
Dietary Patterns and Hypothyroidism in U.S. Adult Population



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
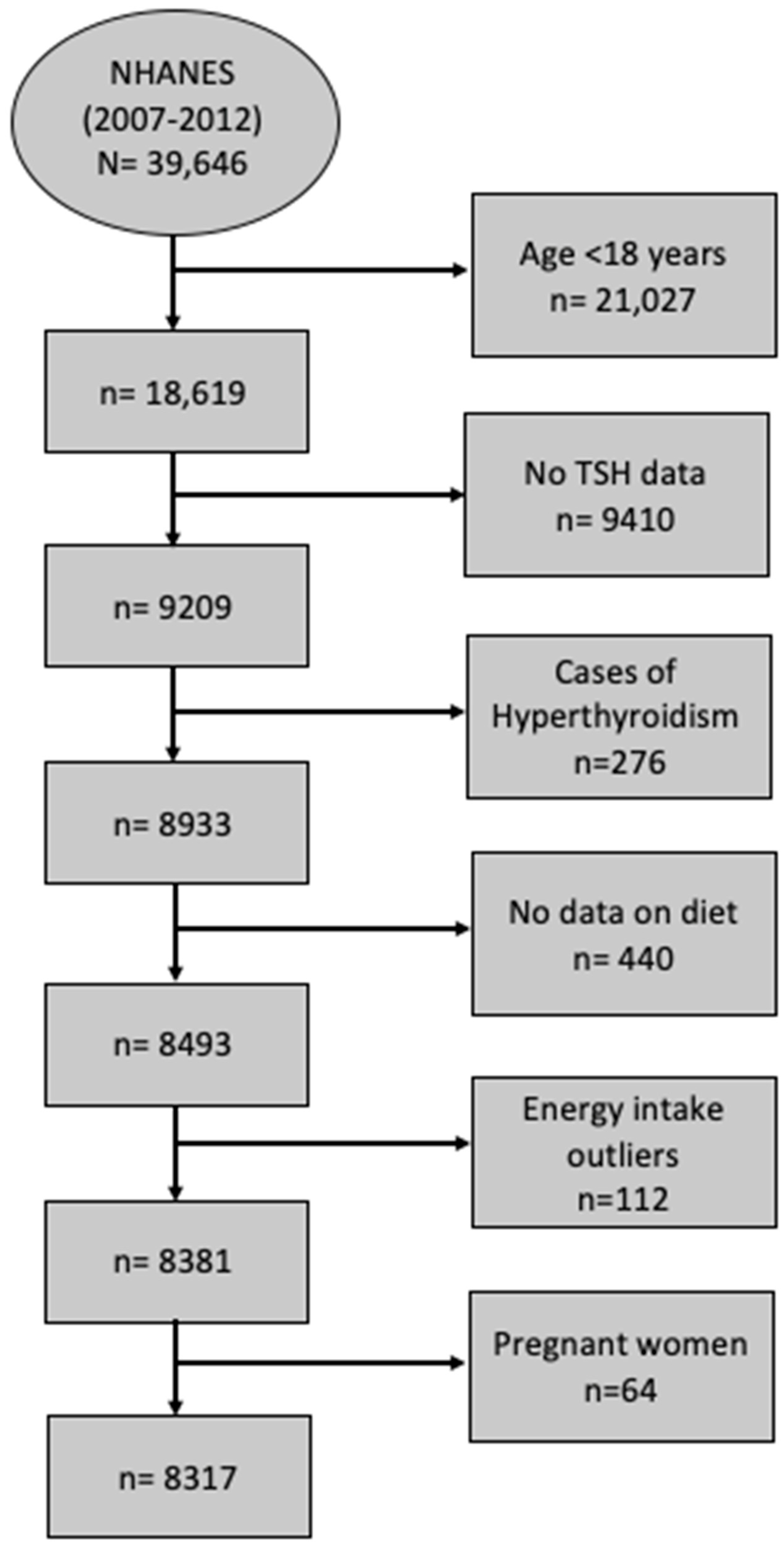
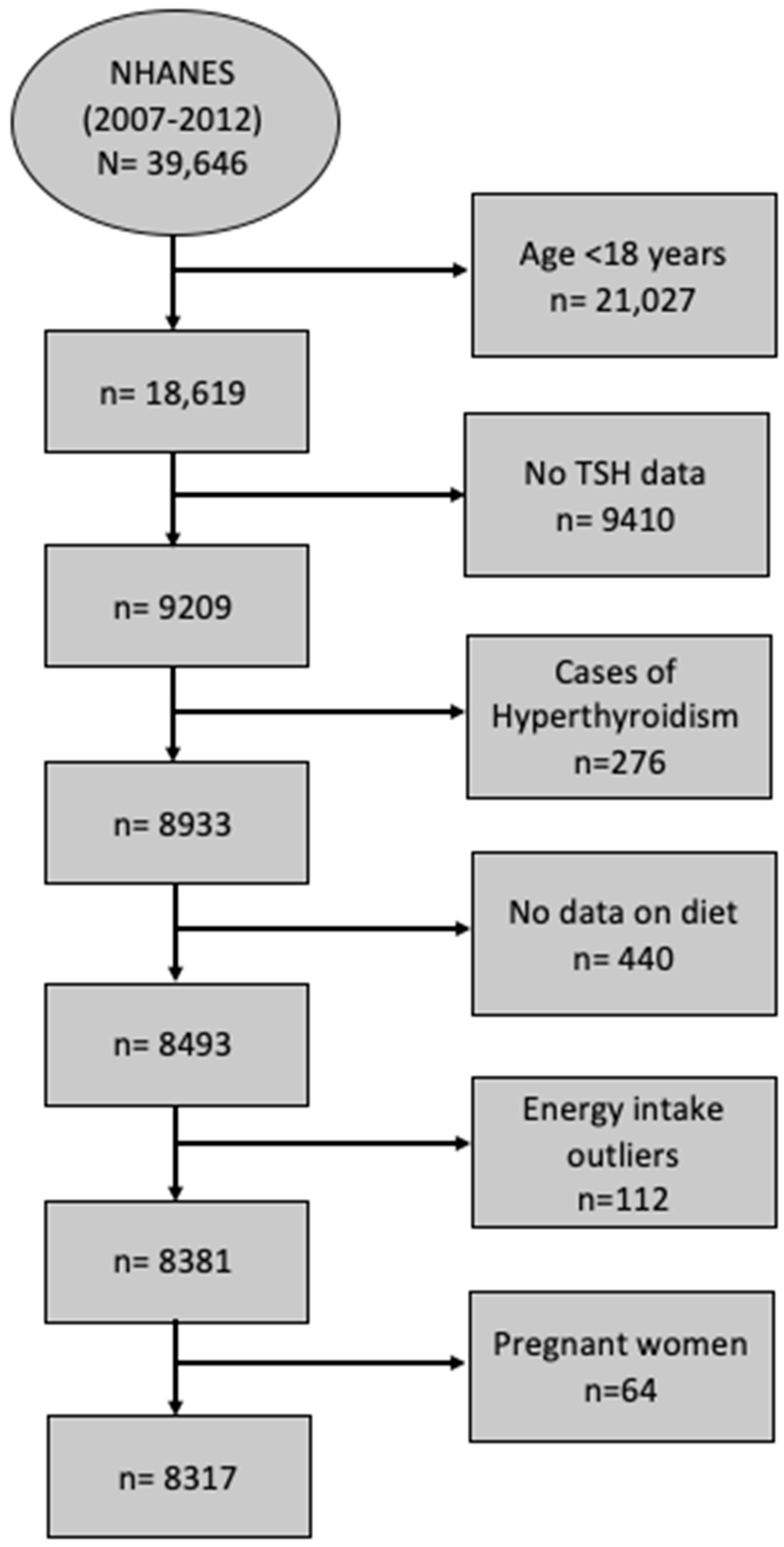
2.2. Study Population
2.3. Dietary Intake Assessment
2.4. Biochemical Measurements
2.5. Other Measurements
2.6. Statistical Analysis
3. Results
3.1. Study Sample Characteristics by Hypothyroidism Status
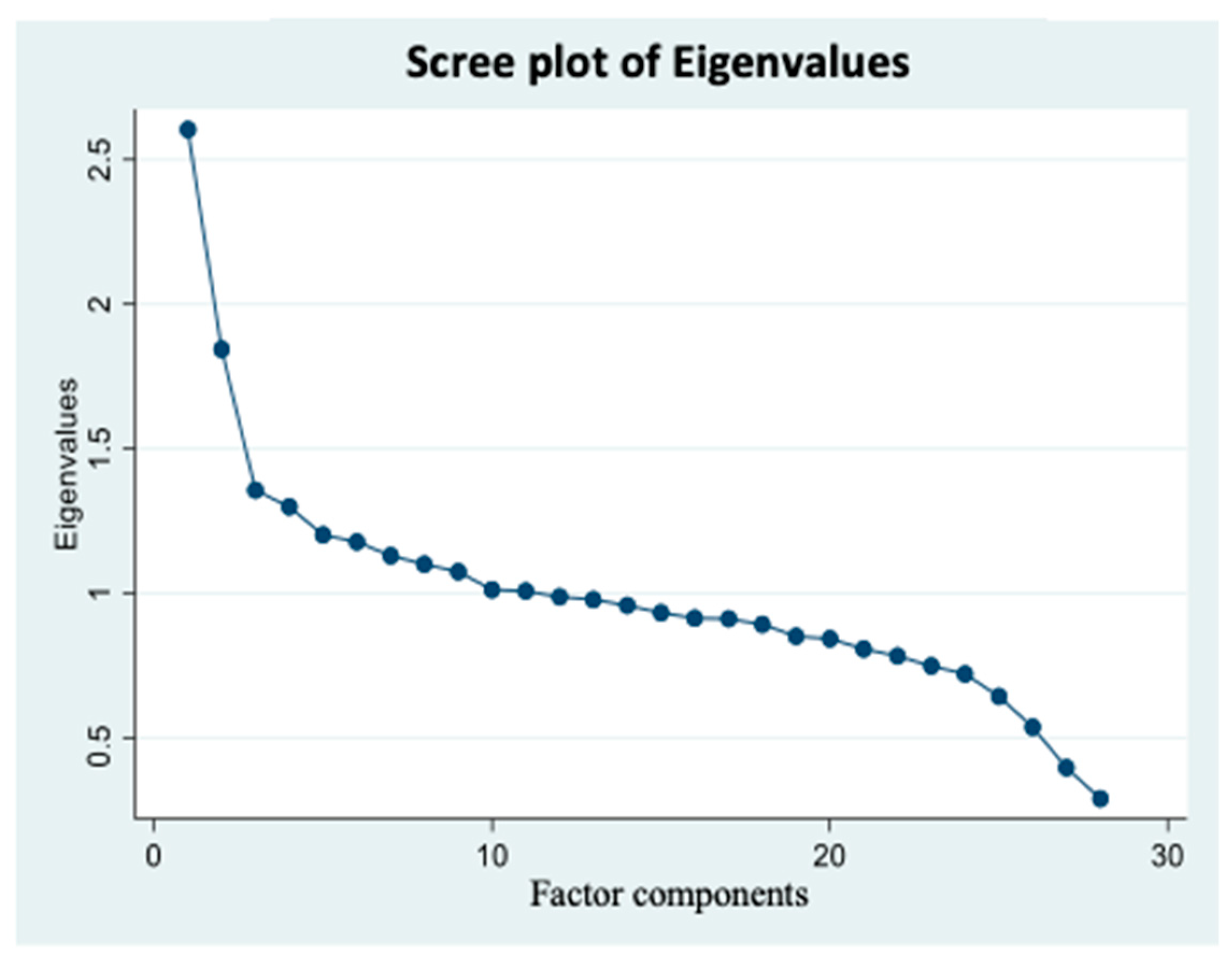
3.2. Dietary Intake Patterns Description
3.3. Association between Food Patterns and Hypothyroidism
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patil, N.; Rehman, A.; Jialal, I. Hypothyroidism. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Chiovato, L.; Magri, F.; Carlé, A. Hypothyroidism in Context: Where We’ve Been and Where We’re Going. Adv. Ther. 2019, 36, 47. [Google Scholar] [CrossRef]
- Mehalingam, V.; Sahoo, J.; Bobby, Z.; Vinod, K.V. Thyroid Dysfunction in Patients with Type 2 Diabetes Mellitus and Its Association with Diabetic Complications. J. Fam. Med. Prim. Care 2020, 9, 4277. [Google Scholar] [CrossRef]
- Chaker, L.; Bianco, A.C.; Jonklaas, J.; Peeters, R.P. Hypothyroidism. Lancet 2017, 390, 1550. [Google Scholar] [CrossRef]
- Hypothyroidism|American Thyroid Association. Available online: https://www.thyroid.org/hypothyroidism/ (accessed on 12 December 2022).
- Triggiani, V.; Tafaro, E.; Giagulli, V.; Sabba, C.; Resta, F.; Licchelli, B.; Guastamacchia, E. Role of Iodine, Selenium and Other Micronutrients in Thyroid Function and Disorders. Endocr. Metab. Immune Disord. Drug Targets 2009, 9, 277–294. [Google Scholar] [CrossRef]
- Krishnamurthy, H.K.; Reddy, S.; Jayaraman, V.; Krishna, K.; Song, Q.; Rajasekaran, K.E.; Wang, T.; Bei, K.; Rajasekaran, J.J. Effect of Micronutrients on Thyroid Parameters. J. Thyroid. Res. 2021, 2021, 1865483. [Google Scholar] [CrossRef]
- Kapil, U. Health Consequences of Iodine Deficiency. Sultan Qaboos Univ. Med. J. 2007, 7, 267. [Google Scholar]
- Chung, H.R. Iodine and Thyroid Function. Ann. Pediatr. Endocrinol. Metab. 2014, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Farebrother, J.; Zimmermann, M.B.; Andersson, M. Excess Iodine Intake: Sources, Assessment, and Effects on Thyroid Function. Ann. N. Y. Acad. Sci. 2019, 1446, 44–65. [Google Scholar] [CrossRef] [PubMed]
- Abeysuriya, V.; Wickremasinghe, A.R.; Perera, P.J.; Kasturiratne, A. Consumption Pattern of Iodised Salt in Households and Serum TSH Levels among 5–9 year old Children in the Plantation Sector of Sri Lanka. Ceylon Med. J. 2012, 57, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Zaletel, K.; Gaberscek, S.; Pirnat, E. Ten-Year Follow-up of Thyroid Epidemiology in Slovenia after Increase in Salt Iodization. Croat. Med. J. 2011, 52, 615. [Google Scholar] [CrossRef] [PubMed]
- Pinto, E.; Gaberscek, S.; Okosieme, O.; Carare Candido, A.; Aparecida Vieira Ribeiro, S.; de Souza Macedo, M.; Aparecida Filomeno Fontes, E.; Carla Gomes De Souza, E.; Sonia Lopes Duarte, M.; Eloiza Priore, S.; et al. Is Dietary Iodine Intake Excessive According to the Theoretical Model of Healthy Dietary Intake Pattern in Pregnant Women and Schoolchildren: Water, Salt, or Food? Front. Nutr. 2021, 8, 770798. [Google Scholar] [CrossRef]
- Ravera, S.; Reyna-Neyra, A.; Ferrandino, G.; Amzel, L.M.; Carrasco, N. The Sodium/Iodide Symporter (NIS): Molecular Physiology and Preclinical and Clinical Applications. Annu. Rev. Physiol. 2017, 79, 261. [Google Scholar] [CrossRef] [PubMed]
- Kalarani, I.B.; Veerabathiran, R. Impact of Iodine Intake on the Pathogenesis of Autoimmune Thyroid Disease in Children and Adults. Ann. Pediatr. Endocrinol. Metab. 2022, 27, 256. [Google Scholar] [CrossRef] [PubMed]
- Dash, S.R.; O’Neil, A.; Jacka, F.N. Diet and Common Mental Disorders: The Imperative to Translate Evidence into Action. Front. Public Health 2016, 4, 81. [Google Scholar] [CrossRef] [PubMed]
- Shao, S.S.; Zhao, Y.F.; Song, Y.F.; Xu, C.; Yang, J.M.; Xuan, S.M.; Yan, H.L.; Yu, C.X.; Zhao, M.; Xu, J.; et al. Dietary High-Fat Lard Intake Induces Thyroid Dysfunction and Abnormal Morphology in Rats. Acta Pharmacol. Sin. 2014, 35, 1411. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, W.; Shao, S.; Xu, G.; Song, Y.; Xu, C.; Gao, L.; Hu, C.; Zhao, J. A High-Fat Diet Rich in Saturated and Mono-Unsaturated Fatty Acids Induces Disturbance of Thyroid Lipid Profile and Hypothyroxinemia in Male Rats. Mol. Nutr. Food Res. 2018, 62, 1700599. [Google Scholar] [CrossRef] [PubMed]
- Giannakou, M.; Saltiki, K.; Mantzou, E.; Loukari, E.; Philippou, G.; Terzidis, K.; Stavrianos, C.; Kyprianou, M.; Psaltopoulou, T.; Karatzi, K.; et al. The Effect of Obesity and Dietary Habits on Oxidative Stress in Hashimoto’s Thyroiditis. Endocr. Connect. 2018, 7, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Zupo, R.; Castellana, F.; Panza, F.; Lampignano, L.; Murro, I.; Di Noia, C.; Triggiani, V.; Giannelli, G.; Sardone, R.; De Pergola, G. Adherence to a Mediterranean Diet and Thyroid Function in Obesity: A Cross-Sectional Apulian Survey. Nutrients 2020, 12, 3173. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; Giovinazzo, S.; Barbalace, M.C.; Cristani, M.; Alibrandi, A.; Vicchio, T.M.; Giuffrida, G.; Aguennouz, M.H.; Malaguti, M.; Angeloni, C.; et al. Influence of Dietary Habits on Oxidative Stress Markers in Hashimoto’s Thyroiditis. Thyroid 2021, 31, 96–105. [Google Scholar] [CrossRef]
- Nation Center for Health Statistics. Vital and Health Statistics Series 2, Number 184 April 2020: Sample Design and Estimation Procedures Data Evaluation and Methods Research. 2015. Available online: https://www.cdc.gov/nchs/data/series/sr_02/sr02-184-508.pdf (accessed on 10 March 2023).
- Centers for Disease Control and Prevention (CDC). Demographic Variables and Sample Weights—Demographic Variables (2007–2008). National Health and Nutrition Examination Survey. Available online: https://wwwn.cdc.gov/nchs/nhanes/2007-2008/demo_e.htm (accessed on 10 March 2023).
- Centers for Disease Control and Prevention (CDC). Demographic Variables and Sample Weights—Demographic Variables (2009–2010). National Health and Nutrition Examination Survey. 2012. Available online: https://wwwn.cdc.gov/nchs/nhanes/search/DataPage.aspx?Component=Demographics&CycleBeginYear=2009 (accessed on 13 March 2023).
- Centers for Disease Control and Prevention (CDC). Demographic Variables and Sample Weights—Demographic Variables (2011–2012). National Health and Nutrition Examination Survey. 2013. Available online: https://wwwn.cdc.gov/nchs/nhanes/search/variablelist.aspx?Component=Demographics&Cycle=2011-2012 (accessed on 13 March 2023).
- AMPM—USDA Automated Multiple-Pass Method: USDA ARS. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/ampm-usda-automated-multiple-pass-method/. (accessed on 12 November 2023).
- Shin, D.; Lee, K.W.; Song, W.O. Dietary Patterns during Pregnancy Are Associated with Risk of Gestational Diabetes Mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef]
- Nation Center for Health Statistics. Laboratory Procedure Manual Thyroid Stimulating Hormone (TSH). Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_01_02/l18t4_b_met_b_tsh.pdf (accessed on 10 March 2023).
- Ogden, C.L.; Carroll, M.D.; Lawman, H.G.; Fryar, C.D.; Kruszon-Moran, D.; Kit, B.K.; Flegal, K.M. Trends in Obesity Prevalence Among Children and Adolescents in the United States, 1988–1994 Through 2013–2014. JAMA 2016, 315, 2292–2299. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Physical Activity (PAQ)-Data Documentation, Codebook, and Frequencies (2011–2012). National Health and Nutrition Examination Survey. 2012. Available online: https://wwwn.cdc.gov/nchs/nhanes/search/DataPage.aspx?Component=Examination&CycleBeginYear=2011 (accessed on 13 March 2023).
- Ganji, V.; Shi, Z.; Al-Abdi, T.; Al Hejap, D.; Attia, Y.; Koukach, D.; Elkassas, H. Association between Food Intake Patterns and Serum Vitamin D Concentrations in US Adults. Br J Nutr 2023, 129, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Kopp, W. How Western Diet And Lifestyle Drive The Pandemic of Obesity And Civilization Diseases. Diabetes Metab. Syndr. Obes. 2019, 12, 2221. [Google Scholar] [CrossRef] [PubMed]
- Statovci, D.; Aguilera, M.; MacSharry, J.; Melgar, S. The Impact of Western Diet and Nutrients on the Microbiota and Immune Response at Mucosal Interfaces. Front. Immunol. 2017, 8, 838. [Google Scholar] [CrossRef] [PubMed]
- Myles, I.A. Fast Food Fever: Reviewing the Impacts of the Western Diet on Immunity. Nutr. J. 2014, 13, 61. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Xue, S.; Zhang, L.; Chen, G. Trace Elements and the Thyroid. Front. Endocrinol. 2022, 13, 904889. [Google Scholar] [CrossRef] [PubMed]
- Krajcovicova-Kudlackova, M.; Bučková, K.; Klimeš, I.; Šeboková, E. Iodine Deficiency in Vegetarians and Vegans. Ann. Nutr. Metab. 2003, 47, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Sorrenti, S.; Baldini, E.; Pironi, D.; Lauro, A.; D’Orazi, V.; Tartaglia, F.; Tripodi, D.; Lori, E.; Gagliardi, F.; Praticò, M.; et al. Iodine: Its Role in Thyroid Hormone Biosynthesis and Beyond. Nutrients 2021, 13, 4469. [Google Scholar] [CrossRef]
- Vitamin B12—Health Professional Fact Sheet. Available online: https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/ (accessed on 11 February 2023).
- Kaličanin, D.; Brčić, L.; Ljubetić, K.; Barić, A.; Gračan, S.; Brekalo, M.; Torlak Lovrić, V.; Kolčić, I.; Polašek, O.; Zemunik, T.; et al. Differences in Food Consumption between Patients with Hashimoto’s Thyroiditis and Healthy Individuals. Sci. Rep. 2020, 10, 10670. [Google Scholar] [CrossRef]
- Appunni, S.; Rubens, M.; Ramamoorthy, V.; Saxena, A.; Tonse, R.; Veledar, E.; McGranaghan, P. Association between Vitamin D Deficiency and Hypothyroidism: Results from the National Health and Nutrition Examination Survey (NHANES) 2007–2012. BMC Endocr. Disord. 2021, 21, 224. [Google Scholar] [CrossRef]
- Siriwardhana, N.; Kalupahana, N.S.; Moustaid-Moussa, N. Health Benefits of N-3 Polyunsaturated Fatty Acids: Eicosapentaenoic Acid and Docosahexaenoic Acid. Adv. Food Nutr. Res. 2012, 65, 211–222. [Google Scholar] [CrossRef]
- Chakrabarti, S.K.; Ghosh, S.; Banerjee, S.; Mukherjee, S.; Chowdhury, S. Oxidative Stress in Hypothyroid Patients and the Role of Antioxidant Supplementation. Indian. J. Endocrinol. Metab. 2016, 20, 674. [Google Scholar] [CrossRef]
- Sakai, K.; Kino, S.; Takeuchi, M.; Ochi, T.; Da Cruz, G.; Tomita, I. Analysis of Antioxidant Activities in Vegetable Oils and Fat Soluble Vitamins and Biofactors by the PAO-SO Method. Methods Mol. Biol. 2010, 594, 241–250. [Google Scholar] [CrossRef]
- Pang, K.L.; Lumintang, J.N.; Chin, K.Y. Thyroid-Modulating Activities of Olive and Its Polyphenols: A Systematic Review. Nutrients 2021, 13, 529. [Google Scholar] [CrossRef]
- Lichtenstein, A.H.; Appel, L.J.; Vadiveloo, M.; Hu, F.B.; Kris-Etherton, P.M.; Rebholz, C.M.; Sacks, F.M.; Thorndike, A.N.; Van Horn, L.; Wylie-Rosett, J. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e472–e487. [Google Scholar] [CrossRef]
- Astrup, A.; Magkos, F.; Bier, D.M.; Brenna, J.T.; de Oliveira Otto, M.C.; Hill, J.O.; King, J.C.; Mente, A.; Ordovas, J.M.; Volek, J.S.; et al. Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 844–857. [Google Scholar] [CrossRef]
- Gershuni, V.M. Saturated Fat: Part of a Healthy Diet. Curr. Nutr. Rep. 2018, 7, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Vega-Vega, O.; Fonseca-Correa, J.I.; Mendoza-De la Garza, A.; Rincón-Pedrero, R.; Espinosa-Cuevas, A.; Baeza-Arias, Y.; Dary, O.; Herrero-Bervera, B.; Nieves-Anaya, I.; Correa-Rotter, R. Contemporary Dietary Intake: Too Much Sodium, Not Enough Potassium, yet Sufficient Iodine: The SALMEX Cohort Results. Nutrients 2018, 10, 816. [Google Scholar] [CrossRef] [PubMed]
- Academy of Nutrition and Dietetics Iodine: A Critically Important Nutrient. Available online: https://www.eatright.org/health/essential-nutrients/minerals/iodine-a-critically-important-nutrient (accessed on 12 March 2023).
- Barrea, L.; Muscogiuri, G.; de Alteriis, G.; Porcelli, T.; Vetrani, C.; Verde, L.; Aprano, S.; Fonderico, F.; Troncone, G.; Colao, A.; et al. Adherence to the Mediterranean Diet as a Modifiable Risk Factor for Thyroid Nodular Disease and Thyroid Cancer: Results From a Pilot Study. Front. Nutr. 2022, 9, 944200. [Google Scholar] [CrossRef] [PubMed]
- De Santis, S.; Liso, M.; Verna, G.; Curci, F.; Milani, G.; Faienza, M.F.; Franchini, C.; Moschetta, A.; Chieppa, M.; Clodoveo, M.L.; et al. Extra Virgin Olive Oil Extracts Modulate the Inflammatory Ability of Murine Dendritic Cells Based on Their Polyphenols Pattern: Correlation between Chemical Composition and Biological Function. Antioxidants 2021, 10, 1016. [Google Scholar] [CrossRef]
- Wojtas, N.; Wadolowska, L.; Bandurska-Stankiewicz, E. Evaluation of Qualitative Dietary Protocol (Diet4Hashi) Application in Dietary Counseling in Hashimoto Thyroiditis: Study Protocol of a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4841. [Google Scholar] [CrossRef]
- Ros, E. Health Benefits of Nut Consumption. Nutrients 2010, 2, 652. [Google Scholar] [CrossRef] [PubMed]
- Gorini, F.; Sabatino, L.; Pingitore, A.; Vassalle, C. Selenium: An Element of Life Essential for Thyroid Function. Molecules 2021, 26, 7084. [Google Scholar] [CrossRef]
- Bellastella, G.; Scappaticcio, L.; Caiazzo, F.; Tomasuolo, M.; Carotenuto, R.; Caputo, M.; Arena, S.; Caruso, P.; Maiorino, M.I.; Esposito, K. Mediterranean Diet and Thyroid: An Interesting Alliance. Nutrients 2022, 14, 4130. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Scientific Update on the Iodine Content of Portuguese Foods; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Marangoni, F.; Corsello, G.; Cricelli, C.; Ferrara, N.; Ghiselli, A.; Lucchin, L.; Poli, A. Role of Poultry Meat in a Balanced Diet Aimed at Maintaining Health and Wellbeing: An Italian Consensus Document. Food Nutr. Res. 2015, 59, 27606. [Google Scholar] [CrossRef] [PubMed]
- Poultry in Human Nutrition|Gateway to Poultry Production and Products|Food and Agriculture Organization of the United Nations. Available online: https://www.fao.org/poultry-production-products/products-processing/poultry-in-human-nutrition/en/ (accessed on 13 February 2023).
- Réhault-Godbert, S.; Guyot, N.; Nys, Y. The Golden Egg: Nutritional Value, Bioactivities, and Emerging Benefits for Human Health. Nutrients 2019, 11, 684. [Google Scholar] [CrossRef]
- Åsgård, R.; Rytter, E.; Basu, S.; Abramsson-Zetterberg, L.; Möller, L.; Vessby, B. High Intake of Fruit and Vegetables Is Related to Low Oxidative Stress and Inflammation in a Group of Patients with Type 2 Diabetes. Scand. J. Food Nutr. 2007, 51, 149. [Google Scholar] [CrossRef]
- Bacchetti, T.; Turco, I.; Urbano, A.; Morresi, C.; Ferretti, G. Relationship of Fruit and Vegetable Intake to Dietary Antioxidant Capacity and Markers of Oxidative Stress: A Sex-Related Study. Nutrition 2019, 61, 164–172. [Google Scholar] [CrossRef]
- Khan, H.; Sureda, A.; Belwal, T.; Çetinkaya, S.; Süntar, İ.; Tejada, S.; Devkota, H.P.; Ullah, H.; Aschner, M. Polyphenols in the Treatment of Autoimmune Diseases. Autoimmun. Rev. 2019, 18, 647. [Google Scholar] [CrossRef]
- Bakırhan, H.; Özyürek Arpa, F.; Uğur, H.; Pehlivan, M.; Saleki, N.; Çelik, T. Metabolic Risks and Prognosis of COVID-19: Are Dietary Patterns Important? Nutr. Food Sci. 2023, 53, 752–768. [Google Scholar] [CrossRef]
- Brouwer-Brolsma, E.M.; Brandl, B.; Buso, M.E.C.; Skurk, T.; Manach, C. Food Intake Biomarkers for Green Leafy Vegetables, Bulb Vegetables, and Stem Vegetables: A Review. Genes. Nutr. 2020, 15, 7. [Google Scholar] [CrossRef] [PubMed]
- Amagloh, F.K.; Atuna, R.A.; McBride, R.; Carey, E.E.; Christides, T. Nutrient and Total Polyphenol Contents of Dark Green Leafy Vegetables, and Estimation of Their Iron Bioaccessibility Using the In Vitro Digestion/Caco-2 Cell Model. Foods 2017, 6, 54. [Google Scholar] [CrossRef] [PubMed]
- Capriello, S.; Stramazzo, I.; Bagaglini, M.F.; Brusca, N.; Virili, C.; Centanni, M. The Relationship between Thyroid Disorders and Vitamin, A.: A Narrative Minireview. Front Endocrinol. 2022, 13, 968215. [Google Scholar] [CrossRef] [PubMed]
- King, J.C.; Slavin, J.L. White Potatoes, Human Health, and Dietary Guidance. Adv. Nutr. 2013, 4, 393S. [Google Scholar] [CrossRef] [PubMed]
- Tonstad, S.; Nathan, E.; Oda, K.; Fraser, G. Vegan Diets and Hypothyroidism. Nutrients 2013, 5, 4642. [Google Scholar] [CrossRef]
- Otun, J.; Sahebkar, A.; Östlundh, L.; Atkin, S.L.; Sathyapalan, T. Systematic Review and Meta-Analysis on the Effect of Soy on Thyroid Function. Sci. Rep. 2019, 9, 3964. [Google Scholar] [CrossRef]
- Wiesner, A.; Gajewska, D.; Paśko, P. Levothyroxine Interactions with Food and Dietary Supplements–A Systematic Review. Pharmaceuticals 2021, 14, 206. [Google Scholar] [CrossRef]
- Chon, D.A.; Reisman, T.; Weinreb, J.E.; Hershman, J.M.; Leung, A.M. Concurrent Milk Ingestion Decreases Absorption of Levothyroxine. Thyroid 2018, 28, 454–457. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| FPED 2011–2012 Food Group | Modified FPED 2011–2012 Subgroups |
|---|---|
| Fruits | Citrus, melons, and berries Other fruits Fruit juice |
| Vegetables | Dark-green vegetables Tomatoes Other red and orange vegetables Potatoes Other starchy vegetables Other vegetables Beans and peas are computed as vegetables |
| Grains | Whole grains Refined grains |
| Protein foods | Meat (beef, veal, pork, lamb, game) Cured meat (frankfurters, sausage, corned beef, cured ham and luncheon meat made from beef, pork, poultry) Organ meat (from beef, veal, pork, lamb, game, poultry) Poultry (chicken, turkey, other fowl) Seafood high in n-3 fatty acids Seafood low in n-3 fatty acids Eggs Soybean products (excludes Ca-fortified soy milk and mature soybeans) Nuts and seeds |
| Dairy | Milk (includes Ca-fortified soy milk) Yogurt Cheese |
| Oils | Oils |
| Solid fats | Solid fats |
| Added sugars | Added sugars |
| Alcoholic drinks | Alcoholic beverages |
| Characteristics | Total 3 | Normal 3 | Hypothyroidism 3 | p-Value 4 |
|---|---|---|---|---|
| n = 8317 | (≤4.5 mIU/L) n = 7555 | (>4.5 mIU/L) n = 762 | ||
| Energy intake, kcal | 2092 ± 930 | 2118 ± 939 | 1829 ± 792 | <0.001 |
| Age, y | 48.6 ± 18.6 | 47.5 ± 18.4 | 59.5 ± 17.2 | <0.001 |
| Sex | <0.001 | |||
| Men, n (%) | 4220 (50.7) | 3972 (52.6) | 248 (32.5) | |
| Women, n (%) | 4097 (49.3) | 3583 (47.4) | 514 (67.5) | |
| Race/ethnicity | <0.001 | |||
| Non-Hispanic white, n (%) | 3851 (46.3) | 3337 (44.2) | 514 (67.5) | |
| Non-Hispanic black, n (%) | 1655 (19.9) | 1599 (21.2) | 56 (7.3) | |
| Mexican American/Hispanic, n (%) | 1365 (16.4) | 1264 (16.7) | 101 (13.3) | |
| Other races/ethnicities, n (%) | 1446 (17.4) | 1355 (17.9) | 91 (11.9) | |
| Education | 0.43 | |||
| <11 grade, n (%) | 2262 (28.6) | 2058 (28.7) | 204 (27.2) | |
| High school/GED, n (%) | 1848 (23.3) | 1671 (23.3) | 177 (23.6) | |
| Some college, n (%) | 2171 (27.4) | 1973 (27.5) | 198 (26.4) | |
| >College, n (%) | 1635 (20.7) | 1464 (20.4) | 171 (22.8) | |
| Smoking status | <0.001 | |||
| Never, n (%) | 4231 (50.9) | 3820 (50.6) | 411 (53.9) | |
| Former, n (%) | 2013 (24.2) | 1785 (23.6) | 228 (29.9) | |
| Current smoker, n (%) | 1677 (20.2) | 1565 (20.7) | 112 (14.7) | |
| Not reported, n (%) | 396 (4.8) | 385 (5.1) | 11 (1.4) | |
| Alcohol drinking (past 12 months) | <0.001 | |||
| No, n (%) | 1447 (17.4) | 1278 (16.9) | 169 (22.2) | |
| Yes, n (%) | 5019 (60.3) | 4598 (60.9) | 421 (55.2) | |
| Not reported, n (%) | 1851 (22.3) | 1679 (22.2) | 172 (22.6) | |
| Body mass index, kg/m2 | 28.8 ± 6.7 | 28.7 ± 6.7 | 29.9 ± 7.3 | <0.001 |
| Physical activity, METs min/wk | <0.001 | |||
| <600, n (%) | 3343 (40.2) | 2949 (39) | 394 (51.7) | |
| 600–1200, n (%) | 849 (10.2) | 759 (10) | 90 (11.8) | |
| ≥1200, n (%) | 4124 (49.6) | 3846 (50.9) | 278 (36.5) | |
| Poverty–income ratio | 0.007 | |||
| <1.30, n (%) | 2424 (29.1) | 2238 (29.6) | 186 (24.4) | |
| 1.3–3.5, n (%) | 2869 (34.5) | 2583 (34.2) | 286 (37.5) | |
| >3.5, n (%) | 2307 (27.7) | 2079 (27.5) | 228 (29.9) | |
| Not reported, n (%) | 717 (8.6) | 655 (8.7) | 62 (8.1) | |
| Hypertension | 2873 (35.6) | 2496 (34.1) | 377(50.4) | <0.001 |
| Food Group 3 | Factor 1 | Factor 2 | Factor 3 |
|---|---|---|---|
| Solid fats (g) | 0.83 | ||
| Refined or non-whole grains | 0.71 | ||
| Cheese (cup) | 0.67 | ||
| Foods defined as added sugars | 0.46 | ||
| Cured/luncheon meat | 0.35 | ||
| Tomatoes and tomato products | 0.34 | 0.28 | |
| Beef, veal, pork, lamb, game | 0.3 | ||
| Oils (g) | 0.21 | 0.81 | |
| Peanuts, tree nuts, and seeds | 0.54 | ||
| White potatoes (cup) | 0.41 | −0.35 | |
| Other vegetables | 0.38 | 0.37 | |
| Chicken, turkey, Cornish hens | 0.34 | ||
| Eggs (chicken, duck, goose) | 0.27 | ||
| Seafood (finfish, shellfish) | 0.26 | ||
| Intact fruits (whole or cut) | 0.51 | ||
| Whole grains (oz) | 0.48 | ||
| Other red and orange vegetables | 0.38 | ||
| Dark-green vegetables (cup) | 0.22 | 0.32 | |
| Yogurt (cup) | 0.29 | ||
| Intact fruits (whole or cut) | 0.29 | ||
| Fluid milk and calcium-fortified | 0.27 | ||
| Soy products | 0.24 | ||
| Legumes computed as vegetables | 0.23 | ||
| Variance explained (%) | 9.3 | 6.6 | 4.8 |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| Food Patterns 4 | OR (95% CI) | p-Value 3 | OR (95% CI) | p-Value 3 | OR (95% CI) | p-Value 3 |
| FPSM | 0.91 (0.68–1.22) | 0.52 | 0.79 (0.6–1.03) | 0.076 | 0.75 (0.5–7.1) | 0.049 |
| ONPL | 0.92 (0.77–1.09) | 0.32 | 0.83 (0.69–0.99) | 0.037 | 0.81 (0.67–0.97) | 0.025 |
| FWVD | 1.06 (0.95–1.19) | 0.3 | 1.01 (0.9–1.14) | 0.84 | 1.03 (0.91–1.16) | 0.63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alkhatib, D.; Shi, Z.; Ganji, V. Dietary Patterns and Hypothyroidism in U.S. Adult Population. Nutrients 2024, 16, 382. https://doi.org/10.3390/nu16030382
Alkhatib D, Shi Z, Ganji V. Dietary Patterns and Hypothyroidism in U.S. Adult Population. Nutrients. 2024; 16(3):382. https://doi.org/10.3390/nu16030382
Chicago/Turabian StyleAlkhatib, Dana, Zumin Shi, and Vijay Ganji. 2024. "Dietary Patterns and Hypothyroidism in U.S. Adult Population" Nutrients 16, no. 3: 382. https://doi.org/10.3390/nu16030382
APA StyleAlkhatib, D., Shi, Z., & Ganji, V. (2024). Dietary Patterns and Hypothyroidism in U.S. Adult Population. Nutrients, 16(3), 382. https://doi.org/10.3390/nu16030382