1. Introduction
The alarming surge in obesity and diabetes rates within the USA is reaching critical levels, with 41.9% and 14.7%, respectively among American adults [
1,
2]. In 2022, 43% of adults in the world were overweight and 16% were living with obesity [
3]. Moreover, obesity stands as a significant precursor to diabetes, amplifying the urgency of this health crisis [
3]. Both conditions demand sustained attention and comprehensive care, presenting formidable challenges to public health. Addressing this pressing issue necessitates the development of innovative, sustainable long-term strategies. There has been strong evidence suggesting that both obesity and diabetes have been strongly linked to gut microbiota, the vast community of microbes in our intestines [
4]. Studies have shown that lean mice gained significant weight after transferring gut bacteria from obese mice, suggesting that gut microbiota play a key role in managing body weight [
5,
6]. Other studies in animals and humans demonstrate an inverse relationship between obesity and diversity of gut microbiota, specifically symbionts including genera Bifidobacteria, Lactobacillus, and Verrucomicrobiota (in which Akk belongs to) [
7,
8]. In addition, gut microbiota has been shown to alter low-grade inflammation and insulin resistance upon modification via dietary interventions [
9]. In particular, a group of gut bacterial metabolites such as short-chain fatty acids (SCFAs) are believed play a role in mediating the effects of gut microbiota [
10]. For instance, diabetes patients were found to have a reduced population of SCFAs-producing gut bacteria, suggesting a potential link of gut bacteria with impaired blood sugar control [
4]. Common SCFAs include acetate, butyrate, and propionate, and their anti-obesity and anti-diabetes bioactivities have been widely studied. These findings also suggest that a potential strategy to manage obesity and type 2 diabetes is targeting gut microbiota.
Akk is a gram-negative gut bacterium belonging to the phylum Verrucomicrobia. It is one of the most abundant gut bacteria in humans, representing 3–5% of the microbial community. A. muciniphila was first isolated and identified in 2004 in purified mucin as an oval-shaped, strictly anaerobic bacterium. Akk has the ability to utilize mucus glycans as carbon sources to grow. As a mucin-degrading bacterium, Akk in turn stimulates the growth of the protective gut lining and enhances gut barrier functions [
11,
12]. Akk has recently gained increased research interest due to its potential benefits against obesity and metabolic syndrome. Research has found that Akk is more abundant in healthy subjects than in diabetic and obese patients. Further support comes from intervention studies that have also found an inverse correlation between Akk abundance and body weight, metabolic syndrome, and type 2 diabetes [
13,
14,
15,
16].
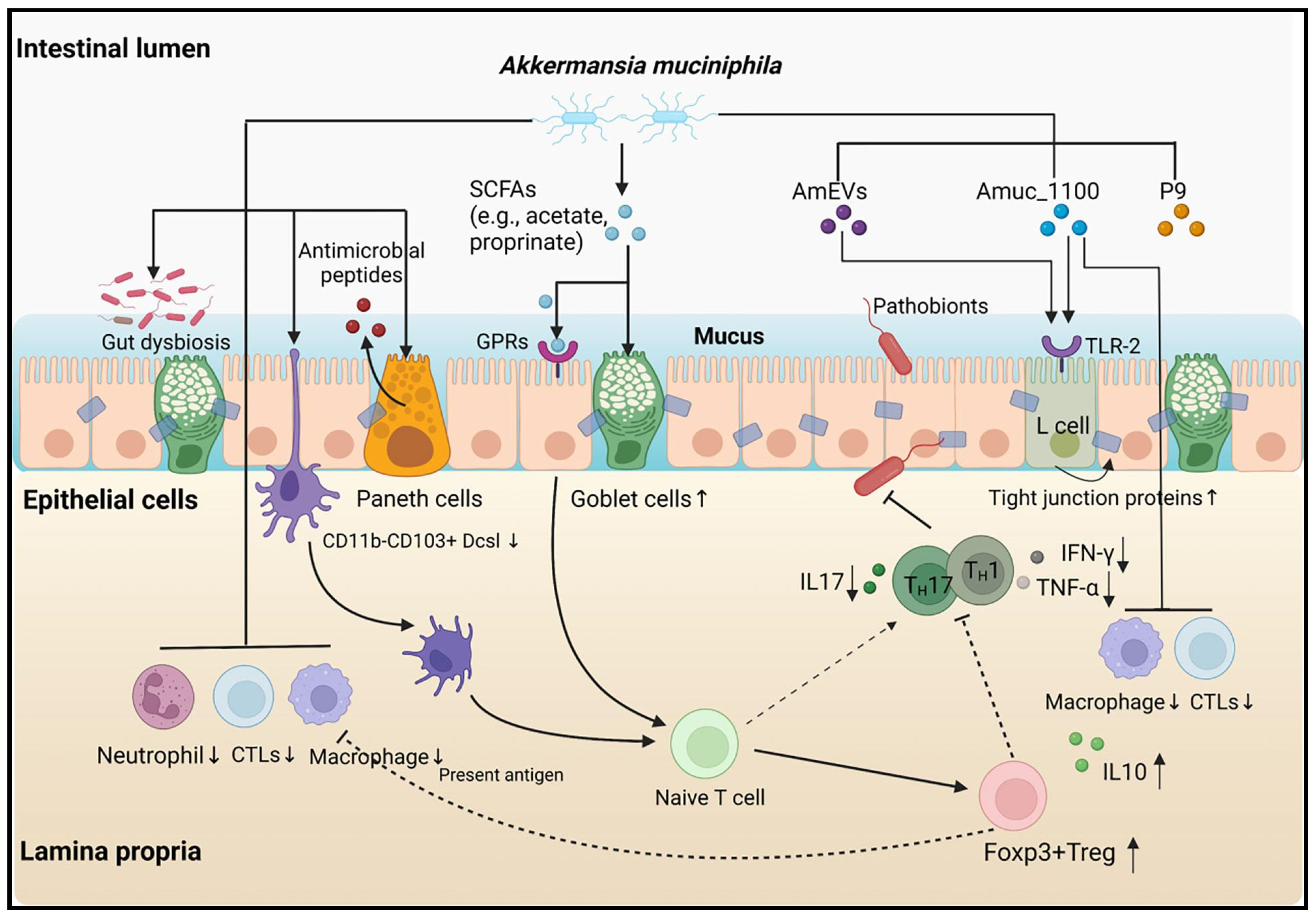
Despite the growing body of evidence suggesting that Akk is a promising probiotic, the exact mechanisms by which it exerts its beneficial impact on health have not been fully elucidated (
Figure 1). Studies have shown that Akk promotes the gut production of short-chain fatty acids (SCFAs), improving insulin resistance and host metabolism—factors linked to obesity and diabetes [
12,
13,
14,
15]. Moreover, Akk has been shown to modify the gut microbiota by stimulating other beneficial gut bacteria such as Bifidobacteria, thereby promoting a healthier gut ecosystem [
13].
There have been a growing number of studies investigating the beneficial role of Akk on obesity and diabetes [
7]. Animal studies have been particularly encouraging. For instance, dietary Akk supplementation has been shown to reduce body weight gain, fasting blood glucose, and insulin resistance in mice fed with a high-fat diet [
14,
15]. Similar findings have been demonstrated in other studies, suggesting the protective role of Akk against obesity and diabetes, though the exact mechanisms are not clear. A recent human trial, while demonstrating improved insulin sensitivity and reduced cholesterol in overweight/obese participants, did not show significant changes in weight or body fat composition [
16]. This discrepancy highlights the need for a more comprehensive analysis of Akk effects on obesity and diabetes. A previous review that compared the effects of Akk on various metabolic diseases found a positive association with the onset of type 2 diabetes following Akk supplementation. However, this association lacked strong evidence [
17]. To address this, our meta-analysis aims to systematically evaluate the latest research and compare the effects of Akk administration in different animal studies. We will employ the most comprehensive subgroup analyses possible to provide a more definitive understanding of the impact of Akk.
4. Discussion
This meta-analysis underscores the multifaceted benefits of Akk intake in mice subjected to a high-fat diet. Overall, dietary supplementation with Akk, as analyzed from nine selected studies, significantly reduced body weight by an average of 10.4%. The dosage of Akk ranged from 2 × 10
8 to 5 × 10
10 CFU/day, which aligns with the dosages commonly used in most probiotic animal studies. Most of the selected studies on Akk used dosages of 2 × 10
8 and 1 × 10
10 CFU. However, two studies by Wang et al. [
40] and Zhang et al. [
43] utilized a higher dose of 5 × 10
10 CFU in mice. Interestingly, both studies showed that Akk had no effect on body weight, despite other studies with lower doses showing a beneficial effect in reducing body weight gain. These results suggest that there is no dose-dependent relationship of Akk in the prevention of body weight gain. The median duration of Akk treatment across the selected nine animal studies was 14 weeks, ranging from 6 to 20 weeks. The most prominent effects of Akk were observed during treatment durations of 6 to 12 weeks. The results suggest that Akk exerts its effect in reducing body weight gain during the early stages of obesity development (as early as 6 weeks), with the probiotic effect likely diminishing over time. For instance, Zhang’s study [
43] extended Akk treatment to 20 weeks at higher dose, but showed no inhibiting effect on body weight gain. Obesity is a chronic disease that requires a long-term solution. The current animal studies were all of short duration (less than 20 weeks). Long-term studies are needed to verify Akk’s effect on obesity development.
The effect of Akk supplementation on the prevention of type 2 diabetes is reflected in its significant reduction of fasting blood glucose (by 21.2%) and improvement in glucose tolerance (by 22.1%), suggesting that Akk treatment is effective in preventing type 2 diabetes. Nine studies have measured fasting blood glucose. Except for two studies, all others showed a significant reduction in fasting blood glucose with Akk treatment. These two studies had a short treatment duration of 6 weeks, while the others were longer, suggesting that Akk may require more than 6 weeks to demonstrate a significant effect on blood glucose. No dose–response relationship was observed across the tested doses between 2 × 10
8 and 5 × 10
10 CFU/day in the nine studies. It was unclear if and how treatment duration affected the efficiency of the probiotic during administration. Additionally, a discrepancy emerged regarding the inclusion of antibiotics, which was the predominant method. In the study by Acharya et al., the administration of the antibiotic before the probiotic was actually more effective than administering the probiotic by itself [
30]. Few authors provided clear justifications for the model choice and dosing parameters utilized in their studies.
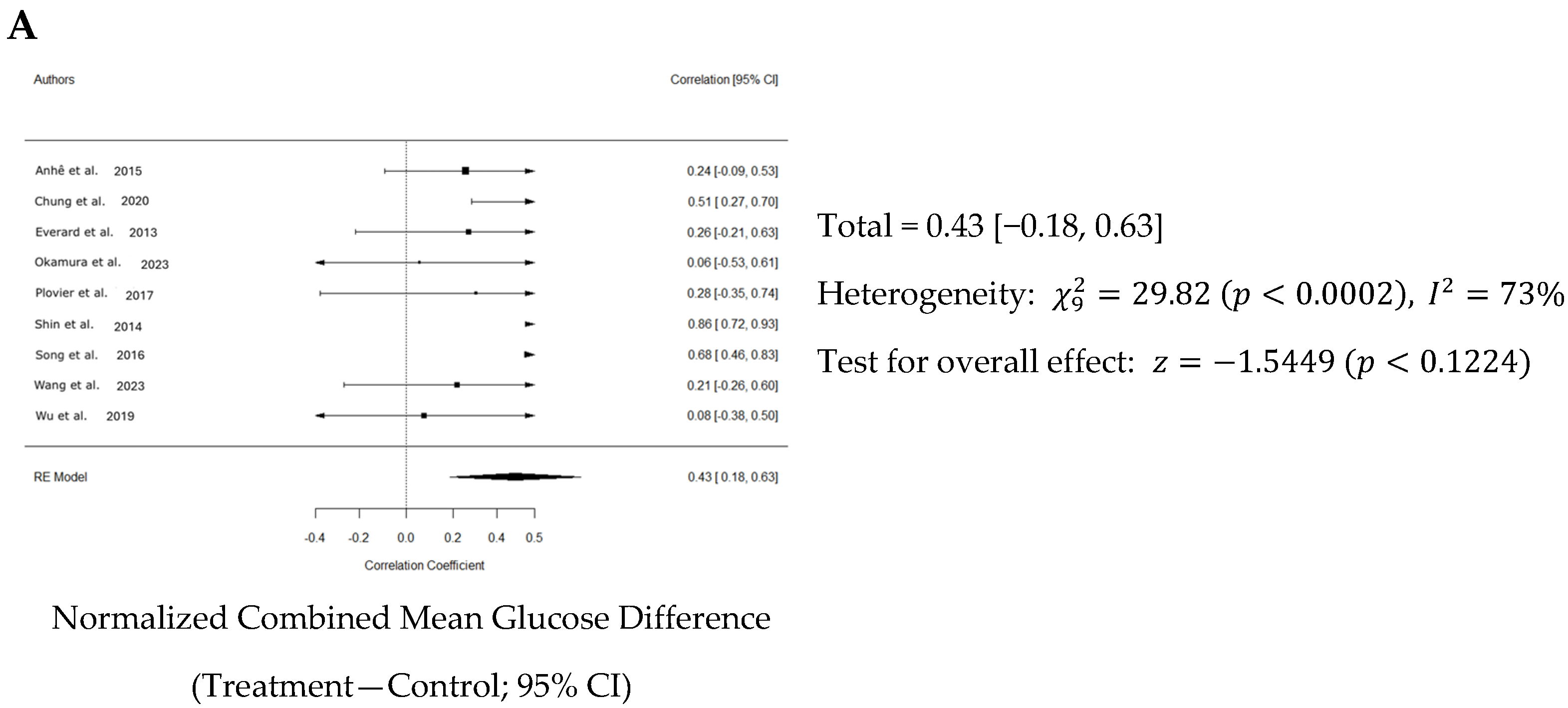
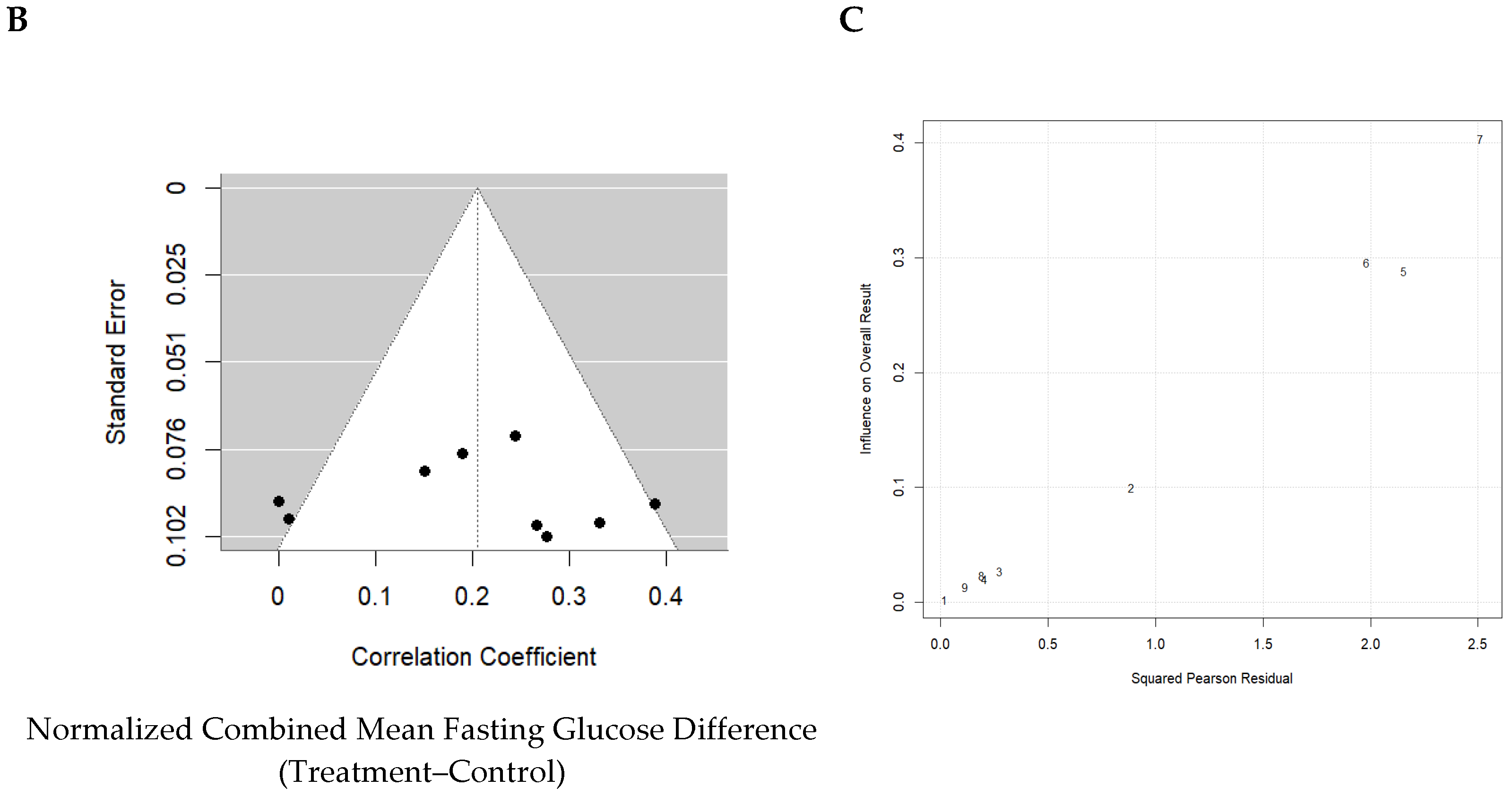
Nine studies measured glucose tolerance. The meta-analysis showed that Akk significantly improved glucose tolerance in mice by reducing the 2 h AUC by 22.1%. However, there was substantial variation in the results across studies, as reflected by I2 = 73%. Indeed, six of nine studies showed modest but non-significant effects. The median duration of Akk treatment across studies was 12 weeks, ranging from 6 to 16 weeks. Shin et al. found that six weeks of Akk treatment significantly reduced DIO mice 2 h AUC by an estimated 27.3%. This mouse study of Akk treatment showed the most prominent effect among the studies with a normalized effect size of 0.856. Plovier et al. also investigated six weeks of Akk treatment on mouse glucose tolerance but with a lower dose (2 × 108 CFU/d versus 1 × 1010 CFU/d in Shin’s study) and found no significant effect. The other two studies with significant effects by Akk treatment also used doses at or above 1 × 1010 CFU/d, suggesting that the Akk treatment dose may need to be no less than 1 × 1010 CFU/d to be effective. It should be noted that one study by Wang et al. used a model of FFAR4 knockout mice, which has been shown to cause severely impaired glucose tolerance under high-fat feeding conditions. FFAR4 regulates glucagon-like peptide 1 secretion by modifying Akk abundance. However, our meta-analysis showed that Akk treatment at 5 × 1010 CFU/d for 12 weeks in Wang’s study did not significantly improve glucose tolerance. There was substantial heterogeneity among the studies. The studies differed in terms of doses, duration, sample size, and other factors, which could significantly influence the results. Further research is needed to confirm the consistency and magnitude of the effect of Akk on glucose tolerance. Overall, fasting blood glucose decreased by 21.2%, whilst blood insulin increased by 26.9% when comparing control to treatment groups likely because insulin and blood glucose are inversely correlated.
Thirteen studies investigated the effect of Akk treatment on blood insulin levels in animals. The meta-analysis revealed a significant increase in blood insulin levels, from 1.9 to 2.6 µg/mL. Notably, three studies—Zhang et al. [
43], Chung et al. [
33], and Zhai et al. [
42]—demonstrated strong treatment effects, with effect sizes of 1.64, 1.44, and 1.17, respectively. Interestingly, all three studies also reported significant reductions in fasting blood glucose levels. Additionally, some studies explored the anti-inflammatory efficacy of Akk; however, due to the heterogeneity of inflammation biomarkers across blood and tissue, a meta-analysis on the anti-inflammatory effects was not feasible.
One of the primary objectives of this meta-analysis was to identify the variables that contribute to the efficacy of Akk, such as changes in body weight and treatment duration. Surprisingly, the random-effects meta-regression model is not able to determine these expected variables. A random-effects model was selected for meta-regression because of the aforementioned variables in study design, such as probiotic duration, infusion parameters (including temperature, rate volume), and overall methodological quality. Notably, treatment duration which has been a critical determinant of efficacy in previous studies (both preclinical and clinical), did not emerge as a significant factor in our analysis [
20,
28]. This discrepancy might be due to the limited exploration of treatment durations in the analyzed studies. Only one study specifically investigated the impact of different treatment durations, reporting no significant effect of the probiotic beyond 14 weeks [
18].
There are several limitations leading to inclusive results in our meta-regression models. First, the limited number of studies assessing fasting blood glucose levels restricted our ability to conduct a comprehensive meta-regression due to constraints in degrees of freedom [
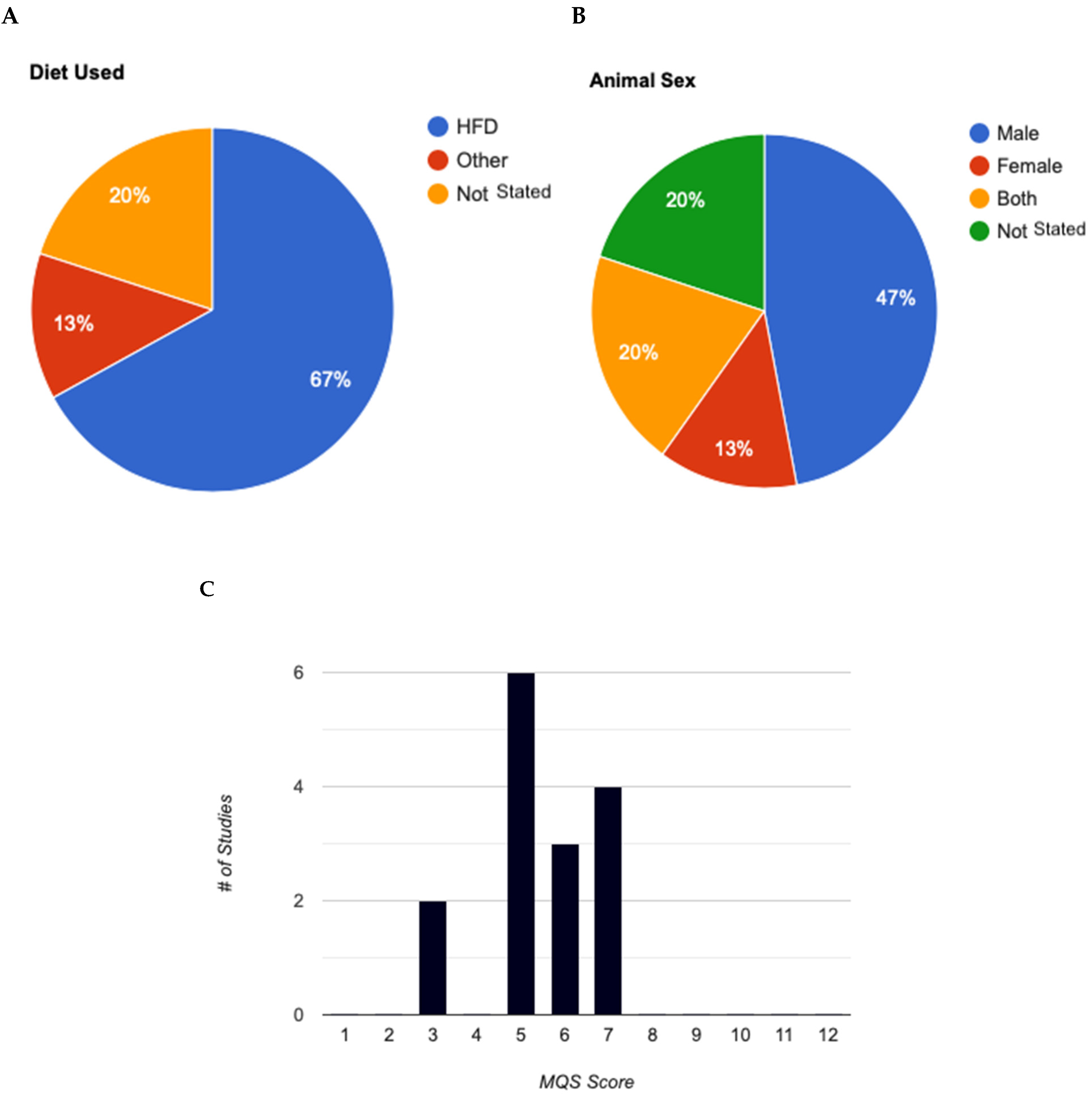
45]. Second, the presence of substantial variability among studies can compromise the power of meta-regression. Our analysis revealed significant variation between studies, as indicated by heterogeneity statistics in our primary endpoints model. This could be due to factors such as system errors among different laboratories, such as experiment duration, sample preparation, and administration parameters of Akk. Third, the animal models used (age, sex, and species) were inconsistent. This significant methodological and model variability among the studies made it challenging to identify clear cause-and-effect relationships. Fourth, most studies employed young, male C57BL/6J mice. Only two studies included female mice, but neither considered biological sex as a variable parameter or specified the number of females per group. Consequently, the potential effects of Akk on female animals remain unclear. Moreover, the inconclusive results regarding microbiota suggest that Akk’s influence on gut microbiota might be more critical than its direct metabolic effects on parameters such as blood glucose levels. On the other hand, the current data make it difficult to definitively determine the key factors influencing treatment outcomes.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}