
Comparison of the Gut Microbiota of Patients Who Improve with Antibiotic Combination Therapy for Ulcerative Colitis and Those Who Do Not: Investigation by Fecal Metagenomic Analyses
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Study Subjects
2.2. Study Design
2.3. Sample Collection
2.4. DNA Isolation from Fecal Samples
2.5. Whole-DNA Sequencing and Metagenomic Analyses
2.6. Data Deposition
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
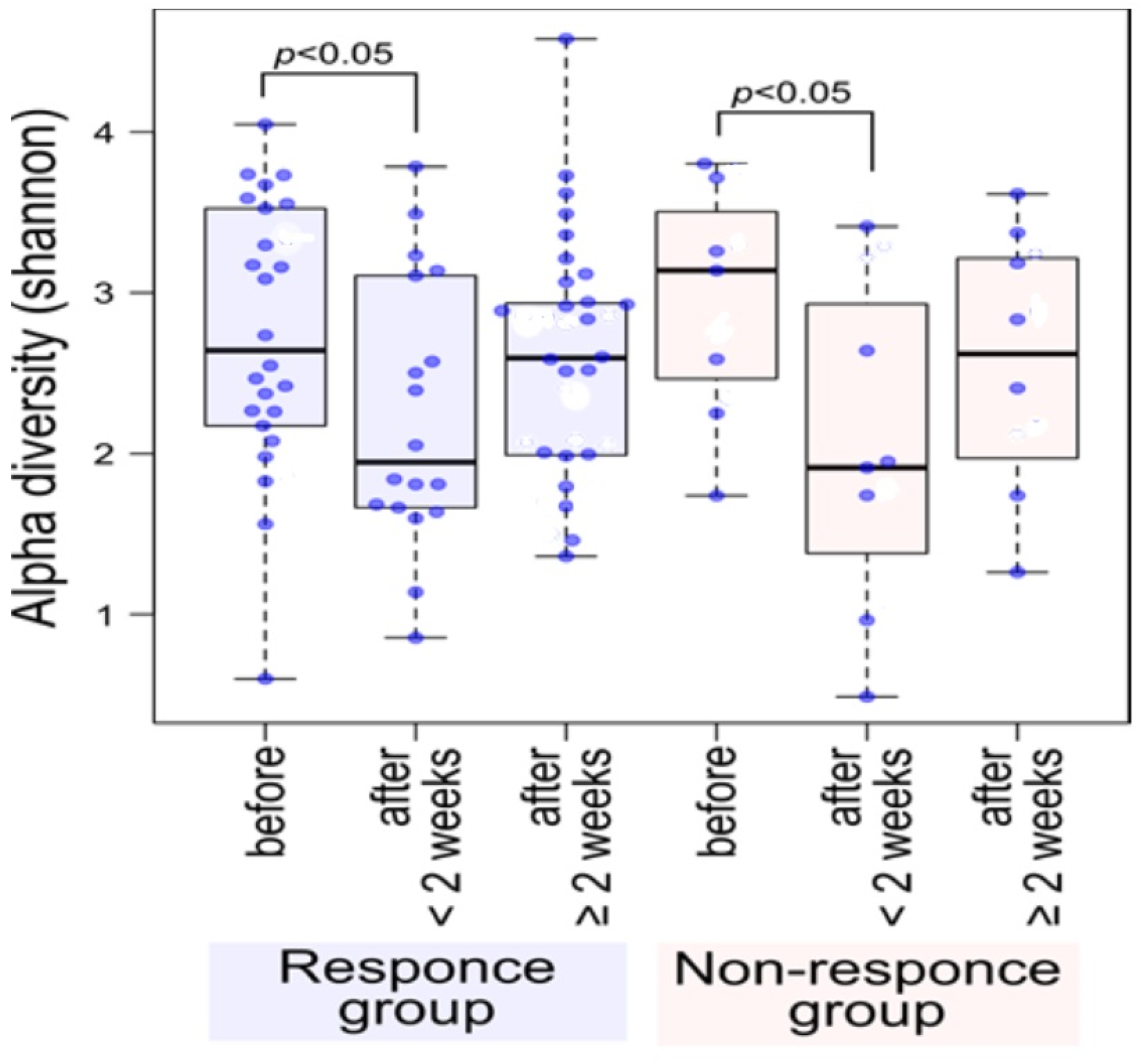
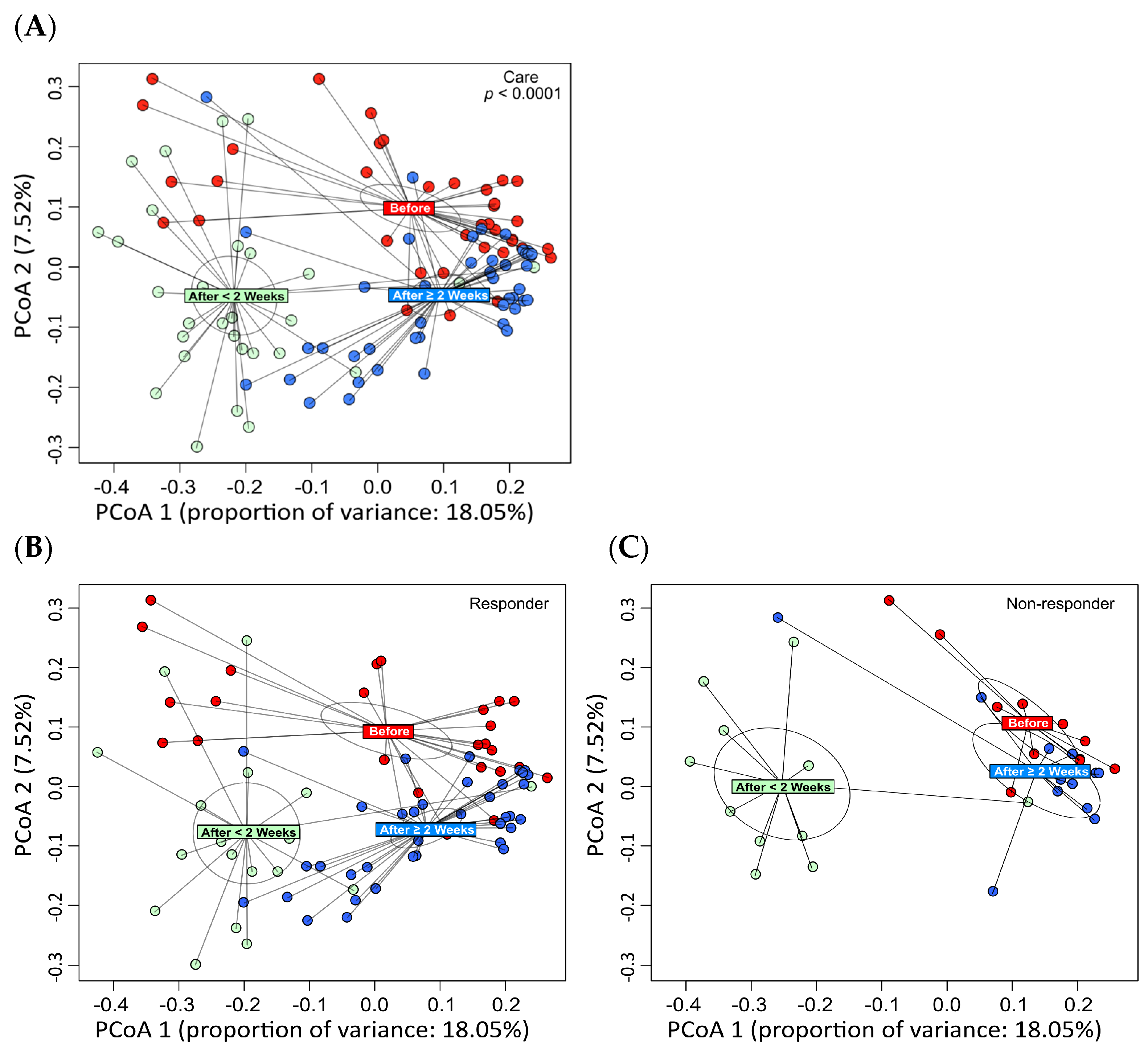
3.2. Metagenomic Analyses
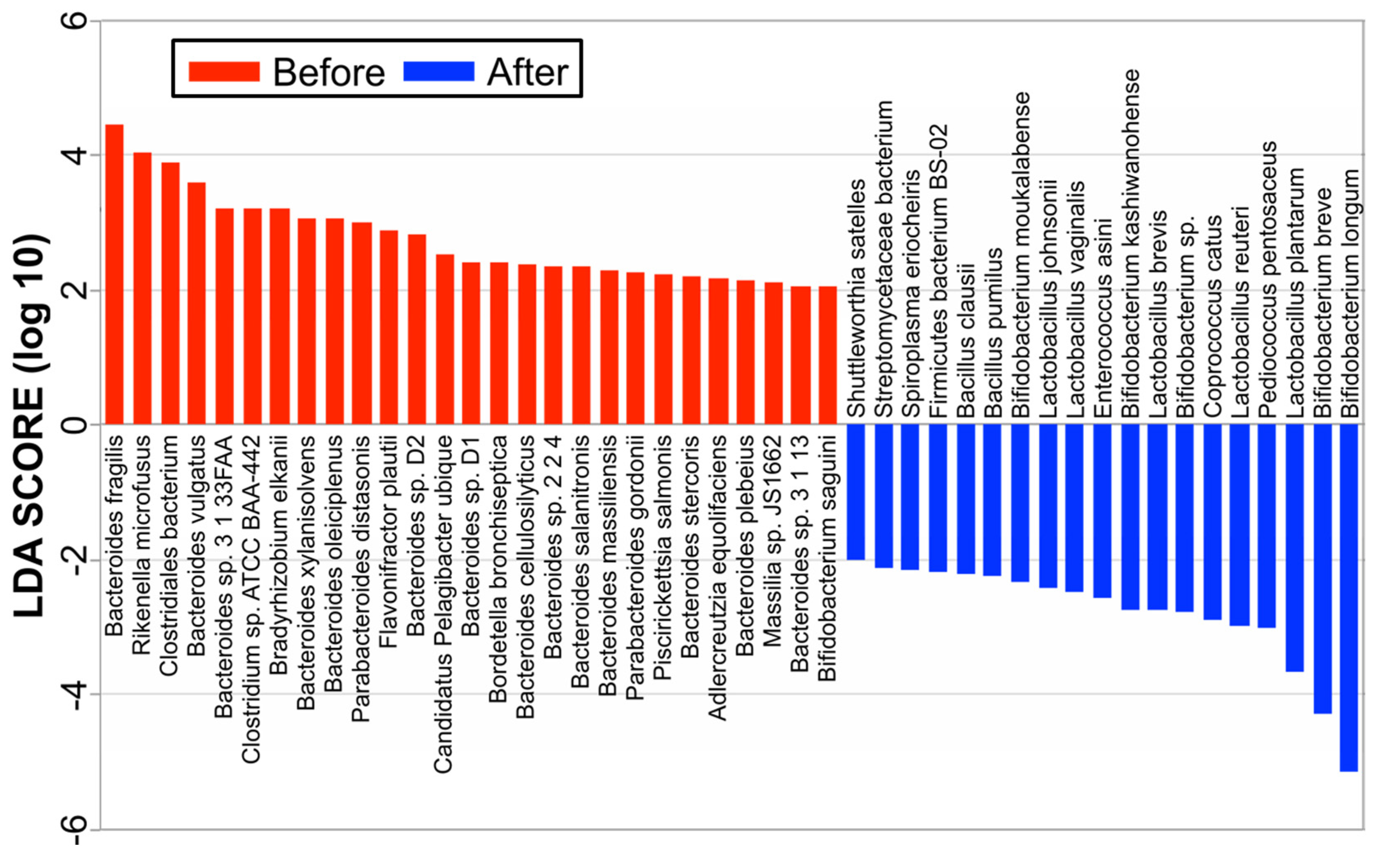
3.3. Linear Discriminant Analysis Effect Size (LEfSe) at the Species Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oka, A.; Sartor, R.B. Microbial-Based and Microbial-Targeted Therapies for Inflammatory Bowel Diseases. Dig. Dis. Sci. 2020, 65, 757–788. [Google Scholar] [CrossRef]
- Jergens, A.E.; Parvinroo, S.; Kopper, J.; Wannemuehler, M.J. Rules of Engagement: Epithelial-Microbe Interactions and Inflammatory Bowel Disease. Front. Med. 2021, 27, 669913. [Google Scholar] [CrossRef]
- Ohkusa, T.; Sato, N.; Ogihara, T.; Morita, K.; Ogawa, M.; Okayasu, I. Fusobacterium varium localized in the colonic mucosa of patients with ulcerative colitis stimulates species-specific antibody. J. Gastroenterol. Hepatol. 2002, 17, 849–853. [Google Scholar] [CrossRef]
- Ohkusa, T.; Okayasu, I.; Ogihara, T.; Morita, K.; Ogawa, M.; Sato, N. Induction of experimental ulcerative colitis by Fusobacterium varium isolated from colonic mucosa of patients with ulcerative colitis. Gut 2003, 52, 79–83. [Google Scholar] [CrossRef]
- Ohkusa, T.; Kato, K.; Terao, S.; Chiba, T.; Mabe, K.; Murakami, K.; Mizokami, Y.; Sugiyama, T.; Yanaka, A.; Takeuchi, Y.; et al. Newly developed antibiotic combination therapy for ulcerative colitis: A double-blind placebo-controlled multicenter trial. Am. J. Gastroenterol. 2010, 105, 1820–1829. [Google Scholar] [CrossRef]
- Nomura, T.; Ohkusa, T.; Okayasu, I.; Yoshida, T.; Sakamoto, M.; Hayashi, H.; Benno, Y.; Hirai, S.; Hojo, M.; Kobayashi, O.; et al. Mucosa-associated baceria in ulcerative colitis before and after antibiotic combination therapy. Aliment. Pharmacol. Ther. 2005, 21, 1017–1027. [Google Scholar] [CrossRef]
- Nishikawa, Y.; Sato, N.; Tsukinaga, S.; Uchiyama, K.; Koido, S.; Ishikawa, D.; Ohkusa, T. Long-term outcomes of antibiotic combination therapy for ulcerative colitis. Ther. Adv. Chronic Dis. 2021, 12, 20406223211028790. [Google Scholar] [CrossRef]
- Eindor-Abarbanel, A.; Healey, G.R.; Jacobson, K. Therapeutic Advances in Gut Microbiome Modulation in Patients with Inflammatory Bowel Disease from Pediatrics to Adulthood. Int. J. Mol. Sci. 2021, 22, 12506. [Google Scholar] [CrossRef]
- Haifer, C.; Paramsothy, S.; Kaakoush, N.O.; Saikal, A.; Ghaly, S.; Yang, T.; Luu, L.D.W.; Borody, T.J.; Leong, R.W. Lyophilised oral faecal microbiota transplantation for ulcerative colitis (LOTUS): A randomised, double-blind, placebo-controlled trial. Lancet Gastroenterol. Hepatol. 2022, 7, 141–151. [Google Scholar] [CrossRef]
- Matson, V.; Chervin, C.S.; Gajewski, T.F. Cancer and the Microbiome-Influence of the Commensal Microbiota on Cancer, Immune Responses, and Immunotherapy. Gastroenterology 2021, 160, 600–613. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Olson, A.; Johanns, J.; Travers, S.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2005, 353, 2462–2476. [Google Scholar] [CrossRef]
- Amiot, A.; Filippi, J.; Abitbol, V.; Cadiot, G.; Laharie, D.; Serrero, M.; Altwegg, R.; Bouhnik, Y.; Peyrin-Biroulet, L.; Gilletta, C.; et al. UC-USK-GETAID Study Group. Effectiveness and safety of ustekinumab induction therapy for 103 patients with ulcerative colitis: A GETAID multicenter real-world cohort study. Aliment. Pharmacol. Ther. 2020, 51, 1039–1046. [Google Scholar] [CrossRef]
- Li, H.; Durbin, R. Fast and accurate long-read alignment with Burrows–Wheeler transform. Bioinformatics. 2010, 26, 589–595. [Google Scholar] [CrossRef]
- Huson, D.H.; Mitra, S.; Ruscheweyh, H.J.; Weber, N.; Schuster, S.C. Integrative analysis of environmental sequences using MEGAN4. Genome Res. 2011, 21, 1552–1560. [Google Scholar] [CrossRef]
- Anderson, K.E.; Russell, J.A.; Moreau, C.S.; Kautz, S.; Sullam, K.E.; Hu, Y.; Basinger, U.; Mott, B.M.; Buck, N.; Wheeler, D.E. Highly similar microbial communities are shared among related and trophically similar ant species. Mol. Ecol. 2012, 21, 2282–2296. [Google Scholar] [CrossRef]
- Segata, N.; Izard, J.; Waldron, L.; Gevers, D.; Miropolsky, L.; Garrett, W.S.; Huttenhower, C. Metagenomic biomarker discovery and explanation. Genome Biol. 2011, 12, R60. [Google Scholar] [CrossRef]
- Sarbagili-Shabat, C.; Albenberg, L.; Van Limbergen, J.; Pressman, N.; Otley, A.; Yaakov, M.; Wine, E.; Weiner, D.; Levine, A. A Novel UC Exclusion Diet and Antibiotics for Treatment of Mild to Moderate Pediatric Ulcerative Colitis: A Prospective Open-Label Pilot Study. Nutrients 2021, 13, 3736. [Google Scholar] [CrossRef]
- Turner, D.; Bishai, J.; Reshef, L.; Abitbol, G.; Focht, G.; Marcus, D.; Ledder, O.; Lev-Tzion, R.; Orlanski-Meyer, E.; Yerushalmi, B.; et al. Antibiotic Cocktail for Pediatric Acute Severe Colitis and the Microbiome: The PRASCO Randomized Controlled Trial. Inflamm. Bowel Dis. 2020, 26, 1733–1742. [Google Scholar] [CrossRef]
- Breton, J.; Kastl, A.; Hoffmann, N.; Rogers, R.; Grossman, A.B.; Mamula, P.; Kelsen, J.R.; Baldassano, R.N.; Albenberg, L. Efficacy of Combination Antibiotic Therapy for Refractory Pediatric Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 1586–1593. [Google Scholar] [CrossRef]
- Kordy, K.; Romeo, A.C.; Lee, D.J.; Li, F.; Zabih, S.; Saavedra, M.; Cunningham, N.J.; Tobin, N.; Aldrovandi, G.M. Combination Antibiotics Improves Disease Activity and Alters Microbial Communities in Children with Ulcerative Colitis. J. Pediatr. Gastroenterol. Nutr. 2018, 67, e60–e63. [Google Scholar] [CrossRef]
- Mishra, S.; Mandavdhare, H.S.; Singh, H.; Choudhury, A.; Shah, J.; Ram, S.; Kalsi, D.; Samanta, J.; Prasad, K.K.; Sharma, A.K.; et al. Adjuvant use of combination of antibiotics in acute severe ulcerative colitis: A placebo controlled randomized trial. Expert. Rev. Anti Infect. Ther. 2021, 19, 949–955. [Google Scholar] [CrossRef]
- Koido, S.; Ohkusa, T.; Kajiura, T.; Shinozaki, J.; Suzuki, M.; Saito, K.; Takakura, K.; Tsukinaga, S.; Odahara, S.; Yukawa, T.; et al. Long-term alteration of intestinal microbiota in patients with ulcerative colitis by antibiotic combination therapy. PLoS ONE 2014, 9, e86702. [Google Scholar] [CrossRef]
- Reshef, L.; Kovacs, A.; Ofer, A.; Yahav, L.; Maharshak, N.; Keren, N.; Konikoff, F.M.; Tulchinsky, H.; Gophna, U.; Dotan, I. Pouch inflammation is associated with a decrease in specific bacterial taxa. Gastroenterology 2015, 149, 718–727. [Google Scholar] [CrossRef]
- Kostic, A.D.; Xavier, R.J.; Gevers, D. The microbiome in inflammatory bowel disease: Current status and the future ahead. Gastroenterology 2014, 146, 1489–1499. [Google Scholar] [CrossRef]
- Tahara, T.; Shibata, T.; Kawamura, T.; Okubo, M.; Ichikawa, Y.; Sumi, K.; Miyata, M.; Ishizuka, T.; Nakamura, M.; Nagasaka, M.; et al. Fusobacterium detected in colonic biopsy and clinicopathological features of ulcerative colitis in Japan. Dig. Dis. Sci. 2015, 60, 205–210. [Google Scholar] [CrossRef]
- Paramsothy, S.; Nielsen, S.; Kamm, M.A.; Deshpande, N.P.; Faith, J.J.; Clemente, J.C.; Paramsothy, R.; Walsh, A.J.; van den Bogaerde, J.; Samuel, D.; et al. Specific bacteria and metabolites associated with response to fecal microbiota transplantation in patients with ulcerative colitis. Gastroenterology 2019, 156, 1440–1454.e2. [Google Scholar] [CrossRef]
- Ott, S.J.; Musfeldt, M.; Wenderoth, D.F.; Hampe, J.; Brant, O.; Fölsch, U.R.; Timmis, K.N.; Schreiber, S. Reduction in diversity of the colonic mucosa associated bacterial microflora in patients with active inflammatory bowel disease. Gut 2004, 53, 685–693. [Google Scholar] [CrossRef]
- Lepage, P.; Häsler, R.; Spehlmann, M.E.; Rehman, A.; Zvirbliene, A.; Begun, A.; Ott, S.; Kupcinskas, L.; Doré, J.; Raedler, A.; et al. Twin study indicates loss of interaction between microbiota and mucosa of patients with ulcerative colitis. Gastroenterology 2011, 141, 227–236. [Google Scholar] [CrossRef]
- White, R.; Atherly, T.; Guard, B.; Rossi, G.; Wang, C.; Mosher, C.; Webb, C.; Hill, S.; Ackermann, M.; Sciabarra, P.; et al. Randomized, controlled trial evaluating the effect of multistrain probiotic on the mucosal microbiota in canine idiopathic inflammatory bowel disease. Gut Microbes 2017, 8, 451–466. [Google Scholar] [CrossRef]
- Sugahara, H.; Odamaki, T.; Fukuda, S.; Kato, T.; Xiao, J.-Z.; Abe, F.; Kikuchi, J.; Ohno, H. Probiotic Bifidobacterium longum alters gut luminal metabolism through modification of the gut microbial community. Sci. Rep. 2015, 5, 13548. [Google Scholar] [CrossRef]
- Ishikawa, D.; Sasaki, T.; Osada, T.; Kuwahara-Arai, K.; Haga, K.; Shibuya, T.; Hiramatsu, K.; Watanabe, S. Changes in Intestinal Microbiota Following Combination Therapy with Fecal Microbial Transplantation and Antibiotics for Ulcerative Colitis. Inflamm. Bowel Dis. 2017, 23, 116–125. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Total | Responder | Nonresponder | |
|---|---|---|---|
| Median age, year (range) | 45 (22–66) | 45 (22–66) | 47 (23–53) |
| Male/female, number of patients | 17/14 | 12/12 | 5/2 |
| Median disease duration, years (range) | 8 (0–30) | 10 (0–30) | 4 (1–9) |
| Partial Mayo score, median (range) | 5 (2–9) | 5 (2–9) | 7 (5–9) |
| Mayo score, median (range, n = 28) | 8 (4–12) | 7 (3–12) | 9 (6–12) |
| Mayo endoscopic score, median (range, n = 28) | 2 (1–3) | 2 (1–3) | 2 (1–3) |
| Extent of disease, number of patients | |||
| Extensive colitis | 20 (65%) | 17 | 3 |
| Left-side colitis | 10 (32%) | 6 | 4 |
| Proctitis | 1 (3%) | 1 | 0 |
| Clinical severity of disease, number of patients | |||
| Severe | 2 (7%) | 1 | 1 |
| Moderate | 25 (81%) | 19 | 6 |
| Mild | 4 (13%) | 3 | 0 |
| Steroid use, number of patients | |||
| Steroid dependent | 17 (55%) | 10 | 7 |
| Steroid resistant | 4 (13%) | 3 | 1 |
| None | 10 (32%) | 8 | 2 |
| Medication, number of patients | |||
| Sulfasalazine | 5 (16%) | 5 | 0 |
| 5-ASA | 24 (77%) | 17 | 7 |
| Corticosteroid | 5 (16%) | 4 | 1 |
| thiopurine | 4 (13%) | 2 | 2 |
| anti-TNF | 2 (6%) | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohkusa, T.; Kato, K.; Sekizuka, T.; Sugiyama, T.; Sato, N.; Kuroda, M. Comparison of the Gut Microbiota of Patients Who Improve with Antibiotic Combination Therapy for Ulcerative Colitis and Those Who Do Not: Investigation by Fecal Metagenomic Analyses. Nutrients 2024, 16, 3500. https://doi.org/10.3390/nu16203500
Ohkusa T, Kato K, Sekizuka T, Sugiyama T, Sato N, Kuroda M. Comparison of the Gut Microbiota of Patients Who Improve with Antibiotic Combination Therapy for Ulcerative Colitis and Those Who Do Not: Investigation by Fecal Metagenomic Analyses. Nutrients. 2024; 16(20):3500. https://doi.org/10.3390/nu16203500
Chicago/Turabian StyleOhkusa, Toshifumi, Kimitoshi Kato, Tsuyoshi Sekizuka, Toshiro Sugiyama, Nobuhiro Sato, and Makoto Kuroda. 2024. "Comparison of the Gut Microbiota of Patients Who Improve with Antibiotic Combination Therapy for Ulcerative Colitis and Those Who Do Not: Investigation by Fecal Metagenomic Analyses" Nutrients 16, no. 20: 3500. https://doi.org/10.3390/nu16203500
APA StyleOhkusa, T., Kato, K., Sekizuka, T., Sugiyama, T., Sato, N., & Kuroda, M. (2024). Comparison of the Gut Microbiota of Patients Who Improve with Antibiotic Combination Therapy for Ulcerative Colitis and Those Who Do Not: Investigation by Fecal Metagenomic Analyses. Nutrients, 16(20), 3500. https://doi.org/10.3390/nu16203500