 2002, 37, 640–643. [Google Scholar] [CrossRef] [PubMed]
- Merrett, N.D.; Wilson, R.B.; Cosman, P.; Biankin, A.V. Superior mesenteric artery syndrome: Diagnosis and treatment strategies. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2009, 13, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Raman, S.P.; Neyman, E.G.; Horton, K.M.; Eckhauser, F.E.; Fishman, E.K. Superior mesenteric artery syndrome: Spectrum of CT findings with multiplanar reconstructions and 3-D imaging. Abdom. Imaging 2012, 37, 1079–1088. [Google Scholar] [CrossRef] [PubMed]
- Unal, B.; Aktaş, A.; Kemal, G.; Bilgili, Y.; Güliter, S.; Daphan, C.; Aydinuraz, K. Superior mesenteric artery syndrome: CT and ultrasonography findings. Diagn. Interv. Radiol. 2005, 11, 90–95. [Google Scholar] [PubMed]
- Chan, D.K.; Mak, K.S.; Cheah, Y.L. Successful nutritional therapy for superior mesenteric artery syndrome. Singap. Med. J. 2012, 53, e233–e236. [Google Scholar]
- Oka, A.; Awoniyi, M.; Hasegawa, N.; Yoshida, Y.; Tobita, H.; Ishimura, N.; Ishihara, S. Superior mesenteric artery syndrome: Diagnosis and management. World J. Clin. Cases 2023, 11, 3369–3384. [Google Scholar] [CrossRef]
- Yakan, S.; Calıskan, C.; Kaplan, H.; Deneclı, A.G.; Coker, A. Superior mesenteric artery syndrome: A rare cause of intestinal obstruction. Diagnosis and surgical management. Indian J. Surg. 2013, 75, 106–110. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Sex | Age (Years) | Weight Loss (kg) | BMI (kg/m2) | Comorbidities | Complications | Medical Treatment | Surgical Treatment |
|---|---|---|---|---|---|---|---|---|
| Case index | F | 13 | 20 | 12.2 | AN Sexual abuse | Acute gastric dilatation | NGT PN NJT | No |
| 1 (Bloomberg L et al.) [7] | F | 18 | 6.8 | 15.5 | AN | No | NGT PN | No |
| 2 (Gwee K et al.) [6] | F | 17 | 10 | 16.4 | AN | Pancreatitis | NGT NJT | No |
| 3 (Osegueda de Rodríguez EJ et al.) [5] | F | 17 | 22.5 | 8.3 | AN | Nutcracker syndrome, Gastro duodenal expansion | NGT PN NJT | Division of the ligament of Treitz and left renal vein. Partial gastrectomy. Duodenal and jejunal anastomosis |
| 4 (Elbadaway MH et al.) [8] | F | 18 | Unknown | 12.7 | AN | No | Unknown | Gastrojejunostomy |
| 5 (Sours JA et al.) [9] | F | 17 | 35 | Unknown | AN | No | NGT PN | No |
| 6 (Lee Cw et al.) [10] | F | 15 | 4 | 16.4 | AN | No | PN | No |
| 7 (Froese AP et al.) [11] | M | 16 | Unknown | Unknown | AN | No | Conservative (not specified) | No |
| 8 (Stheneur C et al.) [12] | F | 14 | 17 | 14.4 | AN | Acute gastric dilatation | NGT PN | No |
| 9 (Miyazawa Y et al.) [15] | F | 17 | 16 | 13.8 | AN | No | NGT | Duodenal anterior replacement |
| 10 (Kim T et al.) [13] | F | 17 | 9.2 | 11.9 | AN | Gastric Emphysema | NGT NJT PN | No |
| 11 (Verhoef PA et al.) [14] | F | 16 | 22 | 15 | AN | No | NGT NJT | No |
| Reference | Acute or Chronic Presentation | Symptoms | Time from Weight Loss Onset and Hospitalization | Radiologic Methods Used in the Diagnosis | ||||
| Case index | Acute | Weight loss, Vomiting | 5 months | Upper gastrointestinal endoscopy | ||||
| 1 (Bloomberg L et al.) [7] | Acute | Weight loss, Abdominal pain, Abdominal distension, Nausea, Vomiting | 3 months | Contrast-enhanced abdominal CT | ||||
| 2 (Gwee K et al.) [6] | Acute | Weight loss, Vomiting, Abdominal distension, Abdominal pain | 1 year | Contrast-enhanced abdominal CT | ||||
| 3 (Osegueda de Rodríguez EJ et al.) [5] | Acute | Weight loss | 1 year | Contrast-enhanced abdominal CT | ||||
| 4 (Elbadaway MH et al.) [8] | Chronic | Weight loss, Heartburn, Abdominal pain, Post-prandial vomiting | 4 years | X-ray fluoroscopy | ||||
| 5 (Sours JA et al.) [9] | Chronic | Weight loss, Nausea, Post-prandial vomiting, Abdominal distension | 6 months | X-ray | ||||
| 6 (Lee Cw et al.) [10] | Chronic | Weight loss, Abdominal pain, Abdominal distension | 2 months | Contrast-enhanced abdominal CT | ||||
| 7 (Froese AP et al.) [11] | Acute | Weight loss, Nausea, Vomiting | 13 months | X-ray | ||||
| 8 (Stheneur C et al.) [12] | Chronic | Weight loss, Nausea, Post-prandial vomiting, Abdominal pain, Abdominal distension | 6 months | X-ray | ||||
| 9 (Miyazawa Y et al.) [15] | Acute | Weight loss, Recurrent vomiting, Abdominal pain | 18 months | Ultrasonography Arteriography Endoscopy | ||||
| 10 (Kim T et al.) [13] | Chronic | Weight loss, Nausea, Post-prandial vomiting | 2 years | Contrast-enhanced abdominal CT | ||||
| 11 (Verhoef PA et al.) [14] | Chronic | Weight loss, Nausea, Abdominal pain, Vomiting | 16 months | Contrast-enhanced abdominal CT | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bozzola, E.; Irrera, M.; Cirillo, F.; Zanna, V.; Petrelli, I.; Diamanti, A.; Scire, Y.; Park, J.; Marchesi, A.; Marchili, M.R.; et al. Superior Mesenteric Artery Syndrome in Anorexia Nervosa: A Case Report and a Systematic Revision of the Literature. Nutrients 2024, 16, 541. https://doi.org/10.3390/nu16040541
Bozzola E, Irrera M, Cirillo F, Zanna V, Petrelli I, Diamanti A, Scire Y, Park J, Marchesi A, Marchili MR, et al. Superior Mesenteric Artery Syndrome in Anorexia Nervosa: A Case Report and a Systematic Revision of the Literature. Nutrients. 2024; 16(4):541. https://doi.org/10.3390/nu16040541
Chicago/Turabian StyleBozzola, Elena, Mariangela Irrera, Flavia Cirillo, Valeria Zanna, Italo Petrelli, Antonella Diamanti, Ylenia Scire, Jibin Park, Alessandra Marchesi, Maria Rosaria Marchili, and et al. 2024. "Superior Mesenteric Artery Syndrome in Anorexia Nervosa: A Case Report and a Systematic Revision of the Literature" Nutrients 16, no. 4: 541. https://doi.org/10.3390/nu16040541
APA StyleBozzola, E., Irrera, M., Cirillo, F., Zanna, V., Petrelli, I., Diamanti, A., Scire, Y., Park, J., Marchesi, A., Marchili, M. R., & Villani, A. (2024). Superior Mesenteric Artery Syndrome in Anorexia Nervosa: A Case Report and a Systematic Revision of the Literature. Nutrients, 16(4), 541. https://doi.org/10.3390/nu16040541