
ApaI Polymorphism in the Vitamin D Receptor Gene Decreases the Risk of Perianal Fistulas in Crohn’s Disease

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Primary Fibroblast Isolation
2.3. DNA Extraction and Genotyping
2.4. Real Time-PCR
2.5. Statistical Analysis
3. Results
3.1. No Association Is Detected between CD Risk and the VDR FokI, BsmI, ApaI, and TaqI Gene Polymorphisms
3.2. A Linkage Disequilibrium between BsmI, ApaI, and TaqI Is Detected
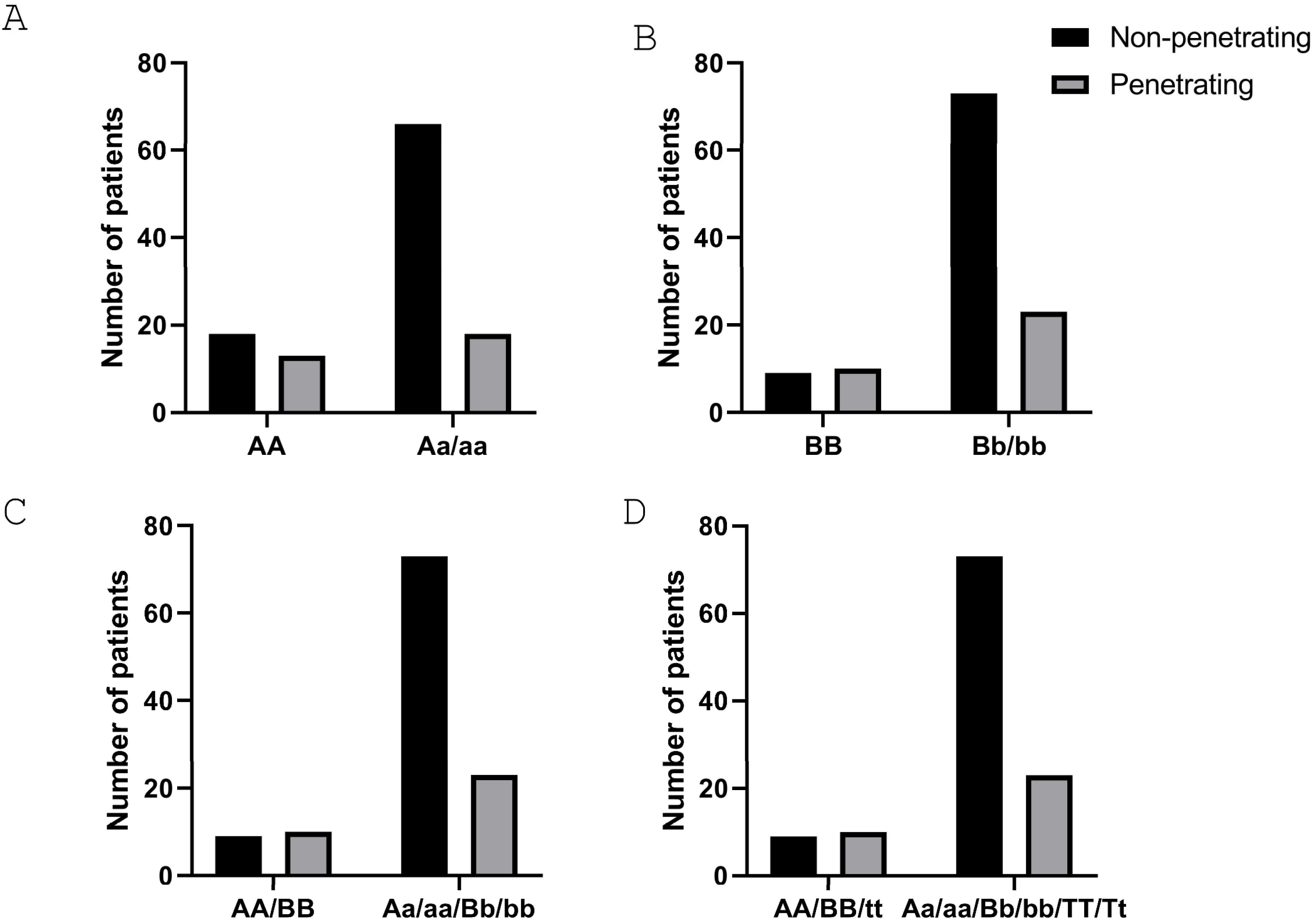
3.3. CD Patients Carrying the aa Genotype Have a Lower Risk of Developing a Perianal Fistula
3.4. CD Patients Carrying the bb Genotype Have a Lower Risk of Requiring Surgery
3.5. No Differences Were Detected in Any of the Clinical Parameters among the Three Genotypes in the FokI SNP of the VDR Gene
3.6. Fibroblasts Carrying the aa Genotype Expressed Lower Levels of Fibrotic Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Verstockt, B.; Bressler, B.; Martinez-Lozano, H.; McGovern, D.; Silverberg, M.S. Time to Revisit Disease Classification in Inflammatory Bowel Disease: Is the Current Classification of Inflammatory Bowel Disease Good Enough for Optimal Clinical Management? Gastroenterology 2022, 162, 1370–1382. [Google Scholar] [CrossRef] [PubMed]
- Householder, S.; Picoraro, J.A. Diagnosis and Classification of Fistula from Inflammatory Bowel Disease and Inflammatory Bowel Disease-Related Surgery. Gastrointest. Endosc. Clin. N. Am. 2022, 32, 631–650. [Google Scholar] [CrossRef] [PubMed]
- Geldof, J.; Iqbal, N.; LeBlanc, J.F.; Anandabaskaran, S.; Sawyer, R.; Buskens, C.; Bemelman, W.; Gecse, K.; Lundby, L.; Lightner, A.L.; et al. Classifying perianal fistulising Crohn’s disease: An expert consensus to guide decision-making in daily practice and clinical trials. Lancet Gastroenterol. Hepatol. 2022, 7, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N.; Panaccione, R.; Nugent, Z.; Marshall, D.A.; Kaplan, G.G.; Vanner, S.; Dieleman, L.A.; Graff, L.A.; Otley, A.; Jones, J.; et al. Crohn’s Disease Phenotypes and Associations with Comorbidities, Surgery Risk, Medications and Nonmedication Approaches: The MAGIC in IMAGINE Study. Inflamm. Bowel Dis. 2024, izae055. [Google Scholar] [CrossRef] [PubMed]
- Annese, V. Genetics and epigenetics of IBD. Pharmacol. Res. 2020, 159, 104892. [Google Scholar] [CrossRef]
- Bakke, D.; Sun, J. Ancient Nuclear Receptor VDR with New Functions: Microbiome and Inflammation. Inflamm. Bowel Dis. 2018, 24, 1149–1154. [Google Scholar] [CrossRef]
- Martin, K.; Radlmayr, M.; Borchers, R.; Heinzlmann, M.; Folwaczny, C. Candidate genes colocalized to linkage regions in inflammatory bowel disease. Digestion 2002, 66, 121–126. [Google Scholar] [CrossRef]
- Simmons, J.D.; Mullighan, C.; Welsh, K.I.; Jewell, D.P. Vitamin D receptor gene polymorphism: Association with Crohn’s disease susceptibility. Gut 2000, 47, 211–214. [Google Scholar] [CrossRef]
- Xue, L.N.; Xu, K.Q.; Zhang, W.; Wang, Q.; Wu, J.; Wang, X.Y. Associations between vitamin D receptor polymorphisms and susceptibility to ulcerative colitis and Crohn’s disease: A meta-analysis. Inflamm. Bowel Dis. 2013, 19, 54–60. [Google Scholar] [CrossRef]
- Wang, L.; Wang, Z.T.; Hu, J.J.; Fan, R.; Zhou, J.; Zhong, J. Polymorphisms of the vitamin D receptor gene and the risk of inflammatory bowel disease: A meta-analysis. Genet. Mol. Res. 2014, 13, 2598–2610. [Google Scholar] [CrossRef]
- Xia, S.L.; Lin, X.X.; Guo, M.D.; Zhang, D.G.; Zheng, S.Z.; Jiang, L.J.; Jin, J.; Lin, X.Q.; Ding, R.; Jiang, Y. Association of vitamin D receptor gene polymorphisms and serum 25-hydroxyvitamin D levels with Crohn’s disease in Chinese patients. J. Gastroenterol. Hepatol. 2016, 31, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Naderi, N.; Farnood, A.; Habibi, M.; Derakhshan, F.; Balaii, H.; Motahari, Z.; Agah, M.R.; Firouzi, F.; Rad, M.G.; Aghazadeh, R.; et al. Association of vitamin D receptor gene polymorphisms in Iranian patients with inflammatory bowel disease. J. Gastroenterol. Hepatol. 2008, 23, 1816–1822. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.Y.; Shu, X.L.; Zhao, H.; Yu, J.D.; Ma, M.; Chen, J. Association between vitamin D receptor gene polymorphisms and pediatric Crohn’s disease in China: A study based on gene sequencing. Zhongguo Dang Dai Er Ke Za Zhi 2013, 15, 1006–1008. [Google Scholar]
- Limketkai, B.N.; Singla, M.B.; Rodriguez, B.; Veerappan, G.R.; Betteridge, J.D.; Ramos, M.A.; Hutfless, S.M.; Brant, S.R. Levels of Vitamin D Are Low After Crohn’s Disease Is Established but Not Before. Clin. Gastroenterol. Hepatol. 2020, 18, 1769–1776 e1761. [Google Scholar] [CrossRef] [PubMed]
- Gisbert-Ferrandiz, L.; Salvador, P.; Ortiz-Masia, D.; Macias-Ceja, D.C.; Orden, S.; Esplugues, J.V.; Calatayud, S.; Hinojosa, J.; Barrachina, M.D.; Hernandez, C. A Single Nucleotide Polymorphism in the Vitamin D Receptor Gene Is Associated with Decreased Levels of the Protein and a Penetrating Pattern in Crohn’s Disease. Inflamm. Bowel Dis. 2018, 24, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Cusato, J.; Cafasso, C.; Antonucci, M.; Palermiti, A.; Manca, A.; Caviglia, G.P.; Vernero, M.; Armandi, A.; Saracco, G.M.; D’Avolio, A.; et al. Correlation between Polymorphisms of Vitamin D Metabolism Genes and Perianal Disease in Crohn’s Disease. Biomedicines 2024, 12, 320. [Google Scholar] [CrossRef]
- Gisbert-Ferrandiz, L.; Cosin-Roger, J.; Hernandez, C.; Macias-Ceja, D.C.; Ortiz-Masia, D.; Salvador, P.; Wildenberg, M.E.; Esplugues, J.V.; Alos, R.; Navarro, F.; et al. The vitamin D receptor Taq I polymorphism is associated with reduced VDR and increased PDIA3 protein levels in human intestinal fibroblasts. J. Steroid Biochem. Mol. Biol. 2020, 202, 105720. [Google Scholar] [CrossRef]
- Macias-Ceja, D.C.; Ortiz-Masia, D.; Salvador, P.; Gisbert-Ferrandiz, L.; Hernandez, C.; Hausmann, M.; Rogler, G.; Esplugues, J.V.; Hinojosa, J.; Alos, R.; et al. Succinate receptor mediates intestinal inflammation and fibrosis. Mucosal Immunol. 2019, 12, 178–187. [Google Scholar] [CrossRef]
- Hughes, D.J.; McManus, R.; Neary, P.; O’Morain, C.; O’Sullivan, M. Common variation in the vitamin D receptor gene and risk of inflammatory bowel disease in an Irish case-control study. Eur. J. Gastroenterol. Hepatol. 2011, 23, 807–812. [Google Scholar] [CrossRef]
- Lye, M.S.; Tor, Y.S.; Tey, Y.Y.; Shahabudin, A.; Loh, S.P.; Ibrahim, N.; Stanslas, J.; Rosli, R.; Ling, K.H. BsmI-ApaI-TaqI TAC (BAt) Haplotype of Vitamin D Receptor Gene Is Associated with Increased Risk of Major Depressive Disorder. J. Mol. Neurosci. 2021, 71, 981–990. [Google Scholar] [CrossRef]
- Cao, S.; Colonna, M.; Deepak, P. Pathogenesis of Perianal Fistulising Crohn’s Disease: Current Knowledge, Gaps in Understanding, and Future Research Directions. J. Crohn’s Colitis 2023, 17, 1010–1022. [Google Scholar] [CrossRef] [PubMed]
- Lenti, M.V.; Santacroce, G.; Broglio, G.; Rossi, C.M.; Di Sabatino, A. Recent advances in intestinal fibrosis. Mol. Asp. Med. 2024, 96, 101251. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Yu, T.; Cong, Y. Stromal Cell Regulation of Intestinal Inflammatory Fibrosis. Cell. Mol. Gastroenterol. Hepatol. 2024, 17, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhou, Y.; Wen, D.; Wang, J. Noncoding RNAs: Master Regulator of Fibroblast to Myofibroblast Transition in Fibrosis. Int. J. Mol. Sci. 2023, 24, 1801. [Google Scholar] [CrossRef]
- Ferrer-Suay, S.; Alonso-Iglesias, E.; Tortajada-Girbes, M.; Carrasco-Luna, J.; Codoner-Franch, P. Vitamin D receptor gene ApaI and FokI polymorphisms and its association with inflammation and oxidative stress in vitamin D sufficient Caucasian Spanish children. Transl. Pediatr. 2021, 10, 103–111. [Google Scholar] [CrossRef]
- Seco-Cervera, M.; Ortiz-Masia, D.; Macias-Ceja, D.C.; Coll, S.; Gisbert-Ferrandiz, L.; Cosin-Roger, J.; Bauset, C.; Ortega, M.; Heras-Moran, B.; Navarro-Vicente, F.; et al. Resistance to apoptosis in complicated Crohn’s disease: Relevance in ileal fibrosis. Biochim. Biophys. Acta Mol. Basis Dis. 2024, 1870, 166966. [Google Scholar] [CrossRef]
- Gisbert-Ferrándiz, L.; Cosín-Roger, J.; Hernández, C.; Macias-Ceja, D.C.; Ortiz-Masiá, D.; Salvador, P.; Esplugues, J.V.; Hinojosa, J.; Navarro, F.; Calatayud, S.; et al. Diminished Vitamin D Receptor Protein Levels in Crohn’s Disease Fibroblasts: Effects of Vitamin D. Nutrients 2020, 12, 973. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| CD Patients | n = 115 |
|---|---|
| Gender | |
| Female | 63 (54.7%) |
| Male | 52 (45.2%) |
| Age at diagnosis (mean ± SD; years) | 28.07 ± 12.67 |
| A1 (<17 years) | 15 (13.0%) |
| A2 (17–40 years) | 78 (67.8%) |
| A3 (>40 years) | 22 (19.1%) |
| Follow-up time (mean ± SD; years) | 11.26 ± 10.62 |
| Disease location | |
| L1—ileal | 57 (49.6%) |
| L2—colonic | 15 (13.0%) |
| L3—ileocolonic | 33 (28.7%) |
| L4—upper GI a | 10 (7%) |
| Disease behavior | |
| B1—inflammatory | 52 (45.2%) |
| B2—stricturing | 32 (27%) |
| B3—penetrating | 31 (26.9%) |
| Surgery | 47 (40.8%) |
| Perianal fistula | 41 (35.6%) |
| EIM b | 28 (24.3%) |
| Family history | 11 (9%) |
| Smoker or ex-smoker | 45 (38%) |
| CD Patients | n = 10 |
|---|---|
| Gender | |
| Female | 7 (70%) |
| Male | 3 (30%) |
| Age (mean ± SD; years) | 47.9 ± 20.32 |
| Disease location | |
| L1—ileal | 7 (70%) |
| L2—colonic | 0 (0%) |
| L3—ileocolonic | 3 (30%) |
| L4—upper GI a | 0 (0%) |
| Disease behavior | |
| B1—inflammatory | 0 (0%) |
| B2—stricturing | 5 (50%) |
| B3—penetrating | 5 (50%) |
| Sense Primer (5′–3′) | Antisense Primer (5′–3′) | T Annealing (°C) | Enzyme Restriction | T Enzyme (°C) | |
|---|---|---|---|---|---|
| rs7975232 (ApaI) | CAGAGCATGGACAGGGAGCAA | GCAACTCCTCATGGCTGAGGTCTC | 60 | ApaI (R0114S) | 25 |
| rs1544410 (BsmI) | CAACCAAGACTACAAGTACCGCGTCAGTGA | AACCAGCGGGAAGAGGTCAAGGG | 65 | BsmI (R0134S) | 65 |
| rs2228570 (FokI) | AGCTGGCCCTGGCACTGACTCTGCTCT | ATGGAAACACCTTGCTTCTTCCCTCTC | 60 | FokI (R0109S) | 37 |
| rs731236 (TaqI) | ATGCACGGAGAAGTCACTGG | GGTCGGCTAGCTTCTGGATC | 60 | TaqI (R0149S) | 65 |
| Sense Primer (5′–3′) | Antisense Primer (5′–3′) | |
|---|---|---|
| VDR | TGGAGACTTTGACCGGAACG | AAGGGGCAGGTGAATAGTGC |
| COL1A1 | GGAGCAGACGGGAGTTTCTC | CCGTTCTGTACGCAGGTGAT |
| COL4A1 | CCGGATCACATTGACATGAAACC | CCGGATCACATTGACATGAAACC |
| COL3A1 | CGCCCTCCTAATGGTCAAGG | TTCTGAGGACCAGTAGGGCA |
| ACTA2 (αSMA) | GACCTTTGGCTTGGCTTGTC | AGCTGCTTCACAGGATTCCC |
| Vimentin | ATGAAGGAGGAAATGGCTCGTC | GGGTATCAACCAGAGGGAGTGAA |
| TNFα | GCTGCACTTTGGAGTGATCG | GGGTTTGCTACAACATGGGC |
| TGFβ1 | GGGCTACCATGCCAACTTCT | GACACAGAGATCCGCAGTCC |
| FSP1 | TCTTGGTTTGATCCTGACTGCT | CCTGTTGCTGTCCAAGTTGC |
| MMP2 | CATTCCCTGCAAAGAACACA | GTATTTGATGGCATCGCTCA |
| MMP3 | TCCTACTGTTGCTGTGCGTG | CTTCCCCGTCACCTCCAATC |
| IL1β | GCTCGCCAGTGAAATGATGG | TCGTGCACATAAGCCTCGTT |
| IL6 | ATGAGGAGACTTGCCTGGTG | CTGGCATTTGTGGTTGGGTC |
| ACTB (βActin) | GGACTTCGAGCAAGAGATGG | AGCACTGTGTTGGCGTACAG |
| Control | CD | Total | p-Value | ||
|---|---|---|---|---|---|
| FokI | FF | 7 (35%) | 45 (39.1%) | 52 | 0.6356 |
| Ff | 9 (45%) | 56 (48.7%) | 65 | ||
| ff | 4 (20%) | 14 (12.2%) | 18 | ||
| ApaI | AA | 8 (40%) | 31 (26.9%) | 39 | 0.1848 |
| Aa | 5 (25%) | 54 (46.9%) | 59 | ||
| aa | 7 (35%) | 30 (26.1%) | 37 | ||
| Bsml | BB | 6 (30%) | 19 (16.5%) | 25 | 0.2858 |
| Bb | 6 (30%) | 51 (44.3%) | 57 | ||
| bb | 8 (40%) | 45 (39.2%) | 53 | ||
| TaqI | TT | 8 (40%) | 45 (39.1%) | 53 | 0.3981 |
| Tt | 6 (30%) | 49 (42.6%) | 55 | ||
| tt | 6 (30%) | 21 (18.2%) | 27 | ||
| SNP | FokI | BsmI | ApaI | TaqI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FF | Ff | ff | BB | Bb | bb | AA | Aa | aa | TT | Tt | tt | ||
| FokI | FF | 6 | 20 | 19 | 9 | 25 | 11 | 20 | 19 | 6 | |||
| Ff | 10 | 26 | 20 | 19 | 22 | 15 | 19 | 25 | 12 | ||||
| ff | 3 | 5 | 6 | 3 | 7 | 4 | 6 | 5 | 3 | ||||
| p | 0.8182 | 0.4772 | 0.7437 | ||||||||||
| BsmI | BB | 19 | 0 | 0 | 0 | 0 | 19 | ||||||
| Bb | 11 | 40 | 0 | 3 | 47 | 1 | |||||||
| bb | 1 | 14 | 30 | 42 | 2 | 1 | |||||||
| p | <0.001 | <0.001 | |||||||||||
| ApaI | AA | 2 | 9 | 20 | |||||||||
| Aa | 14 | 39 | 1 | ||||||||||
| aa | 29 | 1 | 0 | ||||||||||
| p | <0.001 | ||||||||||||
| Variable | AA (n = 31) | Aa (n = 54) | aa (n = 30) | p-Value a | |
|---|---|---|---|---|---|
| Gender | |||||
| Female | 18 | 29 | 16 | 0.9114 | |
| Male | 13 | 25 | 14 | ||
| Age at onset | |||||
| A1 + A2 | 28 | 41 | 24 | 0.2647 | |
| A3 | 3 | 13 | 6 | ||
| Location | |||||
| L1 | 17 | 22 | 18 | 0.3153 | |
| L2 | 3 | 11 | 1 | ||
| L3 | 9 | 15 | 9 | ||
| L4 | 2 | 6 | 2 | ||
| Behavior | |||||
| B1 | 13 | 25 | 14 | 0.2098 | |
| B2 | 5 | 18 | 9 | ||
| B3 | 13 | 11 | 7 | ||
| Perianal fistula | |||||
| Yes | 16 | 19 | 6 | 0.0360 | |
| No | 15 | 35 | 24 | ||
| Surgery | |||||
| Yes | 16 | 20 | 11 | 0.3628 | |
| No | 15 | 34 | 19 | ||
| EIM b | |||||
| Yes | 5 | 15 | 8 | 0.4563 | |
| No | 26 | 39 | 22 | ||
| Variable | BB (n = 19) | Bb (n = 51) | bb (n = 45) | p-Value a | |
|---|---|---|---|---|---|
| Gender | |||||
| Female | 12 | 28 | 24 | 0.5434 | |
| Male | 7 | 23 | 21 | ||
| Age at onset | |||||
| A1 + A2 | 17 | 42 | 35 | 0.5359 | |
| A3 | 2 | 9 | 10 | ||
| Location | |||||
| L1 | 10 | 25 | 22 | 0.8812 | |
| L2 | 3 | 6 | 4 | ||
| L3 | 4 | 14 | 16 | ||
| L4 | 2 | 6 | 3 | ||
| Behavior | |||||
| B1 | 6 | 25 | 18 | 0.1036 | |
| B2 | 3 | 16 | 14 | ||
| B3 | 10 | 10 | 13 | ||
| Perianal fistula | |||||
| Yes | 7 | 22 | 13 | 0.3509 | |
| No | 12 | 29 | 32 | ||
| Surgery | |||||
| Yes | 13 | 14 | 20 | 0.0067 | |
| No | 6 | 37 | 25 | ||
| EIM b | |||||
| Yes | 2 | 13 | 13 | 0.2850 | |
| No | 17 | 38 | 32 | ||
| Variable | FF (n = 45) | Ff (n = 56) | ff (n = 14) | p-Value a | |
|---|---|---|---|---|---|
| Gender | |||||
| Female | 25 | 33 | 6 | 0.5564 | |
| Male | 20 | 23 | 8 | ||
| Age at onset | |||||
| A1 + A2 | 40 | 43 | 10 | 0.1939 | |
| A3 | 5 | 13 | 4 | ||
| Location | |||||
| L1 | 21 | 30 | 7 | 0.4100 | |
| L2 | 8 | 4 | 3 | ||
| L3 | 12 | 19 | 2 | ||
| L4 | 4 | 3 | 2 | ||
| Behavior | |||||
| B1 | 20 | 26 | 5 | 0.8227 | |
| B2 | 14 | 13 | 5 | ||
| B3 | 11 | 17 | 4 | ||
| Perianal fistula | |||||
| Yes | 17 | 17 | 6 | 0.5875 | |
| No | 28 | 39 | 8 | ||
| Surgery | |||||
| Yes | 20 | 23 | 4 | 0.5726 | |
| No | 25 | 33 | 10 | ||
| EIM b | |||||
| Yes | 10 | 15 | 3 | 0.8370 | |
| No | 35 | 41 | 11 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gisbert-Ferrándiz, L.; Llau, J.; Ortiz-Masia, D.; Cosín-Roger, J.; Macias-Ceja, D.C.; Hinojosa, J.; Calatayud, S.; Barrachina, M.D. ApaI Polymorphism in the Vitamin D Receptor Gene Decreases the Risk of Perianal Fistulas in Crohn’s Disease. Nutrients 2024, 16, 3485. https://doi.org/10.3390/nu16203485
Gisbert-Ferrándiz L, Llau J, Ortiz-Masia D, Cosín-Roger J, Macias-Ceja DC, Hinojosa J, Calatayud S, Barrachina MD. ApaI Polymorphism in the Vitamin D Receptor Gene Decreases the Risk of Perianal Fistulas in Crohn’s Disease. Nutrients. 2024; 16(20):3485. https://doi.org/10.3390/nu16203485
Chicago/Turabian StyleGisbert-Ferrándiz, Laura, Jorge Llau, Dolores Ortiz-Masia, Jesús Cosín-Roger, Dulce Carolina Macias-Ceja, Joaquín Hinojosa, Sara Calatayud, and Maria Dolores Barrachina. 2024. "ApaI Polymorphism in the Vitamin D Receptor Gene Decreases the Risk of Perianal Fistulas in Crohn’s Disease" Nutrients 16, no. 20: 3485. https://doi.org/10.3390/nu16203485
APA StyleGisbert-Ferrándiz, L., Llau, J., Ortiz-Masia, D., Cosín-Roger, J., Macias-Ceja, D. C., Hinojosa, J., Calatayud, S., & Barrachina, M. D. (2024). ApaI Polymorphism in the Vitamin D Receptor Gene Decreases the Risk of Perianal Fistulas in Crohn’s Disease. Nutrients, 16(20), 3485. https://doi.org/10.3390/nu16203485