
Altered Nutrient Composition of Lactose-Reduced Infant Formula

Abstract
1. Introduction
2. Materials and Methods
2.1. Formula Subgroup Categorization
2.2. Nutrient Information
2.3. Sugars
2.4. Glycemic Index
2.5. Fat Components
2.6. Protein Components
2.7. Statistical Analysis
3. Results
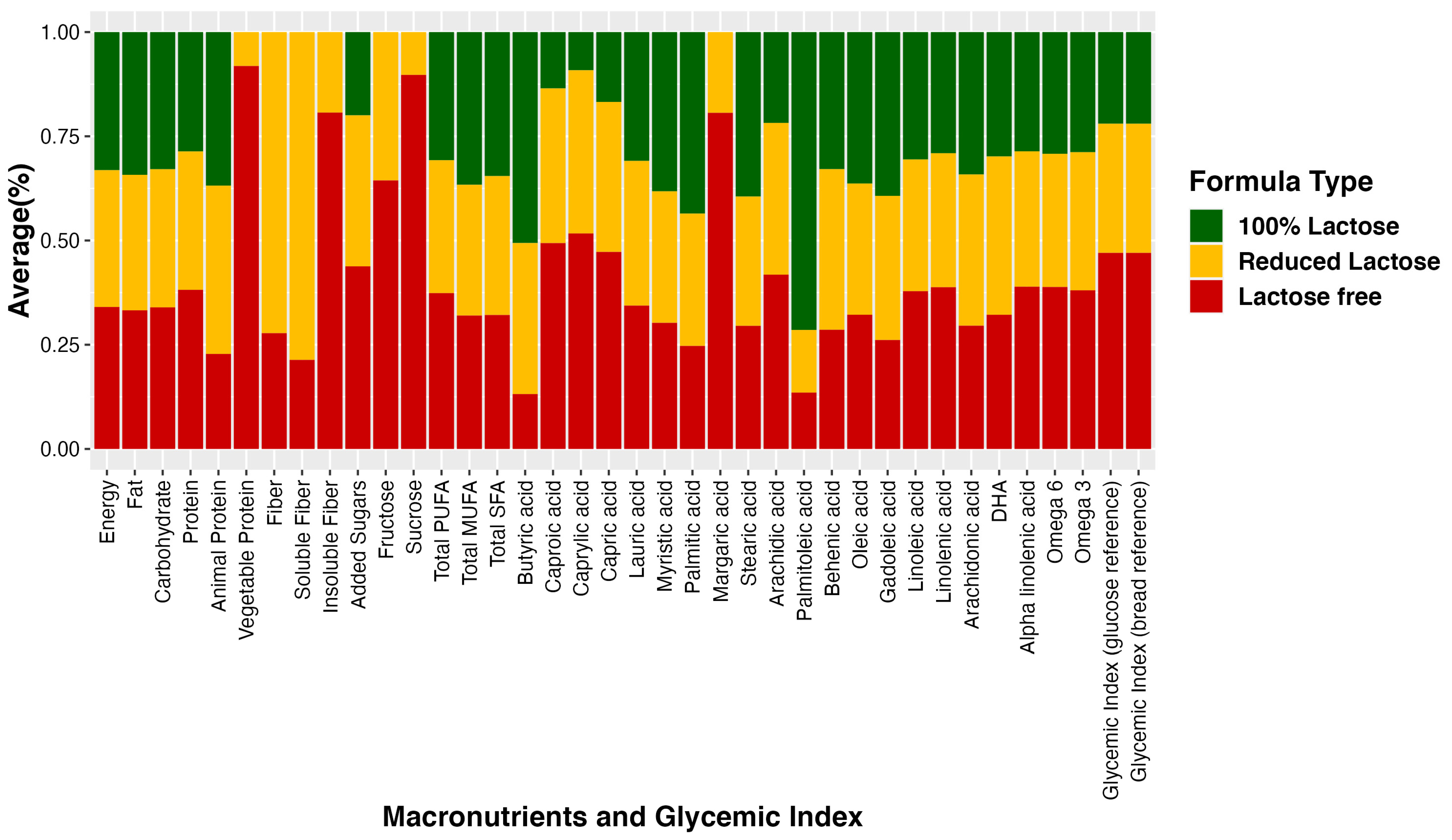
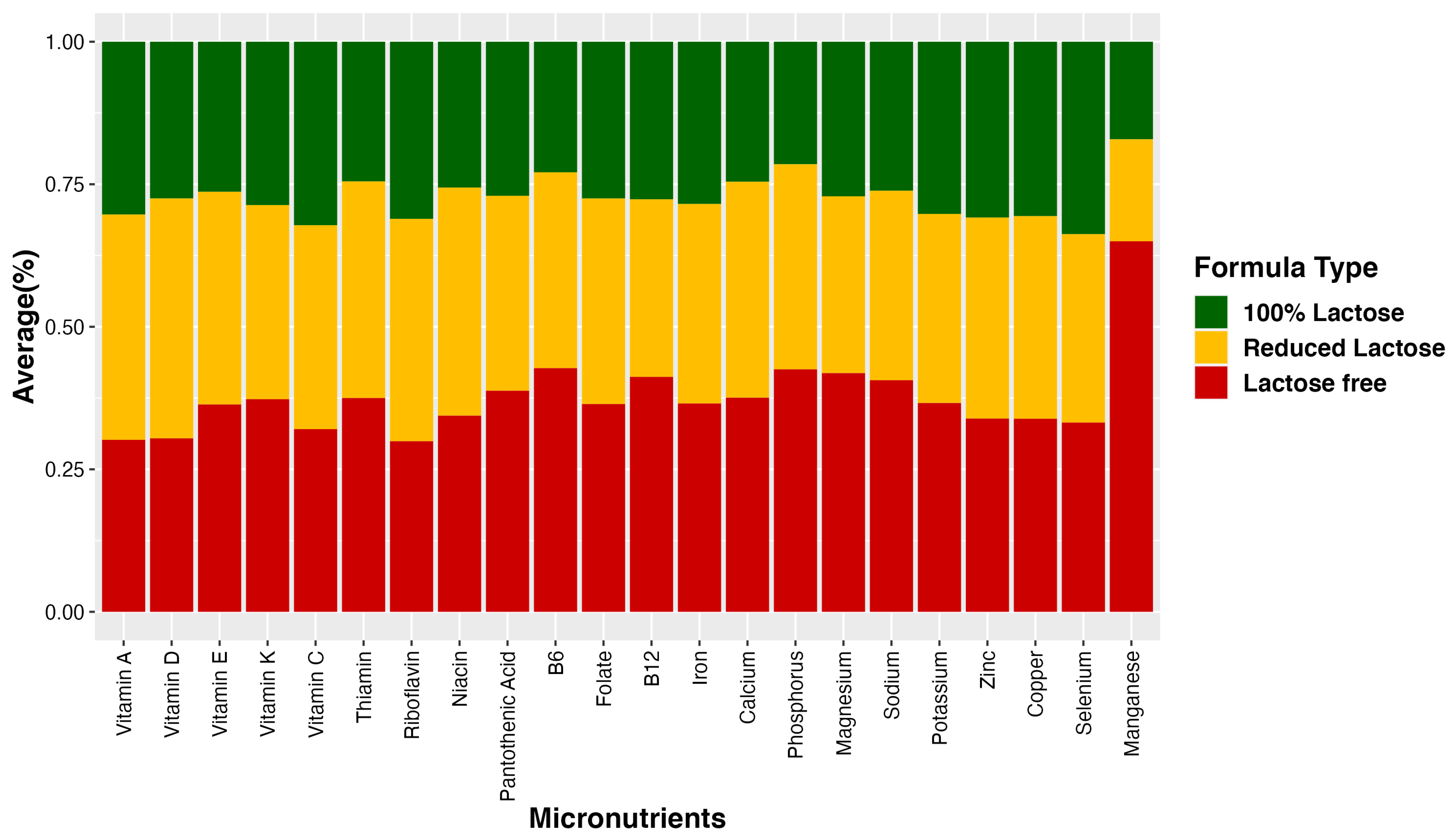
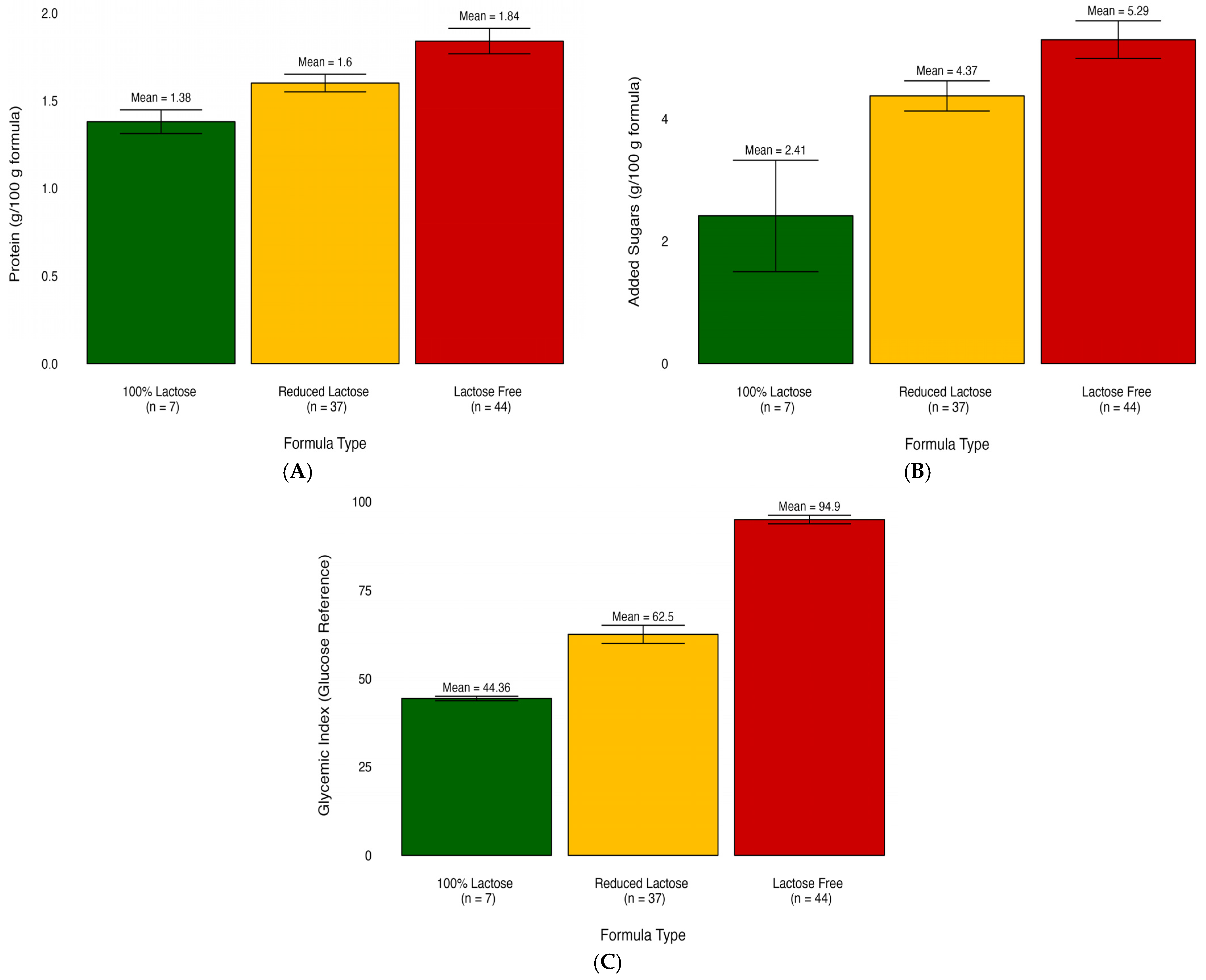
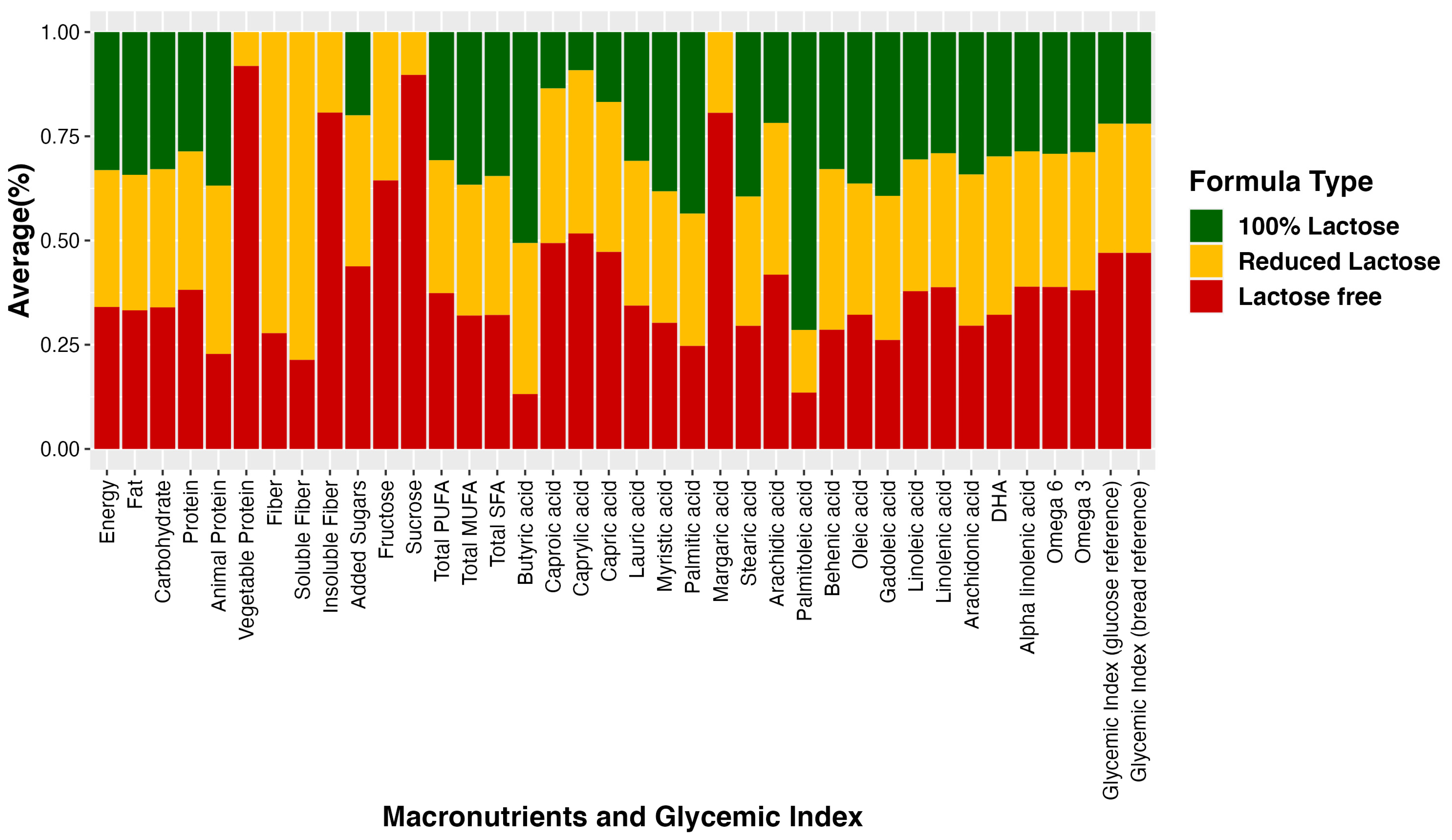
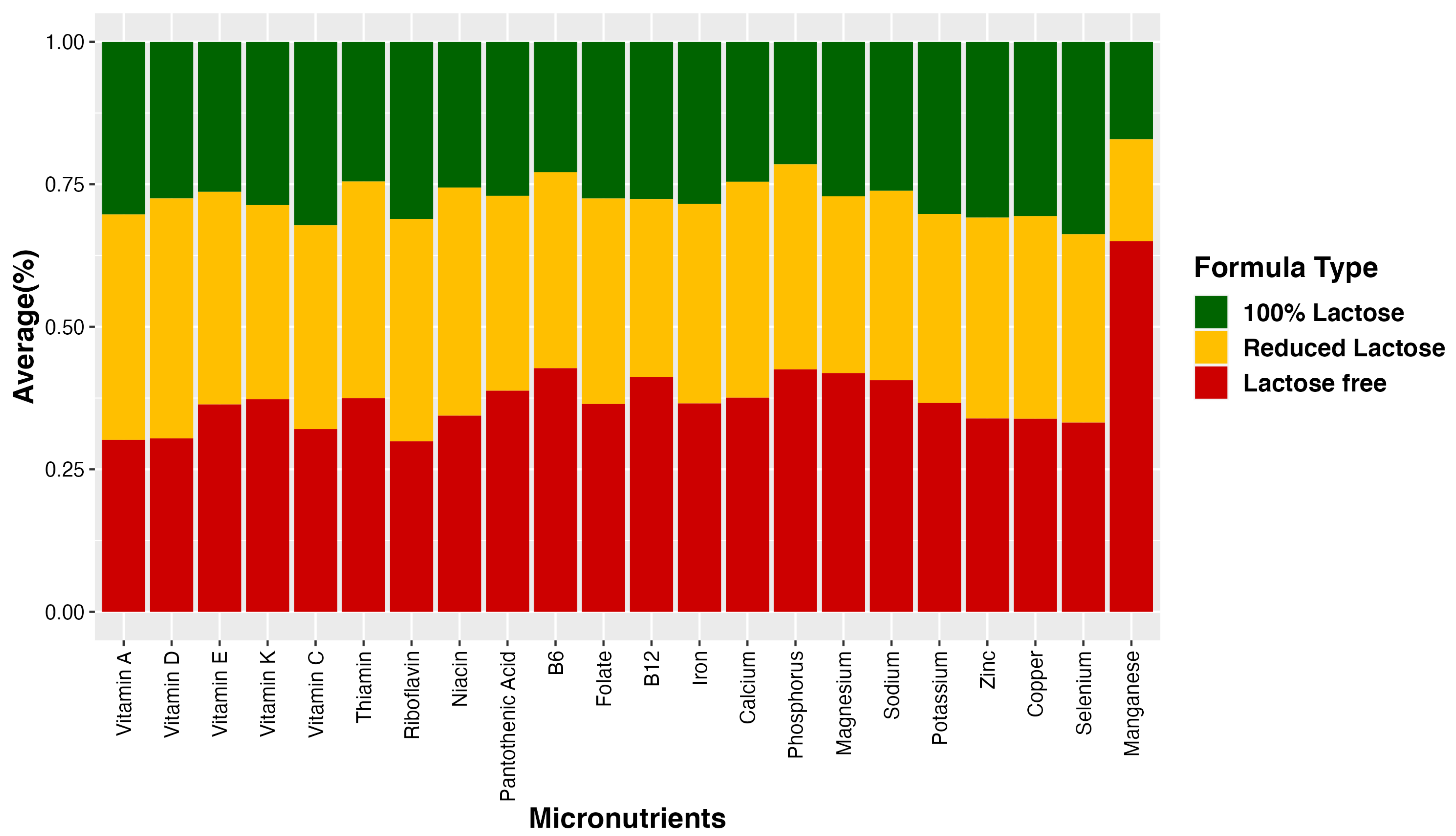
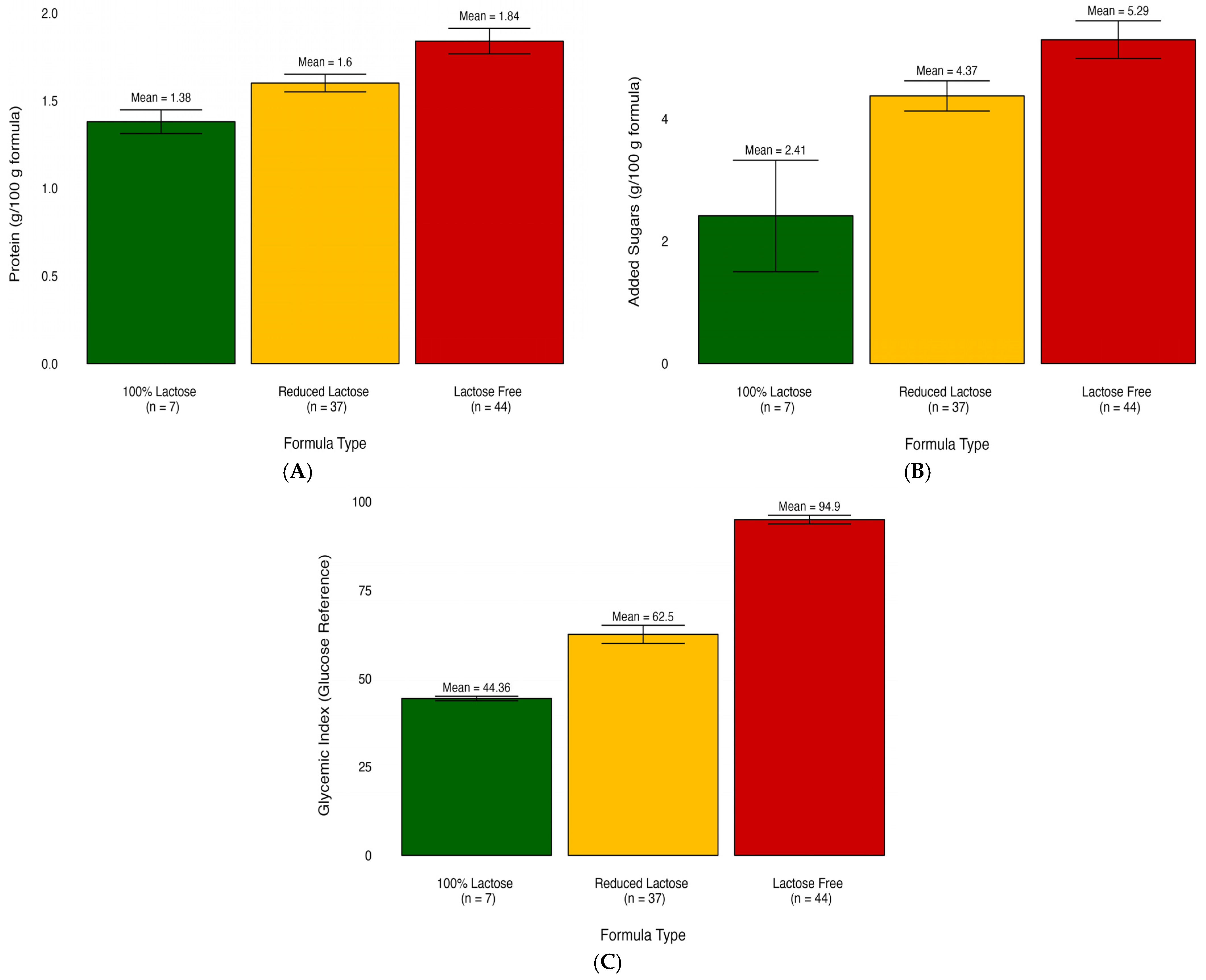
3.1. Mean Difference Analysis among Different Formula Groups
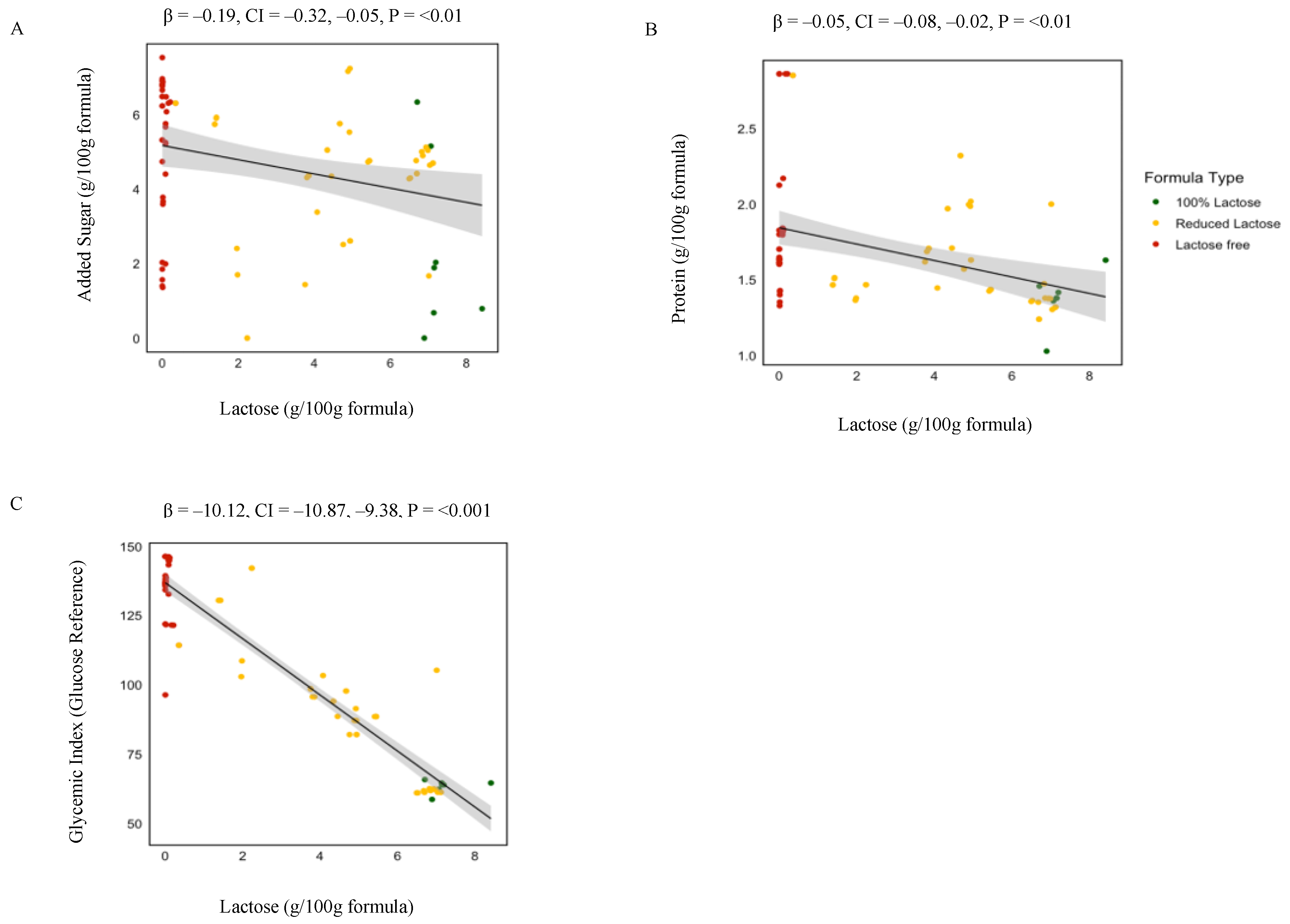
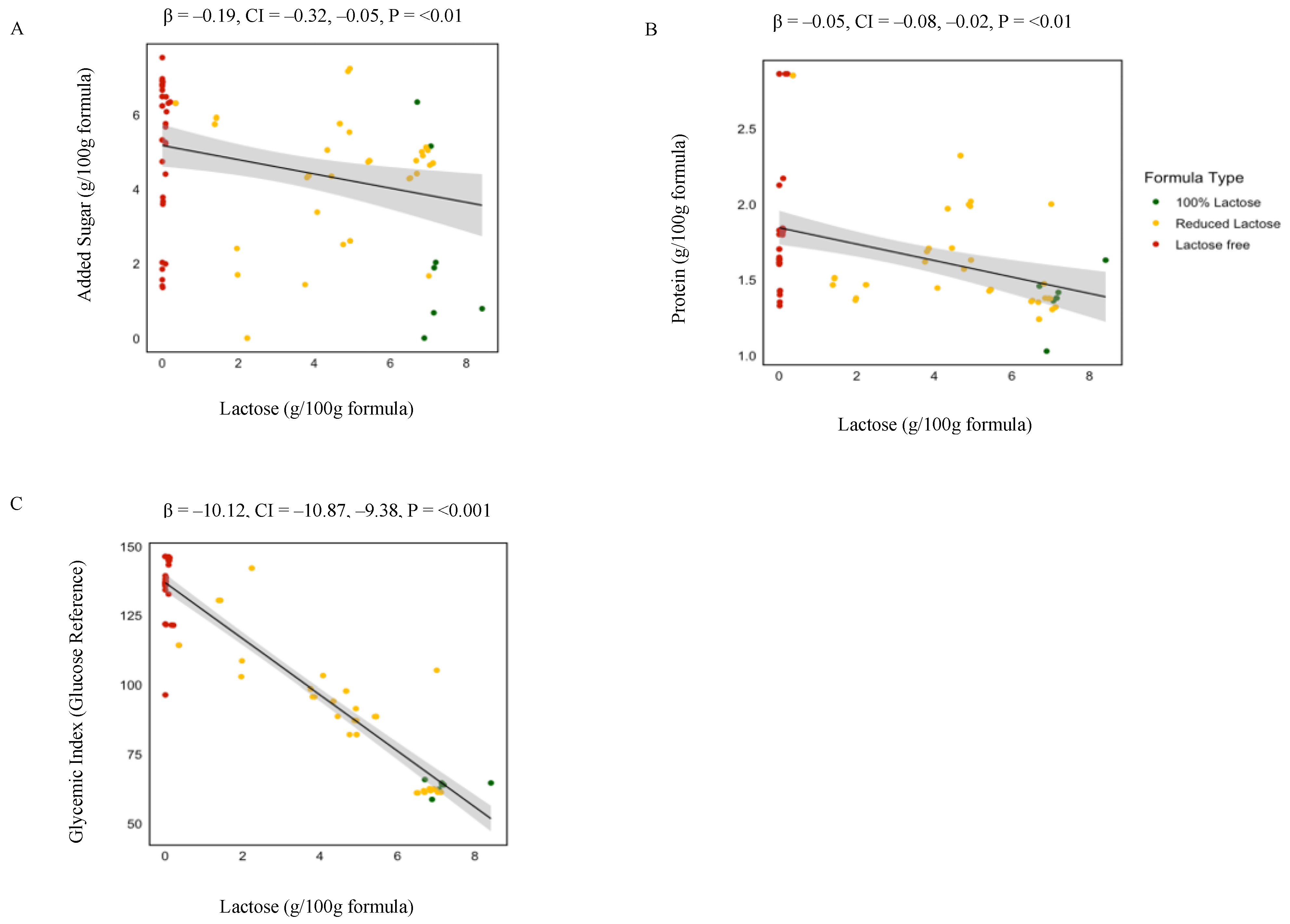
3.2. Linear Regression Analysis: Nutrient–Lactose Concentration Associations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Dellen, S.; Wisse, B.; Mobach, M.P.; Dijkstra, A. The effect of a breastfeeding support programme on breastfeeding duration and exclusivity: A quasi-experiment. BMC Public Health 2019, 19, 993. [Google Scholar] [CrossRef]
- Kuehn, B. Breastfeeding report card. JAMA 2018, 320, 1426. [Google Scholar] [CrossRef] [PubMed]
- Strzalkowski, A.J.; Järvinen, K.M.; Schmidt, B.; Young, B.E. Protein and carbohydrate content of infant formula purchased in the United States. Clin. Exp. Allergy 2022, 52, 1291–1301. [Google Scholar] [CrossRef]
- Crisa, A. Milk Carbohydrates and Oligosaccharides in Milk and Dairy Products in Human Nutrition: Production, Composition and Health; Park, Y.W., Haenlein, G.F.W., Eds.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2013. [Google Scholar]
- Clouard, C.; Le Bourgot, C.; Respondek, F.; Bolhuis, J.E.; Gerrits, W.J. A milk formula containing maltodextrin, vs. lactose, as main carbohydrate source, improves cognitive performance of piglets in a spatial task. Sci. Rep. 2018, 8, 9433. [Google Scholar] [CrossRef] [PubMed]
- Martinez, J.A.; Ballew, M.P. Infant formulas. Pediatr. Rev. 2011, 32, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Papachristoforou, R.; Petrou, P.P.; Sawyer, H.; Williams, M.; Drousiotou, A. Classic galactosaemia in the Greek Cypriot population: An epidemiological and molecular study. Ann. Hum. Genet. 2019, 83, 291–298. [Google Scholar] [CrossRef]
- Batra, A.; Keys, S.C.; Johnson, M.J.; Wheeler, R.A.; Beattie, R.M. Epidemiology, management and outcome of ultrashort bowel syndrome in infancy. Arch. Dis. Child.-Fetal Neonatal Ed. 2017, 102, F551–F556. [Google Scholar] [CrossRef] [PubMed]
- Tzanetakou, I.P.; Mikhailidis, D.P.; Perrea, D.N. Nutrition during pregnancy and the effect of carbohydrates on the offspring’s metabolic profile: In search of the “Perfect Maternal Diet”. Open Cardiovasc. Med. J. 2011, 5, 103. [Google Scholar] [CrossRef] [PubMed]
- Schakel, S.F. Maintaining a nutrient database in a changing marketplace: Keeping pace with changing food products—A research perspective. J. Food Compos. Anal. 2001, 14, 315–322. [Google Scholar] [CrossRef]
- Dietary Guidelines for Americans, 2020–2025, 9th ed.; 2020. Available online: https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf (accessed on 17 August 2023).
- Mozaffarian, D.; Ludwig, D.S. Dietary guidelines in the 21st century—A time for food. JAMA 2010, 304, 681–682. [Google Scholar] [CrossRef] [PubMed]
- Joint, F.; Consultation, W.E. Carbohydrates in Human Nutrition (FAO Food and Nutrition Paper 66); FAO: Rome, Italy, 1998. [Google Scholar]
- Wright, C.; Atkinson, F.; Ramalingam, N.; Buyken, A.; Brand-Miller, J. Effects of human milk and formula on postprandial glycaemia and insulinaemia. Eur. J. Clin. Nutr. 2015, 69, 939–943. [Google Scholar] [CrossRef]
- Brand-Miller, J.; Atkinson, F.; Rowan, A. Effect of added carbohydrates on glycemic and insulin responses to children’s milk products. Nutrients 2013, 5, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; Van Horn, L.V.; Feig, D.I.; Anderson, C.A.; Patel, M.J.; Cruz Munos, J.; Krebs, N.F.; Xanthakos, S.A. Added sugars and cardiovascular disease risk in children: A scientific statement from the American Heart Association. Circulation 2017, 135, e1017–e1034. [Google Scholar] [CrossRef] [PubMed]
- Sanyaolu, A.; Okorie, C.; Qi, X.; Locke, J.; Rehman, S. Childhood and adolescent obesity in the United States: A public health concern. Glob. Pediatr. Health 2019, 6, 2333794X19891305. [Google Scholar] [CrossRef] [PubMed]
- Magriplis, E.; Michas, G.; Petridi, E.; Chrousos, G.P.; Roma, E.; Benetou, V.; Cholopoulos, N.; Micha, R.; Panagiotakos, D.; Zampelas, A. Dietary Sugar Intake and Its Association with Obesity in Children and Adolescents. Children 2021, 8, 676. [Google Scholar] [CrossRef]
- Slupsky, C.M.; He, X.; Hernell, O.; Andersson, Y.; Rudolph, C.; Lönnerdal, B.; West, C.E. Postprandial metabolic response of breast-fed infants and infants fed lactose-free vs regular infant formula: A randomized controlled trial. Sci. Rep. 2017, 7, 3640. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, M.P.; Wang, M.C.; Anderson, C.E.; Crespi, C.M.; Whaley, S.E. The association between the 2009 WIC food package change and early childhood obesity risk varies by type of infant package received. J. Acad. Nutr. Diet. 2020, 120, 371–385. [Google Scholar] [CrossRef]
- Anderson, C.E.; Whaley, S.E.; Goran, M.I. Lactose-reduced infant formula with corn syrup solids and obesity risk among participants in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Am. J. Clin. Nutr. 2022, 116, 1002–1009. [Google Scholar] [CrossRef]
- Mahato, D.K.; Keast, R.; Liem, D.G.; Russell, C.G.; Cicerale, S.; Gamlath, S. Sugar reduction in dairy food: An overview with flavoured milk as an example. Foods 2020, 9, 1400. [Google Scholar] [CrossRef]
- Polk, S.; Thornton, R.J.; Caulfield, L.; Muñoz, A. Rapid infant weight gain and early childhood obesity in low-income Latinos and non-Latinos. Public Health Nutr. 2016, 19, 1777–1784. [Google Scholar] [CrossRef]
- Jones, R.B.; Berger, P.K.; Plows, J.F.; Alderete, T.L.; Millstein, J.; Fogel, J.; Iablokov, S.N.; Rodionov, D.A.; Osterman, A.L.; Bode, L. Lactose-reduced infant formula with added corn syrup solids is associated with a distinct gut microbiota in Hispanic infants. Gut Microbes 2020, 12, 1813534. [Google Scholar] [CrossRef] [PubMed]
- Alderete, T.L.; Jones, R.B.; Shaffer, J.P.; Holzhausen, E.A.; Patterson, W.B.; Kazemian, E.; Chatzi, L.; Knight, R.; Plows, J.F.; Berger, P.K. Early life gut microbiota is associated with rapid infant growth in Hispanics from Southern California. Gut Microbes 2021, 13, 1961203. [Google Scholar] [CrossRef]
- Patel, M.; Srinivasan, M.; Laychock, S. Metabolic programming: Role of nutrition in the immediate postnatal life. J. Inherit. Metab. Dis. Off. J. Soc. Study Inborn Errors Metab. 2009, 32, 218–228. [Google Scholar] [CrossRef]
- Mendonça, M.A.; Araújo, W.M.C.; Borgo, L.A.; Alencar, E.d.R. Lipid profile of different infant formulas for infants. PLoS ONE 2017, 12, e0177812. [Google Scholar] [CrossRef] [PubMed]
- Martinat, M.; Rossitto, M.; Di Miceli, M.; Layé, S. Perinatal Dietary Polyunsaturated Fatty Acids in Brain Development, Role in Neurodevelopmental Disorders. Nutrients 2021, 13, 1185. [Google Scholar] [CrossRef] [PubMed]
- Michaelsen, K.F.; Greer, F.R. Protein needs early in life and long-term health. Am. J. Clin. Nutr. 2014, 99, 718S–722S. [Google Scholar] [CrossRef] [PubMed]
- Liotto, N. Protein Content of Infant Formula for the Healthy Full-Term Infant; Oxford University Press: Oxford, UK, 2020; Volume 111, pp. 946–947. [Google Scholar]
- Patro-Gołąb, B.; Zalewski, B.M.; Kouwenhoven, S.M.; Karaś, J.; Koletzko, B.; Bernard van Goudoever, J.; Szajewska, H. Protein concentration in milk formula, growth, and later risk of obesity: A systematic review. J. Nutr. 2016, 146, 551–564. [Google Scholar] [CrossRef]
- Richter, M.; Baerlocher, K.; Bauer, J.M.; Elmadfa, I.; Heseker, H.; Leschik-Bonnet, E.; Stangl, G.; Volkert, D.; Stehle, P. Revised Reference Values for the Intake of Protein. Ann. Nutr. Metab. 2019, 74, 242–250. [Google Scholar] [CrossRef]
- Arnesen, E.K.; Thorisdottir, B.; Lamberg-Allardt, C.; Bärebring, L.; Nwaru, B.; Dierkes, J.; Ramel, A.; Åkesson, A. Protein intake in children and growth and risk of overweight or obesity: A systematic review and meta-analysis. Food Nutr. Res. 2022, 66, 8242. [Google Scholar] [CrossRef]
- Martin, C.R.; Ling, P.-R.; Blackburn, G.L. Review of Infant Feeding: Key Features of Breast Milk and Infant Formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef]
- Yao, Y.; Cai, X.; Ye, Y.; Wang, F.; Chen, F.; Zheng, C. The Role of Microbiota in Infant Health: From Early Life to Adulthood. Front. Immunol. 2021, 12, 708472. [Google Scholar] [CrossRef]
- Hampson, H.E.; Jones, R.B.; Berger, P.K.; Plows, J.F.; Schmidt, K.A.; Alderete, T.L.; Goran, M.I. Adverse Effects of Infant Formula Made with Corn-Syrup Solids on the Development of Eating Behaviors in Hispanic Children. Nutrients 2022, 14, 1115. [Google Scholar] [CrossRef]
- Satokari, R. High Intake of Sugar and the Balance between Pro- and Anti-Inflammatory Gut Bacteria. Nutrients 2020, 12, 1348. [Google Scholar] [CrossRef] [PubMed]
- Mennella, J.A.; Li, Y.; Bittinger, K.; Friedman, E.S.; Zhao, C.; Li, H.; Wu, G.D.; Trabulsi, J.C. The Macronutrient Composition of Infant Formula Produces Differences in Gut Microbiota Maturation That Associate with Weight Gain Velocity and Weight Status. Nutrients 2022, 14, 1241. [Google Scholar] [CrossRef] [PubMed]
- Davis, E.C.; Dinsmoor, A.M.; Wang, M.; Donovan, S.M. Microbiome Composition in Pediatric Populations from Birth to Adolescence: Impact of Diet and Prebiotic and Probiotic Interventions. Dig. Dis. Sci. 2020, 65, 706–722. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P. Influence of Foods and Nutrition on the Gut Microbiome and Implications for Intestinal Health. Int. J. Mol. Sci. 2022, 23, 9588. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 100% Lactose n = 7 | Reduced Lactose n = 37 | Lactose Free n = 44 | Human Milk * | p-Value | |
|---|---|---|---|---|---|
| Dietary Variables | |||||
| glycemic index (glucose reference) | 44.36 ± 1.65 | 62.5 ± 16.97 | 94.9 ± 7.48 | 41 | <0.001 |
| glycemic index (bread reference) | 63.38 ± 2.34 | 89.28 ± 24.24 | 135.57 ± 10.68 | 58.63 | <0.001 |
| Carbohydrate (g) | |||||
| Sucrose | 0 ± 0 | 0.25 ± 1.03 | 2.14 ± 2.41 | 0 | <0.001 |
| Added Sugars | 2.41 ± 2.41 | 4.37 ± 1.63 | 5.29 ± 1.87 | 0 | <0.01 |
| Soluble Fiber | 0 ± 0 | 0.14 ± 0.21 | 0.04 ± 0.11 | 0 | 0.01 |
| Fiber | 0 ± 0 | 0.14 ± 0.21 | 0.06 ± 0.13 | 0 | 0.02 |
| Protein (g) | |||||
| Total Protein | 1.38 ± 0.18 | 1.6 ± 0.33 | 1.84 ± 0.44 | 1.03 | <0.001 |
| Animal Protein | 1.38 ± 0.18 | 1.51 ± 0.46 | 0.85 ± 0.99 | 1.03 | <0.01 |
| Vegetable Protein | 0 ± 0 | 0.09 ± 0.28 | 0.99 ± 0.93 | 0 | <0.001 |
| Fats (g) | |||||
| Total PUFA | 0.65 ± 0.08 | 0.68 ± 0.08 | 0.8 ± 0.22 | 0.49 | <0.01 |
| PUFA Linoleic Acid (LA) | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.7 ± 0.2 | 0.29 | <0.01 |
| Omega-6 | 0.5 ± 0.1 | 0.55 ± 0.1 | 0.67 ± 0.22 | 0.32 | <0.01 |
| Omega-3 | 0.06 ± 0.02 | 0.07 ± 0.01 | 0.08 ± 0.02 | 0.04 | 0.01 |
| Linolenic Acid | 0.05 ± 0.01 | 0.06 ± 0.01 | 0.07 ± 0.02 | 0.05 | <0.01 |
| Alpha Linolenic Acid (ALA) | 0.05 ± 0.01 | 0.06 ± 0.01 | 0.07 ± 0.02 | 0.04 | <0.01 |
| Linoleic Acid | 0.57 ± 0.1 | 0.59 ± 0.08 | 0.7 ± 0.21 | 0.37 | <0.01 |
| Stearic Acid | 0.16 ± 0.06 | 0.13 ± 0.03 | 0.12 ± 0.04 | 0.29 | 0.02 |
| Palmitic Acid | 0.72 ± 0.24 | 0.52 ± 0.27 | 0.41 ± 0.24 | 0.91 | <0.01 |
| Palmitoleic Acid | 0.02 ± 0.05 | 0.01 ± 0.01 | 0 ± 0.01 | 0.12 | <0.01 |
| Micronutrients | |||||
| Vitamin D | 0.88 ± 0.36 | 1.35 ± 0.96 | 0.98 ± 0.12 | 0.07 | 0.03 |
| Vitamin K | 4.67 ± 1.96 | 5.56 ± 0.66 | 6.08 ± 1.39 | 0.3 | <0.01 |
| Riboflavin | 0.09 ± 0.02 | 0.11 ± 0.04 | 0.08 ± 0.05 | 0.03 | 0.02 |
| Vitamin B12 | 0.18 ± 0.06 | 0.2 ± 0.06 | 0.27 ± 0.13 | 0.05 | <0.01 |
| Sodium | 19.17 ± 1.57 | 24.37 ± 7 | 29.78 ± 4.66 | 17 | <0.001 |
| Potassium | 67.69 ± 11.63 | 74.34 ± 11.16 | 82.07 ± 21.79 | 51 | 0.03 |
| Calcium | 48.63 ± 9.56 | 75 ± 32.03 | 74.38 ± 17.22 | 32 | 0.03 |
| Phosphorus | 25.38 ± 6.64 | 42.48 ± 20.14 | 50.23 ± 16.51 | 14 | <0.01 |
| Magnesium | 5.15 ± 1.1 | 5.89 ± 2.16 | 7.94 ± 4.61 | 3 | 0.01 |
| Manganese | 0.01 ± 0.01 | 0.01 ± 0.03 | 0.04 ± 0.08 | 0.02 | 0.03 |
| Iron | 0.95 ± 0.5 | 1.16 ± 0.2 | 1.22 ± 0.07 | 0.03 | <0.01 |
| Variable | β | (95% CI) | p-Value |
|---|---|---|---|
| glycemic index (bread reference) | −10.12 | −10.87, −9.37 | <0.001 |
| glycemic index (glucose reference) | −7.09 | −7.61, −6.55 | <0.001 |
| Carbohydrate | |||
| Added Sugars | −0.19 | −0.32, −0.05 | <0.01 |
| Sucrose | −0.33 | −0.46, −0.20 | <0.001 |
| Fiber | 0.01 | 0.004, 0.02 | <0.01 |
| Soluble Fiber | 0.01 | 0.007, 0.03 | <0.01 |
| Protein | |||
| Protein | −0.05 | −0.08, −0.02 | <0.001 |
| Vegetable Protein | −0.15 | −0.19, −0.10 | <0.001 |
| Animal Protein | 0.09 | 0.04, 0.15 | <0.001 |
| Fat | |||
| Total PUFA | −0.01 | −0.02, −0.005 | <0.01 |
| Linoleic Acid | −0.01 | −0.02, −0.005 | <0.01 |
| Arachidonic Acid | 0.001 | 0.0002, 0.001 | <0.01 |
| Linolenic Acid | 0.001 | −0.003, 0.0006 | <0.01 |
| Alpha linolenic Acid | 0.001 | −0.003, −0.0005 | <0.01 |
| Omega-6 | −0.01 | −0.02, −0.004 | <0.01 |
| Omega-3 | −0.001 | −0.002, −0.0003 | 0.01 |
| Palmitic Acid | 0.01 | 0.0001, 0.03 | 0.04 |
| Vitamins and Minerals | |||
| Pantothenic Acid | −0.01 | −0.02, −0.0003 | 0.04 |
| B12 | −0.01 | −0.01, −0.005 | <0.001 |
| Vitamin K | −0.09 | −0.18, −0.01 | 0.02 |
| Magnesium | −0.41 | −0.65, −0.17 | <0.001 |
| Sodium | −1.24 | −1.65, −0.84 | <0.001 |
| Phosphorus | −2.46 | −3.74, −1.18 | <0.001 |
| Manganese | −0.005 | −0.009, −0.001 | <0.01 |
| Potassium | −1.66 | −2.85, −0.48 | <0.01 |
| Iron | −0.01 | −0.03, −0.0009 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mokhtari, P.; Schmidt, K.A.; Babaei, M.; Goran, M.I. Altered Nutrient Composition of Lactose-Reduced Infant Formula. Nutrients 2024, 16, 276. https://doi.org/10.3390/nu16020276
Mokhtari P, Schmidt KA, Babaei M, Goran MI. Altered Nutrient Composition of Lactose-Reduced Infant Formula. Nutrients. 2024; 16(2):276. https://doi.org/10.3390/nu16020276
Chicago/Turabian StyleMokhtari, Pari, Kelsey A. Schmidt, Mahsa Babaei, and Michael I. Goran. 2024. "Altered Nutrient Composition of Lactose-Reduced Infant Formula" Nutrients 16, no. 2: 276. https://doi.org/10.3390/nu16020276
APA StyleMokhtari, P., Schmidt, K. A., Babaei, M., & Goran, M. I. (2024). Altered Nutrient Composition of Lactose-Reduced Infant Formula. Nutrients, 16(2), 276. https://doi.org/10.3390/nu16020276