

Malnutrition as a Risk Factor in the Development of Oral Cancer: A Systematic Literature Review and Meta-Analyses

 , , ,
, , ,  , , ,
, , ,  and
and
Abstract
1. Introduction
- Primary malnutrition, linked to the availability and intake of food;
- Secondary malnutrition, resulting from specific physiological (e.g., pregnancy, lactation, febrile states) and pathological conditions that impair digestion and nutrient absorption [6].
2. Materials and Methods
2.1. Study Objective and PECOS Model
- P. Population/problem/patient: adult patients not affected by any systemic disease;
- E. Exposure: patients exposed to primary or secondary malnutrition due to different causes;
- C. Comparison: the incidence of oral cancer in healthy subjects and in patients not affected by primary or secondary malnutrition;
- O. Outcome: development of oral carcinoma;
- S. Study design: cohort studies, case–control studies, cross-sectional studies, and randomized clinical trials (RCTs) with no fewer than 10 patients.
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
Electronic Search
Manual Search
Unpublished Articles
2.2. Study Selection
2.2.1. Data Extraction
2.2.2. Quality Assessment
2.2.3. Heterogeneity Assessment
- 0−40%: negligible;
- 30−60%: moderate;
- 50−90%: substantial;
- 75−100%: considerable [14].
2.3. Data Analysis
3. Results
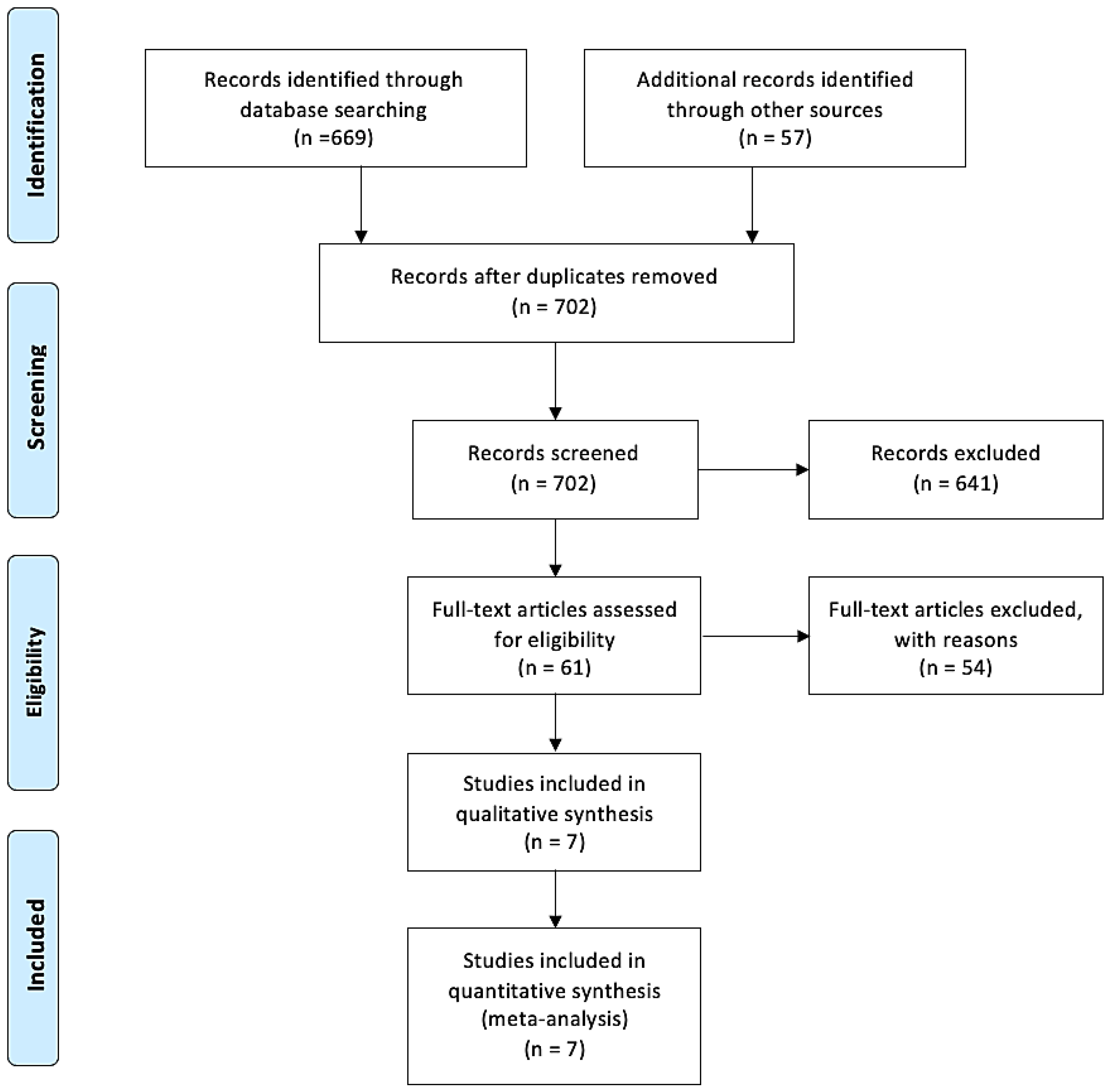
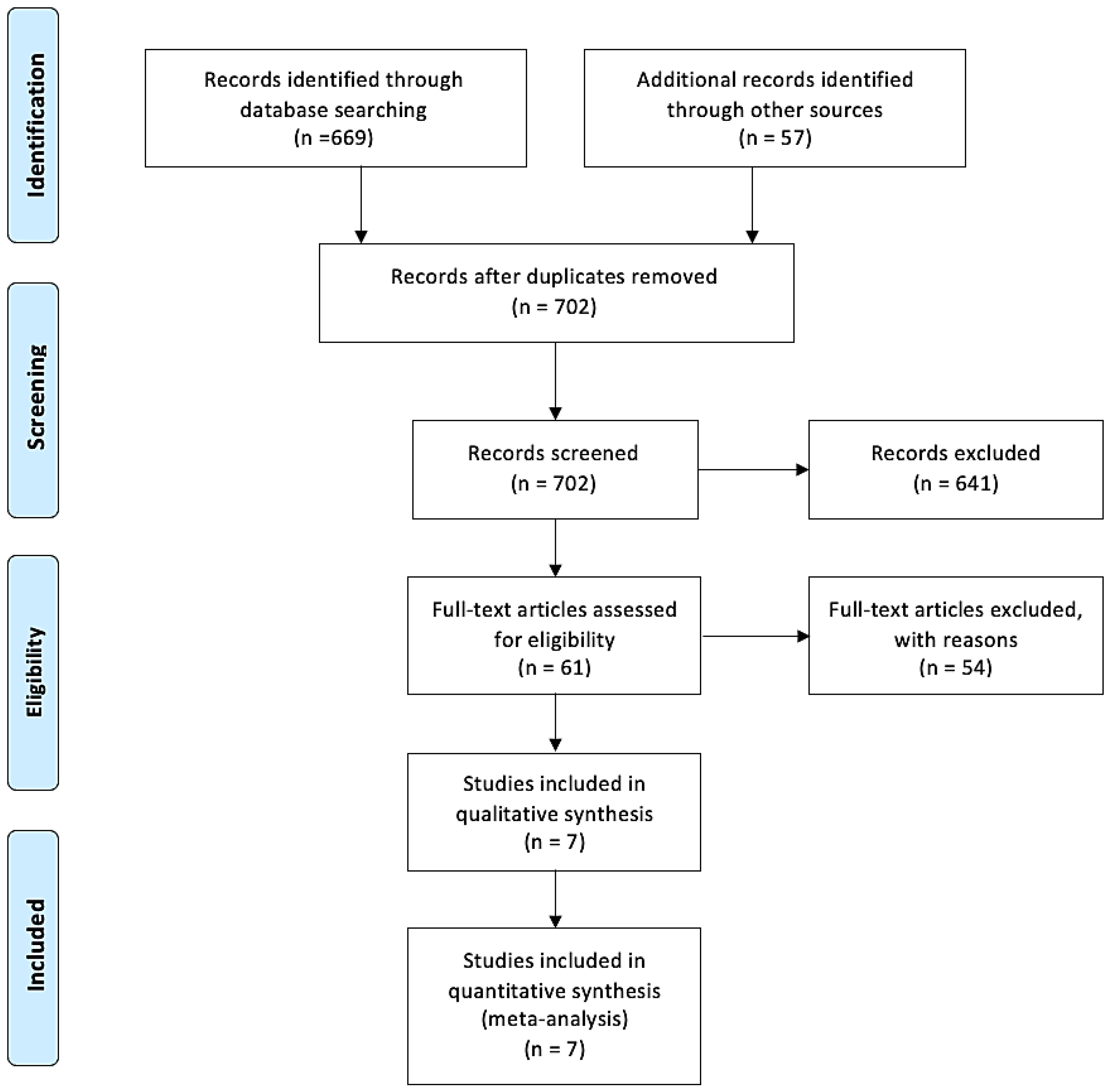
3.1. Study Selection
3.2. Study Characteristics
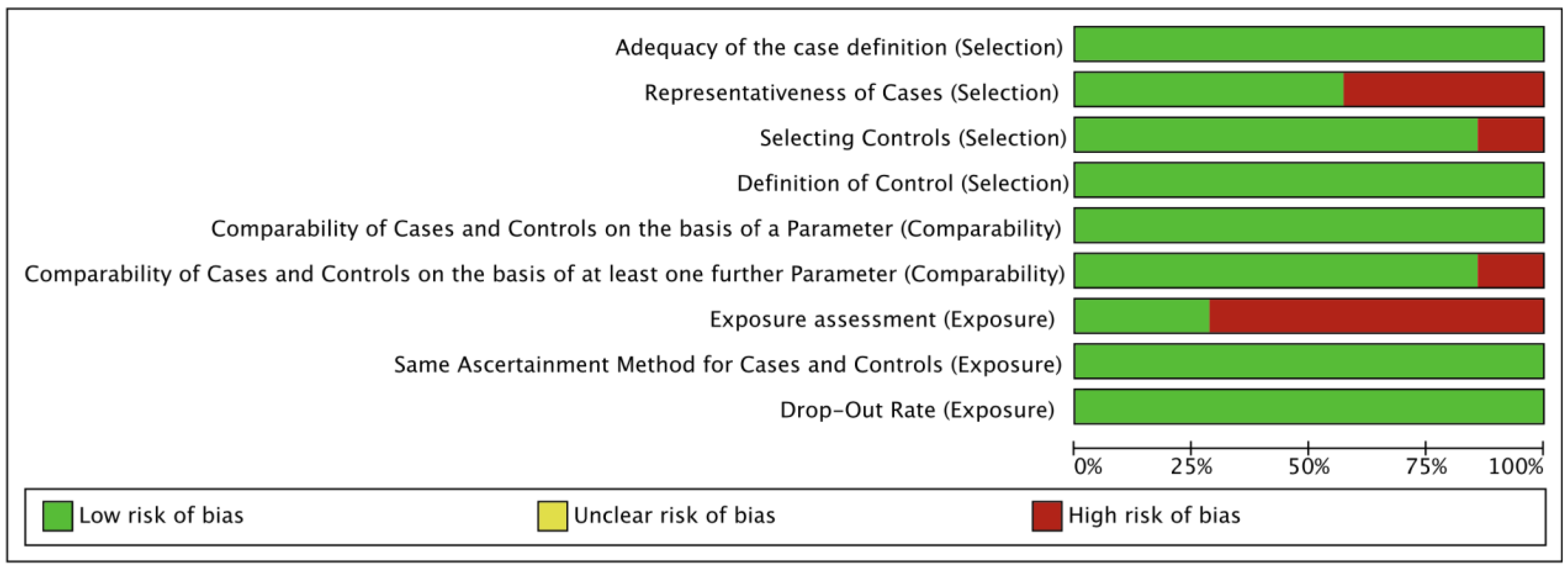
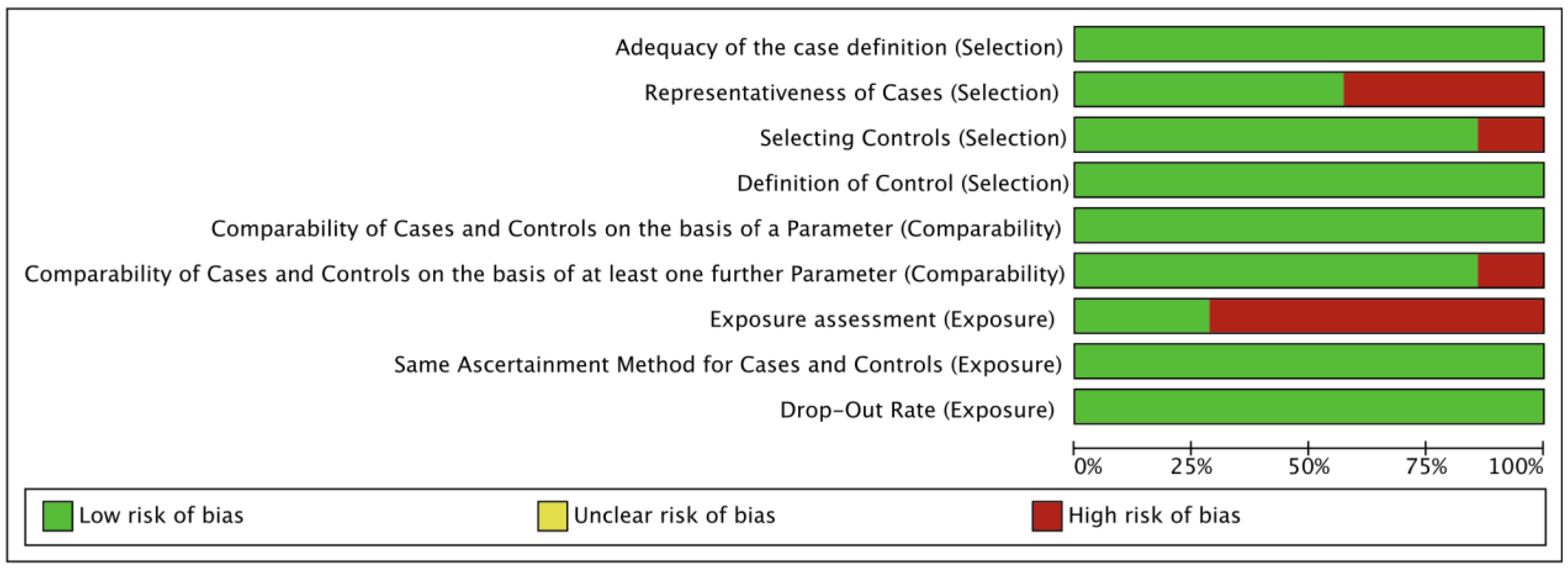
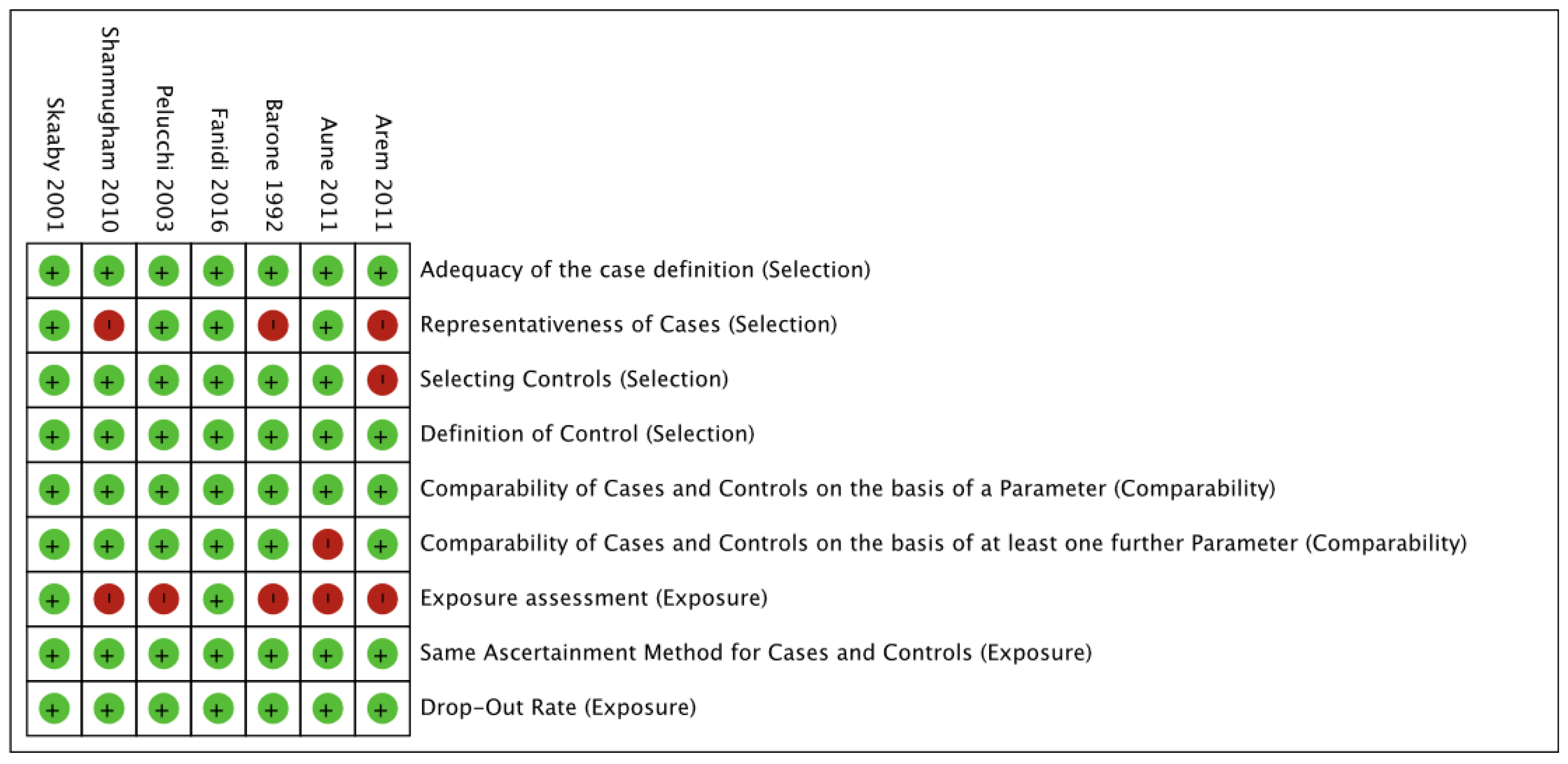
3.3. Risk of Bias Assessment
3.4. Results of the Meta-Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sarode, G.; Maniyar, N.; Sarode, S.C.; Jafer, M.; Patil, S.; Awan, K.H. Epidemiologic aspects of oral cancer. Dis. A Mon. 2020, 66, 100988. [Google Scholar] [CrossRef]
- Schantz, S.P.; Yu, G.P. Head and Neck Cancer Incidence Trends in Young Americans, 1973–1997, with a Special Analysis for Tongue Cancer. Arch. Otolaryngol. Neck Surg. 2002, 128, 268–274. [Google Scholar] [CrossRef]
- Neville, B.W.; Damm, D.D.; Allen, C.M.B.J. Oral and Maxillofacial Pathology, 2nd ed.; Elsevier: Philadelphia, PA, USA, 2002. [Google Scholar]
- Meza-Valderrama, D.; Marco, E.; Dávalos-Yerovi, V.; Muns, M.D.; Tejero-Sánchez, M.; Duarte, E.; Sánchez-Rodríguez, D. Sarcopenia, Malnutrition, and Cachexia: Adapting Definitions and Terminology of Nutritional Disorders in Older People with Cancer. Nutrition 2021, 13, 761. [Google Scholar] [CrossRef]
- Bhattacharyya, A.K. Protein-Energy Malnutrition (Kwashiorkor-Marasmus Syndrome): Terminology, Classification and Evolution. World Rev. Nutr. Diet. 1986, 47, 80–133. [Google Scholar]
- Shahrin, L.; Chisti, M.J.; Ahmed, T. 3.1 Primary and Secondary Malnutrition. World Rev. Nutr. Diet. 2015, 113, 139–146. [Google Scholar]
- Pham, T.P.T.; Alou, M.T.; Golden, M.H.; Million, M.; Raoult, D. Difference between kwashiorkor and marasmus: Comparative meta-analysis of pathogenic characteristics and implications for treatment. Microb. Pathog. 2021, 150, 104702. [Google Scholar] [CrossRef] [PubMed]
- Kang, I.; Kim, Y.S.; Kim, C. Mineral deficiency in patients who have undergone gastrectomy. Nutrition 2007, 23, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Triggiani, V.; Tafaro, E.; Giagulli, V.A.; Sabbà, C.; Resta, F.; Licchelli, B.; Guastamacchia, E. Role of Iodine, Selenium and Other Micronutrients in Thyroid Function and Disorders. Endocr. Metab. Immune Disord. Drug Targets 2009, 9, 277–294. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Medica 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- RevMan. Available online: https://revman.cochrane.org/#/myReviews (accessed on 20 November 2023).
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Barone, J.; Taioli, E.; Hebert, J.R.; Wynder, E. Vitamin supplement use and risk for oral and esophageal cancer. Nutr. Cancer 1992, 18, 31–41. [Google Scholar] [CrossRef]
- Skaaby, T.; Husemoen, L.L.; Thuesen, B.H.; Pisinger, C.; Jørgensen, T.; Roswall, N.; Larsen, S.C.; Linneberg, A. Prospective population-based study of the association between serum 25-hydroxyvitamin-D levels and the incidence of specific types of cancer. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1220–1229. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Talamini, R.; Negri, E.; Levi, F.; Conti, E.; Franceschi, S.; La Vecchia, C. Folate intake and risk of oral and pharyngeal cancer. Ann. Oncol. 2003, 14, 1677–1681. [Google Scholar] [CrossRef]
- Shanmugham, J.R.; Zavras, A.I.; Rosner, B.A.; Giovannucci, E.L. Alcohol-folate interactions in the risk of oral cancer in women: A prospective cohort study. Cancer Epidemiol. Biomarkers Prev. 2010, 19, 2516–2524. [Google Scholar] [CrossRef]
- Arem, H.; Weinstein, S.J.; Horst, R.L.; Virtamo, J.; Yu, K.; Albanes, D.; Abnet, C.C. Serum 25-hydroxyvitamin D and risk of oropharynx and larynx cancers in Finnish men. Cancer Epidemiol. Biomark Prev. 2011, 20, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Deneo-Pellegrini, H.; Ronco, A.L.; Boffetta, P.; Acosta, G.; Mendilaharsu, M.; De Stefani, E. Dietary folate intake and the risk of 11 types of cancer: A case-control study in Uruguay. Ann. Oncol. 2011, 22, 444–451. [Google Scholar] [CrossRef]
- Fanidi, A.; Muller, D.C.; Midttun, Ø.; Ueland, P.M.; Vollset, S.E.; Relton, C.; Vineis, P.; Weiderpass, E.; Skeie, G.; Brustad, M.; et al. Circulating vitamin D in relation to cancer incidence and survival of the head and neck and oesophagus in the EPIC cohort. Sci. Rep. 2016, 6, 36017. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Maggini, S. Vitamin C and Immune Function. Nutrition 2017, 9, 1211. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.; Yu, S.; Zhang, S.; Ding, X.; Su, J.; Cheng, Z. Association between folate intake and risk of head and neck squamous cell carcinoma. Medicine 2017, 96, e8182. [Google Scholar] [CrossRef] [PubMed]
- Clerge, T. Handbook of Vitamins, 4th ed.; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Norman, A.W. From vitamin D to hormone D: Fundamentals of the vitamin D endocrine system essential for good health. Am. J. Clin. Nutr. 2008, 88, 491S–499S. [Google Scholar] [CrossRef] [PubMed]
- Adorini, L.; Giarratana, N.; Penna, G. Pharmacological induction of tolerogenic dendritic cells and regulatory T cells. Semin. Immunol. 2004, 16, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Wallace, J.M.; Horigan, G.; Hill, T.R.; Barnes, M.S.; Lucey, A.J.; Bonham, M.P.; Taylor, N.; Duffy, E.M.; Seamans, K.; et al. Estimation of the dietary requirement for vitamin D in free-living adults ≥64 y of age. Am. J. Clin. Nutr. 2009, 89, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.; Conry-Cantilena, C.; Wang, Y.; Welch, R.W.; Washko, P.W.; Dhariwal, K.R.; Park, J.B.; Lazarev, A.; Graumlich, J.F.; King, J.; et al. Vitamin C pharmacokinetics in healthy volunteers: Evidence for a recommended dietary allowance. Proc. Natl. Acad. Sci. USA 1996, 93, 3704–3709. [Google Scholar] [CrossRef]
- Lippman, S.M.; Meyskens, F.L., Jr. Vitamin A derivatives in the prevention and treatment of human cancer. J. Am. Coll. Nutr. 1988, 7, 269–284. [Google Scholar] [CrossRef]
- Basu, T.K. Vitamin A and cancer of epithelial origin. J. Hum. Nutr. 1979, 33, 24–31. [Google Scholar] [CrossRef]
- See, J.K.L.; Liu, X.; Canfora, F.; Moore, C.; McCullough, M.; Yap, T.; Paolini, R.; Celentano, A. The Role of Vitamins in Oral Potentially Malignant Disorders and Oral Cancer: A Systematic Review. J. Pers. Med. 2023, 13, 1520. [Google Scholar] [CrossRef]
- Bravi, F.; Bosetti, C.; Filomeno, M.; Levi, F.; Garavello, W.; Galimberti, S.; Negri, E.; La Vecchia, C. Foods, nutrients and the risk of oral and pharyngeal cancer. Br. J. Cancer 2013, 109, 2904–2910. [Google Scholar] [CrossRef]
- Ziegler, R.G. Vegetables, fruits, and carotenoids and the risk of cancer. Am. J. Clin. Nutr. 1991, 53 (Suppl. S1), 251S–259S. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Negri, E.; Franceschi, S.; Conti, E.; Levi, F.; Tomei, F.; La Vecchia, C. Risk factors for oral and pharyngeal cancer in women: A study from Italy and Switzerland. Br. J. Cancer 2000, 82, 204–207. [Google Scholar] [CrossRef] [PubMed]
- Kune, G.A.; Kune, S.; Field, B.; Watson, L.F.; Cleland, H.; Merenstein, D.; Vitetta, L. Oral and pharyngeal cancer, diet, smoking, alcohol, and serum vitamin A and beta-carotene levels: A case-control study in men. Nutr. Cancer 1993, 20, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Middleton, B.; Byers, T.; Marshall, J.; Graham, S. Dietary vitamin A and cancer--a multisite case-control study. Nutr. Cancer 1986, 8, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Negri, E.; Franceschi, S.; Bosetti, C.; Levi, F.; Conti, E.; Parpinel, M.; La Vecchia, C. Selected micronutrients and oral and pharyngeal cancer. Int. J. Cancer 2000, 86, 122–127. [Google Scholar] [CrossRef]
- Zhao, H.; Jin, X. Causal associations between dietary antioxidant vitamin intake and lung cancer: A Mendelian randomization study. Front. Nutr. 2022, 9, 965911. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors–Year | Place of Publication | Study Design | Number of Patients | Analyzed Micronutrient | Patients with SCC | Study Objective | Years of Follow-Up | Results |
|---|---|---|---|---|---|---|---|---|
| Barone (1992) [16] | USA | R | 870 | Vitamin C and E | 290 | Use of vitamin supplements and the risk of oral and esophageal carcinogenesis | 0 | It was noted that the intake of vitamin C and E acts as a protective factor in the onset of oral and esophageal cancer. |
| Skaaby (2001) [17] | Denmark | P | 12,204 | Vitamin D | 1248 | Correlation between blood vitamin D concentration and generalized risk of carcinogenesis | 11.3 | There was no observed increase in the risk of a specific tumor, but a generalized risk of the development of neoplasms. |
| Pelucchi (2003) [18] | Italy and French Switzerland | R | 2521 | Folic acid | 749 | To assess whether daily intake of folic acid is considered a protective factor for SCC | 5 | Low intake of folic acid and alcohol consumption increase the risk of SCC. |
| Shanmugham (2010) [19] | USA | P | 87,621 | Folic acid | 147 | Quantifying folate intake as a risk factor for the development of SCC | 26 | Patients who consume >30 g/day of alcohol and <350 μg/day of folate have a 20% increased risk of developing SCC. |
| Arem (2011) [20] | Finland | P | 29,133 | Vitamin D | 348 | Assessing serum vitamin D concentrations as a risk factor for the development of HN tumors | 20 | No correlation was found between low serum levels and an increased incidence of HNC. |
| Aune (2011) [21] | Uruguay | R | 5571 | Folic acid | 3539 | Folic acid as a protective factor against 11 types of cancer | 8 | There is a significant reduction in the incidence of oral and pharyngeal SCC in patients with adequate folate intake. |
| Fanidi (2016) [22] | Europe | P | 385,747 | Vitamin D | 497 | Correlation between circulating vitamin D and the incidence and survival of SCC | 8 | Reduced levels of circulating vitamin D are correlated with an increase in the incidence of laryngeal, hypopharyngeal, and oral cancer. |
| Quality Assessment Outcome: Oral Cancer Incidence in Patients with Malnutrition | ||||||
|---|---|---|---|---|---|---|
| Question: Does malnutrition have an influence on oral cancer incidence? | ||||||
| Number of studies according to meta-analysis | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias |
| Meta-analysis on folate effects (3 studies) | cohort and case–control studies | medium | serious (a) | serious (b) | not serious | N/A |
| Meta-analysis on vitamin C effects (1 study) | case–control study | medium | N/A | serious (b) | not serious | N/A |
| Meta-analysis on vitamin D effects (3 studies) | cohort and case–control studies | medium | not serious | serious (b) | not serious | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patini, R.; Favetti Giaquinto, E.; Gioco, G.; Castagnola, R.; Perrotti, V.; Rupe, C.; Di Gennaro, L.; Nocca, G.; Lajolo, C. Malnutrition as a Risk Factor in the Development of Oral Cancer: A Systematic Literature Review and Meta-Analyses. Nutrients 2024, 16, 360. https://doi.org/10.3390/nu16030360
Patini R, Favetti Giaquinto E, Gioco G, Castagnola R, Perrotti V, Rupe C, Di Gennaro L, Nocca G, Lajolo C. Malnutrition as a Risk Factor in the Development of Oral Cancer: A Systematic Literature Review and Meta-Analyses. Nutrients. 2024; 16(3):360. https://doi.org/10.3390/nu16030360
Chicago/Turabian StylePatini, Romeo, Eleonora Favetti Giaquinto, Gioele Gioco, Raffaella Castagnola, Vittoria Perrotti, Cosimo Rupe, Leonardo Di Gennaro, Giuseppina Nocca, and Carlo Lajolo. 2024. "Malnutrition as a Risk Factor in the Development of Oral Cancer: A Systematic Literature Review and Meta-Analyses" Nutrients 16, no. 3: 360. https://doi.org/10.3390/nu16030360
APA StylePatini, R., Favetti Giaquinto, E., Gioco, G., Castagnola, R., Perrotti, V., Rupe, C., Di Gennaro, L., Nocca, G., & Lajolo, C. (2024). Malnutrition as a Risk Factor in the Development of Oral Cancer: A Systematic Literature Review and Meta-Analyses. Nutrients, 16(3), 360. https://doi.org/10.3390/nu16030360