
Translation, Cultural Adaptation, and Content Validity of the Saudi Sign Language Version of the General Nutrition Knowledge Questionnaire
 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. The GNKQ Tool
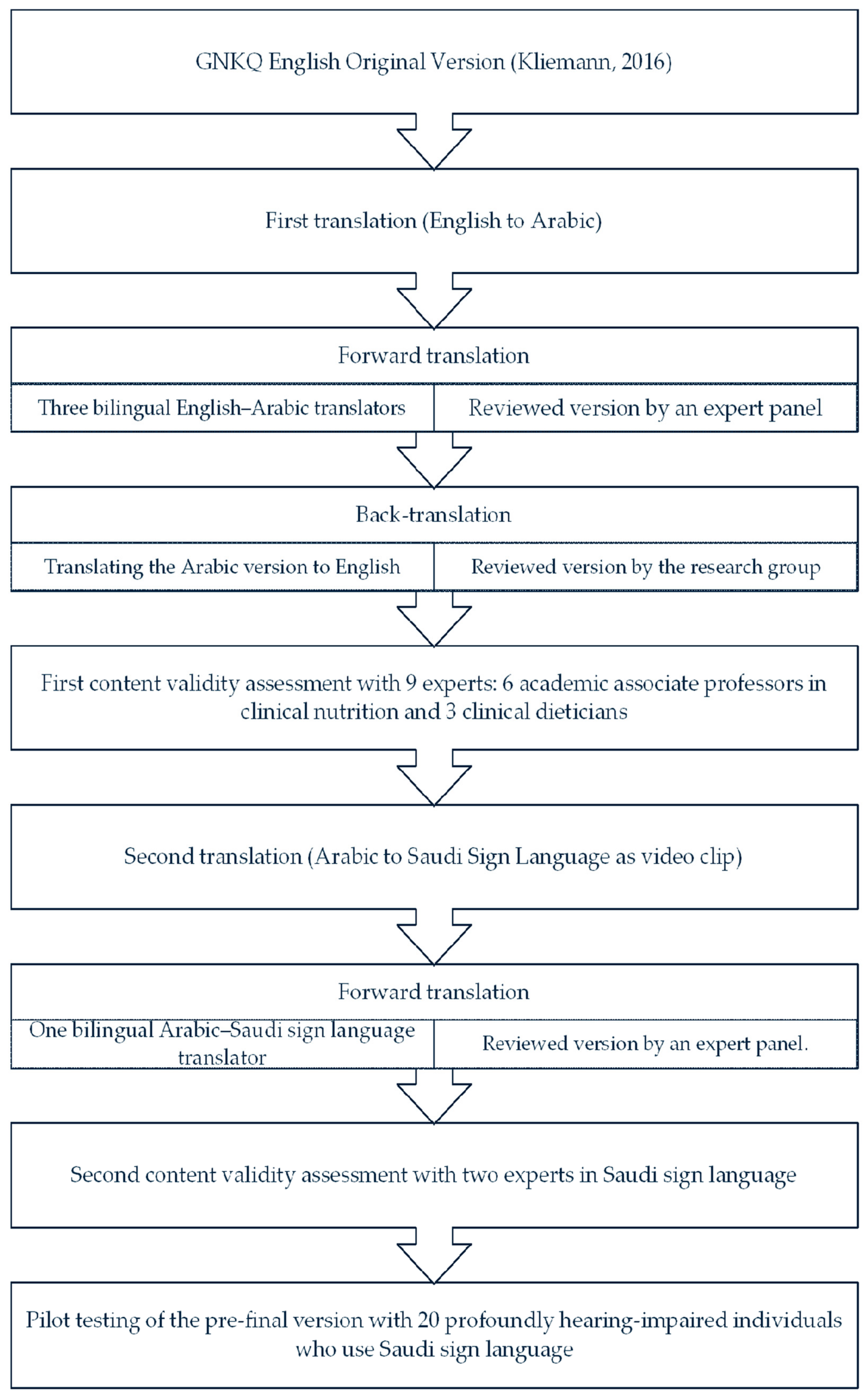
2.2. Translation Process
2.2.1. Translation from English into Arabic
2.2.2. Translation from Arabic into Saudi Sign Language
2.3. Pilot Testing of the Pre-Final Version
2.4. Cultural Adaptation
2.5. Statistical Analysis
3. Results
3.1. Translation from English into Arabic (Forward-Translation)
3.2. Back-Translation from English to Arabic
3.3. Translation from Arabic into Saudi Sign Language (Forward-Translation)
3.4. Pilot Testing of the Pre-Final Version among Profoundly Hearing-Impaired Volunteers
3.5. Descriptive Analysis
3.6. Content Validity
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Deafness and Hearing Loss (Fact Sheet). 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss (accessed on 26 March 2023).
- General Authority for Statistics. Disability Survey. 2017. Available online: https://www.stats.gov.sa/en/904 (accessed on 26 March 2023).
- Al-Obodi, A.H.; Al-Hanine, A.M.; Al-Harbi, K.N.; Al-Dawas, M.S.; Al-Shargabi, A.A. A Saudi Sign Language recognition system based on convolutional neural networks. Build. Serv. Eng. Res. Technol. 2020, 13, 3328–3334. [Google Scholar] [CrossRef]
- Puga, A.M.; Pajares, M.A.; Varela-Moreiras, G.; Partearroyo, T. Interplay between nutrition and hearing loss: State of art. Nutrients 2018, 11, 35. [Google Scholar] [CrossRef] [PubMed]
- Parmenter, K.; Wardle, J. Development of a general nutrition knowledge questionnaire for adults. Eur. J. Clin. Nutr. 1999, 53, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Croll, P.H.; Voortman, T.; Vernooij, M.W.; de Jong, R.J.B.; Lin, F.R.; Rivadeneira, F.; Ikram, M.A.; Goedegebure, A. The association between obesity, diet quality and hearing loss in older adults. Aging 2019, 11, 48–62. [Google Scholar] [CrossRef] [PubMed]
- Emond, A.; Ridd, M.; Sutherland, H.; Allsop, L.; Alexander, A.; Kyle, J. The current health of the signing Deaf community in the UK compared with the general population: A cross-sectional study. BMJ Open 2015, 1, e006668. [Google Scholar] [CrossRef] [PubMed]
- Amin, S.; Al-Shammari, M. A Survey of Vitamin Intake amongst Hearing and Hearing-Impaired Female Students in Saudi Arabia: A Pilot Study. Int. J. Womens Health Wellness 2020, 6, 116. [Google Scholar]
- Kliemann, N.; Wardle, J.; Johnson, F.; Croker, H. Reliability and validity of a revised version of the General Nutrition Knowledge Questionnaire. Eur. J. Clin. Nutr. 2016, 70, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Crogan, N.L.; Jones, E.G.; Kang, Y. Nutritional Health Among Deaf Adults. JADARA 2019, 40, 6. [Google Scholar]
- World Health Organization. Retrieved from WHO Guidelines on Translation and Adpation of Instrument. 2015. Available online: https://www.emro.who.int/emhj-volume-25-2019/volume-25-issue-3/the-translation-and-cultural-adaptation-validity-of-the-actual-scope-of-practice-questionnaire.html (accessed on 31 March 2024).
- American Speech-Language-Hearing Association. Retrieved from Degree of Hearing Loss. Available online: https://www.asha.org/public/hearing/degree-of-hearing-loss/ (accessed on 24 March 2023).
- Alsehemi, N.H.; Alharbi, A.A.; Alamri, R.S.; Fatani, B.A.; Alsenan, S.H.; Elbarazi, I.; Aldhwayan, M.M. Translation and Validation of the Arabic Version of the Eating Behavior After Bariatric Surgery (EBBS) Questionnaire. Obes. Surg. 2023, 33, 1108–1120. [Google Scholar] [CrossRef] [PubMed]
- Kalfoss, M. Translation and adaption of questionnaires: A nursing challenge. SAGE Open Nurs. 2019, 5, 2377960818816810. [Google Scholar] [CrossRef] [PubMed]
- Yusoff, M.S. ABC of content validation and content validity index calculation. Educ. Med. J. 2019, 11, 49–54. [Google Scholar] [CrossRef]
- World Health Organization. Healthy Diet. 19 April 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 26 March 2023).
- Centers for Disease Control and Prevention. Retrieved from Healthy Weight, Nutrition, and Physical Activity. Available online: https://www.cdc.gov/healthyweight/index.html (accessed on 9 June 2023).
- Veinberg, S. United Nations Children’s Fund., Producing Sign Language Videos, Recommendations for Producing Sign Language Videos. 5 July 2019. Available online: https://www.accessibletextbooksforall.org/stories/producing-sign-language-videos (accessed on 31 March 2024).
- Putnoky, S.B.; Banu, A.M.; Moleriu, L.C.; Putnoky, S.; Șerban, D.M.; Niculescu, M.D.; Șerban, C.L. Reliability and validity of a general nutrition knowledge questionnaire for adults in a Romanian population. Eur. J. Clin. Nutr. 2020, 74, 1576–1584. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, S.E. Linguistic and cultural adaptation of the Inventory of Personality Organization (IPO) for the Brazilian culture. J. Depress. Anxiety 2011, 1, 1–7. [Google Scholar] [CrossRef]
- Fageeh, H.N.; Mansoor, M.A. The effectiveness of oral hygiene instructions in sign language among hearing impaired adults in Saudi Arabia. Spec. Care Dent. 2020, 40, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Ozair, M.M.; Baharuddin, K.A.; Mohamed, S.A.; Esa, W.; Yusoff, M.S.B. Development and Validation of the Knowledge and Clinical Reasoning of Acute Asthma Management in Emergency Department (K-CRAMED). Educ. Med. J. 2017, 9, 1–17. [Google Scholar] [CrossRef]
- Marzuki, M.F. Translation, cross-cultural adaptation, and validation of the Malay version of the system usability scale questionnaire for the assessment of mobile apps. JMIR Hum. Factors 2018, 5, e10308. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Gender | Male | 6 (30) |
|---|---|---|
| Female | 14 (70) | |
| Age | 19–29 | 4 (20) |
| 30–39 | 11(55) | |
| 40–49 | 4 (15) | |
| 50–59 | 1 (5) | |
| 60 | 1 (5) | |
| Education level | Elementary | - |
| Intermediate | 1 (5) | |
| High school | 4 (20) | |
| Diploma | 7 (35) | |
| Bachelor’s | 8 (40) | |
| Occupation | Students | 2 (10) |
| Employed | 15 (70) | |
| Unemployed | 1 (5) | |
| Retired | 2 (10) |
| No. Items | CVI |
|---|---|
| section 1 | |
| 1. Do you believe that experts recommend people to have more quantity, the same quantity, or less quantity of the following foods? | 1 |
| 2. What are the main daily portions of fruits and vegetables recommended by experts? (One portion can contain, for example, an apple or hand grip of cut carrots)? | 0.9 |
| 3. Which of those types of fats are recommended by experts to be eaten less? | 1 |
| 4. Which type of dietary products is recommended by experts? | 1 |
| 5. How many times per week are recommended by experts to have fatty fish (such as salmon)? | 1 |
| 6. Approximately, how many alcoholic drinks is the maximum recommended per day (The exact number depends on the size and strength of the drink)? | 0.55 |
| 7. How many times per week do experts recommend having breakfast? | 1 |
| 8. If two fruit juice cups per day are consumed, how many daily rations of fruits and vegetables shall be calculated? | 0.9 |
| 9. According to the “good eating” guide, how must the individual’s system of starches be? * (Guide that indicates the rates of food groups that an individual must have to get a balanced and healthy dietary system)? | 0.9 |
| section 2 | |
| 1. Do you believe that those foods and beverages usually contain added sugar in high or low rates? | 0.9 |
| 2. Do you believe that those foods are usually high or low in salts? | 1 |
| 3. Do you believe that those foods are usually high or low in fibers? | 1 |
| 4. Do you believe that those foods represent a good source of protein? | 1 |
| 5. Which of those foods do you believe that experts classified within the starchy group? | 0.9 |
| 6. What is the main type of fats in each of those foods? | 1 |
| 7. Which of those foods contain higher quantity of trans-fats? | 0.9 |
| 8. Amount of calcium in cup of full cream milk as compared to cup of skimmed milk is:… | 1 |
| 9. Which of the following food items contain more calories for the same quantity of the following foods… | 1 |
| 10. Compared to unprocessed foods, processed foods contain:… | 0.9 |
| section 3 | |
| 1. If yoghurt is purchased from supermarket, which types contains a lower quantity of sugar? | 1 |
| 2. If a person wants to drink soup from a restaurant, which of the following options contains the lowest amount of fats? | 1 |
| 3. What is the healthy and balanced food option of the main course chosen from a restaurant? | 1 |
| 4. Which of the following sandwiches is the healthy option as a meal? | 1 |
| 5. What is the healthiest option of a dessert dish? | 1 |
| 6. Which of the following groups of vegetables in salad provide the highest diversity of vitamins and antioxidants? | 1 |
| 7. If a person wants to reduce the quantity of fats in his diet, but doesn’t want to leave the fried chips, which of the following foods will be the best choice? | 0.9 |
| 8. One of the healthy methods of adding flavor to food without addition of more fats or salt is addition of:… | 1 |
| 9. Which of the following methods of cooking require the addition of fats? | 1 |
| 10. Traffic signs are often used on food labels; what does the yellow of fact content mean in food? | 1 |
| 11. Light foods or diet foods are often considered good options because they are low in calories. | 1 |
| 12. Looking at the first and second products, which of them contains the highest number of calories (kilocalories) per 100 g? | 1 |
| 13. Looking at the first product, what are the sources of sugar on the list of ingredients? | 1 |
| section 4 | |
| 1. Which of the following diseases is related to low eating of fiber? | 0.9 |
| 2. Which of the following diseases is related to the quantity of sugar eaten by the individual? | 1 |
| 3. Which of the following diseases is related to the quantity of salt (or sodium) eaten by the individual? | 1 |
| 4. Which of the following advice is given by experts for the reduction of the chances of cancer? | 1 |
| 5. Which of the following advice is given by experts for the prevention of heart diseases? | 1 |
| 6. Which of the following advice is given by experts for prevention of diabetes? | 1 |
| 7. Which of the following foods are likely to increase the percentage of blood cholesterol? | 1 |
| 8. Which of the flood foods is classified as containing a high glycemic index? * (Glycemic index is the measurement of food’s effect on the level of blood sugar, so an increase in glycemic index means a higher increase in blood sugar after food). | 1 |
| 9. To keep a healthy weight, you must completely prevent fats. | 1 |
| 10. To keep a healthy weight, have a high-protein diet. | 1 |
| 11. Eating bread/rice food always causes overweight. | 1 |
| 12. Eating food that contains fiber reduces likely overweight. | 1 |
| 13. Which of the following options can help people keep a healthy weight? | 1 |
| 14. If the Body Mass Index (BMI) of the individual is 23 kg/m2, what is his weight status? | 0.9 |
| 15. If the Body Mass Index (BMI) of the individual is 31 kg/m2, what is his weight status? | 1 |
| 16. Which of the following body shapes is related to increased cardiovascular diseases *? | 0.9 |
| Expert 1 | Expert 2 | Expert 3 | Expert 4 | Expert 5 | Expert 6 | Expert 7 | Expert 8 | Expert 9 | Expert10 | Expert 11 | Expert Agreement | * I-CVI | **** UA | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Items | |||||||||||||||
| Q1-1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q1-2 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| Q1-3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q1-4 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q1-5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q1-6 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 6 | 0.55 | 0 | |
| Q1-7 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q1-8 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| Q1-9 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| Q2-1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 10 | 0.9 | 0 | |
| Q2-2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q2-3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q2-4 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q2-5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| Q2-6 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q2-7 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| Q2-8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q2-9 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q2-10 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| Q3-1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-4 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-6 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-7 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| Q3-8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-9 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-10 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-11 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-12 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q3-13 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| Q4-2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-4 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-6 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-7 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-9 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-10 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-11 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-12 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-13 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-14 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| Q4-15 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | 1 | 1 | |
| Q4-16 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 10 | 0.9 | 0 | |
| ** S-CVIlAve | 0.96 | ||||||||||||||
| Proportion relevance | 0.95 | 1 | 0.97 | 0.97 | 0.97 | 0.97 | 0.89 | 0.97 | 0.95 | 1 | 1 | *** S-CVIlUA | 0.76 | ||
| Average proportion of items judged as relevant among the eleven experts | 0.96 | ||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljubair, J.M.; Aldisi, D.; Bindayel, I.A.; Aldhwayan, M.M.; Sabico, S.; Alsaawi, T.A.; Alghamdi, E.; Abulmeaty, M.M.A. Translation, Cultural Adaptation, and Content Validity of the Saudi Sign Language Version of the General Nutrition Knowledge Questionnaire. Nutrients 2024, 16, 2664. https://doi.org/10.3390/nu16162664
Aljubair JM, Aldisi D, Bindayel IA, Aldhwayan MM, Sabico S, Alsaawi TA, Alghamdi E, Abulmeaty MMA. Translation, Cultural Adaptation, and Content Validity of the Saudi Sign Language Version of the General Nutrition Knowledge Questionnaire. Nutrients. 2024; 16(16):2664. https://doi.org/10.3390/nu16162664
Chicago/Turabian StyleAljubair, Jenan M., Dara Aldisi, Iman A. Bindayel, Madhawi M. Aldhwayan, Shaun Sabico, Tafany A. Alsaawi, Esraa Alghamdi, and Mahmoud M. A. Abulmeaty. 2024. "Translation, Cultural Adaptation, and Content Validity of the Saudi Sign Language Version of the General Nutrition Knowledge Questionnaire" Nutrients 16, no. 16: 2664. https://doi.org/10.3390/nu16162664
APA StyleAljubair, J. M., Aldisi, D., Bindayel, I. A., Aldhwayan, M. M., Sabico, S., Alsaawi, T. A., Alghamdi, E., & Abulmeaty, M. M. A. (2024). Translation, Cultural Adaptation, and Content Validity of the Saudi Sign Language Version of the General Nutrition Knowledge Questionnaire. Nutrients, 16(16), 2664. https://doi.org/10.3390/nu16162664