
Twenty-Four Hour Glucose Profiles and Glycemic Variability during Intermittent Religious Dry Fasting and Time-Restricted Eating in Subjects without Diabetes: A Preliminary Study

 ,
,  ,
, .png)
Abstract
1. Introduction
2. Materials and Methods
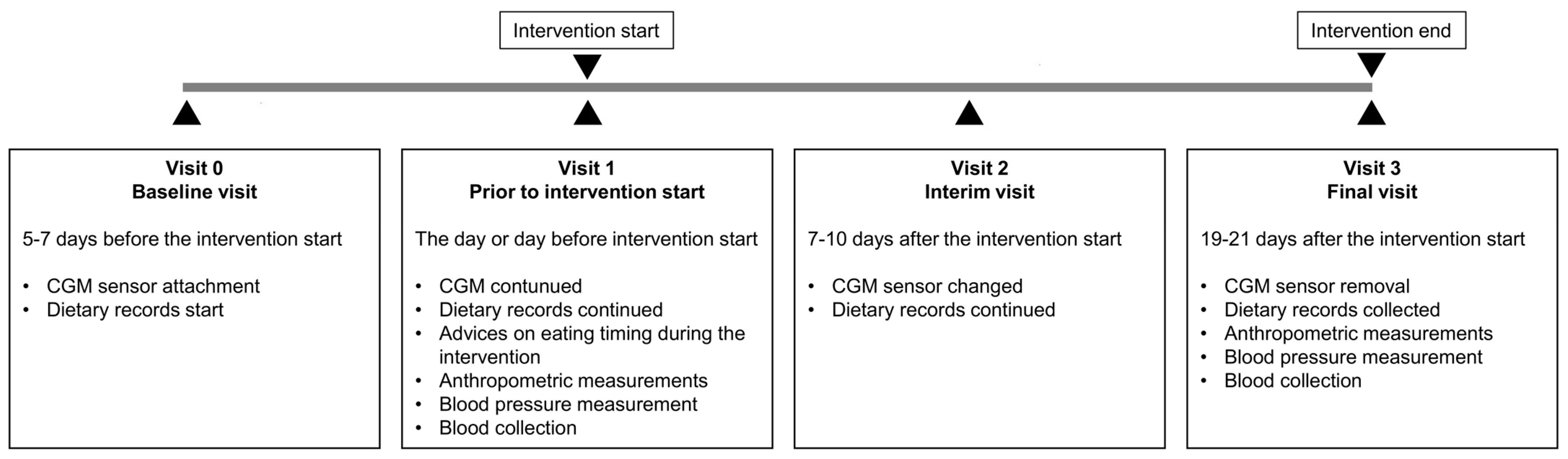
2.1. Study Design
2.2. Study Subjects and Eligibility Criteria
2.3. Fasting Interventions, Dietary Records, and Assessment of Timely Compliance
2.4. Anthropometric Measurements
2.5. Continuous Glucose Monitoring (CGM) and HbA1c Assessment
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Population
3.2. Timely Compliance
3.3. Energy and Macronutrient Intakes
3.4. Anthropometric Measurements and Blood Pressure
3.5. Twenty-Four Hour Glucose Profiles and Glycemic Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Cabo, R.; Mattson, M.P. Effects of Intermittent Fasting on Health, Aging, and Disease. N. Engl. J. Med. 2019, 381, 2541–2551. [Google Scholar] [CrossRef] [PubMed]
- Rahmatullah; Ahmedani, M.Y.; Basit, A.; Zia, S.; Hasan, I.; Masroor, Q.; Shaikh, A.; Khan, J.; Iqbal, W. Evidence-based risk factors for major complications during Ramadan fasting in people with diabetes grouped under IDF-DAR risk categories. Diabetes Res. Clin. Pract. 2022, 185, 109234. [Google Scholar] [CrossRef] [PubMed]
- Ba-Essa, E.M.; Hassanein, M.; Abdulrhman, S.; Alkhalifa, M.; Alsafar, Z. Attitude and safety of patients with diabetes observing the Ramadan fast. Diabetes Res. Clin. Pract. 2019, 152, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Baháʼuʼlláh. The Kitáb-i-Aqdas: The Most Holy Book, 1st ed.; Baha’i Publishing Trust: London, UK, 1993; 315p. [Google Scholar]
- Mähler, A.; Jahn, C.; Klug, L.; Klatte, C.; Michalsen, A.; Koppold-Liebscher, D.; Boschmann, M. Metabolic Response to Daytime Dry Fasting in Bahá’í Volunteers-Results of a Preliminary Study. Nutrients 2021, 14, 148. [Google Scholar] [CrossRef] [PubMed]
- Hassanein, M.; Afandi, B.; Yakoob Ahmedani, M.; Mohammad Alamoudi, R.; Alawadi, F.; Bajaj, H.S.; Basit, A.; Bennakhi, A.; El Sayed, A.A.; Hamdy, O.; et al. Diabetes and Ramadan: Practical guidelines 2021. Diabetes Res. Clin. Pract. 2022, 185, 109185. [Google Scholar] [CrossRef] [PubMed]
- Ali, T.; Lessan, N. Chrononutrition in the context of Ramadan: Potential implications. Diabetes Metab. Res. Rev. 2024, 40, e3728. [Google Scholar] [CrossRef] [PubMed]
- Koppold-Liebscher, D.A.; Klatte, C.; Demmrich, S.; Schwarz, J.; Kandil, F.I.; Steckhan, N.; Ring, R.; Kessler, C.S.; Jeitler, M.; Koller, B.; et al. Effects of Daytime Dry Fasting on Hydration, Glucose Metabolism and Circadian Phase: A Prospective Exploratory Cohort Study in Bahá’í Volunteers. Front. Nutr. 2021, 8, 662310. [Google Scholar] [CrossRef] [PubMed]
- Alawadi, F.; Rashid, F.; Bashier, A.; Abdelgadir, E.; Al Saeed, M.; Abuelkheir, S.; Khalifa, A.; Al sayyah, F.; Bachet, F.; Elsayed, M.; et al. The use of Free Style Libre Continues Glucose Monitoring (FSL-CGM) to monitor the impact of Ramadan fasting on glycemic changes and kidney function in high-risk patients with diabetes and chronic kidney disease stage 3 under optimal diabetes care. Diabetes Res. Clin. Pract. 2019, 151, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Salti, I.; Bénard, E.; Detournay, B.; Bianchi-Biscay, M.; Le Brigand, C.; Voinet, C.; Jabbar, A.; EPIDIAR Study Group. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: Results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care 2004, 27, 2306–2311. [Google Scholar] [CrossRef]
- Zouhal, H.; Bagheri, R.; Triki, R.; Saeidi, A.; Wong, A.; Hackney, A.C.; Laher, I.; Suzuki, K.; Ben Abderrahman, A. Effects of Ramadan Intermittent Fasting on Gut Hormones and Body Composition in Males with Obesity. Int. J. Environ. Res. Public Health 2020, 17, 5600. [Google Scholar] [CrossRef]
- Lum, Z.K.; Khoo, Z.R.; Toh, W.Y.S.; Kamaldeen, S.A.K.; Shakoor, A.; Tsou, K.Y.K.; Chew, D.E.K.; Dalan, R.; Kwek, S.C.; Othman, N.; et al. Efficacy and Safety of Use of the Fasting Algorithm for Singaporeans with Type 2 Diabetes (FAST) During Ramadan: A Prospective, Multicenter, Randomized Controlled Trial. Ann. Fam. Med. 2020, 18, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Tay, J.; Thompson, C.H.; Brinkworth, G.D. Glycemic Variability: Assessing Glycemia Differently and the Implications for Dietary Management of Diabetes. Annu. Rev. Nutr. 2015, 35, 389–424. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.H.; Han, K.; Park, S.; Lee, D.Y.; Nam, G.E.; Seo, J.A.; Kim, S.G.; Baik, S.H.; Park, Y.G.; Kim, S.M.; et al. Effects of long-term glycemic variability on incident cardiovascular disease and mortality in subjects without diabetes: A nationwide population-based study. Medicine 2019, 98, e16317. [Google Scholar] [CrossRef] [PubMed]
- Afandi, B.; Kaplan, W.; Al Hassani, N.; Hadi, S.; Mohamed, A. Correlation between pre-ramadan glycemic control and subsequent glucose fluctuation during fasting in adolescents with Type 1 diabetes. J. Endocrinol. Investig. 2017, 40, 741–744. [Google Scholar] [CrossRef] [PubMed]
- Saadane, I.; Ali, T.; El-Laboudi, A.; Lessan, N. Ramadan fasting in insulin-treated patients is associated with potentially unfavourable changes in glucose metrics: A flash glucose monitoring (FGM) study. Diabetes Res. Clin. Pract. 2021, 172, 108592. [Google Scholar] [CrossRef] [PubMed]
- Lessan, N.; Hannoun, Z.; Hasan, H.; Barakat, M.T. Glucose excursions and glycaemic control during Ramadan fasting in diabetic patients: Insights from continuous glucose monitoring (CGM). Diabetes Metab. 2015, 41, 28–36. [Google Scholar] [CrossRef]
- Elmalti, A.; Mukhtar, M.; Kenz, S.; Skaria, S.; Elgzyri, T. Transient increase in glucose variability during Ramadan fasting in patients with insulin-treated type 2 diabetes: A preliminary study. Diabetes Metab. Syndr. 2023, 17, 102745. [Google Scholar] [CrossRef]
- Aldawi, N.; Darwiche, G.; Abusnana, S.; Elbagir, M.; Elgzyri, T. Initial increase in glucose variability during Ramadan fasting in non-insulin-treated patients with diabetes type 2 using continuous glucose monitoring. Libyan J. Med. 2019, 14, 1535747. [Google Scholar] [CrossRef]
- Peters, B.; Koppold-Liebscher, D.A.; Schuppelius, B.; Steckhan, N.; Pfeiffer, A.F.H.; Kramer, A.; Michalsen, A.; Pivovarova-Ramich, O. Effects of Early vs. Late Time-Restricted Eating on Cardiometabolic Health, Inflammation, and Sleep in Overweight and Obese Women: A Study Protocol for the ChronoFast Trial. Front. Nutr. 2021, 8, 765543. [Google Scholar] [CrossRef]
- Schuppelius, B.; Peters, B.; Ottawa, A.; Pivovarova-Ramich, O. Time Restricted Eating: A Dietary Strategy to Prevent and Treat Metabolic Disturbances. Front. Endocrinol. 2021, 12, 683140. [Google Scholar] [CrossRef]
- Tsitsou, S.; Zacharodimos, N.; Poulia, K.A.; Karatzi, K.; Dimitriadis, G.; Papakonstantinou, E. Effects of Time-Restricted Feeding and Ramadan Fasting on Body Weight, Body Composition, Glucose Responses, and Insulin Resistance: A Systematic Review of Randomized Controlled Trials. Nutrients 2022, 14, 4778. [Google Scholar] [CrossRef]
- Obst, M.A.; Heldmann, M.; Alicart, H.; Tittgemeyer, M.; Münte, T.F. Effect of Short-Term Transcutaneous Vagus Nerve Stimulation (tVNS) on Brain Processing of Food Cues: An Electrophysiological Study. Front. Hum. Neurosci. 2020, 14, 206. [Google Scholar] [CrossRef]
- Pappe, C.L.; Peters, B.; Dommisch, H.; Woelber, J.P.; Pivovarova-Ramich, O. Effects of reducing free sugars on 24-hour glucose profiles and glycemic variability in subjects without diabetes. Front. Nutr. 2023, 10, 1213661. [Google Scholar] [CrossRef]
- Aston, L.M.; Jackson, D.; Monsheimer, S.; Whybrow, S.; Handjieva-Darlenska, T.; Kreutzer, M.; Kohl, A.; Papadaki, A.; Martinez, J.A.; Kunova, V.; et al. Developing a methodology for assigning glycaemic index values to foods consumed across Europe. Obes. Rev. 2010, 11, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Manson, J.; Liu, S. Glycemic index, glycemic load, and risk of type 2 diabetes. Am. J. Clin. Nutr. 2002, 76, 274s–280s. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.R.; Oliver, N.S.; Choudhary, P.; Levy, J.C.; Hindmarsh, P.; Matthews, D.R. Normal reference range for mean tissue glucose and glycemic variability derived from continuous glucose monitoring for subjects without diabetes in different ethnic groups. Diabetes Technol. Ther. 2011, 13, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Hermanides, J.; Vriesendorp, T.M.; Bosman, R.J.; Zandstra, D.F.; Hoekstra, J.B.; DeVries, J.H. Glucose variability is associated with intensive care unit mortality. Crit. Care Med. 2010, 38, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, M.N.; Skytte, M.J.; Astrup, A.; Deacon, C.F.; Holst, J.J.; Madsbad, S.; Krarup, T.; Haugaard, S.B.; Samkani, A. The clinical effects of a carbohydrate-reduced high-protein diet on glycaemic variability in metformin-treated patients with type 2 diabetes mellitus: A randomised controlled study. Clin. Nutr. ESPEN 2020, 39, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Antoni, R.; Robertson, T.M.; Robertson, M.D.; Johnston, J.D. A pilot feasibility study exploring the effects of a moderate time-restricted feeding intervention on energy intake, adiposity and metabolic physiology in free-living human subjects. J. Nutr. Sci. 2018, 7, e22. [Google Scholar] [CrossRef]
- Chow, L.S.; Manoogian, E.N.C.; Alvear, A.; Fleischer, J.G.; Thor, H.; Dietsche, K.; Wang, Q.; Hodges, J.S.; Esch, N.; Malaeb, S.; et al. Time-Restricted Eating Effects on Body Composition and Metabolic Measures in Humans who are Overweight: A Feasibility Study. Obesity 2020, 28, 860–869. [Google Scholar] [CrossRef]
- Jamshed, H.; Beyl, R.A.; Della Manna, D.L.; Yang, E.S.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves 24-Hour Glucose Levels and Affects Markers of the Circadian Clock, Aging, and Autophagy in Humans. Nutrients 2019, 11, 1234. [Google Scholar] [CrossRef] [PubMed]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q.F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. J. Transl. Med. 2016, 14, 290. [Google Scholar] [CrossRef] [PubMed]
- Peeke, P.M.; Greenway, F.L.; Billes, S.K.; Zhang, D.; Fujioka, K. Effect of time restricted eating on body weight and fasting glucose in participants with obesity: Results of a randomized, controlled, virtual clinical trial. Nutr. Diabetes 2021, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, A.T.; Regmi, P.; Manoogian, E.N.C.; Fleischer, J.G.; Wittert, G.A.; Panda, S.; Heilbronn, L.K. Time-Restricted Feeding Improves Glucose Tolerance in Men at Risk for Type 2 Diabetes: A Randomized Crossover Trial. Obesity 2019, 27, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Martens, C.R.; Rossman, M.J.; Mazzo, M.R.; Jankowski, L.R.; Nagy, E.E.; Denman, B.A.; Richey, J.J.; Johnson, S.A.; Ziemba, B.P.; Wang, Y.; et al. Short-term time-restricted feeding is safe and feasible in non-obese healthy midlife and older adults. Geroscience 2020, 42, 667–686. [Google Scholar] [CrossRef] [PubMed]
- Parr, E.B.; Devlin, B.L.; Radford, B.E.; Hawley, J.A. A Delayed Morning and Earlier Evening Time-Restricted Feeding Protocol for Improving Glycemic Control and Dietary Adherence in Men with Overweight/Obesity: A Randomized Controlled Trial. Nutrients 2020, 12, 505. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome. Cell Metab. 2020, 31, 92–104.e5. [Google Scholar] [CrossRef]
- Kesztyüs, D.; Cermak, P.; Gulich, M.; Kesztyüs, T. Adherence to Time-Restricted Feeding and Impact on Abdominal Obesity in Primary Care Patients: Results of a Pilot Study in a Pre-Post Design. Nutrients 2019, 11, 2854. [Google Scholar] [CrossRef] [PubMed]
- Lowe, D.A.; Wu, N.; Rohdin-Bibby, L.; Moore, A.H.; Kelly, N.; Liu, Y.E.; Philip, E.; Vittinghoff, E.; Heymsfield, S.B.; Olgin, J.E.; et al. Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men with Overweight and Obesity: The TREAT Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 1491–1499. [Google Scholar] [CrossRef]
- Parr, E.B.; Devlin, B.L.; Lim, K.H.C.; Moresi, L.N.Z.; Geils, C.; Brennan, L.; Hawley, J.A. Time-Restricted Eating as a Nutrition Strategy for Individuals with Type 2 Diabetes: A Feasibility Study. Nutrients 2020, 12, 3228. [Google Scholar] [CrossRef]
- Haganes, K.L.; Silva, C.P.; Eyjólfsdóttir, S.K.; Steen, S.; Grindberg, M.; Lydersen, S.; Hawley, J.A.; Moholdt, T. Time-restricted eating and exercise training improve HbA1c and body composition in women with overweight/obesity: A randomized controlled trial. Cell Metab. 2022, 34, 1457–1471.e4. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, E.C.; Zainudin, S.B.; Loh, W.N.; Chua, C.L.; Fun, S.; Subramaniam, T.; Sum, C.F.; Lim, S.C. Fasting during Ramadan and Associated Changes in Glycaemia, Caloric Intake and Body Composition with Gender Differences in Singapore. Ann. Acad. Med. Singap. 2015, 44, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Fernando, H.A.; Zibellini, J.; Harris, R.A.; Seimon, R.V.; Sainsbury, A. Effect of Ramadan Fasting on Weight and Body Composition in Healthy Non-Athlete Adults: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 478. [Google Scholar] [CrossRef] [PubMed]
- Sadeghirad, B.; Motaghipisheh, S.; Kolahdooz, F.; Zahedi, M.J.; Haghdoost, A.A. Islamic fasting and weight loss: A systematic review and meta-analysis. Public Health Nutr. 2014, 17, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Al-Barha, N.S.; Aljaloud, K.S. The Effect of Ramadan Fasting on Body Composition and Metabolic Syndrome in Apparently Healthy Men. Am. J. Mens Health 2019, 13, 1557988318816925. [Google Scholar] [CrossRef] [PubMed]
- Kessler, K.; Pivovarova-Ramich, O. Meal Timing, Aging, and Metabolic Health. Int. J. Mol. Sci. 2019, 20, 1911. [Google Scholar] [CrossRef] [PubMed]
- Kohsaka, A.; Laposky, A.D.; Ramsey, K.M.; Estrada, C.; Joshu, C.; Kobayashi, Y.; Turek, F.W.; Bass, J. High-fat diet disrupts behavioral and molecular circadian rhythms in mice. Cell Metab. 2007, 6, 414–421. [Google Scholar] [CrossRef]
- Zhao, L.; Hutchison, A.T.; Liu, B.; Wittert, G.A.; Thompson, C.H.; Nguyen, L.; Au, J.; Vincent, A.; Manoogian, E.N.; Le, H.D.; et al. Time-restricted eating alters the 24-hour profile of adipose tissue transcriptome in men with obesity. Obesity 2023, 31, 63–74. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group | BF Group | TRE Group | |
|---|---|---|---|
| Clinical characteristics | |||
| N | 4 | 6 | 6 |
| Male | 2 | 3 | 3 |
| Age [years] | 29 (28–35) | 31 (22–43) | 28 (25–32) |
| Weight [kg] | 85.9 ± 24.2 | 80.1 ± 18.1 | 79.5 ± 14.0 |
| BMI [kg/m2] | 27.4 ± 6.2 | 26.8 ± 3.9 | 25.5 ± 3.9 |
| Waist circumference [cm] | 89.5 ± 21.0 | 91.9 ± 17.8 | 85.2 ± 5.8 |
| SBP [mmHg] | 131.0 ± 20.2 | 132.3 ± 10.5 | 126.2 ± 12.6 |
| DBP [mmHg] | 78.0 ± 13.7 | 83.8 ± 6.6 | 85.0 ± 11.1 |
| Glycemic parameters | |||
| MSG [mmol/L] | 5.74 ± 0.47 | 5.56 ± 0.30 | 5.44 ± 0.57 |
| Minimum [mmol/L] | 4.96 ± 0.54 | 4.79 ± 0.35 | 4.72 ± 0.51 |
| Maximum [mmol/L] | 6.77 ± 0.44 | 6.68 ± 0.38 | 6.69 ± 0.74 |
| TBR < 3.9 mmol/L [%] | 0.20 (0.00–4.39) | 0.78 (0.00–2.73) | 0.23 (0.00–3.83) |
| TAR > 10 mmol/L [%] | 0.10 (0.00–0.37) | 0.00 (0.00–0.81) | 0.00 (0.00–0.12) |
| AUCgluc [min × mmol/L] | 8217 ± 673 | 7964 ± 431 | 7789 ± 813 |
| SD [mmol/L] | 0.81 ± 0.29 | 0.83 ± 0.10 | 0.78 ± 0.11 |
| CV [%] | 14.2 ± 5.69 | 14.9 ± 1.55 | 14.4 ± 1.79 |
| MAGE [mmol/L] | 1.03 ± 0.31 | 1.13 ± 0.05 | 1.09 ± 0.12 |
| CONGA [mmol/L] | 5.23 ± 0.44 | 4.96 ± 0.27 | 4.93 ± 0.57 |
| MAG change [mmol/L/h] | 1.12 ± 0.26 | 1.21 ± 0.08 | 1.09 ± 0.09 |
| MODD [mmol/L] | 0.73 ± 0.21 | 0.75 ± 0.08 | 0.66 ± 0.06 |
| LBGI | 1.28 ± 1.09 | 1.44 ± 0.61 | 1.86 ± 1.40 |
| HBGI | 0.78 ± 0.58 | 0.70 ± 0.31 | 0.59 ± 0.21 |
| HbA1c [%] | 5.10 ± 0.29 | 5.13 ± 0.42 | 5.07 ± 0.16 |
| Control Group | BF Group | TRE Group | p-Value Between-Groups Analysis c | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Changes a | p-Value b | Changes a | p-Value b | Changes a | p-Value b | BF vs. Control | TRE vs. Control | TRE vs. BF | |
| Glycemic Parameters | |||||||||
| MSG [mmol/L] | −0.05 ± 0.24 | 0.710 | 0.17 ± 0.26 | 0.220 | 0.05 ± 0.27 | 0.690 | 0.556 | 0.921 | 0.871 |
| Minimum [mmol/L] | 0.20 ± 0.46 | 0.460 | 0.19 ± 0.27 | 0.187 | 0.08 ± 0.25 | 0.520 | 1.000 | 0.941 | 0.939 |
| Maximum [mmol/L] | −0.55 ± 0.19 | 0.011 | 1.41 ± 1.04 | 0.039 | −0.22 ± 0.75 | 0.556 | 0.010 | 0.901 | 0.022 |
| TBR < 3.9 mmol/L [%] | −0.11 (−2.56–0.00) | 0.180 | −0.78 (−2.45–0.67) | 0.273 | 0.08 (−2.85–0.70) | 0.715 | 1.000 | 1.000 | 1.000 |
| TAR > 10 mmol/L [%] | −0.07 (−0.31–0.00) | 0.180 | 0.38 (0.00–2.52) | 0.109 | 0.00 (0.00–0.15) | 0.317 | 0.012 | 0.180 | 0.209 |
| AUCgluc [min × mmol/L] | −71 ± 343 | 0.705 | 241 ± 367 | 0.216 | 79 ± 388 | 0.673 | 0.548 | 0.912 | 0.876 |
| Glycemic Variability | |||||||||
| SD [mmol/L] | −0.07 ± 0.14 | 0.423 | 0.13 ± 0.18 | 0.184 | −0.02 ± 0.05 | 0.422 | 0.155 | 0.950 | 0.287 |
| CV [%] | −1.19 ± 3.16 | 0.507 | 1.71 ± 2.57 | 0.226 | −0.54 ± 1.34 | 0.422 | 0.270 | 0.971 | 0.422 |
| MAGE [mmol/L] | −0.14 ± 0.13 | 0.121 | 0.19 ± 0.34 | 0.251 | −0.12 ± 0.13 | 0.113 | 0.130 | 0.999 | 0.133 |
| CONGA [mmol/L] | −0.02 ± 0.22 | 0.893 | 0.18 ± 0.26 | 0.188 | 0.14 ± 0.31 | 0.370 | 0.648 | 0.792 | 0.992 |
| MAG change [mmol/L/h] | −0.11 ± 0.06 | 0.036 | −0.10 ± 0.16 | 0.238 | −0.16 ± 0.19 | 0.135 | 1.000 | 0.952 | 0.925 |
| MODD [mmol/L] | −0.04 ± 0.09 | 0.473 | −0.12 ± 0.12 | 0.098 | −0.07 ± 0.07 | 0.098 | 0.599 | 0.957 | 0.848 |
| LBGI | −0.13 ± 0.72 | 0.738 | −0.28 ± 0.46 | 0.244 | −0.27 ± 0.86 | 0.523 | 0.986 | 0.989 | 1.000 |
| HBGI | −0.31 ± 0.40 | 0.220 | 0.60 ± 0.79 | 0.164 | −0.13 ± 0.15 | 0.118 | 0.077 | 0.953 | 0.141 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peters, B.; Pappe, C.L.; Koppold, D.A.; Schipp, K.; Arnrich, B.; Michalsen, A.; Dommisch, H.; Steckhan, N.; Pivovarova-Ramich, O. Twenty-Four Hour Glucose Profiles and Glycemic Variability during Intermittent Religious Dry Fasting and Time-Restricted Eating in Subjects without Diabetes: A Preliminary Study. Nutrients 2024, 16, 2663. https://doi.org/10.3390/nu16162663
Peters B, Pappe CL, Koppold DA, Schipp K, Arnrich B, Michalsen A, Dommisch H, Steckhan N, Pivovarova-Ramich O. Twenty-Four Hour Glucose Profiles and Glycemic Variability during Intermittent Religious Dry Fasting and Time-Restricted Eating in Subjects without Diabetes: A Preliminary Study. Nutrients. 2024; 16(16):2663. https://doi.org/10.3390/nu16162663
Chicago/Turabian StylePeters, Beeke, Christina Laetitia Pappe, Daniela A. Koppold, Katharina Schipp, Bert Arnrich, Andreas Michalsen, Henrik Dommisch, Nico Steckhan, and Olga Pivovarova-Ramich. 2024. "Twenty-Four Hour Glucose Profiles and Glycemic Variability during Intermittent Religious Dry Fasting and Time-Restricted Eating in Subjects without Diabetes: A Preliminary Study" Nutrients 16, no. 16: 2663. https://doi.org/10.3390/nu16162663
APA StylePeters, B., Pappe, C. L., Koppold, D. A., Schipp, K., Arnrich, B., Michalsen, A., Dommisch, H., Steckhan, N., & Pivovarova-Ramich, O. (2024). Twenty-Four Hour Glucose Profiles and Glycemic Variability during Intermittent Religious Dry Fasting and Time-Restricted Eating in Subjects without Diabetes: A Preliminary Study. Nutrients, 16(16), 2663. https://doi.org/10.3390/nu16162663