
Personalized Nutrition in the Pediatric ICU: Steering the Shift from Acute Stress to Metabolic Recovery and Rehabilitation



{kind=link}
{kind=link}
{kind=link}
Highlights
- Accurate assessment of nutritional status and daily energy and protein needs is crucial for critically ill pediatric patients.
- Early, full nutritional support, including early parenteral nutrition, high protein doses, or individual micronutrient supplementation, has not demonstrated benefits in these patients due to anabolic resistance and may lead to poor outcomes.
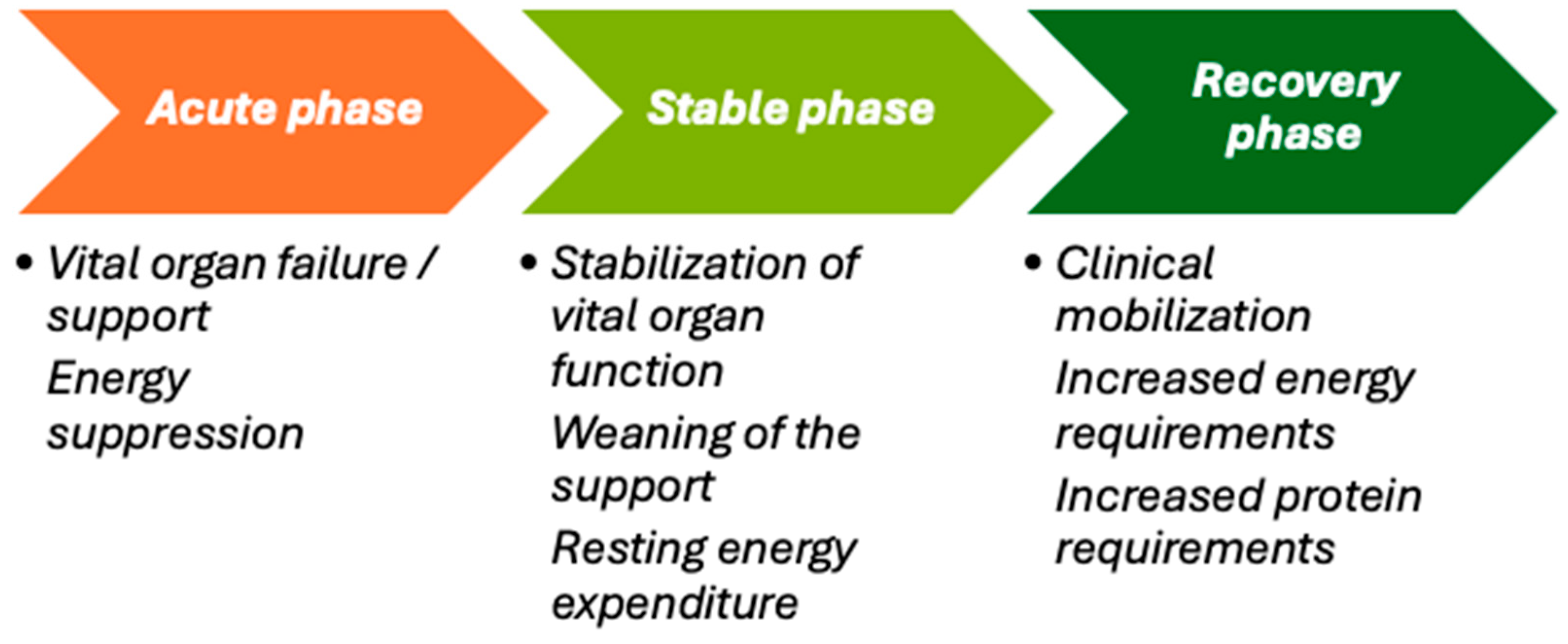
- Early, personalized incremental enteral feeding can help counteract the negative balance during the acute phase, restore organ function during stabilization, and support growth during recovery and beyond.
- Due to the evolving metabolic, neuroendocrine, and immune changes associated with severe illness or trauma, energy and protein needs vary dynamically, necessitating tailored macronutrient intake.
- There is substantial evidence supporting the establishment of a dedicated nutritional team in the ICU to enhance nutritional interventions.
- Implementing tailored nutritional protocols in the ICU is recommended to reduce morbidity and mortality in critically ill children.
Abstract
1. Introduction
2. Methods
3. Metabolism in Critical Illness
3.1. Catabolism
3.2. Anabolism
4. Assessment of Nutritional Status
4.1. Malnutrition
4.2. Nutritional Deterioration
4.3. Muscle Mass Loss
5. Energy Requirements
5.1. The Acute Phase
5.2. The Recovery Phase
5.3. Post-PICU Discharge
6. Energy Expenditure Measurement
6.1. Indirect Calorimetry
6.2. Predictive Equations
7. Macronutrient Requirements
7.1. Protein
7.1.1. Muscle Protein Synthesis
7.1.2. Protein Calculation
7.2. Glucose
7.3. Lipids
8. Micronutrients
9. Nutritional Support
9.1. Underfeeding and Overfeeding
9.2. Refeeding Syndrome
10. Enteral Nutrition
10.1. Early Initiation and Advancement
10.2. Specific Situations
10.3. Contraindications
10.4. Common Barriers to Enteral Nutrition
10.5. Enteral Feeding Formulas
10.6. Pharmaco-Nutrition
10.7. Route and Patterns of Enteral Feeding
11. Parenteral Nutrition
11.1. Autophagy
11.2. Ketones
12. Clinical Guidelines
12.1. Nutrition Protocols
12.2. Implementation Models
12.3. Personalized Monitoring
13. Focused Research
13.1. Uncertainties
13.2. Perspectives for Future Research
13.3. Personalizing Nutrition
14. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kerklaan, D.; Fivez, T.; Mehta, N.M.; Mesotten, D.; van Rosmalen, J.; Hulst, J.M.; Van den Berghe, G.; Joosten, K.F.M.; Verbruggen, S.C.A.T. Worldwide Survey of Nutritional Practices in PICUs. Pediatr. Crit. Care Med. 2016, 17, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.M.; Skillman, H.E.; Irving, S.Y.; Coss-Bu, J.A.; Vermilyea, S.; Farrington, E.A.; McKeever, L.; Hall, A.M.; Goday, P.S.; Braunschweig, C. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition. Pediatr. Crit. Care Med. 2017, 18, 675–715. [Google Scholar] [CrossRef] [PubMed]
- Tume, L.N.; Valla, F.V.; Joosten, K.; Jotterand Chaparro, C.; Latten, L.; Marino, L.V.; Macleod, I.; Moullet, C.; Pathan, N.; Rooze, S.; et al. Nutritional Support for Children during Critical Illness: European Society of Pediatric and Neonatal Intensive Care (ESPNIC) Metabolism, Endocrine and Nutrition Section Position Statement and Clinical Recommendations. Intensive Care Med. 2020, 46, 411–425. [Google Scholar] [CrossRef] [PubMed]
- Joosten, K.F.M.; Kerklaan, D.; Verbruggen, S.C.A.T. Nutritional Support and the Role of the Stress Response in Critically Ill Children. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Joosten, K.F.M.; Eveleens, R.D.; Verbruggen, S.C.A.T. Nutritional Support in the Recovery Phase of Critically Ill Children. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 152–158. [Google Scholar] [CrossRef]
- Keehn, A.; O’Brien, C.; Mazurak, V.; Brunet-Wood, K.; Joffe, A.; de Caen, A.; Larsen, B. Epidemiology of Interruptions to Nutrition Support in Critically Ill Children in the Pediatric Intensive Care Unit. JPEN J. Parenter. Enteral Nutr. 2015, 39, 211–217. [Google Scholar] [CrossRef]
- Hulst, J.M.; van Goudoever, J.B.; Zimmermann, L.J.I.; Hop, W.C.J.; Albers, M.J.I.J.; Tibboel, D.; Joosten, K.F.M. The Effect of Cumulative Energy and Protein Deficiency on Anthropometric Parameters in a Pediatric ICU Population. Clin. Nutr. 2004, 23, 1381–1389. [Google Scholar] [CrossRef]
- Tavladaki, T.; Spanaki, A.M.; Dimitriou, H.; Kondili, E.; Choulaki, C.; Georgopoulos, D.; Briassoulis, G. Similar Metabolic, Innate Immunity, and Adipokine Profiles in Adult and Pediatric Sepsis Versus Systemic Inflammatory Response Syndrome-A Pilot Study. Pediatr. Crit. Care Med. 2017, 18, e494–e505. [Google Scholar] [CrossRef]
- Spanaki, A.M.; Tavladaki, T.; Dimitriou, H.; Kozlov, A.V.; Duvigneau, J.C.; Meleti, E.; Weidinger, A.; Papakonstantinou, E.; Briassoulis, G. Longitudinal Profiles of Metabolism and Bioenergetics Associated with Innate Immune Hormonal Inflammatory Responses and Amino-Acid Kinetics in Severe Sepsis and Systemic Inflammatory Response Syndrome in Children. JPEN J. Parenter. Enteral Nutr. 2018, 42, 1061–1074. [Google Scholar] [CrossRef]
- Fivez, T.; Kerklaan, D.; Mesotten, D.; Verbruggen, S.; Wouters, P.J.; Vanhorebeek, I.; Debaveye, Y.; Vlasselaers, D.; Desmet, L.; Casaer, M.P.; et al. Early versus Late Parenteral Nutrition in Critically Ill Children. N. Engl. J. Med. 2016, 374, 1111–1122. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Rooyackers, O.; Bear, D.E. How to Avoid Harm with Feeding Critically Ill Patients: A Synthesis of Viewpoints of a Basic Scientist, Dietitian and Intensivist. Crit. Care 2023, 27, 258. [Google Scholar] [CrossRef] [PubMed]
- Vanhorebeek, I.; Latronico, N.; Van den Berghe, G. ICU-Acquired Weakness. Intensive Care Med. 2020, 46, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Gunst, J.; Casaer, M.P.; Preiser, J.-C.; Reignier, J.; Van den Berghe, G. Toward Nutrition Improving Outcome of Critically Ill Patients: How to Interpret Recent Feeding RCTs? Crit. Care 2023, 27, 43. [Google Scholar] [CrossRef] [PubMed]
- Abera, E.G.; Sime, H. The Prevalence of Malnutrition among Critically Ill Children: A Systematic Review and Meta-Analysis. BMC Pediatr. 2023, 23, 583. [Google Scholar] [CrossRef]
- Bechard, L.J.; Duggan, C.; Touger-Decker, R.; Parrott, J.S.; Rothpletz-Puglia, P.; Byham-Gray, L.; Heyland, D.; Mehta, N.M. Nutritional Status Based on Body Mass Index Is Associated with Morbidity and Mortality in Mechanically Ventilated Critically Ill Children in the PICU. Crit. Care Med. 2016, 44, 1530–1537. [Google Scholar] [CrossRef]
- Irving, S.Y.; Daly, B.; Verger, J.; Typpo, K.V.; Brown, A.-M.; Hanlon, A.; Weiss, S.L.; Fitzgerald, J.C.; Nadkarni, V.M.; Thomas, N.J.; et al. The Association of Nutrition Status Expressed as Body Mass Index z Score with Outcomes in Children With Severe Sepsis: A Secondary Analysis From the Sepsis Prevalence, Outcomes, and Therapies (SPROUT) Study. Crit. Care Med. 2018, 46, e1029–e1039. [Google Scholar] [CrossRef]
- Solana, M.J.; Manrique, G.; Fernández, R.; Slocker, M.; García, M.; Redondo, S.; Yun, C.; Gil, R.; Balaguer, M.; Rodríguez, E.; et al. Nutritional Status and Nutrition Support in Critically Ill Children in Spain: Results of a Multicentric Study. Nutrition 2021, 84, 110993. [Google Scholar] [CrossRef]
- Briassoulis, G.; Briassouli, E.; Ilia, S.; Briassoulis, P. External Validation of Equations to Estimate Resting Energy Expenditure in Critically Ill Children and Adolescents with and without Malnutrition: A Cross-Sectional Study. Nutrients 2022, 14, 4149. [Google Scholar] [CrossRef]
- Khlevner, J.; Naranjo, K.; Hoyer, C.; Carullo, A.S.; Kerr, K.W.; Marriage, B. Healthcare Burden Associated with Malnutrition Diagnoses in Hospitalized Children with Critical Illnesses. Nutrients 2023, 15, 3011. [Google Scholar] [CrossRef]
- Bagri, N.K.; Jose, B.; Shah, S.K.; Bhutia, T.D.; Kabra, S.K.; Lodha, R. Impact of Malnutrition on the Outcome of Critically Ill Children. Indian. J. Pediatr. 2015, 82, 601–605. [Google Scholar] [CrossRef]
- Teka, S.G.; Kebede, R.A.; Sherman, C. The Prevalence of Malnutrition during Admission to the Pediatric Intensive Care Unit, a Retrospective Cross-Sectional Study at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. Pan Afr. Med. J. 2022, 41, 77. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.M.; Duggan, C.P. Nutritional Deficiencies during Critical Illness. Pediatr. Clin. N. Am. 2009, 56, 1143–1160. [Google Scholar] [CrossRef] [PubMed]
- Briassoulis, G.; Zavras, N.; Hatzis, T. Malnutrition, Nutritional Indices, and Early Enteral Feeding in Critically Ill Children. Nutrition 2001, 17, 548–557. [Google Scholar] [CrossRef] [PubMed]
- Lew, C.C.H.; Yandell, R.; Fraser, R.J.L.; Chua, A.P.; Chong, M.F.F.; Miller, M. Association Between Malnutrition and Clinical Outcomes in the Intensive Care Unit: A Systematic Review. JPEN J. Parenter. Enteral Nutr. 2017, 41, 744–758. [Google Scholar] [CrossRef] [PubMed]
- Ventura, J.C.; Oliveira, L.D. de A.; Silveira, T.T.; Hauschild, D.B.; Mehta, N.M.; Moreno, Y.M.F.; PICU-ScREEN Study Group Admission Factors Associated with Nutritional Status Deterioration and Prolonged Pediatric Intensive Care Unit Stay in Critically Ill Children: PICU-ScREEN Multicenter Study. JPEN J. Parenter. Enteral Nutr. 2022, 46, 330–338. [Google Scholar] [CrossRef]
- Grippa, R.B.; Silva, P.S.; Barbosa, E.; Bresolin, N.L.; Mehta, N.M.; Moreno, Y.M.F. Nutritional Status as a Predictor of Duration of Mechanical Ventilation in Critically Ill Children. Nutrition 2017, 33, 91–95. [Google Scholar] [CrossRef]
- Létourneau, J.; Bélanger, V.; Marchand, V.; Boctor, D.L.; Rashid, M.; Avinashi, V.; Groleau, V.; Spahis, S.; Levy, E.; Marcil, V. Post-Discharge Complications and Hospital Readmissions Are Associated with Nutritional Risk and Malnutrition Status in a Cohort of Canadian Pediatric Patients. BMC Pediatr. 2024, 24, 469. [Google Scholar] [CrossRef]
- Rousseau, A.-F.; Prescott, H.C.; Brett, S.J.; Weiss, B.; Azoulay, E.; Creteur, J.; Latronico, N.; Hough, C.L.; Weber-Carstens, S.; Vincent, J.-L.; et al. Long-Term Outcomes after Critical Illness: Recent Insights. Crit. Care 2021, 25, 108. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM Criteria for the Diagnosis of Malnutrition—A Consensus Report from the Global Clinical Nutrition Community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef]
- Haines, R.W.; Zolfaghari, P.; Wan, Y.; Pearse, R.M.; Puthucheary, Z.; Prowle, J.R. Elevated Urea-to-Creatinine Ratio Provides a Biochemical Signature of Muscle Catabolism and Persistent Critical Illness after Major Trauma. Intensive Care Med. 2019, 45, 1718–1731. [Google Scholar] [CrossRef]
- McNelly, A.S.; Bear, D.E.; Connolly, B.A.; Arbane, G.; Allum, L.; Tarbhai, A.; Cooper, J.A.; Hopkins, P.A.; Wise, M.P.; Brealey, D.; et al. Effect of Intermittent or Continuous Feed on Muscle Wasting in Critical Illness: A Phase 2 Clinical Trial. Chest 2020, 158, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Peres, L.M.; Luis-Silva, F.; Menegueti, M.G.; Lovato, W.J.; do Espirito Santo, D.A.; Donadel, M.D.; Sato, L.; Malek-Zadeh, C.H.; Basile-Filho, A.; Martins-Filho, O.A.; et al. Comparison between Ultrasonography and Computed Tomography for Measuring Skeletal Muscle Mass in Critically Ill Patients with Different Body Mass Index. Clin. Nutr. ESPEN 2024, 59, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Dams, K.; De Meyer, G.R.; Jacobs, R.; Schepens, T.; Perkisas, S.; Moorkens, G.; Jorens, P. Combined Ultrasound of m. Quadriceps and Diaphragm to Determine the Occurrence of Sarcopenia and Prolonged Ventilation in a COVID-19 ICU Cohort: The COVID-SARCUS Trial. Nutrition 2024, 117, 112250. [Google Scholar] [CrossRef] [PubMed]
- Mourtzakis, M.; Parry, S.; Connolly, B.; Puthucheary, Z. Skeletal Muscle Ultrasound in Critical Care: A Tool in Need of Translation. Ann. Am. Thorac. Soc. 2017, 14, 1495–1503. [Google Scholar] [CrossRef]
- Mehta, N.M.; Bechard, L.J.; Cahill, N.; Wang, M.; Day, A.; Duggan, C.P.; Heyland, D.K. Nutritional Practices and Their Relationship to Clinical Outcomes in Critically Ill Children--an International Multicenter Cohort Study*. Crit. Care Med. 2012, 40, 2204–2211. [Google Scholar] [CrossRef]
- Srinivasan, V.; Hasbani, N.R.; Mehta, N.M.; Irving, S.Y.; Kandil, S.B.; Allen, H.C.; Typpo, K.V.; Cvijanovich, N.Z.; Faustino, E.V.S.; Wypij, D.; et al. Early Enteral Nutrition Is Associated with Improved Clinical Outcomes in Critically Ill Children: A Secondary Analysis of Nutrition Support in the Heart and Lung Failure-Pediatric Insulin Titration Trial. Pediatr. Crit. Care Med. 2020, 21, 213–221. [Google Scholar] [CrossRef]
- Joosten, K.; Verbruggen, S. PN Administration in Critically Ill Children in Different Phases of the Stress Response. Nutrients 2022, 14, 1819. [Google Scholar] [CrossRef]
- Wang, L.; Long, Y.; Zhang, Z.; Lin, J.; Zhou, J.; Li, G.; Ye, B.; Zhang, H.; Gao, L.; Tong, Z.; et al. Association of Energy Delivery with Short-Term Survival in Mechanically Ventilated Critically Ill Adult Patients: A Secondary Analysis of the NEED Trial. Eur. J. Clin. Nutr. 2024, 78, 257–263. [Google Scholar] [CrossRef]
- Deane, A.M.; Little, L.; Bellomo, R.; Chapman, M.J.; Davies, A.R.; Ferrie, S.; Horowitz, M.; Hurford, S.; Lange, K.; Litton, E.; et al. Outcomes Six Months after Delivering 100% or 70% of Enteral Calorie Requirements during Critical Illness (TARGET). A Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2020, 201, 814–822. [Google Scholar] [CrossRef]
- TARGET Investigators, for the ANZICS Clinical Trials Group; Chapman, M.; Peake, S.L.; Bellomo, R.; Davies, A.; Deane, A.; Horowitz, M.; Hurford, S.; Lange, K.; Little, L.; et al. Energy-Dense versus Routine Enteral Nutrition in the Critically Ill. N. Engl. J. Med. 2018, 379, 1823–1834. [Google Scholar] [CrossRef]
- Yue, H.-Y.; Peng, W.; Zeng, J.; Zhang, Y.; Wang, Y.; Jiang, H. Efficacy of Permissive Underfeeding for Critically Ill Patients: An Updated Systematic Review and Trial Sequential Meta-Analysis. J. Intensive Care 2024, 12, 4. [Google Scholar] [CrossRef] [PubMed]
- Compher, C.; Bingham, A.L.; McCall, M.; Patel, J.; Rice, T.W.; Braunschweig, C.; McKeever, L. Guidelines for the Provision of Nutrition Support Therapy in the Adult Critically Ill Patient: The American Society for Parenteral and Enteral Nutrition. JPEN J. Parenter. Enter. Nutr. 2022, 46, 12–41. [Google Scholar] [CrossRef] [PubMed]
- Matejovic, M.; Huet, O.; Dams, K.; Elke, G.; Vaquerizo Alonso, C.; Csomos, A.; Krzych, Ł.J.; Tetamo, R.; Puthucheary, Z.; Rooyackers, O.; et al. Medical Nutrition Therapy and Clinical Outcomes in Critically Ill Adults: A European Multinational, Prospective Observational Cohort Study (EuroPN). Crit. Care 2022, 26, 143. [Google Scholar] [CrossRef] [PubMed]
- Preiser, J.-C.; Ichai, C.; Orban, J.-C.; Groeneveld, A.B.J. Metabolic Response to the Stress of Critical Illness. Br. J. Anaesth. 2014, 113, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Briassoulis, G.; Venkataraman, S.; Thompson, A.E. Energy Expenditure in Critically Ill Children. Crit. Care Med. 2000, 28, 1166–1172. [Google Scholar] [CrossRef]
- Herridge, M.S.; Azoulay, É. Outcomes after Critical Illness. N. Engl. J. Med. 2023, 388, 913–924. [Google Scholar] [CrossRef]
- Wernerman, J.; Christopher, K.B.; Annane, D.; Casaer, M.P.; Coopersmith, C.M.; Deane, A.M.; De Waele, E.; Elke, G.; Ichai, C.; Karvellas, C.J.; et al. Metabolic Support in the Critically Ill: A Consensus of 19. Crit. Care 2019, 23, 318. [Google Scholar] [CrossRef]
- Chapple, L.-A.S.; Deane, A.M.; Heyland, D.K.; Lange, K.; Kranz, A.J.; Williams, L.T.; Chapman, M.J. Energy and Protein Deficits throughout Hospitalization in Patients Admitted with a Traumatic Brain Injury. Clin. Nutr. 2016, 35, 1315–1322. [Google Scholar] [CrossRef]
- van Zanten, A.R.H.; De Waele, E.; Wischmeyer, P.E. Nutrition Therapy and Critical Illness: Practical Guidance for the ICU, Post-ICU, and Long-Term Convalescence Phases. Crit. Care 2019, 23, 368. [Google Scholar] [CrossRef]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N.; et al. Individualised Nutritional Support in Medical Inpatients at Nutritional Risk: A Randomised Clinical Trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef]
- Whittle, J.; San-Millán, I. Objective Assessment of Metabolism and Guidance of ICU Rehabilitation with Cardiopulmonary Exercise Testing. Curr. Opin. Crit. Care 2021, 27, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Langouche, L.; Vander Perre, S.; Wouters, P.J.; D’Hoore, A.; Hansen, T.K.; Van den Berghe, G. Effect of Intensive Insulin Therapy on Insulin Sensitivity in the Critically Ill. J. Clin. Endocrinol. Metab. 2007, 92, 3890–3897. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Pichard, C. Feeding Should Be Individualized in the Critically Ill Patients. Curr. Opin. Crit. Care 2019, 25, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Briassoulis, G.; Briassouli, E.; Tavladaki, T.; Ilia, S.; Fitrolaki, D.M.; Spanaki, A.M. Unpredictable Combination of Metabolic and Feeding Patterns in Malnourished Critically Ill Children: The Malnutrition-Energy Assessment Question. Intensive Care Med. 2014, 40, 120–122. [Google Scholar] [CrossRef] [PubMed]
- De Waele, E.; van Zanten, A.R.H. Routine Use of Indirect Calorimetry in Critically Ill Patients: Pros and Cons. Crit. Care 2022, 26, 123. [Google Scholar] [CrossRef]
- Briassoulis, G.; Venkataraman, S.; Thompson, A. Cytokines and Metabolic Patterns in Pediatric Patients with Critical Illness. Clin. Dev. Immunol. 2010, 2010, 354047. [Google Scholar] [CrossRef]
- Singer, P.; Anbar, R.; Cohen, J.; Shapiro, H.; Shalita-Chesner, M.; Lev, S.; Grozovski, E.; Theilla, M.; Frishman, S.; Madar, Z. The Tight Calorie Control Study (TICACOS): A Prospective, Randomized, Controlled Pilot Study of Nutritional Support in Critically Ill Patients. Intensive Care Med. 2011, 37, 601–609. [Google Scholar] [CrossRef]
- Singer, P.; De Waele, E.; Sanchez, C.; Ruiz Santana, S.; Montejo, J.C.; Laterre, P.F.; Soroksky, A.; Moscovici, E.; Kagan, I. TICACOS International: A Multi-Center, Randomized, Prospective Controlled Study Comparing Tight Calorie Control versus Liberal Calorie Administration Study. Clin. Nutr. 2021, 40, 380–387. [Google Scholar] [CrossRef]
- Duan, J.-Y.; Zheng, W.-H.; Zhou, H.; Xu, Y.; Huang, H.-B. Energy Delivery Guided by Indirect Calorimetry in Critically Ill Patients: A Systematic Review and Meta-Analysis. Crit. Care 2021, 25, 88. [Google Scholar] [CrossRef]
- De Waele, E.; Jonckheer, J.; Wischmeyer, P.E. Indirect Calorimetry in Critical Illness: A New Standard of Care? Curr. Opin. Crit. Care 2021, 27, 334–343. [Google Scholar] [CrossRef]
- Pertzov, B.; Bar-Yoseph, H.; Menndel, Y.; Bendavid, I.; Kagan, I.; Glass, Y.D.; Singer, P. The Effect of Indirect Calorimetry Guided Isocaloric Nutrition on Mortality in Critically Ill Patients-a Systematic Review and Meta-Analysis. Eur. J. Clin. Nutr. 2022, 76, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Zusman, O.; Theilla, M.; Cohen, J.; Kagan, I.; Bendavid, I.; Singer, P. Resting Energy Expenditure, Calorie and Protein Consumption in Critically Ill Patients: A Retrospective Cohort Study. Crit. Care 2016, 20, 367. [Google Scholar] [CrossRef] [PubMed]
- Pradelli, L.; Graf, S.; Pichard, C.; Berger, M.M. Supplemental Parenteral Nutrition in Intensive Care Patients: A Cost Saving Strategy. Clin. Nutr. 2018, 37, 573–579. [Google Scholar] [CrossRef] [PubMed]
- De Waele, E.; Honoré, P.M.; Malbrain, M.L.N.G. Does the Use of Indirect Calorimetry Change Outcome in the ICU? Yes It Does. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Preiser, J.-C.; Arabi, Y.M.; Berger, M.M.; Casaer, M.; McClave, S.; Montejo-González, J.C.; Peake, S.; Reintam Blaser, A.; Van den Berghe, G.; van Zanten, A.; et al. A Guide to Enteral Nutrition in Intensive Care Units: 10 Expert Tips for the Daily Practice. Crit. Care 2021, 25, 424. [Google Scholar] [CrossRef] [PubMed]
- Tume, L.N.; Ista, E.; Verbruggen, S.; Jotterand Chaparro, C.; Moullet, C.; Latten, L.; Marino, L.V.; Valla, F.V. Practical Strategies to Implement the ESPNIC Nutrition Clinical Recommendations into PICU Practice. Clin. Nutr. ESPEN 2021, 42, 410–414. [Google Scholar] [CrossRef]
- Schofield, W.N. Predicting Basal Metabolic Rate, New Standards and Review of Previous Work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. S1), 5–41. [Google Scholar]
- Joosten, K.; Embleton, N.; Yan, W.; Senterre, T.; ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Energy. Clin. Nutr. 2018, 37, 2309–2314. [Google Scholar] [CrossRef]
- Briassoulis, P.; Ilia, S.; Briassouli, E.; Briassoulis, G. External Validation with Accuracy Confounders of VCO2-Derived Predicted Energy Expenditure Compared to Resting Energy Expenditure Measured by Indirect Calorimetry in Mechanically Ventilated Children. Nutrients 2022, 14, 4211. [Google Scholar] [CrossRef]
- Larsen, B.M.K.; Beggs, M.R.; Leong, A.Y.; Kang, S.H.; Persad, R.; Garcia Guerra, G. Can Energy Intake Alter Clinical and Hospital Outcomes in PICU? Clin. Nutr. ESPEN 2018, 24, 41–46. [Google Scholar] [CrossRef]
- Oshima, T.; Berger, M.M.; De Waele, E.; Guttormsen, A.B.; Heidegger, C.-P.; Hiesmayr, M.; Singer, P.; Wernerman, J.; Pichard, C. Indirect Calorimetry in Nutritional Therapy. A Position Paper by the ICALIC Study Group. Clin. Nutr. 2017, 36, 651–662. [Google Scholar] [CrossRef] [PubMed]
- De Waele, E.; Opsomer, T.; Honoré, P.M.; Diltoer, M.; Mattens, S.; Huyghens, L.; Spapen, H. Measured versus Calculated Resting Energy Expenditure in Critically Ill Adult Patients. Do Mathematics Match the Gold Standard? Min. Anestesiol. 2015, 81, 272–282. [Google Scholar]
- Niederer, L.E.; Miller, H.; Haines, K.L.; Molinger, J.; Whittle, J.; MacLeod, D.B.; McClave, S.A.; Wischmeyer, P.E. Prolonged Progressive Hypermetabolism during COVID-19 Hospitalization Undetected by Common Predictive Energy Equations. Clin. Nutr. ESPEN 2021, 45, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Whittle, J.; Molinger, J.; MacLeod, D.; Haines, K.; Wischmeyer, P.E.; LEEP-COVID Study Group. Persistent Hypermetabolism and Longitudinal Energy Expenditure in Critically Ill Patients with COVID-19. Crit. Care 2020, 24, 581. [Google Scholar] [CrossRef] [PubMed]
- Wischmeyer, P.E.; Bear, D.E.; Berger, M.M.; De Waele, E.; Gunst, J.; McClave, S.A.; Prado, C.M.; Puthucheary, Z.; Ridley, E.J.; Van den Berghe, G.; et al. Personalized Nutrition Therapy in Critical Care: 10 Expert Recommendations. Crit. Care 2023, 27, 261. [Google Scholar] [CrossRef]
- Coss-Bu, J.A.; Hamilton-Reeves, J.; Patel, J.J.; Morris, C.R.; Hurt, R.T. Protein Requirements of the Critically Ill Pediatric Patient. Nutr. Clin. Pract. 2017, 32, 128S–141S. [Google Scholar] [CrossRef]
- Casaer, M.P.; Stragier, H.; Hermans, G.; Hendrickx, A.; Wouters, P.J.; Dubois, J.; Guiza, F.; Van den Berghe, G.; Gunst, J. Impact of Withholding Early Parenteral Nutrition on 2-Year Mortality and Functional Outcome in Critically Ill Adults. Intensive Care Med. 2024, 50, 1593–1602. [Google Scholar] [CrossRef]
- Hermans, G.; Casaer, M.P.; Clerckx, B.; Güiza, F.; Vanhullebusch, T.; Derde, S.; Meersseman, P.; Derese, I.; Mesotten, D.; Wouters, P.J.; et al. Effect of Tolerating Macronutrient Deficit on the Development of Intensive-Care Unit Acquired Weakness: A Subanalysis of the EPaNIC Trial. Lancet Respir. Med. 2013, 1, 621–629. [Google Scholar] [CrossRef]
- Vanhorebeek, I.; Verbruggen, S.; Casaer, M.P.; Gunst, J.; Wouters, P.J.; Hanot, J.; Guerra, G.G.; Vlasselaers, D.; Joosten, K.; Van den Berghe, G. Effect of Early Supplemental Parenteral Nutrition in the Paediatric ICU: A Preplanned Observational Study of Post-Randomisation Treatments in the PEPaNIC Trial. Lancet Respir. Med. 2017, 5, 475–483. [Google Scholar] [CrossRef]
- Casaer, M.P.; Wilmer, A.; Hermans, G.; Wouters, P.J.; Mesotten, D.; Van den Berghe, G. Role of Disease and Macronutrient Dose in the Randomized Controlled EPaNIC Trial: A Post Hoc Analysis. Am. J. Respir. Crit. Care Med. 2013, 187, 247–255. [Google Scholar] [CrossRef]
- Singer, P.; Berger, M.M.; Van den Berghe, G.; Biolo, G.; Calder, P.; Forbes, A.; Griffiths, R.; Kreyman, G.; Leverve, X.; Pichard, C.; et al. ESPEN Guidelines on Parenteral Nutrition: Intensive Care. Clin. Nutr. 2009, 28, 387–400. [Google Scholar] [CrossRef] [PubMed]
- van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; Sainz de Pipaon, M.; ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Amino Acids. Clin. Nutr. 2018, 37, 2315–2323. [Google Scholar] [CrossRef] [PubMed]
- Lee, Z.-Y.; Yap, C.S.L.; Hasan, M.S.; Engkasan, J.P.; Barakatun-Nisak, M.Y.; Day, A.G.; Patel, J.J.; Heyland, D.K. The Effect of Higher versus Lower Protein Delivery in Critically Ill Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit. Care 2021, 25, 260. [Google Scholar] [CrossRef] [PubMed]
- van Ruijven, I.M.; Abma, J.; Brunsveld-Reinders, A.H.; Stapel, S.N.; van Etten-Jamaludin, F.; Boirie, Y.; Barazzoni, R.; Weijs, P.J.M. High Protein Provision of More than 1.2 g/Kg Improves Muscle Mass Preservation and Mortality in ICU Patients: A Systematic Review and Meta-Analyses. Clin. Nutr. 2023, 42, 2395–2403. [Google Scholar] [CrossRef]
- Heyland, D.K.; Patel, J.; Compher, C.; Rice, T.W.; Bear, D.E.; Lee, Z.-Y.; González, V.C.; O’Reilly, K.; Regala, R.; Wedemire, C.; et al. The Effect of Higher Protein Dosing in Critically Ill Patients with High Nutritional Risk (EFFORT Protein): An International, Multicentre, Pragmatic, Registry-Based Randomised Trial. Lancet 2023, 401, 568–576. [Google Scholar] [CrossRef]
- Stoppe, C.; Patel, J.J.; Zarbock, A.; Lee, Z.-Y.; Rice, T.W.; Mafrici, B.; Wehner, R.; Chan, M.H.M.; Lai, P.C.K.; MacEachern, K.; et al. The Impact of Higher Protein Dosing on Outcomes in Critically Ill Patients with Acute Kidney Injury: A Post Hoc Analysis of the EFFORT Protein Trial. Crit. Care 2023, 27, 399. [Google Scholar] [CrossRef]
- Doig, G.S.; Simpson, F.; Bellomo, R.; Heighes, P.T.; Sweetman, E.A.; Chesher, D.; Pollock, C.; Davies, A.; Botha, J.; Harrigan, P.; et al. Intravenous Amino Acid Therapy for Kidney Function in Critically Ill Patients: A Randomized Controlled Trial. Intensive Care Med. 2015, 41, 1197–1208. [Google Scholar] [CrossRef]
- Tweel, L.E.; Compher, C.; Bear, D.E.; Gutierrez-Castrellon, P.; Leaver, S.K.; MacEachern, K.; Ortiz-Reyes, L.; Pooja, L.; León, A.; Wedemire, C.; et al. A Comparison of High and Usual Protein Dosing in Critically Ill Patients with Obesity: A Post Hoc Analysis of an International, Pragmatic, Single-Blinded, Randomized Clinical Trial. Crit. Care Med. 2024, 52, 586–595. [Google Scholar] [CrossRef]
- Allingstrup, M.J.; Kondrup, J.; Wiis, J.; Claudius, C.; Pedersen, U.G.; Hein-Rasmussen, R.; Bjerregaard, M.R.; Steensen, M.; Jensen, T.H.; Lange, T.; et al. Early Goal-Directed Nutrition versus Standard of Care in Adult Intensive Care Patients: The Single-Centre, Randomised, Outcome Assessor-Blinded EAT-ICU Trial. Intensive Care Med. 2017, 43, 1637–1647. [Google Scholar] [CrossRef]
- Gunst, J.; Vanhorebeek, I.; Casaer, M.P.; Hermans, G.; Wouters, P.J.; Dubois, J.; Claes, K.; Schetz, M.; Van den Berghe, G. Impact of Early Parenteral Nutrition on Metabolism and Kidney Injury. J. Am. Soc. Nephrol. 2013, 24, 995–1005. [Google Scholar] [CrossRef]
- van Gassel, R.J.J.; Baggerman, M.R.; van de Poll, M.C.G. Metabolic Aspects of Muscle Wasting during Critical Illness. Curr. Opin. Clin. Nutr. Metab. Care 2020, 23, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Chapple, L.-A.S.; Kouw, I.W.K.; Summers, M.J.; Weinel, L.M.; Gluck, S.; Raith, E.; Slobodian, P.; Soenen, S.; Deane, A.M.; van Loon, L.J.C.; et al. Muscle Protein Synthesis after Protein Administration in Critical Illness. Am. J. Respir. Crit. Care Med. 2022, 206, 740–749. [Google Scholar] [CrossRef] [PubMed]
- Morton, R.W.; Traylor, D.A.; Weijs, P.J.M.; Phillips, S.M. Defining Anabolic Resistance: Implications for Delivery of Clinical Care Nutrition. Curr. Opin. Crit. Care 2018, 24, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Daum, N.; Drewniok, N.; Bald, A.; Ulm, B.; Buyukli, A.; Grunow, J.J.; Schaller, S.J. Early Mobilisation within 72 Hours after Admission of Critically Ill Patients in the Intensive Care Unit: A Systematic Review with Network Meta-Analysis. Intensive Crit. Care Nurs. 2024, 80, 103573. [Google Scholar] [CrossRef] [PubMed]
- Moonen, H.P.F.X.; Van Zanten, A.R.H. Bioelectric Impedance Analysis for Body Composition Measurement and Other Potential Clinical Applications in Critical Illness. Curr. Opin. Crit. Care 2021, 27, 344–353. [Google Scholar] [CrossRef]
- Kim, T.J.; Park, S.-H.; Jeong, H.-B.; Ha, E.J.; Cho, W.S.; Kang, H.-S.; Kim, J.E.; Ko, S.-B. Optimizing Nitrogen Balance Is Associated with Better Outcomes in Neurocritically Ill Patients. Nutrients 2020, 12, 3137. [Google Scholar] [CrossRef]
- Haines, R.W.; Prowle, J.R.; Day, A.; Bear, D.E.; Heyland, D.K.; Puthucheary, Z. Association between Urea Trajectory and Protein Dose in Critically Ill Adults: A Secondary Exploratory Analysis of the Effort Protein Trial (RE-EFFORT). Crit. Care 2024, 28, 24. [Google Scholar] [CrossRef]
- Eveleens, R.D.; Witjes, B.C.M.; Casaer, M.P.; Vanhorebeek, I.; Guerra, G.G.; Veldscholte, K.; Hanff, L.M.; Cosaert, K.; Desmet, L.; Vlasselaers, D.; et al. Supplementation of Vitamins, Trace Elements and Electrolytes in the PEPaNIC Randomised Controlled Trial: Composition and Preparation of the Prescription. Clin. Nutr. ESPEN 2021, 42, 244–251. [Google Scholar] [CrossRef]
- Mesotten, D.; Joosten, K.; van Kempen, A.; Verbruggen, S.; ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Carbohydrates. Clin. Nutr. 2018, 37, 2337–2343. [Google Scholar] [CrossRef]
- Lapillonne, A.; Fidler Mis, N.; Goulet, O.; van den Akker, C.H.P.; Wu, J.; Koletzko, B.; ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Lipids. Clin. Nutr. 2018, 37, 2324–2336. [Google Scholar] [CrossRef]
- Fivez, T.; Kerklaan, D.; Mesotten, D.; Verbruggen, S.; Joosten, K.; Van den Berghe, G. Evidence for the Use of Parenteral Nutrition in the Pediatric Intensive Care Unit. Clin. Nutr. 2017, 36, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Marino, L.V.; Valla, F.V.; Beattie, R.M.; Verbruggen, S.C.A.T. Micronutrient Status during Paediatric Critical Illness: A Scoping Review. Clin. Nutr. 2020, 39, 3571–3593. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.-K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.-L.; et al. ESPEN Micronutrient Guideline. Clin. Nutr. 2022, 41, 1357–1424. [Google Scholar] [CrossRef] [PubMed]
- Briassoulis, G.; Briassoulis, P.; Ilia, S.; Miliaraki, M.; Briassouli, E. The Anti-Oxidative, Anti-Inflammatory, Anti-Apoptotic, and Anti-Necroptotic Role of Zinc in COVID-19 and Sepsis. Antioxidants 2023, 12, 1942. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C.; Maguire, D.; Talwar, D. Relationship between Nutritional Status and the Systemic Inflammatory Response: Micronutrients. Proc. Nutr. Soc. 2019, 78, 56–67. [Google Scholar] [CrossRef]
- Riskin, A.; Picaud, J.-C.; Shamir, R.; ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Standard versus Individualized Parenteral Nutrition. Clin. Nutr. 2018, 37, 2409–2417. [Google Scholar] [CrossRef]
- Puntis, J.; Hojsak, I.; Ksiazyk, J.; ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Organisational Aspects. Clin. Nutr. 2018, 37, 2392–2400. [Google Scholar] [CrossRef]
- Prieto, M.B.; Cid, J.L.-H. Malnutrition in the Critically Ill Child: The Importance of Enteral Nutrition. Int. J. Environ. Res. Public Health 2011, 8, 4353–4366. [Google Scholar] [CrossRef]
- Salciute-Simene, E.; Stasiunaitis, R.; Ambrasas, E.; Tutkus, J.; Milkevicius, I.; Sostakaite, G.; Klimasauskas, A.; Kekstas, G. Impact of Enteral Nutrition Interruptions on Underfeeding in Intensive Care Unit. Clin. Nutr. 2021, 40, 1310–1317. [Google Scholar] [CrossRef]
- Tanaka, A.; Hamilton, K.; Eastwood, G.M.; Jones, D.; Bellomo, R. The Epidemiology of Overfeeding in Mechanically Ventilated Intensive Care Patients. Clin. Nutr. ESPEN 2020, 36, 139–145. [Google Scholar] [CrossRef]
- Vankrunkelsven, W.; Gunst, J.; Amrein, K.; Bear, D.E.; Berger, M.M.; Christopher, K.B.; Fuhrmann, V.; Hiesmayr, M.; Ichai, C.; Jakob, S.M.; et al. Monitoring and Parenteral Administration of Micronutrients, Phosphate and Magnesium in Critically Ill Patients: The VITA-TRACE Survey. Clin. Nutr. 2021, 40, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Blanc, S.; Vasileva, T.; Tume, L.N.; Baudin, F.; Chessel Ford, C.; Chaparro Jotterand, C.; Valla, F.V. Incidence of Refeeding Syndrome in Critically Ill Children with Nutritional Support. Front. Pediatr. 2022, 10, 932290. [Google Scholar] [CrossRef] [PubMed]
- Olthof, L.E.; Koekkoek, W.A.C.K.; van Setten, C.; Kars, J.C.N.; van Blokland, D.; van Zanten, A.R.H. Impact of Caloric Intake in Critically Ill Patients with, and without, Refeeding Syndrome: A Retrospective Study. Clin. Nutr. 2018, 37, 1609–1617. [Google Scholar] [CrossRef] [PubMed]
- Doig, G.S.; Simpson, F.; Heighes, P.T.; Bellomo, R.; Chesher, D.; Caterson, I.D.; Reade, M.C.; Harrigan, P.W.J.; Refeeding Syndrome Trial Investigators Group. Restricted versus Continued Standard Caloric Intake during the Management of Refeeding Syndrome in Critically Ill Adults: A Randomised, Parallel-Group, Multicentre, Single-Blind Controlled Trial. Lancet Respir. Med. 2015, 3, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Briassoulis, G.C.; Zavras, N.J.; Hatzis MD, T.D. Effectiveness and Safety of a Protocol for Promotion of Early Intragastric Feeding in Critically Ill Children. Pediatr. Crit. Care Med. 2001, 2, 113–121. [Google Scholar] [CrossRef]
- Briassoulis, G.; Ilia, S.; Meyer, R. Enteral Nutrition in PICUs: Mission Not Impossible! Pediatr. Crit. Care Med. 2016, 17, 85–87. [Google Scholar] [CrossRef]
- Moron, R.; Galvez, J.; Colmenero, M.; Anderson, P.; Cabeza, J.; Rodriguez-Cabezas, M.E. The Importance of the Microbiome in Critically Ill Patients: Role of Nutrition. Nutrients 2019, 11, 3002. [Google Scholar] [CrossRef]
- Loh, J.S.; Mak, W.Q.; Tan, L.K.S.; Ng, C.X.; Chan, H.H.; Yeow, S.H.; Foo, J.B.; Ong, Y.S.; How, C.W.; Khaw, K.Y. Microbiota-Gut-Brain Axis and Its Therapeutic Applications in Neurodegenerative Diseases. Signal Transduct. Target. Ther. 2024, 9, 37. [Google Scholar] [CrossRef]
- Carabotti, M.; Scirocco, A.; Maselli, M.A.; Severi, C. The Gut-Brain Axis: Interactions between Enteric Microbiota, Central and Enteric Nervous Systems. Ann. Gastroenterol. 2015, 28, 203–209. [Google Scholar]
- Ziaka, M.; Exadaktylos, A. Exploring the Lung-Gut Direction of the Gut-Lung Axis in Patients with ARDS. Crit. Care 2024, 28, 179. [Google Scholar] [CrossRef]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J. Parenter. Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef] [PubMed]
- Tian, F.; Heighes, P.T.; Allingstrup, M.J.; Doig, G.S. Early Enteral Nutrition Provided within 24 Hours of ICU Admission: A Meta-Analysis of Randomized Controlled Trials. Crit. Care Med. 2018, 46, 1049–1056. [Google Scholar] [CrossRef] [PubMed]
- Haines, K.; Parker, V.; Ohnuma, T.; Krishnamoorthy, V.; Raghunathan, K.; Sulo, S.; Kerr, K.W.; Besecker, B.Y.; Cassady, B.A.; Wischmeyer, P.E. Role of Early Enteral Nutrition in Mechanically Ventilated COVID-19 Patients. Crit. Care Explor. 2022, 4, e0683. [Google Scholar] [CrossRef] [PubMed]
- Khorasani, E.N.; Mansouri, F. Effect of Early Enteral Nutrition on Morbidity and Mortality in Children with Burns. Burns 2010, 36, 1067–1071. [Google Scholar] [CrossRef] [PubMed]
- Solana, M.J.; Manrique, G.; Slocker, M.; Fernández, R.; Gil, R.; Yun, C.; García, M.; Redondo, S.; Balaguer, M.; Rodríguez, E.; et al. Early vs Late Enteral Nutrition in Pediatric Intensive Care Unit: Barriers, Benefits, and Complications. Nutr. Clin. Pract. 2023, 38, 442–448. [Google Scholar] [CrossRef]
- Dike, C.R.; Abu-El-Haija, M. Nutrition Management and Pancreatitis in Children: New Insights. Curr. Opin. Clin. Nutr. Metab. Care 2022, 25, 321–324. [Google Scholar] [CrossRef]
- Hinkelmann, J.V.; de Oliveira, N.A.; Marcato, D.F.; Costa, A.R.R.O.; Ferreira, A.M.; Tomaz, M.; Rodrigues, T.J.; Mendes, A.P. Nutritional Support Protocol for Patients with COVID-19. Clin. Nutr. ESPEN 2022, 49, 544–550. [Google Scholar] [CrossRef]
- Lakenman, P.L.M.; van der Hoven, B.; Schuijs, J.M.; Eveleens, R.D.; van Bommel, J.; Olieman, J.F.; Joosten, K.F.M. Energy Expenditure and Feeding Practices and Tolerance during the Acute and Late Phase of Critically Ill COVID-19 Patients. Clin. Nutr. ESPEN 2021, 43, 383–389. [Google Scholar] [CrossRef]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN Guideline on Clinical Nutrition in the Intensive Care Unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef]
- Wischmeyer, P.E. Enteral Nutrition Can Be Given to Patients on Vasopressors. Crit. Care Med. 2020, 48, 122–125. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Starkopf, J.; Alhazzani, W.; Berger, M.M.; Casaer, M.P.; Deane, A.M.; Fruhwald, S.; Hiesmayr, M.; Ichai, C.; Jakob, S.M.; et al. Early Enteral Nutrition in Critically Ill Patients: ESICM Clinical Practice Guidelines. Intensive Care Med. 2017, 43, 380–398. [Google Scholar] [CrossRef] [PubMed]
- Leong, A.Y.; Cartwright, K.R.; Guerra, G.G.; Joffe, A.R.; Mazurak, V.C.; Larsen, B.M.K. A Canadian Survey of Perceived Barriers to Initiation and Continuation of Enteral Feeding in PICUs. Pediatr. Crit. Care Med. 2014, 15, e49–e55. [Google Scholar] [CrossRef] [PubMed]
- Kozeniecki, M.; Pitts, H.; Patel, J.J. Barriers and Solutions to Delivery of Intensive Care Unit Nutrition Therapy. Nutr. Clin. Pract. 2018, 33, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Panchal, A.K.; Manzi, J.; Connolly, S.; Christensen, M.; Wakeham, M.; Goday, P.S.; Mikhailov, T.A. Safety of Enteral Feedings in Critically Ill Children Receiving Vasoactive Agents. JPEN J. Parenter. Enteral Nutr. 2016, 40, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Briassoulis, G.; Briassoulis, P.; Ilia, S. If You Get Good Nutrition, You Will Become Happy; If You Get a Bad One, You Will Become an ICU Philosopher. Pediatr. Crit. Care Med. 2019, 20, 89–90. [Google Scholar] [CrossRef] [PubMed]
- Cahill, N.E.; Murch, L.; Cook, D.; Heyland, D.K.; Canadian Critical Care Trials Group. Barriers to Feeding Critically Ill Patients: A Multicenter Survey of Critical Care Nurses. J. Crit. Care 2012, 27, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Briassoulis, G.; Filippou, O.; Hatzi, E.; Papassotiriou, I.; Hatzis, T. Early Enteral Administration of Immunonutrition in Critically Ill Children: Results of a Blinded Randomized Controlled Clinical Trial. Nutrition 2005, 21, 799–807. [Google Scholar] [CrossRef]
- Briassoulis, G.; Filippou, O.; Kanariou, M.; Hatzis, T. Comparative Effects of Early Randomized Immune or Non-Immune-Enhancing Enteral Nutrition on Cytokine Production in Children with Septic Shock. Intensive Care Med. 2005, 31, 851–858. [Google Scholar] [CrossRef]
- Briassoulis, G.; Filippou, O.; Kanariou, M.; Papassotiriou, I.; Hatzis, T. Temporal Nutritional and Inflammatory Changes in Children with Severe Head Injury Fed a Regular or an Immune-Enhancing Diet: A Randomized, Controlled Trial. Pediatr. Crit. Care Med. 2006, 7, 56–62. [Google Scholar] [CrossRef]
- Wunderle, C.; von Arx, D.; Mueller, S.C.; Bernasconi, L.; Neyer, P.; Tribolet, P.; Stanga, Z.; Mueller, B.; Schuetz, P. Association of Glutamine and Glutamate Metabolism with Mortality among Patients at Nutritional Risk-A Secondary Analysis of the Randomized Clinical Trial EFFORT. Nutrients 2024, 16, 222. [Google Scholar] [CrossRef]
- Jordan, I.; Balaguer, M.; Esteban, M.E.; Cambra, F.J.; Felipe, A.; Hernández, L.; Alsina, L.; Molero, M.; Villaronga, M.; Esteban, E. Glutamine Effects on Heat Shock Protein 70 and Interleukines 6 and 10: Randomized Trial of Glutamine Supplementation versus Standard Parenteral Nutrition in Critically Ill Children. Clin. Nutr. 2016, 35, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Briassouli, E.; Goukos, D.; Daikos, G.; Apostolou, K.; Routsi, C.; Nanas, S.; Briassoulis, G. Glutamine Suppresses Hsp72 Not Hsp90α and Is Not Inducing Th1, Th2, or Th17 Cytokine Responses in Human Septic PBMCs. Nutrition 2014, 30, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Briassouli, E.; Tzanoudaki, M.; Goukos, D.; Routsi, C.; Nanas, S.; Vardas, K.; Apostolou, K.; Kanariou, M.; Daikos, G.; Briassoulis, G. Glutamine May Repress the Weak LPS and Enhance the Strong Heat Shock Induction of Monocyte and Lymphocyte HSP72 Proteins but May Not Modulate the HSP72 mRNA in Patients with Sepsis or Trauma. Biomed. Res. Int. 2015, 2015, 806042. [Google Scholar] [CrossRef] [PubMed]
- Tadié, J.-M.; Locher, C.; Maamar, A.; Reignier, J.; Asfar, P.; Commereuc, M.; Lesouhaitier, M.; Gregoire, M.; Le Pabic, E.; Bendavid, C.; et al. Enteral Citrulline Supplementation versus Placebo on SOFA Score on Day 7 in Mechanically Ventilated Critically Ill Patients: The IMMUNOCITRE Randomized Clinical Trial. Crit. Care 2023, 27, 381. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.-Y.; Wang, Y.; Wang, L.; Jiang, H. The Efficacy of Omega-3 Polyunsaturated Fatty Acids for Severe Burn Patients: A Systematic Review and Trial Sequential Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. ESPEN 2024, 59, 126–134. [Google Scholar] [CrossRef]
- Manzanares, W.; Lemieux, M.; Langlois, P.L.; Wischmeyer, P.E. Probiotic and Synbiotic Therapy in Critical Illness: A Systematic Review and Meta-Analysis. Crit. Care 2016, 19, 262. [Google Scholar] [CrossRef]
- Puthucheary, Z.; Gunst, J. Are Periods of Feeding and Fasting Protective during Critical Illness? Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 183–188. [Google Scholar] [CrossRef]
- Wilkinson, D.; Gallagher, I.J.; McNelly, A.; Bear, D.E.; Hart, N.; Montgomery, H.E.; Le Guennec, A.; Conte, M.R.; Francis, T.; Harridge, S.D.R.; et al. The Metabolic Effects of Intermittent versus Continuous Feeding in Critically Ill Patients. Sci. Rep. 2023, 13, 19508. [Google Scholar] [CrossRef]
- Kumar, V.; Sankar, J.; Jana, M.; Jat, K.R.; Kabra, S.K.; Lodha, R. Comparison of Protocol-Based Continuous and Intermittent Tube Feeding in Mechanically Ventilated Critically Ill Children—An Open Label Randomized Controlled Trial. Indian J. Pediatr. 2023. [Google Scholar] [CrossRef]
- Veldscholte, K.; Cramer, A.B.G.; de Jonge, R.C.J.; Rizopoulos, D.; Joosten, K.F.M.; Verbruggen, S.C.A.T. Intermittent Feeding with an Overnight Fast versus 24-h Feeding in Critically Ill Neonates, Infants, and Children: An Open-Label, Single-Centre, Randomised Controlled Trial. Clin. Nutr. 2023, 42, 1569–1580. [Google Scholar] [CrossRef]
- Casaer, M.P.; Mesotten, D.; Hermans, G.; Wouters, P.J.; Schetz, M.; Meyfroidt, G.; Van Cromphaut, S.; Ingels, C.; Meersseman, P.; Muller, J.; et al. Early versus Late Parenteral Nutrition in Critically Ill Adults. N. Engl. J. Med. 2011, 365, 506–517. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S.E.; Parrott, F.; Harrison, D.A.; Bear, D.E.; Segaran, E.; Beale, R.; Bellingan, G.; Leonard, R.; Mythen, M.G.; Rowan, K.M.; et al. Trial of the Route of Early Nutritional Support in Critically Ill Adults. N. Engl. J. Med. 2014, 371, 1673–1684. [Google Scholar] [CrossRef] [PubMed]
- Reignier, J.; Boisramé-Helms, J.; Brisard, L.; Lascarrou, J.-B.; Ait Hssain, A.; Anguel, N.; Argaud, L.; Asehnoune, K.; Asfar, P.; Bellec, F.; et al. Enteral versus Parenteral Early Nutrition in Ventilated Adults with Shock: A Randomised, Controlled, Multicentre, Open-Label, Parallel-Group Study (NUTRIREA-2). Lancet 2018, 391, 133–143. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Rice, T. W.; Wheeler, A.P.; Thompson, B.T.; Steingrub, J.; Hite, R.D.; Moss, M.; Morris, A.; Dong, N.; Rock, P. Initial Trophic vs Full Enteral Feeding in Patients with Acute Lung Injury: The EDEN Randomized Trial. J. Am. Med. Assoc. 2012, 307, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Aldawood, A.S.; Haddad, S.H.; Al-Dorzi, H.M.; Tamim, H.M.; Jones, G.; Mehta, S.; McIntyre, L.; Solaiman, O.; Sakkijha, M.H.; et al. Permissive Underfeeding or Standard Enteral Feeding in Critically Ill Adults. N. Engl. J. Med. 2015, 372, 2398–2408. [Google Scholar] [CrossRef]
- Verstraete, S.; Verbruggen, S.C.; Hordijk, J.A.; Vanhorebeek, I.; Dulfer, K.; Güiza, F.; van Puffelen, E.; Jacobs, A.; Leys, S.; Durt, A.; et al. Long-Term Developmental Effects of Withholding Parenteral Nutrition for 1 Week in the Paediatric Intensive Care Unit: A 2-Year Follow-up of the PEPaNIC International, Randomised, Controlled Trial. Lancet Respir. Med. 2019, 7, 141–153. [Google Scholar] [CrossRef]
- Jacobs, A.; Dulfer, K.; Eveleens, R.D.; Hordijk, J.; Van Cleemput, H.; Verlinden, I.; Wouters, P.J.; Mebis, L.; Guerra, G.G.; Joosten, K.; et al. Long-Term Developmental Effect of Withholding Parenteral Nutrition in Paediatric Intensive Care Units: A 4-Year Follow-up of the PEPaNIC Randomised Controlled Trial. Lancet Child. Adolesc. Health 2020, 4, 503–514. [Google Scholar] [CrossRef]
- Jacobs, A.; Güiza, F.; Verlinden, I.; Dulfer, K.; Garcia Guerra, G.; Joosten, K.; Verbruggen, S.C.; Vanhorebeek, I.; Van den Berghe, G. Differential DNA Methylation by Early versus Late Parenteral Nutrition in the PICU: A Biological Basis for Its Impact on Emotional and Behavioral Problems Documented 4 Years Later. Clin. Epigenetics 2021, 13, 146. [Google Scholar] [CrossRef]
- Gunst, J. Recovery from Critical Illness-Induced Organ Failure: The Role of Autophagy. Crit. Care 2017, 21, 209. [Google Scholar] [CrossRef]
- Thiessen, S.E.; Derese, I.; Derde, S.; Dufour, T.; Pauwels, L.; Bekhuis, Y.; Pintelon, I.; Martinet, W.; Van den Berghe, G.; Vanhorebeek, I. The Role of Autophagy in Critical Illness-Induced Liver Damage. Sci. Rep. 2017, 7, 14150. [Google Scholar] [CrossRef]
- Vanhorebeek, I.; Gunst, J.; Derde, S.; Derese, I.; Boussemaere, M.; Güiza, F.; Martinet, W.; Timmermans, J.-P.; D’Hoore, A.; Wouters, P.J.; et al. Insufficient Activation of Autophagy Allows Cellular Damage to Accumulate in Critically Ill Patients. J. Clin. Endocrinol. Metab. 2011, 96, E633–E645. [Google Scholar] [CrossRef] [PubMed]
- Derde, S.; Vanhorebeek, I.; Güiza, F.; Derese, I.; Gunst, J.; Fahrenkrog, B.; Martinet, W.; Vervenne, H.; Ververs, E.-J.; Larsson, L.; et al. Early Parenteral Nutrition Evokes a Phenotype of Autophagy Deficiency in Liver and Skeletal Muscle of Critically Ill Rabbits. Endocrinology 2012, 153, 2267–2276. [Google Scholar] [CrossRef] [PubMed]
- Gunst, J.; Derese, I.; Aertgeerts, A.; Ververs, E.-J.; Wauters, A.; Van den Berghe, G.; Vanhorebeek, I. Insufficient Autophagy Contributes to Mitochondrial Dysfunction, Organ Failure, and Adverse Outcome in an Animal Model of Critical Illness. Crit. Care Med. 2013, 41, 182–194. [Google Scholar] [CrossRef]
- Mizushima, N.; Levine, B. Autophagy in Human Diseases. N. Engl. J. Med. 2020, 383, 1564–1576. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, L.; Casaer, M.P.; Gunst, J. Autophagy and Its Implications Against Early Full Nutrition Support in Critical Illness. Nutr. Clin. Pract. 2018, 33, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Goday, P.S.; Kuhn, E.M.; Mikhailov, T.A. Early Parenteral Nutrition in Critically Ill Children Not Receiving Early Enteral Nutrition Is Associated with Significantly Higher Mortality. JPEN J. Parenter. Enteral Nutr. 2020, 44, 1096–1103. [Google Scholar] [CrossRef]
- De Bruyn, A.; Gunst, J.; Goossens, C.; Vander Perre, S.; Guerra, G.G.; Verbruggen, S.; Joosten, K.; Langouche, L.; Van den Berghe, G. Effect of Withholding Early Parenteral Nutrition in PICU on Ketogenesis as Potential Mediator of Its Outcome Benefit. Crit. Care 2020, 24, 536. [Google Scholar] [CrossRef]
- De Bruyn, A.; Langouche, L.; Vander Perre, S.; Gunst, J.; Van den Berghe, G. Impact of Withholding Early Parenteral Nutrition in Adult Critically Ill Patients on Ketogenesis in Relation to Outcome. Crit. Care 2021, 25, 102. [Google Scholar] [CrossRef]
- Goossens, C.; Weckx, R.; Derde, S.; Dufour, T.; Vander Perre, S.; Pauwels, L.; Thiessen, S.E.; Van Veldhoven, P.P.; Van den Berghe, G.; Langouche, L. Adipose Tissue Protects against Sepsis-Induced Muscle Weakness in Mice: From Lipolysis to Ketones. Crit. Care 2019, 23, 236. [Google Scholar] [CrossRef]
- Roudi, F.; Khademi, G.; Ranjbar, G.; Pouryazdanpanah, M.; Pahlavani, N.; Boskabady, A.; Sezavar, M.; Nematy, M. The Effects of Implementation of a Stepwise Algorithmic Protocol for Nutrition Care Process in Gastro-Intestinal Surgical Children in Pediatric Intensive Care Unit (PICU). Clin. Nutr. ESPEN 2021, 43, 250–258. [Google Scholar] [CrossRef]
- Joosten, K.F.M.; Hulst, J.M. 3.26 Pediatric Intensive Care. World Rev. Nutr. Diet. 2022, 124, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Pronovost, P.J.; Berenholtz, S.M.; Needham, D.M. Translating Evidence into Practice: A Model for Large Scale Knowledge Translation. Br. Med. J. 2008, 337, a1714. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Revelly, J.-P.; Wasserfallen, J.-B.; Schmid, A.; Bouvry, S.; Cayeux, M.-C.; Musset, M.; Maravic, P.; Chiolero, R.L. Impact of a Computerized Information System on Quality of Nutritional Support in the ICU. Nutrition 2006, 22, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Kagan, I.; Hellerman-Itzhaki, M.; Neuman, I.; Glass, Y.D.; Singer, P. Reflux Events Detected by Multichannel Bioimpedance Smart Feeding Tube during High Flow Nasal Cannula Oxygen Therapy and Enteral Feeding: First Case Report. J. Crit. Care 2020, 60, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Calder, P.C.; Casaer, M.; Hiesmayr, M.; Mayer, K.; Montejo-Gonzalez, J.C.; Pichard, C.; Preiser, J.-C.; et al. ESPEN Practical and Partially Revised Guideline: Clinical Nutrition in the Intensive Care Unit. Clin. Nutr. 2023, 42, 1671–1689. [Google Scholar] [CrossRef]
- Veldscholte, K.; Hulst, J.M.; Eveleens, R.D.; de Jonge, R.C.J.; de Koning, B.A.E.; van den Berg, S.A.A.; van der Wal, R.; Ruijter, G.J.G.; Rizopoulos, D.; Vanhorebeek, I.; et al. Gastrointestinal Biomarkers and Their Association with Feeding in the First Five Days of Pediatric Critical Illness. J. Pediatr. Gastroenterol. Nutr. 2023, 77, 811–818. [Google Scholar] [CrossRef]
- Noyahr, J.K.; Tatucu-Babet, O.A.; Chapple, L.-A.S.; Barlow, C.J.; Chapman, M.J.; Deane, A.M.; Fetterplace, K.; Hodgson, C.L.; Winderlich, J.; Udy, A.A.; et al. Methodological Rigor and Transparency in Clinical Practice Guidelines for Nutrition Care in Critically Ill Adults: A Systematic Review Using the AGREE II and AGREE-REX Tools. Nutrients 2022, 14, 2603. [Google Scholar] [CrossRef]
- Kagan, I.; Cohen, J.; Bendavid, I.; Kramer, S.; Mesilati-Stahy, R.; Glass, Y.; Theilla, M.; Singer, P. Effect of Combined Protein-Enriched Enteral Nutrition and Early Cycle Ergometry in Mechanically Ventilated Critically Ill Patients-A Pilot Study. Nutrients 2022, 14, 1589. [Google Scholar] [CrossRef]
- Kim, H.K.; Suzuki, T.; Saito, K.; Yoshida, H.; Kobayashi, H.; Kato, H.; Katayama, M. Effects of Exercise and Amino Acid Supplementation on Body Composition and Physical Function in Community-Dwelling Elderly Japanese Sarcopenic Women: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2012, 60, 16–23. [Google Scholar] [CrossRef]
- Johansson, P.I.; Nakahira, K.; Rogers, A.J.; McGeachie, M.J.; Baron, R.M.; Fredenburgh, L.E.; Harrington, J.; Choi, A.M.K.; Christopher, K.B. Plasma Mitochondrial DNA and Metabolomic Alterations in Severe Critical Illness. Crit. Care 2018, 22, 360. [Google Scholar] [CrossRef]
- Hung, K.-Y.; Chen, T.-H.; Lee, Y.-F.; Fang, W.-F. Using Body Composition Analysis for Improved Nutritional Intervention in Septic Patients: A Prospective Interventional Study. Nutrients 2023, 15, 3814. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briassoulis, G.; Ilia, S.; Briassouli, E. Personalized Nutrition in the Pediatric ICU: Steering the Shift from Acute Stress to Metabolic Recovery and Rehabilitation. Nutrients 2024, 16, 3523. https://doi.org/10.3390/nu16203523
Briassoulis G, Ilia S, Briassouli E. Personalized Nutrition in the Pediatric ICU: Steering the Shift from Acute Stress to Metabolic Recovery and Rehabilitation. Nutrients. 2024; 16(20):3523. https://doi.org/10.3390/nu16203523
Chicago/Turabian StyleBriassoulis, George, Stavroula Ilia, and Efrossini Briassouli. 2024. "Personalized Nutrition in the Pediatric ICU: Steering the Shift from Acute Stress to Metabolic Recovery and Rehabilitation" Nutrients 16, no. 20: 3523. https://doi.org/10.3390/nu16203523
APA StyleBriassoulis, G., Ilia, S., & Briassouli, E. (2024). Personalized Nutrition in the Pediatric ICU: Steering the Shift from Acute Stress to Metabolic Recovery and Rehabilitation. Nutrients, 16(20), 3523. https://doi.org/10.3390/nu16203523