
Efficacy of Lactiplantibacillus plantarum PBS067, Bifidobacterium animalis subsp. lactis BL050, and Lacticaseibacillus rhamnosus LRH020 in the Amelioration of Vaginal Microbiota in Post-Menopausal Women: A Prospective Observational Clinical Trial

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
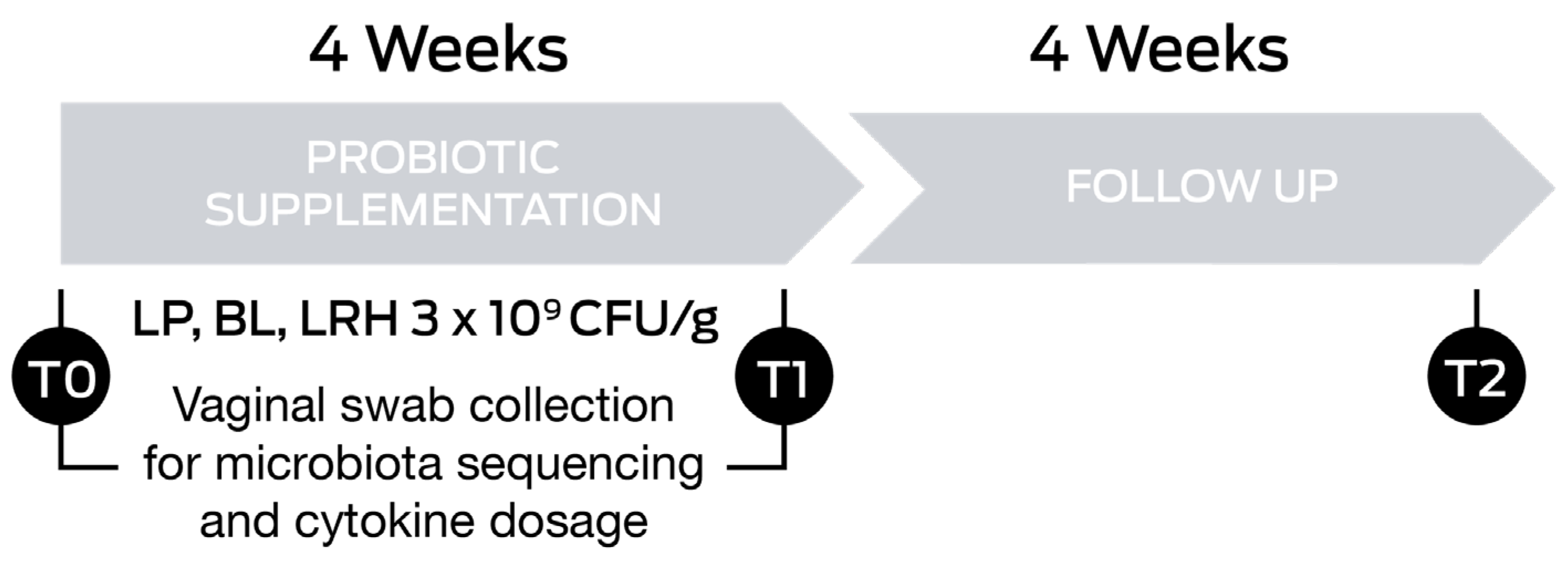
2.1. Study Design
2.2. Intervention
2.3. Endpoints and Outcomes
2.4. Next Generation Sequencing
2.4.1. DNA Extraction and Purification
2.4.2. Determination of Bacterial Profiles by Amplicon Sequencing
2.4.3. Data Processing and Analysis
2.5. Vaginal Health Index
2.6. Cytokine Concentrations
2.7. Statistical Analysis
NGS Statistical Analysis
3. Results
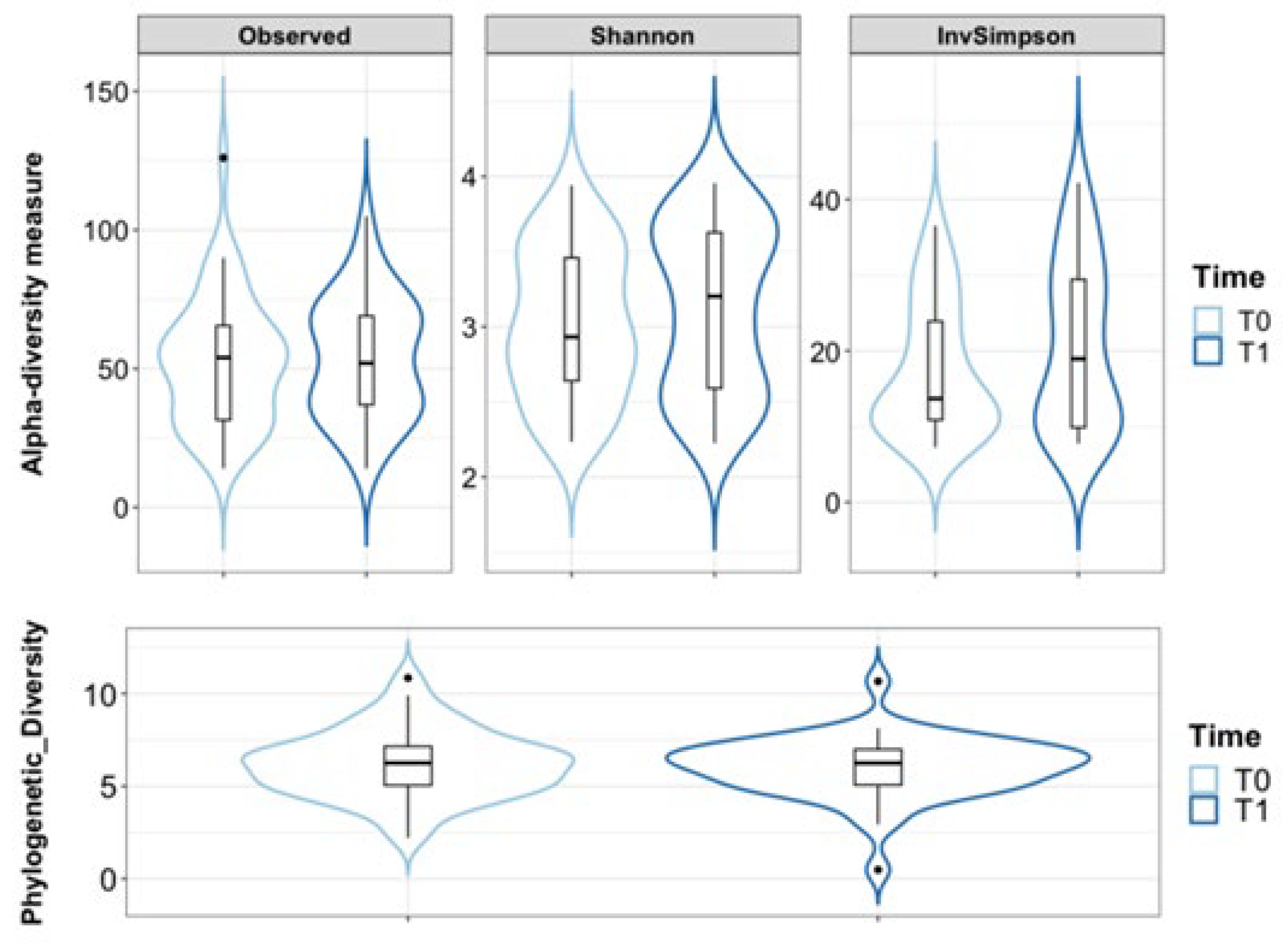
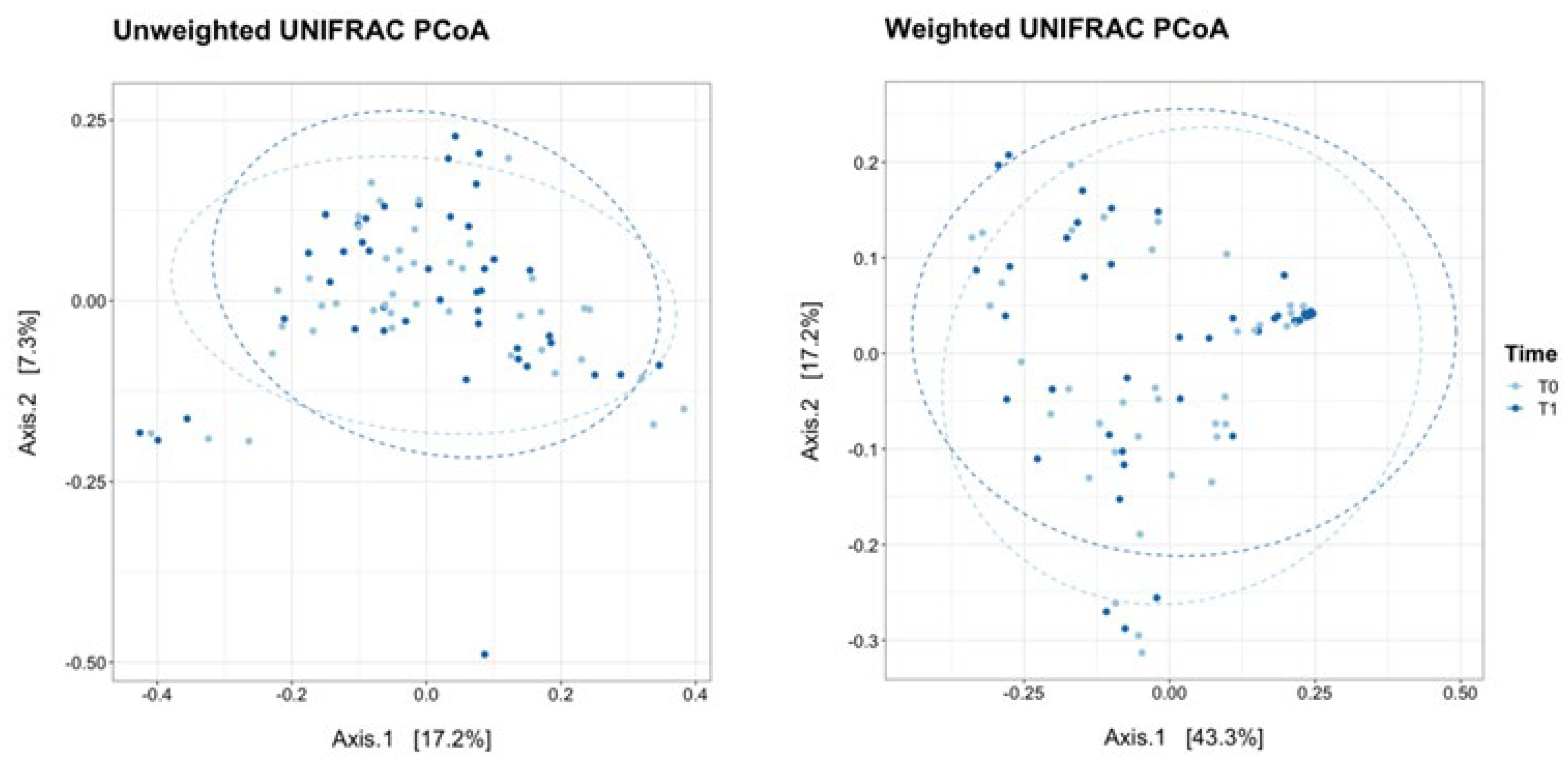
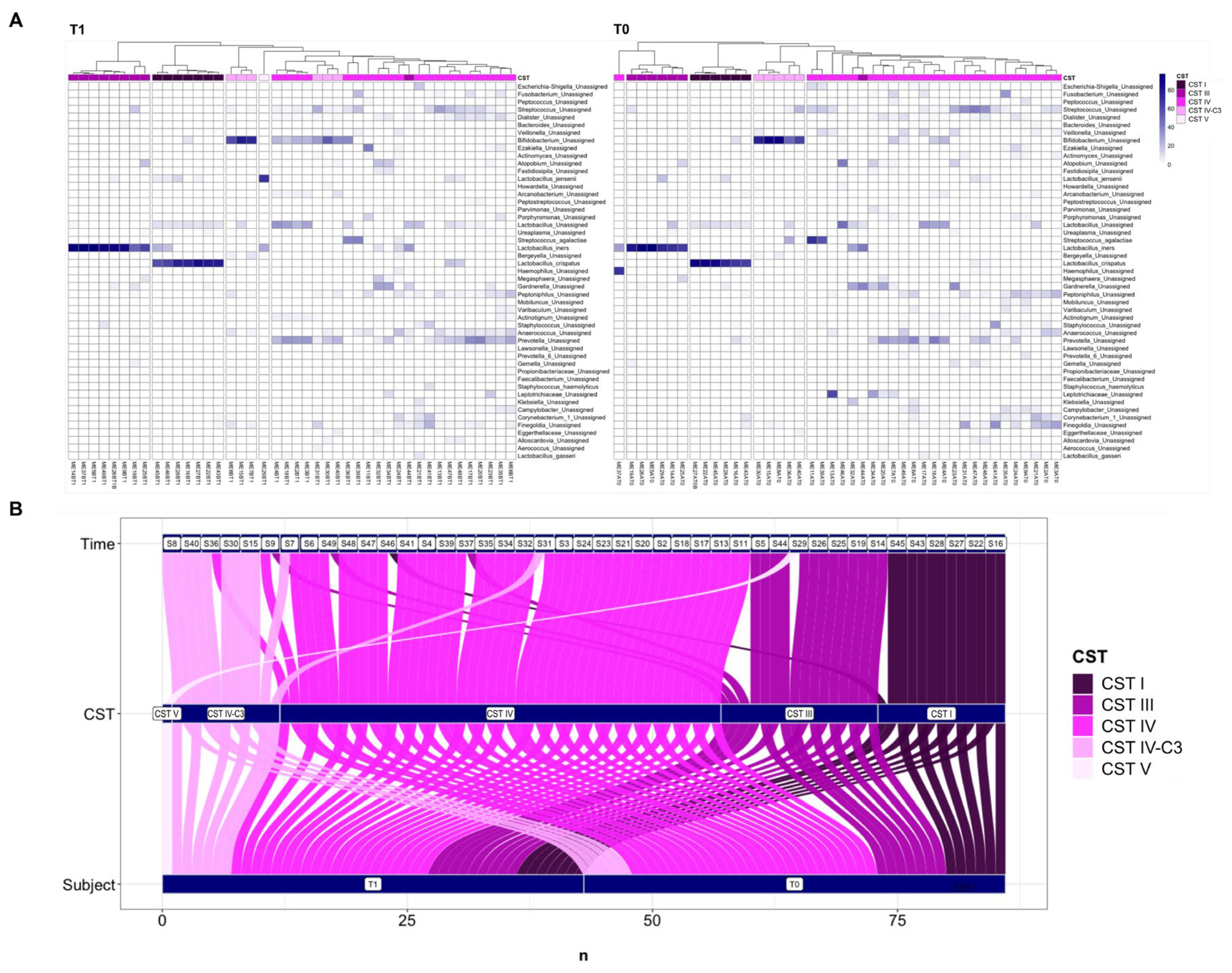
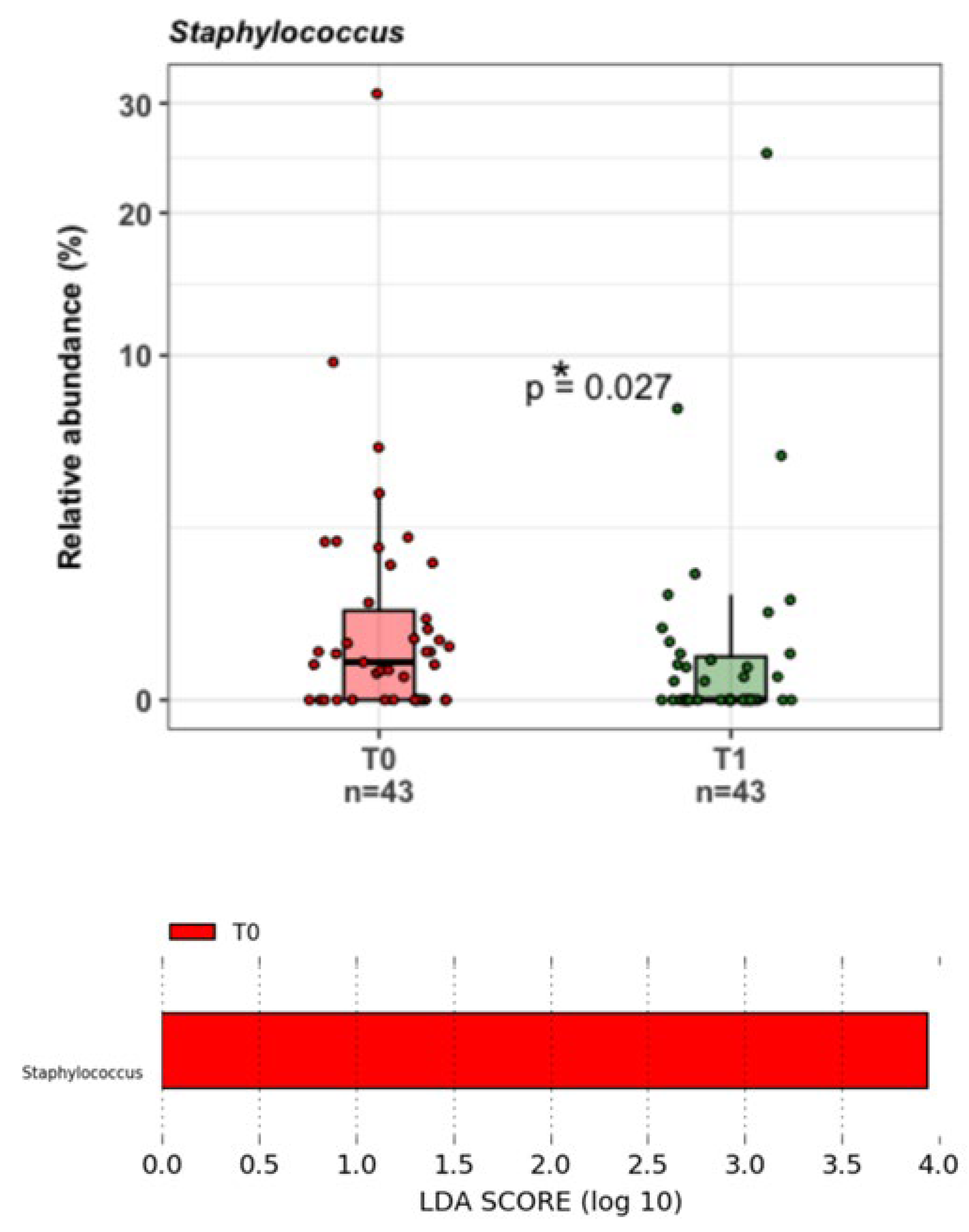
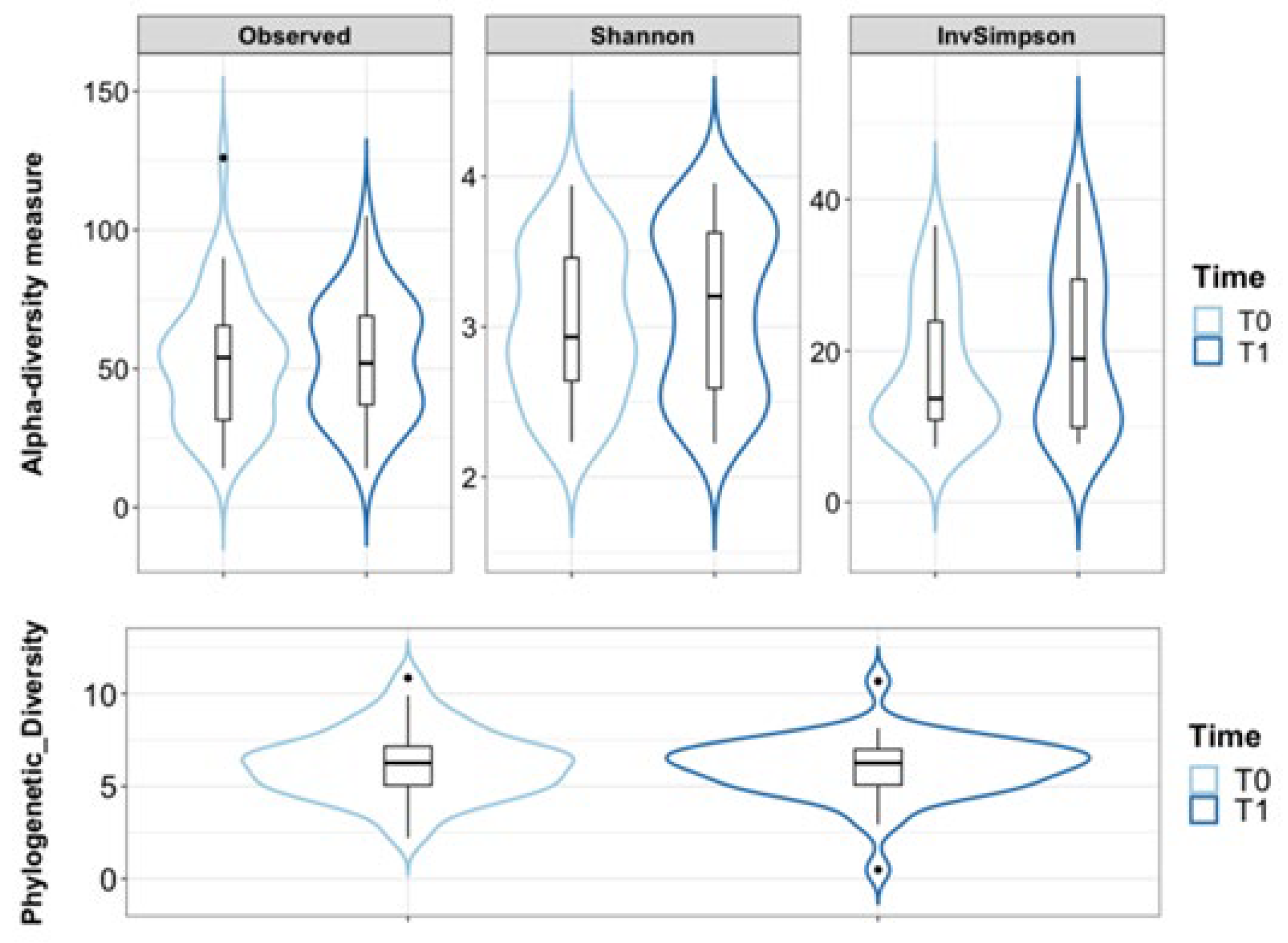
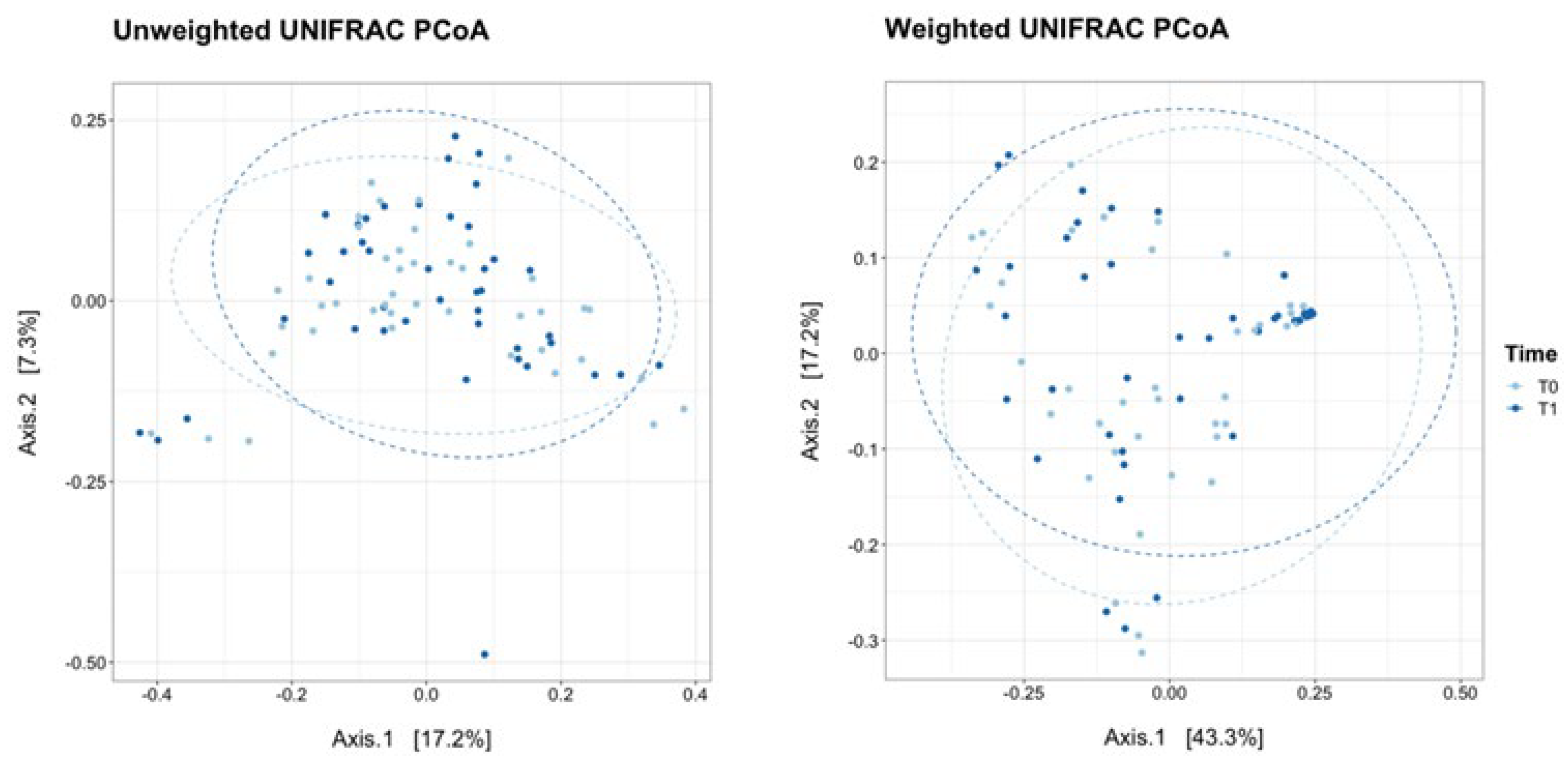
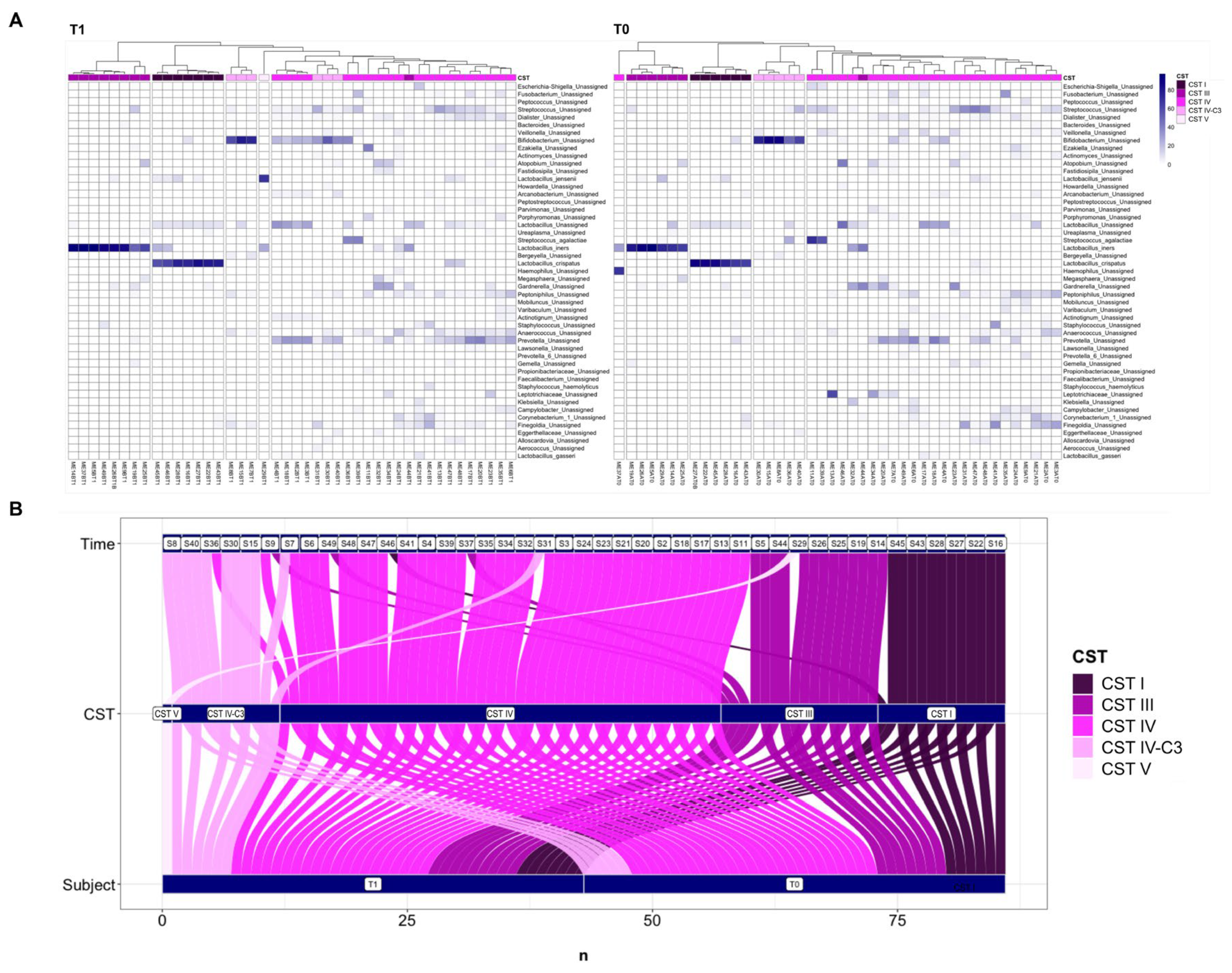
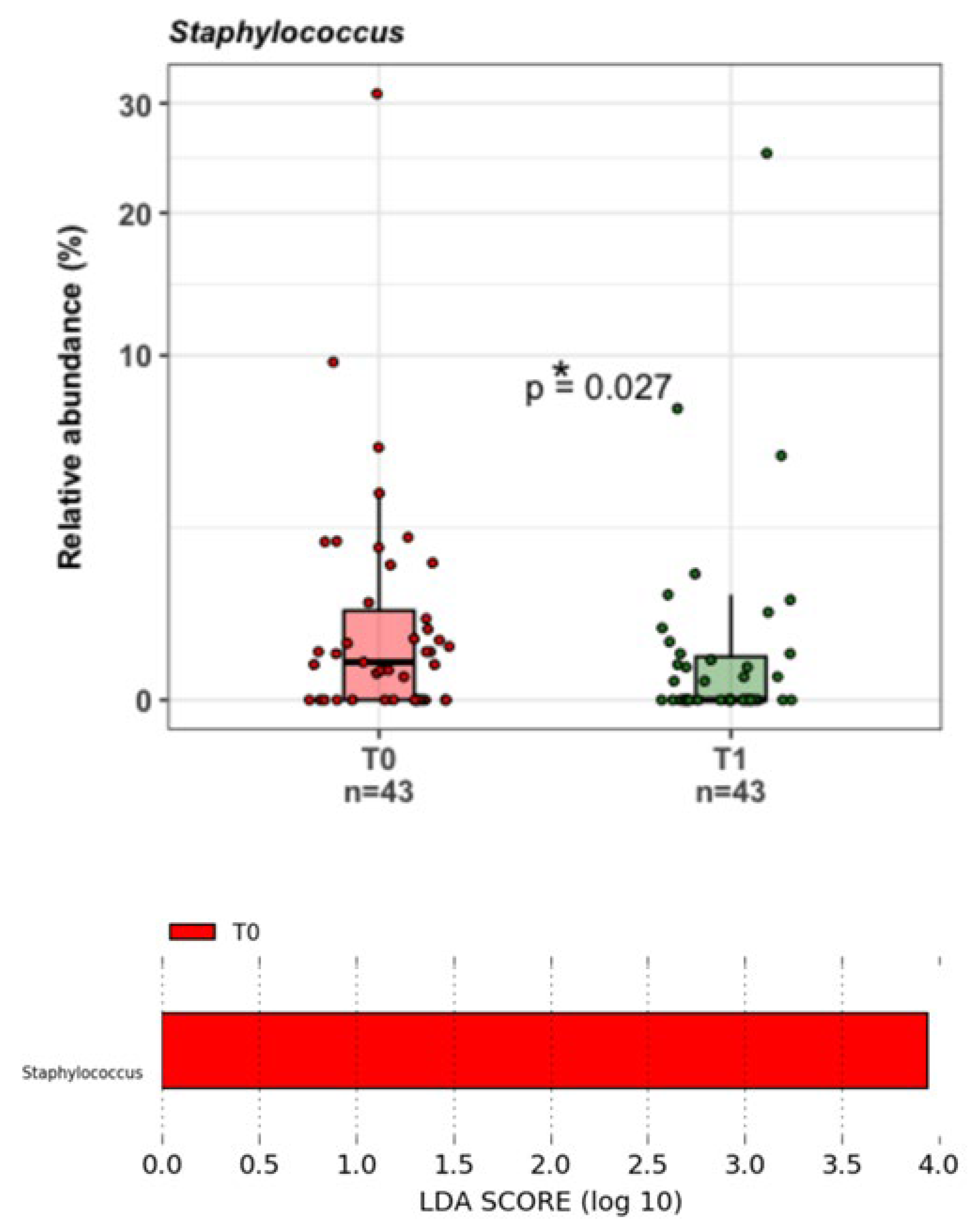
3.1. Vaginal Microbiota by NGS
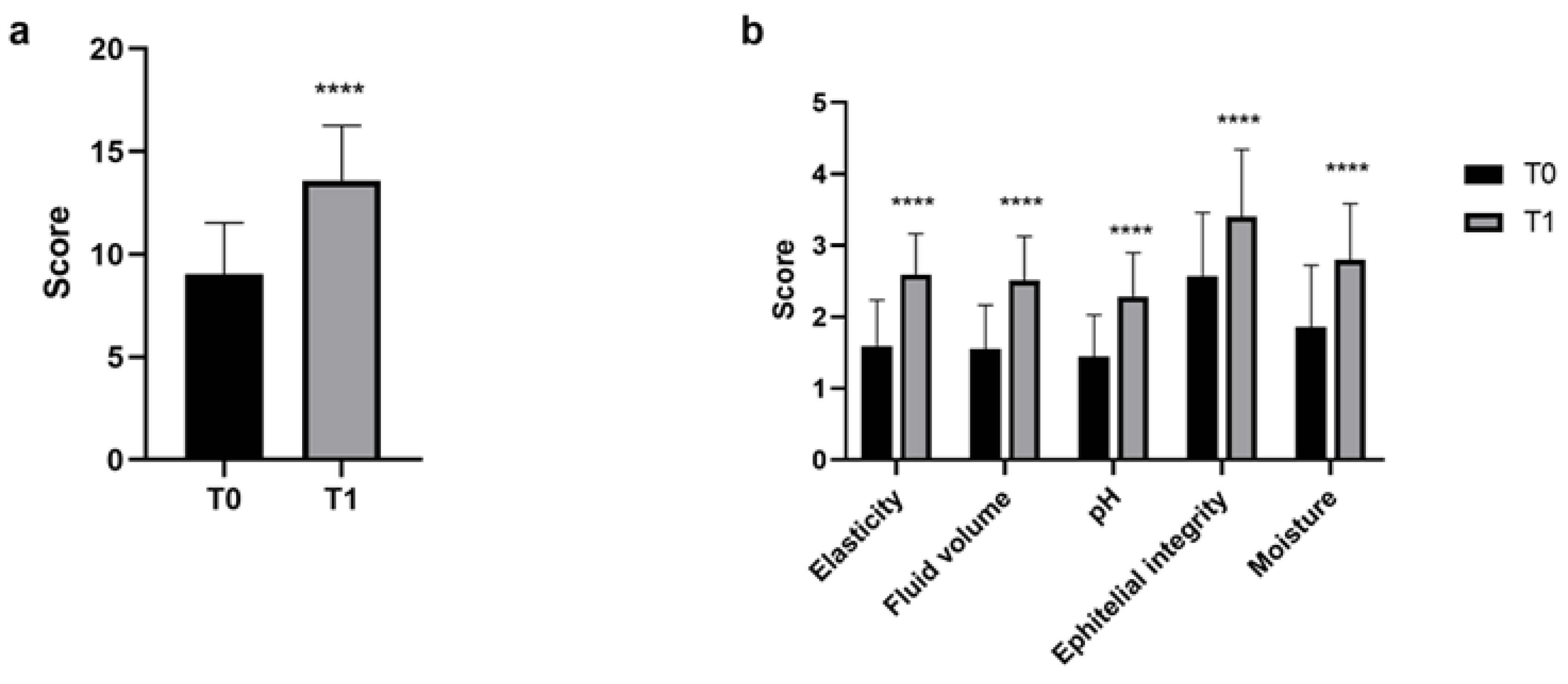
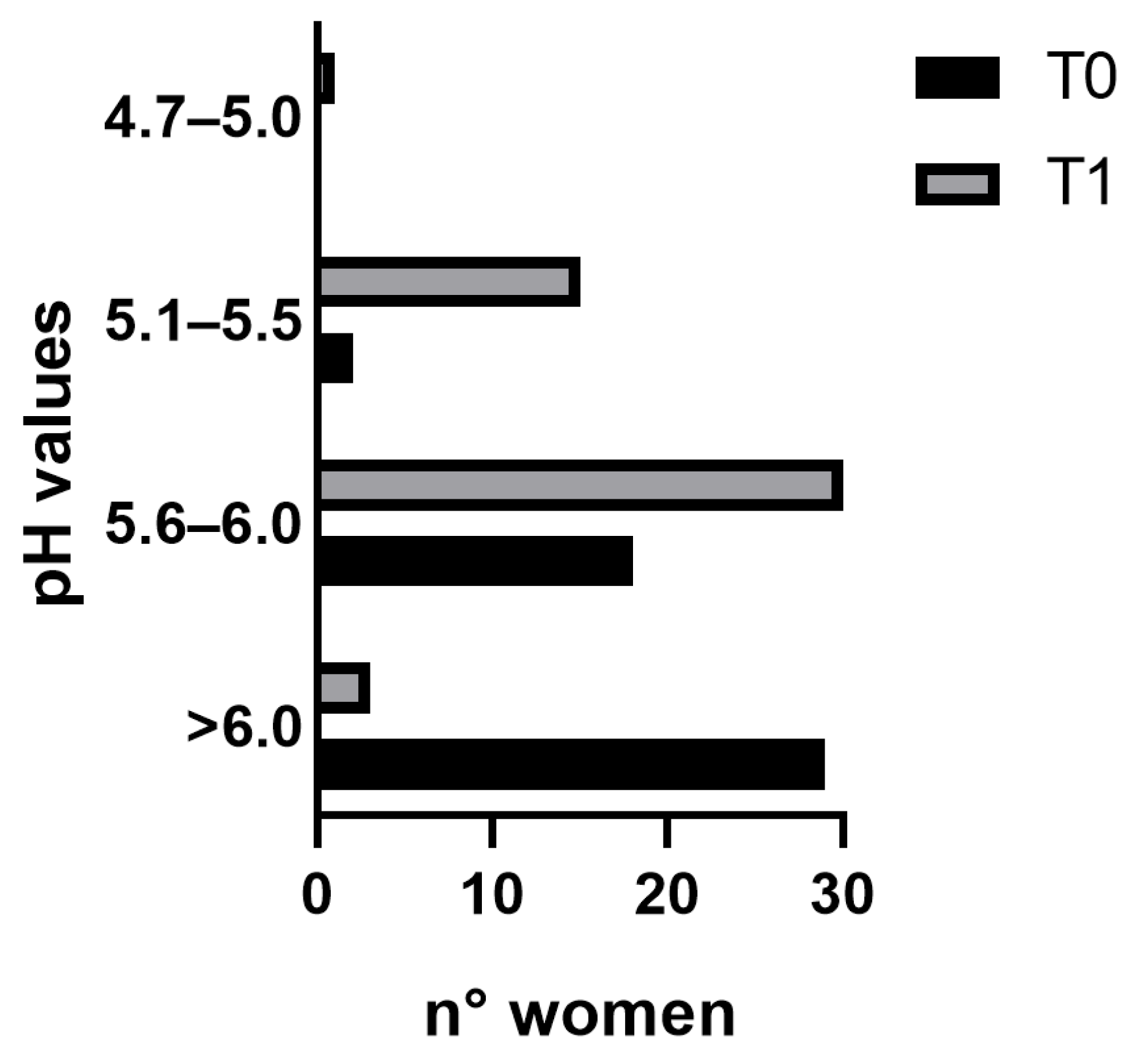
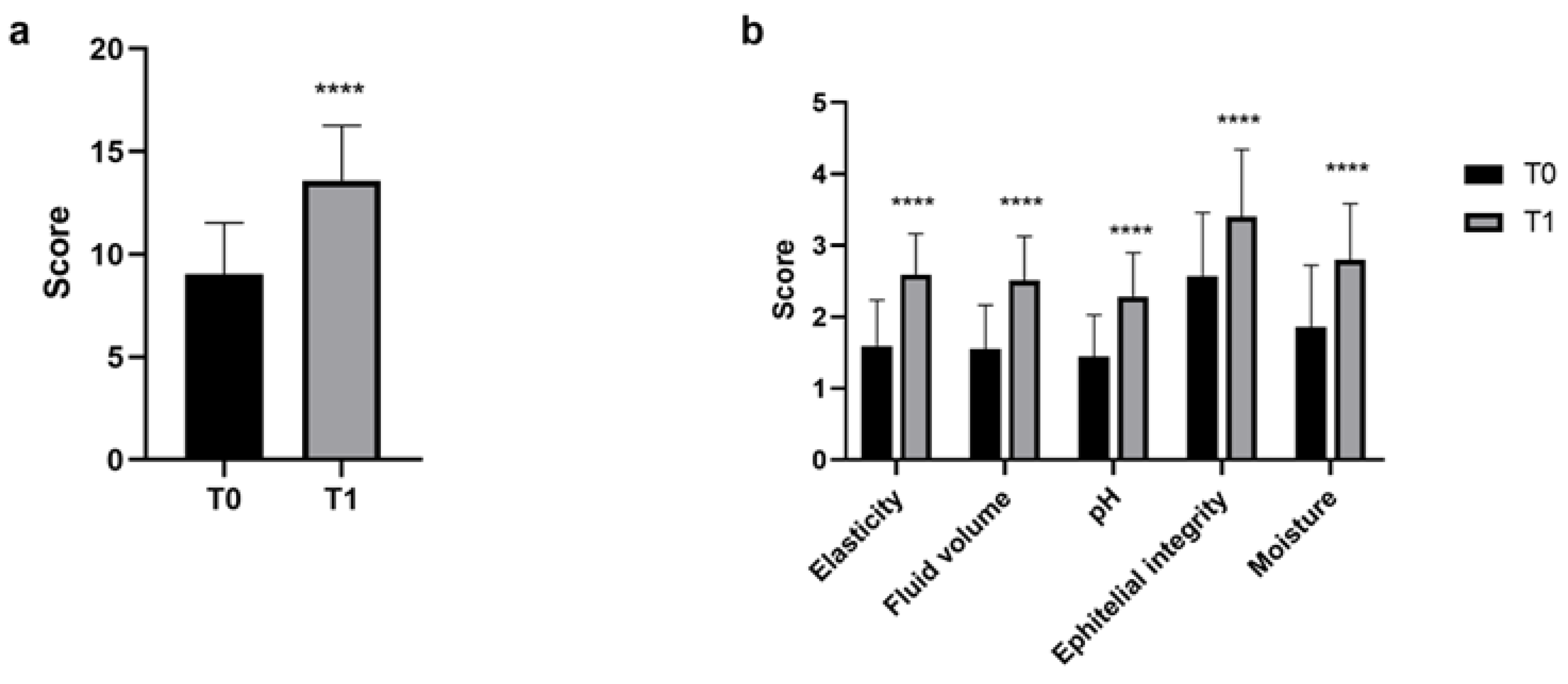
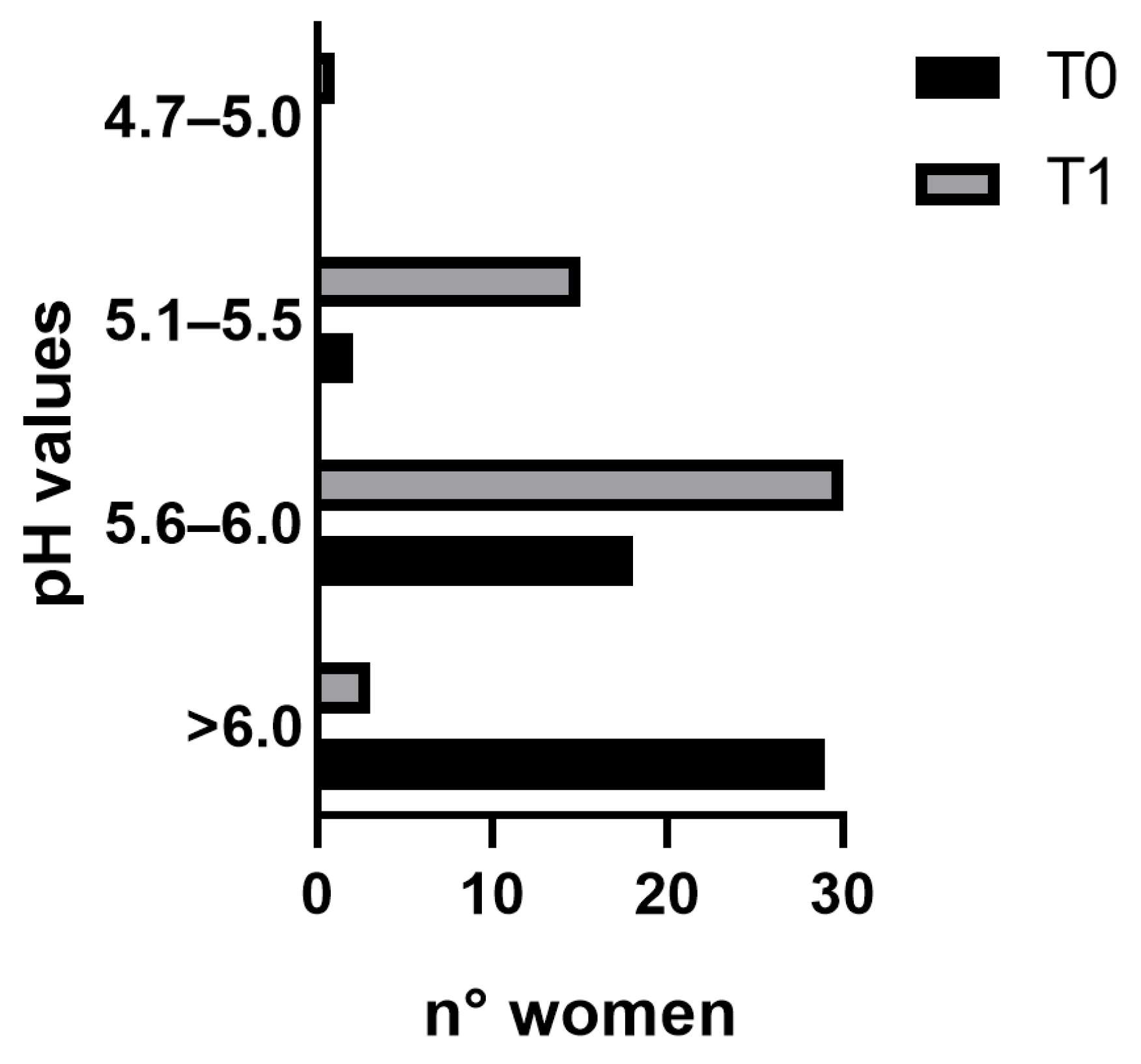
3.2. VHI
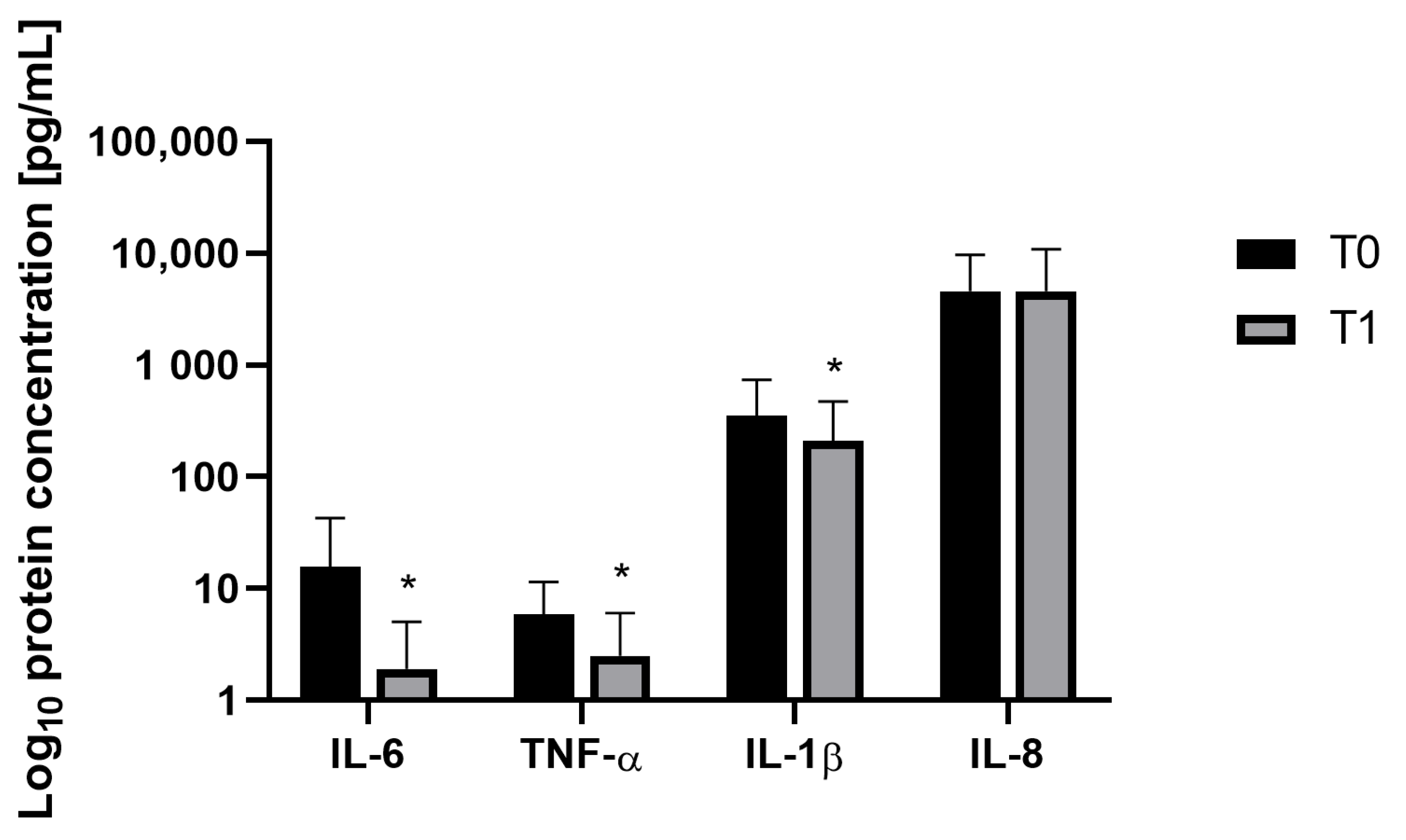
3.3. Cytokine Concentrations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Comparetto, C.; Borruto, F. Treatments and Management of Menopausal Symptoms: Current Status and Future Challenges. OBM Geriatr. 2023, 7, 1–47. [Google Scholar] [CrossRef]
- Gracia, C.R.; Freeman, E.W. Onset of the Menopause Transition. Obstet. Gynecol. Clin. N. Am. 2018, 45, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Harlow, S.D.; Gass, M.; Hall, J.E.; Lobo, R.; Maki, P.; Rebar, R.W.; Sherman, S.; Sluss, P.M.; De Villiers, T.J. Executive Summary of the Stages of Reproductive Aging Workshop + 10: Addressing the Unfinished Agenda of Staging Reproductive Aging. Menopause 2012, 19, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Rindner, L.; Nordeman, L.; Strömme, G.; Hange, D.; Gunnarsson, R.; Rembeck, G. Effect of Group Education and Person-Centered Support in Primary Health Care on Mental Health and Quality of Life in Women Aged 45–60 Years with Symptoms Commonly Associated with Stress: A Randomized Controlled Trial. BMC Womens Health 2023, 23, 128. [Google Scholar] [CrossRef]
- Hyldgaard, J.M.; Jensen, J.B. The Inequality of Females in Bladder Cancer. APMIS 2021, 129, 694–699. [Google Scholar] [CrossRef]
- Jones, H.J.; Huang, A.J.; Subak, L.L.; Brown, J.S.; Lee, K.A. Bladder Symptoms in the Early Menopausal Transition. J. Womens Health 2016, 25, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Alperin, M.; Burnett, L.; Lukacz, E.; Brubaker, L. The Mysteries of Menopause and Urogynecologic Health: Clinical and Scientific Gaps. Menopause 2019, 26, 103–111. [Google Scholar] [CrossRef]
- Amabebe, E.; Anumba, D.O.C. The Vaginal Microenvironment: The Physiologic Role of Lactobacilli. Front. Med. 2018, 5, 181. [Google Scholar] [CrossRef]
- Gänzle, M.G.; Follador, R. Metabolism of Oligosaccharides and Starch in Lactobacilli: A Review. Front. Microbiol. 2012, 3, 340. [Google Scholar] [CrossRef]
- Liu, P.; Lu, Y.; Li, R.; Chen, X. Use of Probiotic Lactobacilli in the Treatment of Vaginal Infections: In Vitro and in Vivo Investigations. Front. Cell. Infect. Microbiol. 2023, 13, 1153894. [Google Scholar] [CrossRef]
- Malfa, P.; Brambilla, L.; Giardina, S.; Masciarelli, M.; Squarzanti, D.F.; Carlomagno, F.; Meloni, M. Evaluation of Antimicrobial, Antiadhesive and Co-Aggregation Activity of a Multi-Strain Probiotic Composition against Different Urogenital Pathogens. Int. J. Mol. Sci. 2023, 24, 1323. [Google Scholar] [CrossRef]
- Murina, F.; Vicariotto, F. Evaluation of an Orally Administered Multistrain Probiotic Supplement in Reducing Recurrences Rate of Bacterial Vaginosis: A Clinical and Microbiological Study. Adv. Infect. Dis. 2019, 9, 151–161. [Google Scholar] [CrossRef]
- Nader-Macías, M.E.F.; Juárez Tomás, M.S. Profiles and Technological Requirements of Urogenital Probiotics. Adv. Drug Deliv. Rev. 2015, 92, 84–104. [Google Scholar] [CrossRef] [PubMed]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.K.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal Microbiome of Reproductive-Age Women. Proc. Natl. Acad. Sci. USA 2011, 108, 4680–4687. [Google Scholar] [CrossRef] [PubMed]
- Brotman, R.M.; Shardell, M.D.; Gajer, P.; Fadrosh, D.; Chang, K.; Silver, M.I.; Viscidi, R.P.; Burke, A.E.; Ravel, J.; Gravitt, P.E. Association between the Vaginal Microbiota, Menopause Status, and Signs of Vulvovaginal Atrophy. Menopause 2014, 21, 450–458. [Google Scholar] [CrossRef]
- Mitchell, C.; Marrazzo, J. Bacterial Vaginosis and the Cervicovaginal Immune Response. Am. J. Reprod. Immunol. 2014, 71, 555–563. [Google Scholar] [CrossRef]
- Meštrović, T.; Matijašić, M.; Perić, M.; Čipčić Paljetak, H.; Barešić, A.; Verbanac, D. The Role of Gut, Vaginal, and Urinary Microbiome in Urinary Tract Infections: From Bench to Bedside. Diagnostics 2020, 11, 7. [Google Scholar] [CrossRef]
- Barrea, L.; Verde, L.; Auriemma, R.S.; Vetrani, C.; Cataldi, M.; Frias-Toral, E.; Pugliese, G.; Camajani, E.; Savastano, S.; Colao, A.; et al. Probiotics and Prebiotics: Any Role in Menopause-Related Diseases? Curr. Nutr. Rep. 2023, 12, 83–97. [Google Scholar] [CrossRef]
- Vieira, A.T.; Castelo, P.M.; Ribeiro, D.A.; Ferreira, C.M. Influence of Oral and Gut Microbiota in the Health of Menopausal Women. Front. Microbiol. 2017, 8, 1884. [Google Scholar] [CrossRef]
- Dupuit, M.; Rance, M.; Morel, C.; Bouillon, P.; Boscaro, A.; Martin, V.; Vazeille, E.; Barnich, N.; Chassaing, B.; Boisseau, N. Effect of Concurrent Training on Body Composition and Gut Microbiota in Postmenopausal Women with Overweight or Obesity. Med. Sci. Sports Exerc. 2022, 54, 517–529. [Google Scholar] [CrossRef]
- Vigneswaran, K.; Hamoda, H. Hormone Replacement Therapy—Current Recommendations. Best Pract. Res. Clin. Obstet. Gynaecol. 2022, 81, 8–21. [Google Scholar] [CrossRef] [PubMed]
- Cagnacci, A.; Venier, M. The Controversial History of Hormone Replacement Therapy. Medicina 2019, 55, 602. [Google Scholar] [CrossRef] [PubMed]
- Klindworth, A.; Pruesse, E.; Schweer, T.; Peplies, J.; Quast, C.; Horn, M.; Glöckner, F.O. Evaluation of General 16S Ribosomal RNA Gene PCR Primers for Classical and Next-Generation Sequencing-Based Diversity Studies. Nucleic Acids Res. 2013, 41, e1. [Google Scholar] [CrossRef] [PubMed]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, Interactive, Scalable and Extensible Microbiome Data Science Using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Hall, M.; Beiko, R.G. 16S rRNA Gene Analysis with QIIME2. In Microbiome Analysis; Beiko, R.G., Hsiao, W., Parkinson, J., Eds.; Methods in Molecular Biology; Springer: New York, NY, USA, 2018; Volume 1849, pp. 113–129. ISBN 978-1-4939-8726-9. [Google Scholar]
- Rognes, T.; Flouri, T.; Nichols, B.; Quince, C.; Mahé, F. VSEARCH: A Versatile Open Source Tool for Metagenomics. PeerJ 2016, 4, e2584. [Google Scholar] [CrossRef]
- Yilmaz, P.; Parfrey, L.W.; Yarza, P.; Gerken, J.; Pruesse, E.; Quast, C.; Schweer, T.; Peplies, J.; Ludwig, W.; Glöckner, F.O. The SILVA and “All-Species Living Tree Project (LTP)” Taxonomic Frameworks. Nucleic Acids Res. 2014, 42, D643–D648. [Google Scholar] [CrossRef]
- McMurdie, P.J.; Holmes, S. Phyloseq: An R Package for Reproducible Interactive Analysis and Graphics of Microbiome Census Data. PLoS ONE 2013, 8, e61217. [Google Scholar] [CrossRef]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Davis, N.M.; Proctor, D.M.; Holmes, S.P.; Relman, D.A.; Callahan, B.J. Simple Statistical Identification and Removal of Contaminant Sequences in Marker-Gene and Metagenomics Data. Microbiome 2018, 6, 226. [Google Scholar] [CrossRef] [PubMed]
- Lozupone, C.; Knight, R. UniFrac: A New Phylogenetic Method for Comparing Microbial Communities. Appl. Environ. Microbiol. 2005, 71, 8228–8235. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.J.; Walsh, D.C.I. PERMANOVA, ANOSIM, and the Mantel Test in the Face of Heterogeneous Dispersions: What Null Hypothesis Are You Testing? Ecol. Monogr. 2013, 83, 557–574. [Google Scholar] [CrossRef]
- Segata, N.; Izard, J.; Waldron, L.; Gevers, D.; Miropolsky, L.; Garrett, W.S.; Huttenhower, C. Metagenomic Biomarker Discovery and Explanation. Genome Biol. 2011, 12, R60. [Google Scholar] [CrossRef] [PubMed]
- Sarmento, A.C.A.; Costa, A.P.F.; Vieira-Baptista, P.; Giraldo, P.C.; Eleutério, J.; Gonçalves, A.K. Genitourinary Syndrome of Menopause: Epidemiology, Physiopathology, Clinical Manifestation and Diagnostic. Front. Reprod. Health 2021, 3, 779398. [Google Scholar] [CrossRef]
- Alvisi, S.; Gava, G.; Orsili, I.; Giacomelli, G.; Baldassarre, M.; Seracchioli, R.; Meriggiola, M.C. Vaginal Health in Menopausal Women. Medicina 2019, 55, 615. [Google Scholar] [CrossRef] [PubMed]
- Morris, E.K.; Caruso, T.; Buscot, F.; Fischer, M.; Hancock, C.; Maier, T.S.; Meiners, T.; Müller, C.; Obermaier, E.; Prati, D.; et al. Choosing and Using Diversity Indices: Insights for Ecological Applications from the German Biodiversity Exploratories. Ecol. Evol. 2014, 4, 3514–3524. [Google Scholar] [CrossRef] [PubMed]
- France, M.T.; Ma, B.; Gajer, P.; Brown, S.; Humphrys, M.S.; Holm, J.B.; Waetjen, L.E.; Brotman, R.M.; Ravel, J. VALENCIA: A Nearest Centroid Classification Method for Vaginal Microbial Communities Based on Composition. Microbiome 2020, 8, 166. [Google Scholar] [CrossRef]
- Santoro, N.; Roeca, C.; Peters, B.A.; Neal-Perry, G. The Menopause Transition: Signs, Symptoms, and Management Options. J. Clin. Endocrinol. Metab. 2021, 106, 1–15. [Google Scholar] [CrossRef]
- Bacon, J.L. The Menopausal Transition. Obstet. Gynecol. Clin. N. Am. 2017, 44, 285–296. [Google Scholar] [CrossRef]
- Ayers, B.; Forshaw, M.; Hunter, M.S. The Impact of Attitudes towards the Menopause on Women’s Symptom Experience: A Systematic Review. Maturitas 2010, 65, 28–36. [Google Scholar] [CrossRef]
- Wang, Q.; Ferreira, D.L.S.; Nelson, S.M.; Sattar, N.; Ala-Korpela, M.; Lawlor, D.A. Metabolic Characterization of Menopause: Cross-Sectional and Longitudinal Evidence. BMC Med. 2018, 16, 17. [Google Scholar] [CrossRef]
- Humphries, K.H.; Gill, S. Risks and Benefits of Hormone Replacement Therapy: The Evidence Speaks. Horm. Replace. Ther. 2003, 168, 1001–1010. [Google Scholar]
- De Seta, F.; Campisciano, G.; Zanotta, N.; Ricci, G.; Comar, M. The Vaginal Community State Types Microbiome-Immune Network as Key Factor for Bacterial Vaginosis and Aerobic Vaginitis. Front. Microbiol. 2019, 10, 2451. [Google Scholar] [CrossRef]
- Borges, S.; Silva, J.; Teixeira, P. The Role of Lactobacilli and Probiotics in Maintaining Vaginal Health. Arch. Gynecol. Obstet. 2014, 289, 479–489. [Google Scholar] [CrossRef]
- Aldunate, M.; Srbinovski, D.; Hearps, A.C.; Latham, C.F.; Ramsland, P.A.; Gugasyan, R.; Cone, R.A.; Tachedjian, G. Antimicrobial and Immune Modulatory Effects of Lactic Acid and Short Chain Fatty Acids Produced by Vaginal Microbiota Associated with Eubiosis and Bacterial Vaginosis. Front. Physiol. 2015, 6, 164. [Google Scholar] [CrossRef]
- Presti, I.; D’Orazio, G.; Labra, M.; La Ferla, B.; Mezzasalma, V.; Bizzaro, G.; Giardina, S.; Michelotti, A.; Tursi, F.; Vassallo, M.; et al. Evaluation of the Probiotic Properties of New Lactobacillus and Bifidobacterium Strains and Their in Vitro Effect. Appl. Microbiol. Biotechnol. 2015, 99, 5613–5626. [Google Scholar] [CrossRef]
- Mezzasalma, V.; Manfrini, E.; Ferri, E.; Sandionigi, A.; La Ferla, B.; Schiano, I.; Michelotti, A.; Nobile, V.; Labra, M.; Di Gennaro, P. A Randomized, Double-Blind, Placebo-Controlled Trial: The Efficacy of Multispecies Probiotic Supplementation in Alleviating Symptoms of Irritable Bowel Syndrome Associated with Constipation. BioMed. Res. Int. 2016, 2016, 4740907. [Google Scholar] [CrossRef]
- Chee, W.J.Y.; Chew, S.Y.; Than, L.T.L. Vaginal Microbiota and the Potential of Lactobacillus Derivatives in Maintaining Vaginal Health. Microb. Cell Factories 2020, 19, 203. [Google Scholar] [CrossRef]
- Vicariotto, F.; Mogna, L.; Del Piano, M. Effectiveness of the Two Microorganisms Lactobacillus fermentum LF15 and Lactobacillus plantarum LP01, Formulated in Slow-Release Vaginal Tablets, in Women Affected by Bacterial Vaginosis: A Pilot Study. J. Clin. Gastroenterol. 2014, 48, S106–S112. [Google Scholar] [CrossRef]
- Xu, K.; Wang, Y.; Jian, Y.; Chen, T.; Liu, Q.; Wang, H.; Li, M.; He, L. Staphylococcus Aureus ST1 Promotes Persistent Urinary Tract Infection by Highly Expressing the Urease. Front. Microbiol. 2023, 14, 1101754. [Google Scholar] [CrossRef]
- Smith, S.B.; Ravel, J. The Vaginal Microbiota, Host Defence and Reproductive Physiology. J. Physiol. 2017, 595, 451–463. [Google Scholar] [CrossRef]
- Nappi, R.E.; Kotek, M.; Brešt’anský, A.; Giordan, N.; Tramentozzi, E. Effectiveness of Hyaluronate-Based Pessaries in the Treatment of Vulvovaginal Atrophy in Postmenopausal Women. Climacteric 2020, 23, 519–524. [Google Scholar] [CrossRef]
- Nappi, R.E.; Martini, E.; Cucinella, L.; Martella, S.; Tiranini, L.; Inzoli, A.; Brambilla, E.; Bosoni, D.; Cassani, C.; Gardella, B. Addressing Vulvovaginal Atrophy (VVA)/Genitourinary Syndrome of Menopause (GSM) for Healthy Aging in Women. Front. Endocrinol. 2019, 10, 561. [Google Scholar] [CrossRef]
- Domoney, C. Treatment of Vaginal Atrophy. Womens Health 2014, 10, 191–200. [Google Scholar] [CrossRef]
- Han, A.; Kim, J.Y.; Kwak-Kim, J.; Lee, S.K. Menopause Is an Inflection Point of Age-Related Immune Changes in Women. J. Reprod. Immunol. 2021, 146, 103346. [Google Scholar] [CrossRef]
- Levit, R.; Savoy De Giori, G.; De Moreno De LeBlanc, A.; LeBlanc, J.G. Folate-Producing Lactic Acid Bacteria Reduce Inflammation in Mice with Induced Intestinal Mucositis. J. Appl. Microbiol. 2018, 125, 1494–1501. [Google Scholar] [CrossRef]
- Chen, Q.; Wang, H.; Wang, G.; Zhao, J.; Chen, H.; Lu, X.; Chen, W. Lactic Acid Bacteria: A Promising Tool for Menopausal Health Management in Women. Nutrients 2022, 14, 4466. [Google Scholar] [CrossRef]
- Spear, G.T.; Zariffard, M.R.; Cohen, M.H.; Sha, B.E. Vaginal IL-8 Levels Are Positively Associated with Candida Albicans and Inversely with Lactobacilli in HIV-Infected Women. J. Reprod. Immunol. 2008, 78, 76–79. [Google Scholar] [CrossRef]
- Kaambo, E.; Africa, C.; Chambuso, R.; Passmore, J.-A.S. Vaginal Microbiomes Associated With Aerobic Vaginitis and Bacterial Vaginosis. Front. Public Health 2018, 6, 78. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Post-menopausal women for 18 months (last menstruation observed) | Women undergoing HRT |
| Women with BMI ≤ 27 | Women with BMI > 27 |
| Women with vaginal pH ≥ 5 | Women with a demonstrated allergy to one or more ingredients contained in the product |
| Menopausal women with typical menopausal complaints such as burning, redness, stinging sensation, oedema, dyspareunia, and discharge | Women who intend to use probiotic products (e.g., yoghurt fortified with probiotics or probiotic-based dietary supplements) and have used them in the past 2 weeks |
| Women who intend to use the probiotic product and undergo follow-up visits | Women who have undergone antimicrobial treatment within the past 4 weeks |
| Post-menopausal women for 18 months (last menstruation observed) | Women undergoing HRT |
| Women with BMI ≤ 27 | Women with BMI > 27 |
| Women with vaginal pH ≥ 5 | Women with a demonstrated allergy to one or more ingredients contained in the product |
| Score | Overall Elasticity | Fluid Secretion Type and Consistency | pH | Epithelial Mucous | Moisture |
|---|---|---|---|---|---|
| 1 | None | None | >6.0 | Petechiae noted before contact | None, mucosa inflamed |
| 2 | Poor | Scant, thin yellow | 5.6–6.0 | Bleeds with light contact | None, mucosa not inflamed |
| 3 | Fair | Superficial, thin white | 5.1–5.5 | Bleeds with scraping | Minimal |
| 4 | Good | Moderate, thin white | 4.7–5.0 | Not friable, thin mucous | Moderate |
| 5 | Excellent | Normal (white flocculent) | <4.6 | Not friable, normal mucosa | Normal |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicariotto, F.; Malfa, P.; Viciani, E.; Dell’Atti, F.; Squarzanti, D.F.; Marcante, A.; Castagnetti, A.; Ponchia, R.; Governini, L.; De Leo, V. Efficacy of Lactiplantibacillus plantarum PBS067, Bifidobacterium animalis subsp. lactis BL050, and Lacticaseibacillus rhamnosus LRH020 in the Amelioration of Vaginal Microbiota in Post-Menopausal Women: A Prospective Observational Clinical Trial. Nutrients 2024, 16, 402. https://doi.org/10.3390/nu16030402
Vicariotto F, Malfa P, Viciani E, Dell’Atti F, Squarzanti DF, Marcante A, Castagnetti A, Ponchia R, Governini L, De Leo V. Efficacy of Lactiplantibacillus plantarum PBS067, Bifidobacterium animalis subsp. lactis BL050, and Lacticaseibacillus rhamnosus LRH020 in the Amelioration of Vaginal Microbiota in Post-Menopausal Women: A Prospective Observational Clinical Trial. Nutrients. 2024; 16(3):402. https://doi.org/10.3390/nu16030402
Chicago/Turabian StyleVicariotto, Franco, Patrizia Malfa, Elisa Viciani, Federica Dell’Atti, Diletta F. Squarzanti, Andrea Marcante, Andrea Castagnetti, Rosetta Ponchia, Laura Governini, and Vincenzo De Leo. 2024. "Efficacy of Lactiplantibacillus plantarum PBS067, Bifidobacterium animalis subsp. lactis BL050, and Lacticaseibacillus rhamnosus LRH020 in the Amelioration of Vaginal Microbiota in Post-Menopausal Women: A Prospective Observational Clinical Trial" Nutrients 16, no. 3: 402. https://doi.org/10.3390/nu16030402
APA StyleVicariotto, F., Malfa, P., Viciani, E., Dell’Atti, F., Squarzanti, D. F., Marcante, A., Castagnetti, A., Ponchia, R., Governini, L., & De Leo, V. (2024). Efficacy of Lactiplantibacillus plantarum PBS067, Bifidobacterium animalis subsp. lactis BL050, and Lacticaseibacillus rhamnosus LRH020 in the Amelioration of Vaginal Microbiota in Post-Menopausal Women: A Prospective Observational Clinical Trial. Nutrients, 16(3), 402. https://doi.org/10.3390/nu16030402