

Political Economy of Maternal Child Malnutrition: Experiences about Water, Food, and Nutrition Policies in Pakistan

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Analysis
2.2. Ethical Consideration
2.3. Strength and Limitation
3. Results
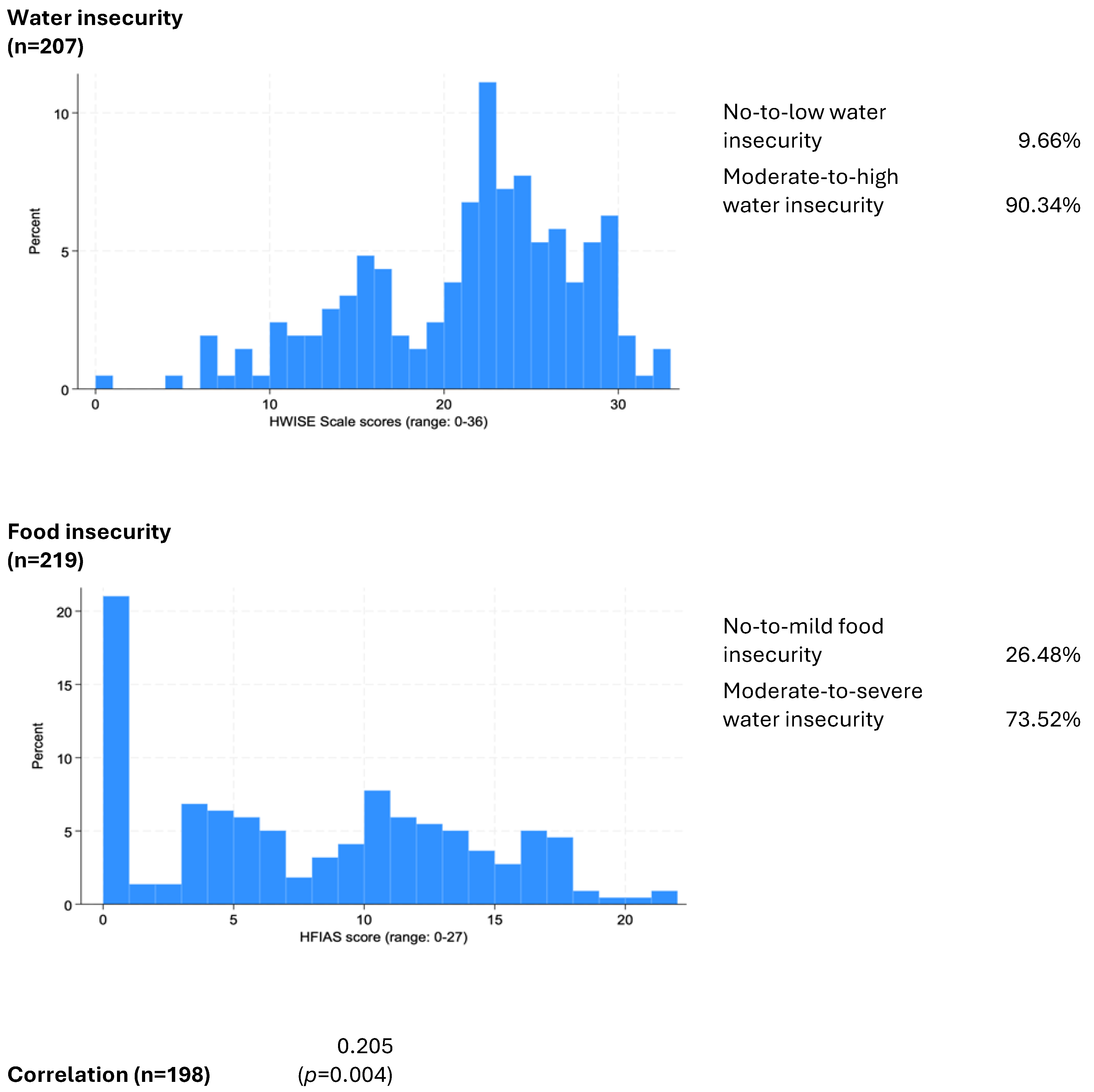
3.1. Quantitative Water and Food Insecurity Experiences
3.2. Qualitative Water and Food Insecurity Experiences
3.2.1. Water Insecurity Experiences at the Community Level
3.2.2. Food Insecurity Experiences at Community Level
3.2.3. Experiences with Nutritional Programs and Policies
4. Discussion
4.1. Political Economy of Water Insecurity
4.2. Political Economy of Food Insecurity
4.3. Political-Economy of Nutrition Programs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Children Fund. Nutrition, for Every Child: UNICEF Nutrition Strategy 2020–2030; UNICEF: New York, NY, USA, 2020; Available online: https://www.unicef.org/media/92031/file/UNICEF%20Nutrition%20Strategy%202020-2030.pdf (accessed on 2 August 2023).
- Demissie, S.; Worku, A. Magnitude and factors associated with malnutrition in children 6–59 months of age in pastoral community of Dollo Ado district, Somali region, Ethiopia. Sci. J. Public Health 2013, 1, 175–183. [Google Scholar] [CrossRef]
- United Nations Children Fund. Tracking Progress on Child and Maternal Nutrition: A Survival and Development Priority; United Nations Children Fund: New York, NY, USA, 2009. [Google Scholar]
- UNICEF; WHO; World Bank. Levels and Trends in Child Malnutrition. In Joint Child Malnutrition Estimates; UNICEF: New York, NY, USA; WHO: Geneva, Switzerland; World Bank: Washington, DC, USA, 2012. [Google Scholar]
- Gross, R.; Webb, P. Wasting time for wasted children: Severe child undernutrition must be resolved in non-emergency settings. Lancet 2006, 367, 1209–1211. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Gazdar, H.; Haddad, L. Seeing the unseen: Breaking the logjam of undernutrition in Pakistan. IDS Bull. 2013, 44, 1–9. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Hafeez, A.; Rizvi, A. Reproductive, maternal, newborn, and child health in Pakistan: Challenges and opportunities. Lancet 2013, 381, 2207–2218. [Google Scholar] [CrossRef] [PubMed]
- Pakistan Demographic and Health Survey; Islamabad and Calverton, National Institute of Population Studies and ICF International: MA, USA, 2013; Available online: https://dhsprogram.com/pubs/pdf/FR290/FR290.pdf (accessed on 2 August 2023).
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- Govt of Pakistan; UNICEF. UKAID Pakistan National Nutrition Survey. 2018. Available online: https://www.unicef.org/pakistan/reports/national-nutrition-survey-2018-key-findings-report (accessed on 17 July 2024).
- Katoch, O.R. Determinants of malnutrition among children: A systematic review. Nutrition 2022, 96, 111565. [Google Scholar] [CrossRef]
- Toma, A.; Talukder, A.; Shirin Khan, S.; Razu, S.R. An assessment of the association between antenatal care and child malnutrition in Bangladesh. Fam. Med. Prim. Care Rev. 2018, 4, 373–378. [Google Scholar] [CrossRef]
- Rahman, M.; Islam, M.J.; Haque, S.E.; Saw, Y.M.; Haque, M.N.; Duc, N.H.; Al-Sobaihi, S.; Saw, T.N.; Mostofa, M.G.; Islam, M.R. Association between high-risk fertility behaviours and the likelihood of chronic undernutrition and anaemia among married Bangladeshi women of reproductive age. Public Health Nutr. 2017, 20, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Shahid, M.; Cao, Y.; Ahmed, F.; Raza, S.; Guo, J.; Malik, N.I.; Rauf, U.; Qureshi, M.G.; Saheed, R.; Maryam, R. Does Mothers’ Awareness of Health and Nutrition Matter? A Case Study of Child Malnutrition in Marginalized Rural Community of Punjab, Pakistan. Front. Public Health 2022, 10, 792164. [Google Scholar] [CrossRef]
- Nguyen, P.H.; Saha, K.K.; Ali, D.; Menon, P.; Manohar, S.; Mai, L.T.; Rawat, R.; Ruel, M.T. Maternal mental health is associated with child undernutrition and illness in Bangladesh, Vietnam and Ethiopia. Public Health Nutr. 2014, 17, 1318–1327. [Google Scholar] [CrossRef]
- Mukhopadhyay, S. The intersection of gender, caste and class inequalities in child nutrition in rural India. Asian Popu Studs. 2015, 2, 17–31. [Google Scholar] [CrossRef]
- Shahid, M.; Ahmed, F.; Ameer, W.; Guo, J.; Raza, S.; Fatima, S.; Qureshi, M.G. Prevalence of child malnutrition and household socioeconomic deprivation: A case study of marginalized district in Punjab, Pakistan. PLoS ONE 2022, 17, e0263470. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, S.; Haddad, L.; Mannar, V.; Menon, P.; Nisbett, N. The politics of reducing malnutrition: Building commitment and accelerating progress. Lancet 2013, 10, 552–569. [Google Scholar] [CrossRef] [PubMed]
- Fakir, A.M.S.; Khan, M.W.R. Determinants of malnutrition among urban slum children in Bangladesh. Health Econ. Rev. 2015, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, N.; Schuster, R.; Brewis, A.; Wutich, A. Water insecurity potentially undermines dietary diversity of children aged6–23 months: Evidence from India. Matern. Child. Nutri. 2020, 16, e12929. [Google Scholar] [CrossRef] [PubMed]
- Sultana, F.; Loftus, A. Water Politics: Governance, Justice, and the Right to Water; Routledge: Abingdon, UK; New York, NY, USA, 2020. [Google Scholar]
- Puett, C.; Guerrero, S. Barriers to access for severe acute malnutrition treatment services in Pakistan and Ethiopia: A comparative qualitative analysis. Public Health Nutr. 2015, 18, 1873–1882. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Malik, N.I.; Malik, N.; Qureshi, M.G.; Shahzad, M.; Shahid, M.; Zia, S.; Tang, K. Key challenges to optimal therapeutic coverage and maternal utilization of CMAM Program in rural southern Pakistan: A qualitative exploratory study. Nutrients 2022, 14, 2612. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Malik, N.I.; Zia, S.; Akbar, A.S.; Li, X.; Shahid, M.; Tang, K. Rural mothers’ beliefs and practices about diagnosis, treatment, and management of children health problems: A qualitative study in marginalized Southern Pakistan. Front. Public Health 2023, 10, 1001668. [Google Scholar] [CrossRef]
- Scheper-Hughes, N.; Lock, M. The Mindful Body: A Prolegomenon to Future Work in Medical Anthropology. Med. Anthro. Quarter 1987, 1, 6–41. [Google Scholar] [CrossRef]
- Escobar, A. Encountering Development: The Making and Unmaking of the Third World; Princeton University Press: Princeton, NJ, USA, 1995. [Google Scholar]
- Ferguson, J. The Anti-Politics Machine: “Development,” Depoliticization and Bureaucratic Power in Lesotho; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar]
- Khan, S.R.; Aftab, S. Sustainable Development Policy Institute. In Structural Adjustment, Labor and the Poor in Pakistan; Sustainable Development Policy Institute: Islamabad, Pakistan, 1995. [Google Scholar]
- Abbasi, K. The World Bank and world health: Focus on South Asia-II: India and Pakistan. BMJ 1999, 318, 1132–1135. [Google Scholar] [CrossRef]
- Haider, M. Pakistan’s Total Debt, Liabilities Rise to Rs35tr. 21 May 2019. Available online: https://www.thenews.com.pk/print/473930-pakistan-s-total-debt-liabilities-rise-to-rs35tr (accessed on 6 March 2020).
- Younus, U. Pakistan’s Debt Policy Has Brought Us to the Brink. Another Five Years of the Same is Unsustainable. DAWN. 30 October 2018. Available online: https://www.dawn.com/news/1442378 (accessed on 16 October 2019).
- Bhutta, Z.A. Structural adjustments and their impact on health and society: A perspective from Pakistan. Int. J. Epi. 2001, 30, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Himmelgreen, D.; Romero-Daza, N. Anthropological approaches to the global food crisis: Understanding and addressing the “Silent Tsunami”. Napa Bull. 2009, 32, 1–11. [Google Scholar] [CrossRef]
- Young, S.L.; Boateng, G.O.; Jamaluddine, Z.; Miller, J.D.; Frongillo, E.A.; Neilands, T.B.; Collins, S.M.; Wutich, A.; Jepson, W.E.; Stoler, J. The Household Water InSecurity Experiences (HWISE) Scale: Development and validation of a household water insecurity measure for low-income and middle-income countries. BMJ Global Health 2019, 4, e001750. [Google Scholar] [CrossRef]
- Workman, C.L.; Ureksoy, H. Water insecurity in a syndemic context: Understanding the psycho-emotional stress of water insecurity in Lesotho, Africa. Soc. Sci. Med. 2017, 179, 52–60. [Google Scholar] [CrossRef]
- Workman, C.L.; Brewis, A.; Wutich, A.; Young, S.; Stoler, J.; Kearns, J. Understanding biopsychosocial health outcomes of syndemic water and food insecurity: Applications for global health. Am. J. Trop. Med. Hyg. 2021, 104, 8. [Google Scholar] [CrossRef]
- Boateng, G.O.; Workman, C.L.; Miller, J.D.; Onono, M.; Neilands, T.B.; Young, S.L. The syndemic effects of food insecurity, water insecurity, and HIV on depressive symptomatology among Kenyan women. Soc. Sci. Med. 2022, 1, 113043. [Google Scholar] [CrossRef] [PubMed]
- Kohrt, B.A.; Mendenhall, E. Social and structural origins of mental illness in global context. In Global Mental Health: Anthropological Perspectives; Routledge: New York, NY, USA, 2016; pp. 51–56. [Google Scholar]
- Brewis, A.; Choudhary, N.; Wutich, A. Household water insecurity may influence common mental disorders directly and indirectly through multiple pathways: Evidence from Haiti. Soc. Sci. Med. 2019, 1, 112520. [Google Scholar] [CrossRef] [PubMed]
- Wutich, A.; Brewis, A.; Tsai, A. Water and mental health. Wiley Interdisciplinary Reviews: Water 2020, 7, e1461. [Google Scholar] [CrossRef]
- Young, S.; Frongillo, E.; Jamaluddine, Z.; Melgar-Quiñonez, H.; Pérez-Escamilla, R.; Ringler, C.; Rosinger, A. The importance of water security for ensuring food security, good nutrition, and well-being. Adv. Nutri 2021, 1, 1058–1073. [Google Scholar] [CrossRef]
- Ringler, C.; Paulo, D. Water and nutrition: Harmonizing Actions for the United Nations Decade of Action on Nutrition and the United Nations Water Action Decade; United Nations System Standing Committee on Nutrition: Rome, Italy, 2020; Available online: https://www.unscn.org/uploads/web/news/document/Water-Paper-EN-WEB-12feb.pdf (accessed on 22 September 2020).
- Miller, J.D.; Frongillo, E.A.; Weke, E.; Burger, R.; Wekesa, P.; Sheira, L.A.; Mocello, A.R.; Bukusi, E.A.; Otieno, P.; Cohen, C.R.; et al. Household water and food insecurity are positively associated with poor mental and physical health among adults living with HIV in Western Kenya. J. Nutri. 2021, 151, 1656–1664. [Google Scholar] [CrossRef]
- D’Souza, R. Water in British India: The Making of a Colonial Hydrology. Hist. Compass 2006, 4, 621–628. [Google Scholar] [CrossRef]
- Agnihotri, I. Ecology, Land Use and Colonization: The Canal Colonies of Punjab. Indian Eco. Soc. Hist. Rev. 1996, 33, 37–58. [Google Scholar] [CrossRef]
- Mustafa, D.; Gioli, G.; Karner, M.; Khan, I. Contested Waters: The Sub-National Scale of Water and Conflict in Pakistan; United States Institute for Peace USIP: Washington, DC, USA, 2017. [Google Scholar]
- Gilmartin, D. Water and Waste: Nature, Productivity and Colonialism in the Indus Basin. Econ. Polit. Wkly. 2003, 38, 5057–5065. [Google Scholar]
- Farooqi, H.; Wegerich, K. Institutionalizing Inequities in Land Ownership and Water Allocations during Colonial Times in Punjab, Pakistan. Water Hist. 2015, 7, 131–146. [Google Scholar] [CrossRef]
- Ali, I. Malign Growth? Agricultural Colonization and the Roots of Backwardness in the Punjab. Past. Present. 1987, 114, 110–132. [Google Scholar] [CrossRef]
- Mustafa, D.; Sawas, A. Urbanization and Political Change in Pakistan: Exploring the Known Unknowns. Third World Q. 2013, 34, 1293–1304. [Google Scholar] [CrossRef]
- Gera, N. Food Security under Structural Adjustment in Pakistan. Asian Surv. 2004, 44, 353–368. [Google Scholar] [CrossRef]
- Kugelman, M. Pakistan’s Food Insecurity: Roots, Ramifications, and Responses. In HUNGER PAINS: Pakistan’s Food Insecurity; Kugelman, M., Hathaway, R., Eds.; The Woodrow Wilson International Center for Scholars: Washington, DC, USA, 2010; pp. 13–14. [Google Scholar]
- National Planning Commission. Government of Pakistan. Task Force on Food Security Report, 2009. Pakistan. 2009. Available online: https://www.pc.gov.pk/uploads/annualplan/2009-2010.pdf (accessed on 6 May 2017).
- Malik, S.J. Food Supply Challenges and Implications for Food Security. In HUNGER PAINS: Pakistan’s Food Insecurity; Kugelman, M., Hathaway, R., Eds.; The Woodrow Wilson International Center for Scholars: Washington, DC, USA, 2010; pp. 13–14. [Google Scholar]
- World Bank. 2015. Available online: http://data.worldbank.org/country/pakistan (accessed on 12 June 2016).
- Di-Cesare, M.; Bhatti, Z.; Soofi, S.B.; Fortunato, L.; Ezzati, M.; Bhutta, Z.A. Geographical and socioeconomic inequalities in women and children’s nutritional status in Pakistan in 2011, An analysis of data from a nationally representative survey. Lancet Glob. Health 2015, 3, e229–e239. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, S.; Bhutta, Z.A.; Rashid, A.; Nawaz, G.; Hayat, N.; Mohmand, S.K.; Acosta, A.M. Nutrition Political Economy, Pakistan; Province Report; Agha Khan University: Karachi, Pakistan, 2013. [Google Scholar]
- Ebrahim, Z. Bottle vs. Breast if Mothers Milk Is Best Why Use Formula Milk; Dawn: Karachi, Pakistan, 2015; Available online: https://www.dawn.com/news/1198547 (accessed on 25 February 2020).
- Wasif, S. Doctors Promoting Formula Milk at the Expense of Babies’ Lives. The Express Tribune, 5 October 2013. Available online: https://tribune.com.pk/story/613582/doctorspromoting-formula-milk-at-expense-of-babies-lives-islamabad-city/ (accessed on 25 February 2020).
- The News. Formula Milk Marketing Banned in Hospitals. The News, 7 October 2017. Available online: https://www.thenews.com.pk/print/235121-Formula-milk-marketingbanned-in-hospitals (accessed on 26 March 2020).
- Aziz, A.; Khan, F.A.; Wood, G. Who is excluded and how? An analysis of community spaces for maternal and child health in Pakistan. Health Res. Policy Syst. 2015, 13 (Suppl. S1), 56. [Google Scholar] [CrossRef]
- Kwiatkowski, L.M. Struggling with Development: The Politics of Hunger and Gender in the Philippines; Westview Press: Boulder, CO, USA, 1998. [Google Scholar]
- Hull, M.S. The file: Agency, authority, and autography in an Islamabad bureaucracy. Lang. Comm. 2003, 23, 287–314. [Google Scholar] [CrossRef]
- Maqbool, S. 2543 Govt. Officers among Ineligible BISP Beneficiaries. The News. 9 January 2020. Available online: https://www.thenews.com.pk/print/595841-2-543-govt-officers-among-ineligible-bisp-beneficiaries (accessed on 5 March 2020).
- Nott, J. “How Little Progress”? A Political Economy of Postcolonial Nutrition: “How Little Progress”? A Political Economy of Postcolonial Nutrition. Popul. Dev. Rev. 2018, 44, 771–791. [Google Scholar] [CrossRef]
- Ahmed, F.; Shahid, M. Understanding food insecurity experiences, dietary perceptions and practices in the households facing hunger and malnutrition in Rajanpur District, Punjab Pakistan. Pak. Perspect. 2019, 24, 115–133. [Google Scholar]
- Ahmed, F.; Malik, N.I.; Shahzad, M.; Ahmad, M.; Shahid, M.; Feng, X.L.; Guo, J. Determinants of Infant Young Child Feeding Among Mothers of Malnourished Children in South Punjab, Pakistan: A Qualitative Study. Front. Public Health 2022, 10, 834089. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Shahid, M.; Cao, Y.; Qureshi, M.G.; Zia, S.; Fatima, S.; Guo, J. A qualitative exploration in causes of water insecurity experiences, and gender and nutritional consequences in South Punjab, Pakistan. Int. J. Environ. Res. Public Health 2021, 18, 12534. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Hafeez, A. What can Pakistan do to address maternal and child health over the next decade? Health Res. Policy Sys. 2015, 13 (Suppl. S1), S49. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Details about Discussion and Interviews of This Study | No of Respondents (n) |
|---|---|
| 2 FGDs (1 with males and 1 with Females) | 20 |
| Key Informant Interviews in the Community | 5 |
| Key Informant Interviews with Healthcare Providers | 5 |
| Key Informant Interviews Officers in Nutrition Stabilization Centers | 5 |
| In-depth Interviews of local mothers availing Nutrition Programs | 20 |
| Indicator | Frequency | Percentage |
|---|---|---|
| Mothers’ Age | ||
| 18 to 24 | 6 | (30%) |
| 25 to 29 | 5 | (25%) |
| 30 to 34 | 5 | (25%) |
| 34 to 40 | 4 | (20%) |
| Literacy of Mothers | ||
| Illiterate | 16 | (80%) |
| ~5th–8th | 3 | (15%) |
| ~10th | 1 | (5%) |
| 15 to 20 | 2 | (10%) |
| Occupation of Mothers | ||
| Agriculture | 11 | (55%) |
| Domestic labour | 7 | (35%) |
| Other | 2 | (10%) |
| Income of Household per Month | ||
| ~10 K PKR (~90 USD) | 10 | (50%) |
| ~15 K PKR (~135 USD) | 7 | (35%) |
| ≥16 K PKR (~150 USD) | 3 | (15%) |
| Indicator | Frequency | Percentage |
|---|---|---|
| Sex of Participants | ||
| Female | 135 | 57.45% |
| Male | 100 | 42.55% |
| Occupation of Household Head | ||
| Cultivation | 110 | 46.80% |
| Laborers | 52 | 22.12% |
| Small business | 30 | 12.76% |
| Basic subsistence | 28 | 11.91% |
| Salaried | 13 | 5.53% |
| Monthly Income of Household | ||
| ≤Rs. 10,000 (~90 USD) | 135 | 57.45% |
| ≤Rs. 20,000 (~180 USD) | 56 | 23.82% |
| ≥Rs. 21,000 (~200 USD) | 44 | 18.72% |
| No-to-Low Water Insecurity | Moderate Water Insecurity | High Water Insecurity | ||
|---|---|---|---|---|
| (N = 20) | (N = 108) | (N = 79) | p | |
| Woman household head | 5.0% | 10.2% | 11.4% | 0.699 |
| Respondent age (years), mean ± SD | 35.3 ± 8.5 | 34.3 ± 9.6 | 36.0 ± 9.7 | 0.471 |
| Number of children living in household, mean ± SD | 3.0 ± 1.8 | 3.6 ± 2.0 | 4.8 ± 2.2 | <0.001 |
| Monthly income (USD), median (IQR) | 99 (47–180) | 90 (59–180) | 63 (45–99) | <0.001 |
| Perceived SES standing (1 = best, 10 = worst), mean ± SD | 6.3 ± 1.5 | 7.3 ± 1.5 | 8.0 ± 1.1 | <0.001 |
| Basic drinking water source | 73.7% | 92.4% | 94.9% | 0.010 |
| Drank water thought to be unsafe | 80.0% | 98.1% | 100.0% | <0.001 |
| Borrowed water from others | 57.9% | 84.8% | 96.2% | <0.001 |
| Perceived Stress Score (range: 0–16), median (IQR) | 4 (2–5) | 5 (4–9) | 7 (3–10) | 0.028 |
| HFIAS score (range: 0–27), median (IQR) | 5 (0–9) | 7 (3–12) | 8 (0–14) | 0.201 |
| Food insecurity category | ||||
| No-to-mild | 33.3% | 23.5% | 30.8% | 0.041 |
| Moderate | 38.9% | 43.1% | 21.8% | |
| Severe | 27.8% | 33.3% | 47.4% |
| No-to-Mild Food Insecurity | Moderate Food Insecurity | Severe Food Insecurity | ||
|---|---|---|---|---|
| (N = 58) | (N = 75) | (N = 86) | p | |
| Woman household head | 17.2% | 5.3% | 7.0% | 0.041 |
| Respondent age (years), mean ± SD | 33.7 ± 8.5 | 35.7 ± 9.7 | 36.3 ± 10.1 | 0.268 |
| Number of children living in household, mean ± SD | 4.1 ± 2.3 | 3.5 ± 2.0 | 4.3 ± 2.2 | 0.065 |
| Monthly income (USD), median (IQR) | 144 (90–225) | 108 (63–180) | 63 (45–90) | <0.001 |
| Perceived SES standing (1 = best, 10 = worst), mean ± SD | 6.9 ± 1.6 | 6.8 ± 1.7 | 8.3 ± 1.0 | <0.001 |
| Perceived Stress Score (range: 0–16), median (IQR) | 4 (2–4) | 4 (4–9) | 8 (6–10) | <0.001 |
| Theme | Sub-Theme | Narratives |
|---|---|---|
| Water injustice and communities’ coping strategies | Absence of water supply and availability of bad-quality water | “In the past, water distribution was much better, but now it primarily benefits large landlords and people in power. Small landholders in the South frequently experience water shortages. This change began after colonization and land control, and the situation worsened when landlords started profiting from cash crops in the 1960s”. (KII, Male, 48) “Canal water distribution in the South Punjab region is unfair, as water is available for less than six months. The canals are controlled by bureaucracy. In many areas of the D.G. Khan division, floodwater is collected in ditches because the underground water is heavy and salty. There is no water supply available here, so water supply schemes are essential. People rely solely on rain or floodwater and pray for rain in the Suleiman Mountains. The responsibility of carrying water primarily falls on women and children”. (KII, Male, 45) “The public water supply is consistently unreliable, and the available water is unclean. We have no choice but to use this poor-quality water. The government supports foreign private companies in selling water, but we can’t afford bottled water, so we are forced to drink the unclean water”. (FGD, Mother, 34) |
| Corruption in administration | “The canal’s width is narrow, and powerful individuals illegally divert water by creating cuts due to corruption in the irrigation department. As a result, the water level at the tail end is reduced, leaving insufficient water for crops”. (KII, Male, 57) | |
| Displacement as a last resort | “People often have to migrate when the water supply runs out. During their journey, they frequently become homeless and lack access to food, water, and toilets”. (FGD, Male, 53) | |
| Water fetching and gender vulnerabilities | Stigmas and harassment | “People may provide water, but they demand something difficult in return. Harassment and even rape are common occurrences while fetching water. (KII, Female, 53) |
| Fetching water difficulties | “Fetching water is exhausting; it takes children and women an hour, and in the summer, it becomes even greater challenge”. (FGD, Mother, 27) | |
| Fights and injuries | “Fetching water results in health problems, injuries, and conflicts”. | |
| Water scarcity, WASH and IYCF | Feeding requires safe water | “Dirty and muddy water often makes our young children sick and contaminates our food. Doctors recommend mineral water from private companies for sick children, but it is too expensive for most poor and rural mothers to afford”. (FGD, Female, 26) |
| Fetching affects breastfeeding behaviors | “During the summer months of June, July, and August, the water situation causes significant stress for mothers, leading to increased maternal stress. Consequently, infants suffer due to reduced breastfeeding”. (FGD, Female, 19) | |
| Water-food nexus | Low agricultural production | “We can’t grow crops during water shortages, which causes our lands to dry up. As hunger increases, we are forced to sell our land at low prices and migrate to earn money for survival”. (KII, Female, 53) |
| Less milk production | “Our cattle have stopped producing milk due to a lack of food. When our livestock drink less water, their milk production decreases significantly”. (FGD, Male, 40) |
| Themes | Sub-Themes | Narratives |
|---|---|---|
| Diet quality vs. quantity | Daily diet or staple food | “The government historically supported profitable crops like tobacco, sugar, cotton, and wheat, which significantly reduced the cultivation of fruits and vegetables”. (KII, 45) “While a variety of items are available in the market, wheat remains the staple diet for most people here. The poor mainly eat wheat bread with a mixture of mint, green chili, and onion”. (KII, 38) |
| Inflation reduces buying capacity | “Inflation has made our lives very difficult; we dilute a liter of milk with water to stretch its quantity. Meat and fruit are rare in our diet because they are too expensive. Everyone seems worried and mentally stressed due to the rampant inflation”. (FGD, Mother, 34) | |
| Preferred vs. disliked food | Unable to make choices freely | “Highly marginalized household domestic workers often collect expired or leftover food from the homes where they work. To manage the smell, we heat the food because we can’t afford to buy fresh items”. (IDI, Domestic household servant, 29) |
| Food availability and accessibility | Selling domestic food items to earn a little money | “Poor rural people often sell milk, eggs, or chickens in the local market to earn a little money, but their children often go hungry. They are compelled to sell these items, especially when they are ill or need money for medical treatment. One day at the market, I saw two young children selling a chicken. I asked how much they were selling it for, and the older boy said ‘400 rupees.’ After I paid and took the chicken, the younger child began to cry. I asked him why he was crying, and his older brother said, ‘There is nothing.’ I was puzzled and asked the older brother to explain. The older boy tearfully revealed that the chicken belonged to his younger brother, who had also eaten its eggs. They were selling it out of necessity because their mother was very sick, and they needed the money for her treatment. The younger brother was distressed because he didn’t want to part with the chicken he loved”. (KII, Journalist) |
| Food diversity | Limited food variety and hidden hunger | “Poor mothers and their children can only fill their stomachs with potatoes, peas, and wheat. A diverse and nutritious diet is also crucial”. (KII, Nutrition expert from the community) |
| All is good for the poor | “Only the names of desirable foods can be mentioned, but they cannot be eaten. For the poor and hungry, anything that is available and accessible is acceptable”. (IDI, Mother, 33) | |
| Reliability of food and governance | Commercialization of low-quality junk food | “In the past, people were healthier and happier, free from many diseases. Now, everything is becoming expensive and of poor quality due to a lack of regulation. Milk, medicine, cooking oil—everything is substandard, and there is no one to enforce price and quality controls”. (IDI, Local traditional pharmacist) |
| Themes | Sub-Themes | Narratives |
|---|---|---|
| Global impact of private sector and formula milk companies on countries | Formula milk companies hunt for clients in healthcare settings | “Multinational formula milk representatives are allowed to operate in healthcare centers and promote formula milk to parents of malnourished children. After children recover from SAM with the use of formula 75 or 100 and then Ready-to-Use Therapeutic Food (RUTF), mothers are encouraged by doctors and these representatives to continue using their products”. (KII, Nutrition Stabilization Center staff) |
| Formula milk companies ‘control over the government | “The deliberate lack of oversight or restrictions on the free movement of formula milk company representatives in hospitals indicates a strong influence of these companies over government institutions and bureaucracy”. (KII) | |
| Baby food industry advertisement | “The baby food industry frequently misleads and deceives parents about their products. They use labeling to enhance their messaging and boost sales, but restrictions are seldom imposed”. (KII) | |
| Pakistan Medical Association promotes MNCs | “On what basis is the Pakistan Medical Association running advertisements against open milk? Is it driven by public concern or the funding from multinational companies (MNCs)? Poor farmers sell cow or buffalo milk to these companies at low rates (50–60 rupees), which is then processed into products. In the village, we used to consume open milk and everyone was healthy. The government should investigate these ads and uncover the hidden interests behind them, with the support of the Punjab Food Authority, to ensure transparency and ease in the delivery of open milk”. (KII, journalist) | |
| Formula milk companies in alliance with the medical community | “Although legislation exists to restrict formula milk, companies bribe medical doctors to promote their products. As of now, a federal board and provincial sub-committees to oversee this issue have not yet been established”. (KII, Health Official) | |
| Barriers to nutrition-specific and sensitive programs | Lack of a sustainable nutrition policy | Historically, the country has lacked a consistent nutrition policy. Policies have frequently shifted, ranging from food distribution and card-based rationing to cash transfers like BISP, and programs such as Safe Motherhood, CMAM, EPI, MNCH, School Health and Nutrition Program, Tawana Pakistan Project, Sasti Roti Scheme, and the recent “No One Sleeps Hungry” initiative. Each government introduces its policies and programs, highlighting the need for a sustainable and consistent approach”. (KII, Nutrition expert) |
| Social exclusion of people with low social capital and bureaucratic red-tapism | “Poor and low-caste women often face challenges accessing health and therapeutic programs, while those who are better-off benefit more easily due to their connections with staff and influential figures. To become beneficiaries of the BISP cash program, some women who were missing documentation went to file a complaint but were stopped by the police at the gate. Those who managed to enter the office were shuffled from one department to another, with staff telling them, ‘I can’t help you; go talk to someone else’ or ‘I don’t have time, come back next month.’ The process is exhausting and frustrating, with the poor having to navigate bureaucratic hurdles for years, while the wealthy can get assistance in just minutes”. (IDI, Widow enrolled in BISP Program) | |
| Sociocultural factors, inadequate care, maternal illiteracy, high fertility, and time poverty | “Poverty, traditional gender roles, social stigma against contraception, preference for male children, and side effects of modern contraceptives are key factors contributing to high fertility rates. Frequent pregnancies and inadequate healthcare lead to maternal malnutrition. The demands of economic activities, caring for the husband and his family, domestic chores, and working in agricultural fields significantly burden mothers”. (KII, Population Officer) | |
| Inadequate funding deprioritizes nutrition by health bureaucracy | “The CMAM program has become less effective as a significant portion of funds are diverted to other public programs, such as the polio eradication initiative. The coverage of nutrition-related projects is limited due to insufficient budgetary allocations”. (KII, Nutrition Coordinator) | |
| Insufficient allocation of resources and a shortage of healthcare staff in remote areas | “In South Punjab, a marginalized and underdeveloped region with low literacy rates, structural issues hinder female health workers from filling their designated roles in remote health units. In Southern Punjab, less than half of the Basic Health Units have successfully appointed Lady Health Workers (LHWs) to fill vacancies. For instance, the Rajanpur District Health Information System reported that out of 900 LHW positions, only 650 were filled, leaving 250 positions still vacant”. (KII, Health Official) | |
| Absenteeism and engaging health workers in non-nutrition programs | “In several remote areas, LHWs are frequently absent. Their excessive involvement in other tasks has led to the deprioritization of nutrition activities within the health department. The workload for LHWs should be reduced, and maternal-child health and nutrition should be given a higher priority on their agenda”. (KII, Healthcare Provider) | |
| Geographical constraints | “Nutritional aid delivery is frequently limited due to logistical challenges faced by rural and marginalized communities”. | |
| Other stakeholders’ performance | “Many female school teachers and NGO staff were involved in misusing and selling food that was intended for distribution among girls in rural public schools”. (IDI, Mother, 40) | |
| Left against medical advice (LAMA) cases | “Most cases of SAM were from poor, geographically isolated, and flood-affected areas. Children with SAM were admitted to the Nutrition Stabilization Center for treatment with antibiotics and formula milk 75 or 100 until they recovered. Poor mothers, fathers, or grandmothers often had to stay at the center to care for their severely ill and malnourished children. However, many of them eventually abandoned the treatment because they needed to care for other children at home”. (KII, Nutrition stabilization center staff) | |
| Weak system of data management, monitoring, corruption, | “The system for collecting, monitoring, and evaluating data is weak, making strategic planning difficult. Corruption and unethical sales of therapeutic food require monitoring and fair distribution. These issues hinder the effective implementation of nutrition programs”. (KII, Senior Health Official) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, F.; Malik, N.I.; Bashir, S.; Noureen, N.; Ahmad, J.B.; Tang, K. Political Economy of Maternal Child Malnutrition: Experiences about Water, Food, and Nutrition Policies in Pakistan. Nutrients 2024, 16, 2642. https://doi.org/10.3390/nu16162642
Ahmed F, Malik NI, Bashir S, Noureen N, Ahmad JB, Tang K. Political Economy of Maternal Child Malnutrition: Experiences about Water, Food, and Nutrition Policies in Pakistan. Nutrients. 2024; 16(16):2642. https://doi.org/10.3390/nu16162642
Chicago/Turabian StyleAhmed, Farooq, Najma Iqbal Malik, Shamshad Bashir, Nazia Noureen, Jam Bilal Ahmad, and Kun Tang. 2024. "Political Economy of Maternal Child Malnutrition: Experiences about Water, Food, and Nutrition Policies in Pakistan" Nutrients 16, no. 16: 2642. https://doi.org/10.3390/nu16162642
APA StyleAhmed, F., Malik, N. I., Bashir, S., Noureen, N., Ahmad, J. B., & Tang, K. (2024). Political Economy of Maternal Child Malnutrition: Experiences about Water, Food, and Nutrition Policies in Pakistan. Nutrients, 16(16), 2642. https://doi.org/10.3390/nu16162642