

Healthy Snack Project: Improving Healthy Choices through Multidisciplinary Food Education Actions

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Target Definition and Timing of Implementation
- In May 2022, the training offer of ULSS 1 Dolomiti aimed at schools was published and teachers were recruited.
- In September 2022, a training event was held with teachers to ensure class participation by October for the whole 2022–2023 school year, ending in June 2023. After approval by the class council, the teachers enrolled their classes in the project and the competition.
2.2. Project Path
- Signing of the co-responsibility agreement.
- Carrying out the recording of snacks.
- Holding a workshop on the topic of nutrition, aimed at each registered class, by healthcare workers (HCWs) of the Health Promotion Service of the Prevention Department of ULSS 1 Dolomiti.
- Teachers, students, and parents signed the co-responsibility pact, valid for the entire school year. Teachers explained the benefits of a correct diet and constant, regular physical activity; promoted healthy eating habits at school and proposed that children also engage in games and physical activities at home; and supported students in recording their snacks. At the same time, students learned the information provided by teachers, brought a healthy snack to school, and committed to being more active every day (walking to school, taking the stairs, riding a bike, walking, helping their parents with housework) and spending as little time as possible with TV, video games, and computers. Students registered the snacks they consumed at school twice a week. In this context, parents can set a good example by providing their children with healthy snacks to take to school and offering fruits and vegetables at home (for breakfast, lunch, snack, and dinner), and organizing family exercise activities in their free time (walks, bike rides, etc.).
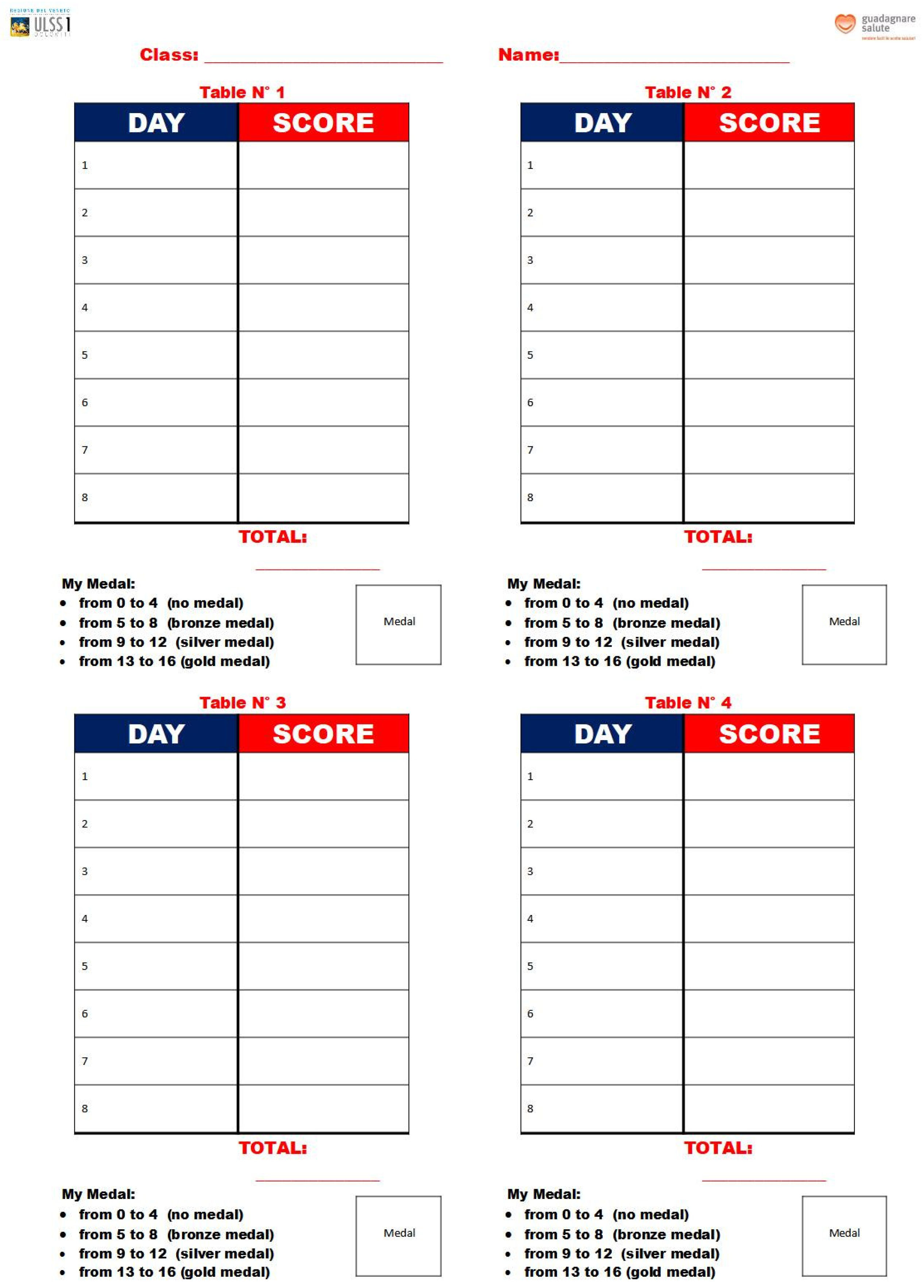
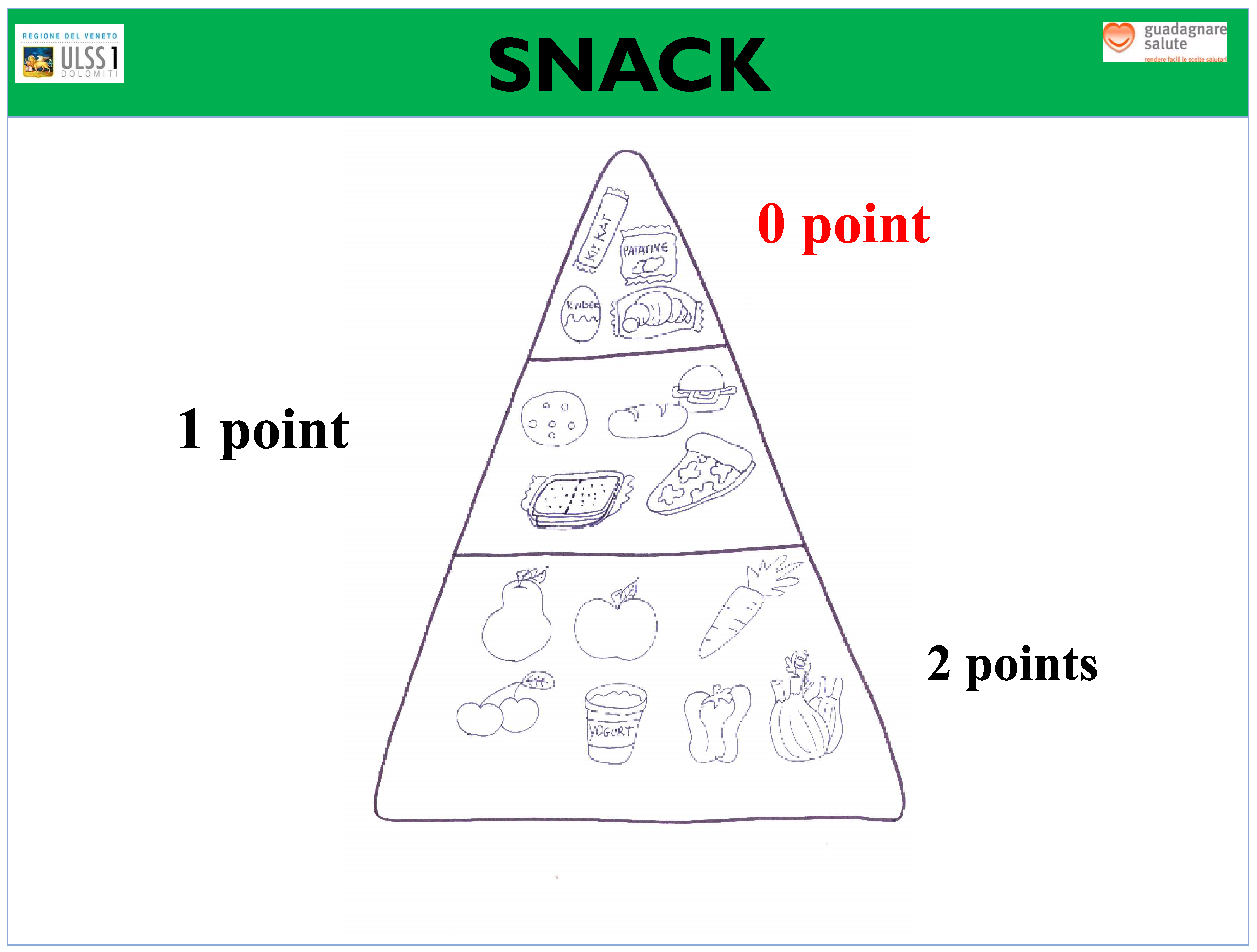
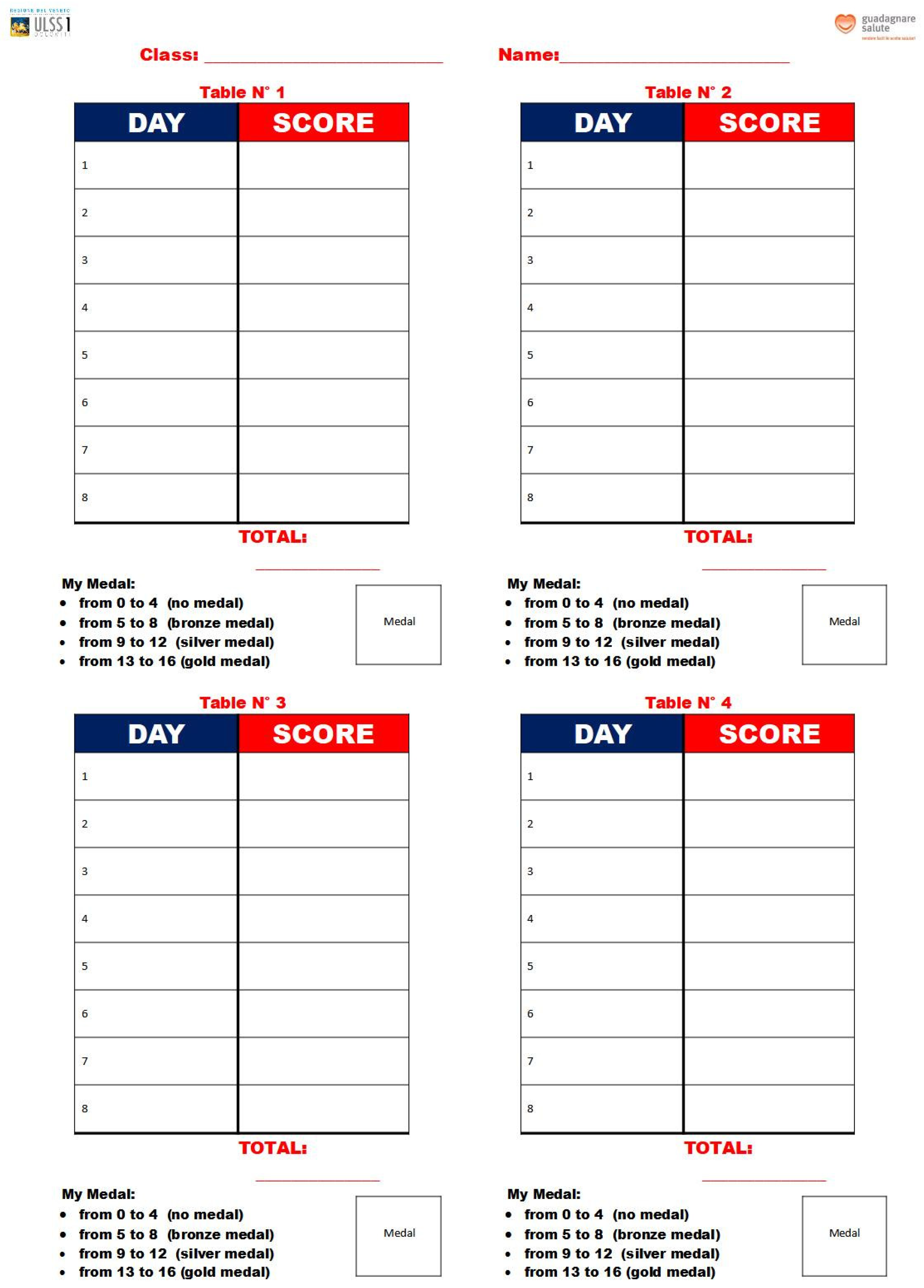
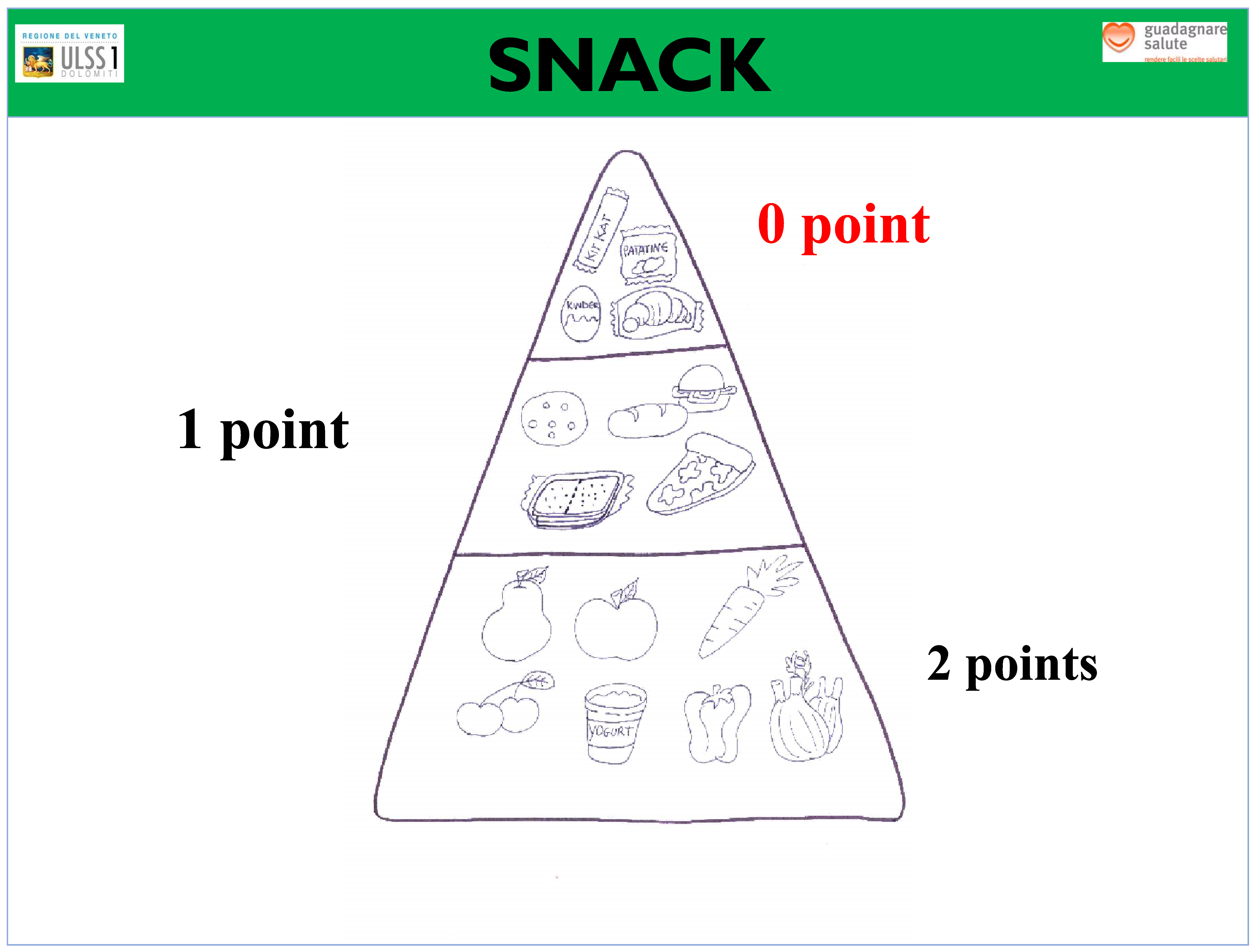
- Using a specific table that was provided for them, students recorded the snacks they consumed at school twice a week, for a total of 32 registrations for each participating student during the school year (Figure 1). On days randomly chosen by the teacher to carry out self-assessment, children filled out their own table by entering their score in relation to the snacks they consumed according to the food pyramid (Figure 2). The daily score was assigned as follows:
- ▪
- No snack: 0 points.
- ▪
- Inadequate snack (excessive portions of carbohydrates, sweet/savory snacks, packaged snacks): 0 points.
- ▪
- Partially adequate snack (small sandwich, crackers, homemade biscuits): 1 point.
- ▪
- Adequate snack (fruit, vegetables, or yogurt): 2 points.
- c.
- A nutrition laboratory was held for each enrolled class during the school year, particularly in the months when the students joined the project. The workshops promoted correct nutrition and encouraged children to choose what and how to eat. The information was provided for children in a playful way, paying particular attention to the daily consumption of fruits and vegetables. The laboratories supported and integrated the activities carried out in class by the teachers.The laboratory activities were carried out by a pair of HCWs with different profiles: dietician, health visitor, social health educator, and environmental health officer. The five workshops, each lasting 2 h, were differentiated based on the ages of students and were structured as follows:
- ▪
- Playground games workshop: intended for pupils attending the first classes of primary school. The HCWs introduced the children to the pleasure of experimenting with new group games and moving, preferably in the open air, through education using music, rhythm, and motor coordination.
- ▪
- Creative–sensory laboratory: intended for pupils in the second year of primary school. Children had the opportunity to learn about fruits and vegetables through stories and sensory journeys.
- ▪
- Laboratory on oral hygiene: intended for pupils in the third year of primary school. This laboratory was aimed at helping children understand the importance of oral hygiene, and described friendly, hostile, and junk foods.
- ▪
- Scientific laboratory: intended for pupils in the fourth grade of primary school. This laboratory was aimed at transmitting basic information to children about macronutrients, their function within the body, and the division and composition of meals during the day.
- ▪
- Motor skills workshop: intended for pupils in the fifth grade of primary school. This workshop was aimed at helping children understand the path of food within the body through motor activities (Figure 5). The main objectives were achieved by observing and reflecting on the methods of digestion of foods.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haines, J.; Haycraft, E.; Lytle, L.; Nicklaus, S.; Kok, F.J.; Merdji, M.; Fisberg, M.; Moreno, L.A.; Goulet, O.; Hughes, S.O. Nurturing Children’s Healthy Eating: Position statement. Appetite 2019, 137, 124–133. [Google Scholar] [CrossRef]
- Almoraie, N.M.; Saqaan, R.; Alharthi, R.; Alamoudi, A.; Badh, L.; Shatwan, I.M. Snacking patterns throughout the life span: Potential implications on health. Nutr. Res. 2021, 91, 81–94. [Google Scholar] [CrossRef]
- Ortega, F.B.; Lavie, C.J.; Blair, S.N. Obesity and Cardiovascular Disease. Circ. Res. 2016, 118, 1752–1770. [Google Scholar] [CrossRef]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef]
- Jaacks, L.M.; Vandevijvere, S.; Pan, A.; McGowan, C.J.; Wallace, C.; Imamura, F.; Mozaffarian, D.; Swinburn, B.; Ezzati, M. The obesity transition: Stages of the global epidemic. Lancet Diabetes Endocrinol. 2019, 7, 231–240. [Google Scholar] [CrossRef]
- Withrow, D.; Alter, D.A. The economic burden of obesity worldwide: A systematic review of the direct costs of obesity. Obes. Rev. 2011, 12, 131–141. [Google Scholar] [CrossRef]
- Thomas-Eapen, N. Childhood Obesity. Prim. Care 2021, 48, 505–515. [Google Scholar] [CrossRef]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef]
- Lambrinou, C.P.; Androutsos, O.; Karaglani, E.; Cardon, G.; Huys, N.; Wikström, K.; Kivelä, J.; Ko, W.; Karuranga, E.; Tsochev, K.; et al. Effective strategies for childhood obesity prevention via school based, family involved interventions: A critical review for the development of the Feel4Diabetes-study school based component. BMC Endocr. Disord. 2020, 20 (Suppl. 2), 52. [Google Scholar] [CrossRef]
- Monzani, A.; Ricotti, R.; Caputo, M.; Solito, A.; Archero, F.; Bellone, S.; Prodam, F. A Systematic Review of the Association of Skipping Breakfast with Weight and Cardiometabolic Risk Factors in Children and Adolescents. What Should We Better Investigate in the Future? Nutrients 2019, 11, 387. [Google Scholar] [CrossRef]
- Verduci, E.; Bronsky, J.; Embleton, N.; Gerasimidis, K.; Indrio, F.; Köglmeier, J.; de Koning, B.; Lapillonne, A.; Moltu, S.J.; Norsa, L.; et al. Role of Dietary Factors, Food Habits, and Lifestyle in Childhood Obesity Development: A Position Paper from the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2021, 72, 769–783. [Google Scholar] [CrossRef]
- Roblin, L. Childhood obesity: Food, nutrient, and eating-habit trends and influences. Appl. Physiol. Nutr. Metab. 2007, 32, 635–645. [Google Scholar] [CrossRef]
- Centro di Ricerca Alimenti e Nutrizione—CREA. Linee Guida per una Sana Alimentazione. Revisione 2018. Available online: https://www.crea.gov.it/documents/59764/0/LINEE-GUIDA+DEFINITIVO.pdf/ (accessed on 22 November 2023).
- SIPPS. Manuale di Nutrizione in Età Evolutiva; Cuzzolin: Naples, Italy, 2016. [Google Scholar]
- Istituto Superiore di Sanità. Obesità e Stili di Vita dei Bambini: OKkio alla Salute 2019; Rapporti ISTISAN 22/27; Nardone, P., Spinelli, A., Ciardullo, S., Salvatore, M.A., Andreozzi, S., Galeone, D., Eds.; Istituto Superiore di Sanità: Rome, Italy, 2022; Volume 6, 82p. [Google Scholar]
- Chamorro-Garcia, R.; Veiga-Lopez, A. The new kids on the block: Emerging obesogens. Adv. Pharmacol. 2021, 92, 457–484. [Google Scholar] [CrossRef]
- Trude, A.C.B.; Surkan, P.J.; Cheskin, L.J.; Gittelsohn, J. A multilevel, multicomponent childhood obesity prevention group-randomized controlled trial improves healthier food purchasing and reduces sweet-snack consumption among low-income African-American youth. Nutr. J. 2018, 17, 96. [Google Scholar] [CrossRef]
- Sacchetti, R.; Dallolio, L.; Musti, M.A.; Guberti, E.; Garulli, A.; Beltrami, P.; Castellazzi, F.; Centis, E.; Zenesini, C.; Coppini, C.; et al. Effects of a school based intervention to promote healthy habits in children 8–11 years old, living in the lowland area of Bologna Local Health Unit. Ann. Ig. 2015, 27, 432–446. [Google Scholar] [CrossRef]
- Verrotti, A.; Penta, L.; Zenzeri, L.; Agostinelli, S.; De Feo, P. Childhood obesity: Prevention and strategies of intervention. A systematic review of school-based interventions in primary schools. J. Endocrinol. Investig. 2014, 37, 1155–1164. [Google Scholar] [CrossRef]
- Dudley, D.A.; Cotton, W.G.; Peralta, L.R. Teaching approaches and strategies that promote healthy eating in primary school children: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 28. [Google Scholar] [CrossRef]
- Marcotrigiano, V.; Stingi, G.D.; Nugnes, P.T.; Mancano, S.; Lagreca, V.M.; Tarricone, T.; Salerno, G.; Pasquale, P.; Marchet, P.; Sava, G.A.; et al. Collective Catering Activities and Official Controls: Dietary Promotion, Sustainability and Future Perspectives. Healthcare 2023, 11, 1347. [Google Scholar] [CrossRef]
- Sanmarchi, F.; Masini, A.; Poli, C.; Kawalec, A.; Esposito, F.; Scrimaglia, S.; Scheier, L.M.; Dallolio, L.; Sacchetti, R. Cross-Sectional Analysis of Family Factors Associated with Lifestyle Habits in a Sample of Italian Primary School Children: The I-MOVE Project. Int. J. Environ. Res. Public Health 2023, 20, 4240. [Google Scholar] [CrossRef]
- Marcotrigiano, V.; Stingi, G.D.; Fregnan, S.; Magarelli, P.; Pasquale, P.; Russo, S.; Orsi, G.B.; Montagna, M.T.; Napoli, C.; Napoli, C. An Integrated Control Plan in Primary Schools: Results of a Field Investigation on Nutritional and Hygienic Features in the Apulia Region (Southern Italy). Nutrients 2021, 13, 3006. [Google Scholar] [CrossRef]
- Boyland, E.J.; Nolan, S.; Kelly, B.; Tudur-Smith, C.; Jones, A.; Halford, J.C.; Robinson, E. Advertising as a cue to consume: A systematic review and meta-analysis of the effects of acute exposure to unhealthy food and nonalcoholic beverage advertising on intake in children and adults. Am. J. Clin. Nutr. 2016, 103, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary School Classes | Number of Classes Enrolled | Number of Students Enrolled | Number of Total Classes | Number of Total Students |
|---|---|---|---|---|
| First class | 11 | 160 | 81 | 1250 |
| Second class | 13 | 195 | 80 | 1283 |
| Third class | 12 | 187 | 91 | 1333 |
| Fourth class | 12 | 213 | 85 | 1368 |
| Fifth class | 11 | 170 | 91 | 1457 |
| Total | 59 | 925 | 428 | 6691 |
| Medals at T0 (%) | Medals at T1 (%) | p-Value | |
|---|---|---|---|
| Assigned Medals | 2209 (59.7) | 3172 (85.7) | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Federici, G.; Marcotrigiano, V.; Bino, E.; Lovat, A.; Padoin, A.; Salerno, G.; D’Incà, P.; Napoli, C.; Cinquetti, S. Healthy Snack Project: Improving Healthy Choices through Multidisciplinary Food Education Actions. Nutrients 2024, 16, 255. https://doi.org/10.3390/nu16020255
Federici G, Marcotrigiano V, Bino E, Lovat A, Padoin A, Salerno G, D’Incà P, Napoli C, Cinquetti S. Healthy Snack Project: Improving Healthy Choices through Multidisciplinary Food Education Actions. Nutrients. 2024; 16(2):255. https://doi.org/10.3390/nu16020255
Chicago/Turabian StyleFederici, Giuseppina, Vincenzo Marcotrigiano, Erica Bino, Alberto Lovat, Angela Padoin, Gerardo Salerno, Pamela D’Incà, Christian Napoli, and Sandro Cinquetti. 2024. "Healthy Snack Project: Improving Healthy Choices through Multidisciplinary Food Education Actions" Nutrients 16, no. 2: 255. https://doi.org/10.3390/nu16020255
APA StyleFederici, G., Marcotrigiano, V., Bino, E., Lovat, A., Padoin, A., Salerno, G., D’Incà, P., Napoli, C., & Cinquetti, S. (2024). Healthy Snack Project: Improving Healthy Choices through Multidisciplinary Food Education Actions. Nutrients, 16(2), 255. https://doi.org/10.3390/nu16020255