

The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet and Metabolites in Chronic Kidney Disease

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
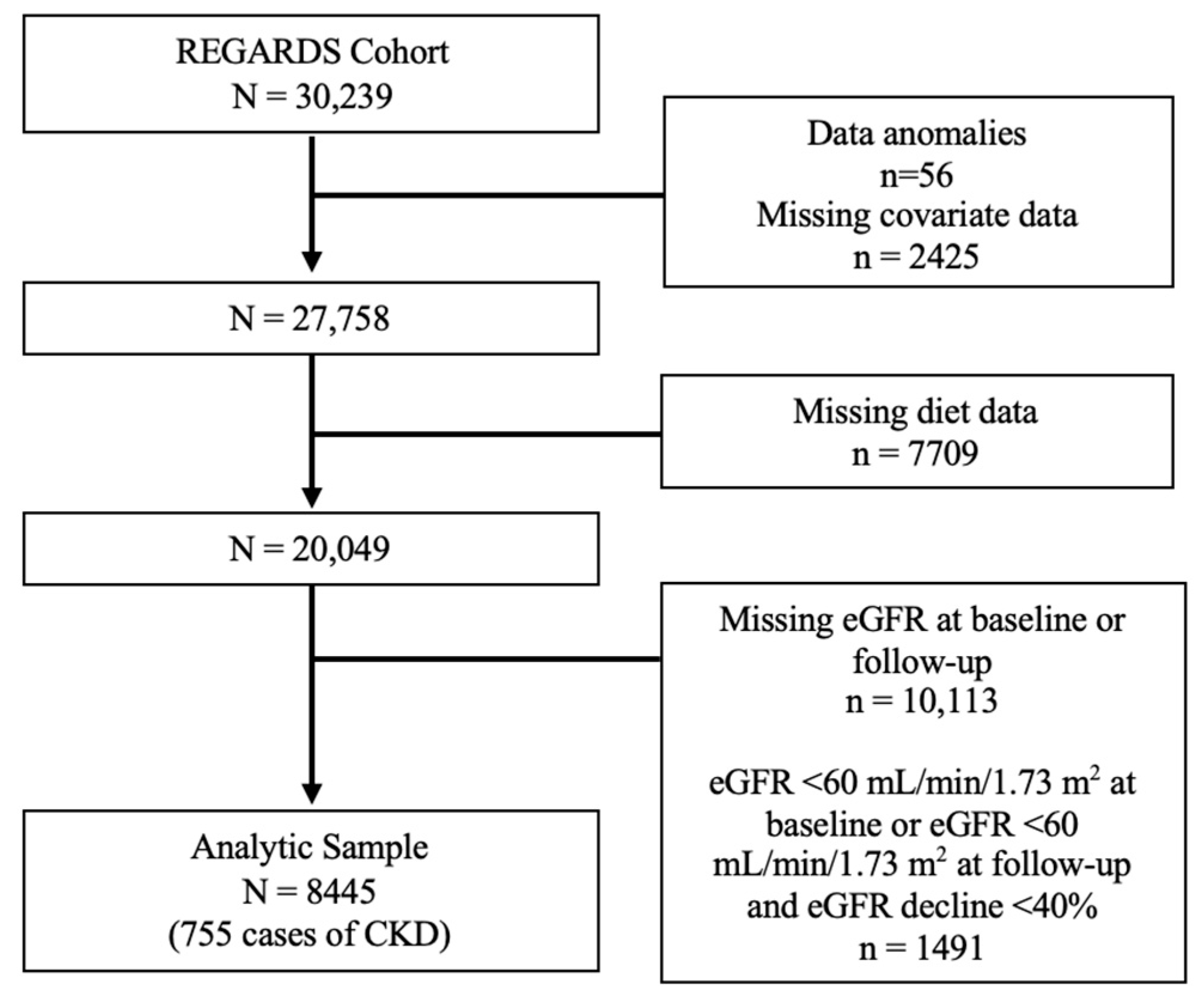
2.1. Study Population
2.2. MIND Diet
2.3. Outcome Definition
2.4. Metabolomics
2.5. Covariates
2.6. Statistical Analyses
3. Results
3.1. Characteristics of Participants
3.2. The MIND Diet and CKD
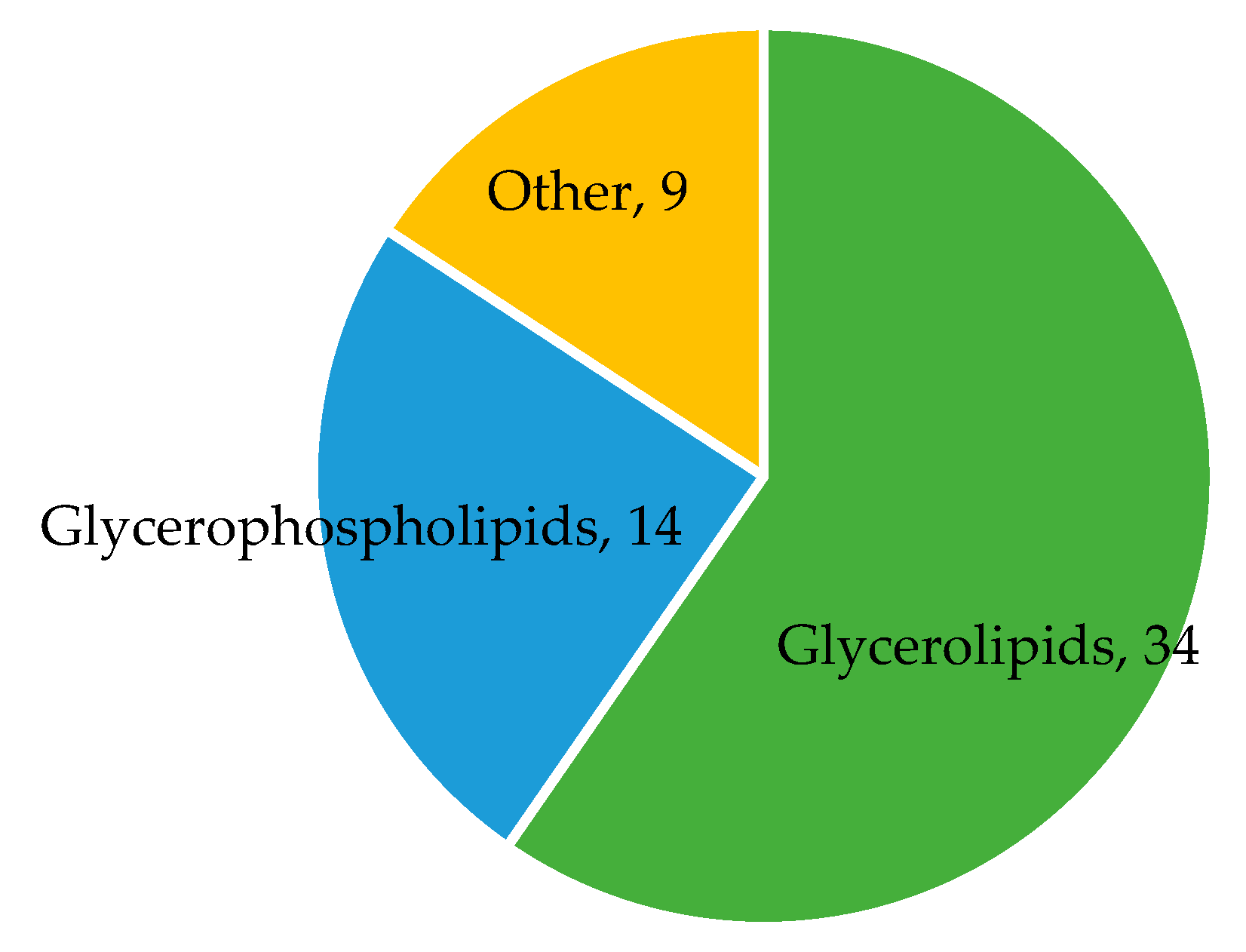
3.3. Metabolites Associated with the MIND Diet
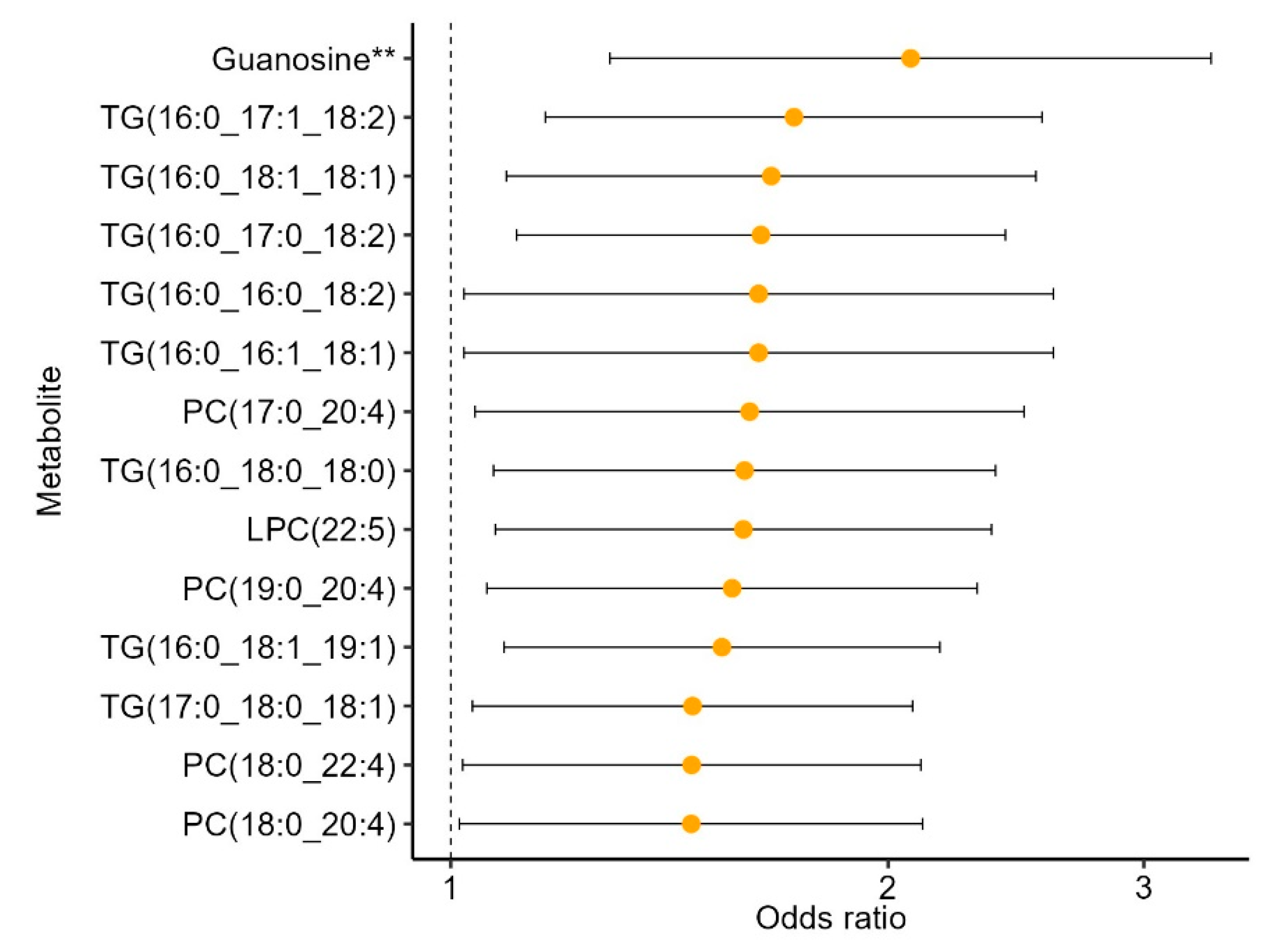
3.4. MIND-Metabolites Associated with CKD
3.5. Mediation Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Barnes, L.L.; Bennett, D.A.; Aggarwal, N.T. MIND diet slows cognitive decline with aging. Alzheimer’s Dement. 2015, 11, 1015–1022. [Google Scholar] [CrossRef]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimer’s Dement. 2015, 11, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Ascherio, A.; Grodstein, F. Fruit and vegetable consumption and cognitive decline in aging women. Ann. Neurol. 2005, 57, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Evans, D.A.; Tangney, C.C.; Bienias, J.L.; Wilson, R.S. Associations of vegetable and fruit consumption with age-related cognitive change. Neurology 2006, 67, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef] [PubMed]
- Psaltopoulou, T.; Naska, A.; Orfanos, P.; Trichopoulos, D.; Mountokalakis, T.; Trichopoulou, A. Olive oil, the Mediterranean diet, and arterial blood pressure: The Greek European Prospective Investigation into Cancer and Nutrition (EPIC) study. Am. J. Clin. Nutr. 2004, 80, 1012–1018. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R., 3rd; Simons-Morton, D.G.; et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef]
- Filippou, C.D.; Tsioufis, C.P.; Thomopoulos, C.G.; Mihas, C.C.; Dimitriadis, K.S.; Sotiropoulou, L.I.; Chrysochoou, C.A.; Nihoyannopoulos, P.I.; Tousoulis, D.M. Dietary Approaches to Stop Hypertension (DASH) Diet and Blood Pressure Reduction in Adults with and without Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 1150–1160. [Google Scholar] [CrossRef]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef]
- Rebholz, C.M.; Crews, D.C.; Grams, M.E.; Steffen, L.M.; Levey, A.S.; Miller, E.R., 3rd; Appel, L.J.; Coresh, J. DASH (Dietary Approaches to Stop Hypertension) Diet and Risk of Subsequent Kidney Disease. Am. J. Kidney Dis. 2016, 68, 853–861. [Google Scholar] [CrossRef]
- Chrysohoou, C.; Panagiotakos, D.B.; Pitsavos, C.; Skoumas, J.; Zeimbekis, A.; Kastorini, C.M.; Stefanadis, C. Adherence to the Mediterranean diet is associated with renal function among healthy adults: The ATTICA study. J. Ren. Nutr. 2010, 20, 176–184. [Google Scholar] [CrossRef]
- Razmpoosh, E.; Moslehi, N.; Abdollahi, S.; Soltani, S.; Mirmiran, P.; Azizi, F. The Mediterranean, DASH, and MIND diets and the incident of hypertension over a median follow-up of 7.4 years in the Tehran Lipid and Glucose Study. BMC Public Health 2022, 22, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chrysohoou, C.; Panagiotakos, D.B.; Pitsavos, C.; Das, U.N.; Stefanadis, C. Adherence to the Mediterranean diet attenuates inflammation and coagulation process in healthy adults: The ATTICA Study. J. Am. Coll. Cardiol. 2004, 44, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Golzarand, M.; Mirmiran, P.; Azizi, F. Adherence to the MIND diet and the risk of cardiovascular disease in adults: A cohort study. Food Funct. 2022, 13, 1651–1658. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Chang, Z.G.; Jia, L.; Song, W.; Wang, H.; Dong, Q.; Dou, K. Better adherence to the MIND diet is associated with lower risk of all-cause death and cardiovascular death in patients with atherosclerotic cardiovascular disease or stroke: A cohort study from NHANES analysis. Food Funct. 2023, 14, 1740–1749. [Google Scholar] [CrossRef]
- Bhave, V.M.; Ament, Z.; Patki, A.; Gao, Y.; Kijpaisalratana, N.; Guo, B.; Chaudhary, N.S.; Guarniz, A.L.G.; Gerszten, R.; Correa, A.; et al. Plasma Metabolites Link Dietary Patterns to Stroke Risk. Ann. Neurol. 2022, 93, 500–510. [Google Scholar] [CrossRef]
- Li, J.; Guasch-Ferré, M.; Chung, W.; Ruiz-Canela, M.; Toledo, E.; Corella, D.; Bhupathiraju, S.N.; Tobias, D.K.; Tabung, F.K.; Hu, J.; et al. The Mediterranean diet, plasma metabolome, and cardiovascular disease risk. Eur. Heart J. 2020, 41, 2645–2656. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.H.; Kraus, W.E.; Newgard, C.B. Metabolomic profiling for the identification of novel biomarkers and mechanisms related to common cardiovascular diseases: Form and function. Circulation 2012, 126, 1110–1120. [Google Scholar] [CrossRef]
- Rhee, E.P. A Systems-Level View of Renal Metabolomics. Semin. Nephrol. 2018, 38, 142–150. [Google Scholar] [CrossRef]
- Howard, V.J.; Cushman, M.; Pulley, L.; Gomez, C.R.; Go, R.C.; Prineas, R.J.; Graham, A.; Moy, C.S.; Howard, G. The reasons for geographic and racial differences in stroke study: Objectives and design. Neuroepidemiology 2005, 25, 135–143. [Google Scholar] [CrossRef]
- Howard, V.J.; Kleindorfer, D.O.; Judd, S.E.; McClure, L.A.; Safford, M.M.; Rhodes, J.D.; Cushman, M.; Moy, C.S.; Soliman, E.Z.; Kissela, B.M.; et al. Disparities in stroke incidence contributing to disparities in stroke mortality. Ann. Neurol. 2011, 69, 619–627. [Google Scholar] [CrossRef]
- Gillett, S.R.; Boyle, R.H.; Zakai, N.A.; McClure, L.A.; Jenny, N.S.; Cushman, M. Validating laboratory results in a national observational cohort study without field centers: The Reasons for Geographic and Racial Differences in Stroke cohort. Clin. Biochem. 2014, 47, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Cushman, M.; Judd, S.E.; Howard, V.J.; Kissela, B.; Gutiérrez, O.M.; Jenny, N.S.; Ahmed, A.; Thacker, E.L.; Zakai, N.A. N-Terminal Pro–B-type Natriuretic Peptide and Stroke Risk. Stroke 2014, 45, 1646–1650. [Google Scholar] [CrossRef] [PubMed]
- Olson, N.C.; Cushman, M.; Judd, S.E.; Kissela, B.M.; Safford, M.M.; Howard, G.; Zakai, N.A. Associations of coagulation factors IX and XI levels with incident coronary heart disease and ischemic stroke: The REGARDS study. J. Thromb. Haemost. 2017, 15, 1086–1094. [Google Scholar] [CrossRef] [PubMed]
- Block, G.; Woods, M.; Potosky, A.; Clifford, C. Validation of a self-administered diet history questionnaire using multiple diet records. J. Clin. Epidemiol. 1990, 43, 1327–1335. [Google Scholar] [CrossRef]
- Judd, S.E.; Letter, A.J.; Shikany, J.M.; Roth, D.L.; Newby, P.K. Dietary Patterns Derived Using Exploratory and Confirmatory Factor Analysis are Stable and Generalizable Across Race, Region, and Gender Subgroups in the REGARDS Study. Front. Nutr. 2014, 1, 29. [Google Scholar] [CrossRef]
- Cheung, K.L.; Crews, D.C.; Cushman, M.; Yuan, Y.; Wilkinson, K.; Long, D.L.; Judd, S.E.; Shlipak, M.G.; Ix, J.H.; Bullen, A.L.; et al. Risk Factors for Incident CKD in Black and White Americans: The REGARDS Study. Am. J. Kidney Dis. 2023, 82, 11–21.e11. [Google Scholar] [CrossRef]
- Kurella Tamura, M.; Wadley, V.; Yaffe, K.; McClure, L.A.; Howard, G.; Go, R.; Allman, R.M.; Warnock, D.G.; McClellan, W. Kidney function and cognitive impairment in US adults: The Reasons for Geographic and Racial Differences in Stroke (REGARDS) Study. Am. J. Kidney Dis. 2008, 52, 227–234. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C–Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- Ament, Z.; Bevers, M.B.; Wolcott, Z.; Kimberly, W.T.; Acharjee, A. Uric Acid and Gluconic Acid as Predictors of Hyperglycemia and Cytotoxic Injury after Stroke. Transl. Stroke Res. 2021, 12, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Ament, Z.; Patki, A.; Chaudhary, N.; Bhave, V.M.; Garcia Guarniz, A.L.; Gao, Y.; Gerszten, R.E.; Correa, A.; Judd, S.E.; Cushman, M.; et al. Nucleosides Associated With Incident Ischemic Stroke in the REGARDS and JHS Cohorts. Neurology 2022, 98, e2097–e2107. [Google Scholar] [CrossRef]
- Ament, Z.; Patki, A.; Bhave, V.M.; Kijpaisalratana, N.; Jones, A.C.; Couch, C.A.; Stanton, R.J.; Rist, P.M.; Cushman, M.; Judd, S.E.; et al. Omega-3 Fatty Acids and Risk of Ischemic Stroke in REGARDS. Transl. Stroke Res. 2024. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Ji, L. Adjusting multiple testing in multilocus analyses using the eigenvalues of a correlation matrix. Heredity 2005, 95, 221–227. [Google Scholar] [CrossRef]
- Stevens, P.E.; Levin, A. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef]
- Chen, G.C.; Neelakantan, N.; Martin-Calvo, N.; Koh, W.P.; Yuan, J.M.; Bonaccio, M.; Iacoviello, L.; Martinez-Gonzalez, M.A.; Qin, L.Q.; van Dam, R.M. Adherence to the Mediterranean diet and risk of stroke and stroke subtypes. Eur. J. Epidemiol. 2019, 34, 337–349. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Lowe, G.D.; Rumley, A.; Bruckdorfer, K.R.; Whincup, P.H. Associations of vitamin C status, fruit and vegetable intakes, and markers of inflammation and hemostasis. Am. J. Clin. Nutr. 2006, 83, 567–574. [Google Scholar] [CrossRef]
- Nettleton, J.A.; Steffen, L.M.; Mayer-Davis, E.J.; Jenny, N.S.; Jiang, R.; Herrington, D.M.; Jacobs, D.R., Jr. Dietary patterns are associated with biochemical markers of inflammation and endothelial activation in the Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Clin. Nutr. 2006, 83, 1369–1379. [Google Scholar] [CrossRef]
- Du, S.; Kim, H.; Crews, D.C.; White, K.; Rebholz, C.M. Association Between Ultraprocessed Food Consumption and Risk of Incident CKD: A Prospective Cohort Study. Am. J. Kidney Dis. 2022, 80, 589–598.e1. [Google Scholar] [CrossRef]
- Sanvictores, T.; Chauhan, S. Vitamin B5 (Pantothenic Acid). In StatPearls; StatPearls Publishing Copyright © 2024; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2024. [Google Scholar]
- Peron, G.; Meroño, T.; Gargari, G.; Hidalgo-Liberona, N.; Miñarro, A.; Lozano, E.V.; Castellano-Escuder, P.; González-Domínguez, R.; Del Bo, C.; Bernardi, S.; et al. A Polyphenol-Rich Diet Increases the Gut Microbiota Metabolite Indole 3-Propionic Acid in Older Adults with Preserved Kidney Function. Mol. Nutr. Food Res. 2022, 66, e2100349. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.J.; Miller, E.R.; Jee, S.H.; Stolzenberg-Solomon, R.; Lin, P.-H.; Erlinger, T.; Nadeau, M.R.; Selhub, J. Effect of Dietary Patterns on Serum Homocysteine. Circulation 2000, 102, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Ottosson, F.; Ericson, U.; Almgren, P.; Smith, E.; Brunkwall, L.; Hellstrand, S.; Nilsson, P.M.; Orho-Melander, M.; Fernandez, C.; Melander, O. Dimethylguanidino Valerate: A Lifestyle-Related Metabolite Associated With Future Coronary Artery Disease and Cardiovascular Mortality. J. Am. Heart Assoc. 2019, 8, e012846. [Google Scholar] [CrossRef] [PubMed]
- Rohatgi, N.; Nielsen, T.K.; Bjørn, S.P.; Axelsson, I.; Paglia, G.; Voldborg, B.G.; Palsson, B.O.; Rolfsson, Ó. Biochemical Characterization of Human Gluconokinase and the Proposed Metabolic Impact of Gluconic Acid as Determined by Constraint Based Metabolic Network Analysis. PLoS ONE 2014, 9, e98760. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, K.; Aoyagi, Y.; Fukuuchi, T.; Inazawa, K.; Yamaoka, N. Total purine and purine base content of common foodstuffs for facilitating nutritional therapy for gout and hyperuricemia. Biol. Pharm. Bull. 2014, 37, 709–721. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Bulló, M.; Babio, N.; Martínez-González, M.A.; Estruch, R.; Covas, M.I.; Wärnberg, J.; Arós, F.; Lapetra, J.; Serra-Majem, L.; et al. Mediterranean diet and risk of hyperuricemia in elderly participants at high cardiovascular risk. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1263–1270. [Google Scholar] [CrossRef]
- Gao, Y.; Cui, L.F.; Sun, Y.Y.; Yang, W.H.; Wang, J.R.; Wu, S.L.; Gao, X. Adherence to the Dietary Approaches to Stop Hypertension Diet and Hyperuricemia: A Cross-Sectional Study. Arthritis Care Res. 2021, 73, 603–611. [Google Scholar] [CrossRef]
- Zhou, M.; Huang, X.; Li, R.; Zhang, Z.; Zhang, L.; Gao, X.; Yang, H.; Ma, Y. Association of dietary patterns with blood uric acid concentration and hyperuricemia in northern Chinese adults. Nutr. J. 2022, 21, 42. [Google Scholar] [CrossRef]
- Broadus, A.E.; Kaminsky, N.I.; Hardman, J.G.; Sutherland, E.W.; Liddle, G.W. Kinetic parameters and renal clearances of plasma adenosine 3′,5′-monophosphate and guanosine 3′,5′-monophosphate in man. J. Clin. Investig. 1970, 49, 2222–2236. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Q1 (Lowest Consumption) (N = 2112) | Q2 (N = 2111) | Q3 (N = 2111) | Q4 (Greatest Consumption) (N = 2111) |
|---|---|---|---|---|
| MIND diet score | 5.08 ± 0.8 | 6.7 ± 0.4 | 8.0 ± 0.4 | 9.8 ± 0.8 |
| Age, years | 61.4 ± 8.1 | 62.0 ± 8.0 | 62.4 ± 7.9 | 63.0 ± 7.9 |
| Female sex | 1063 (50.3) | 1168 (55.3) | 1288 (61.0) | 1411 (66.8) |
| Black race | 774 (36.7) | 653 (30.9) | 576 (27.3) | 500 (23.7) |
| Education | ||||
| • Less than HS | 212 (10.0) | 113 (5.4) | 87 (4.1) | 78 (3.7) |
| • HS graduate | 644 (30.5) | 495 (23.5) | 405 (19.2) | 342 (16.2) |
| • Some college | 599 (28.4) | 583 (27.6) | 573 (27.1) | 482 (22.8) |
| • College graduate and above | 657 (31.1) | 920 (43.6) | 1046 (49.6) | 1209 (57.3) |
| Income | ||||
| • <USD 20,000 | 323 (15.3) | 235 (11.1) | 193 (9.1) | 144 (6.8) |
| • USD 20,000–USD 34,999 | 522 (24.7) | 464 (22.0) | 410 (19.4) | 388 (18.4) |
| • USD 35,000–USD 74,999 | 698 (33.1) | 720 (34.1) | 755 (35.8) | 730 (34.6) |
| • ≥USD 75,000 | 364 (17.2) | 481 (22.8) | 532 (25.2) | 616 (29.2) |
| • Refused | 205 (9.7) | 211 (10.0) | 221 (10.5) | 233 (11.0) |
| Region | ||||
| • Belt/buckle | 1296 (61.4) | 1257 (59.6) | 1144 (54.2) | 1061 (50.3) |
| • Non-belt/buckle | 816 (38.6) | 854 (40.5) | 967 (45.8) | 1050 (49.7) |
| Alcohol Use | ||||
| • None | 1308 (61.9) | 1179 (55.9) | 1099 (52.1) | 992 (47.0) |
| • Moderate | 701 (33.2) | 833 (39.5) | 900 (42.6) | 1006 (47.7) |
| • Heavy | 103 (4.9) | 99 (4.7) | 112 (5.3) | 113 (5.4) |
| Current Smoker | 367 (17.4) | 245 (11.6) | 205 (9.7) | 105 (5.0) |
| Physical Activity | ||||
| • None | 745 (35.3) | 629 (29.8) | 534 (25.3) | 428 (20.3) |
| • Some | 1367 (64.7) | 1482 (70.2) | 1577 (74.7) | 1683 (79.7) |
| BMI, kg/m2 | 29.7 ± 6.0 | 29.2 ± 5.8 | 28.7 ± 5.7 | 27.7 ± 5.6 |
| Diabetes | 339 (16.1) | 317 (15.0) | 251 (11.9) | 226 (10.7) |
| Hypertension | 1486 (70.4) | 1425 (67.5) | 1373 (65.0) | 1283 (60.8) |
| eGFR, mL/min/1.73 m2 | 100.9 ± 21.1 | 102.4 ± 21.9 | 104.1 ± 21.6 | 106.4 ± 26.2 |
| ACR, mg/g | 6.2 [4.0–11.1] | 6.2 [4.2–11.0] | 6.3 [4.3–10.6] | 6.2 [4.3–10.7] |
| Model | RR (95% CI) | p-Value |
|---|---|---|
| Model 1 | 0.85 (0.82, 0.88) | 4.46 × 10−18 |
| Model 2 | 0.87 (0.84, 0.90) | 4.74 × 10−13 |
| Model 3 | 0.90 (0.86, 0.94) | 2.03 × 10−7 |
| OR Total Effect | OR Natural Direct Effect | OR Natural Indirect Effect | p-Value For Indirect Effect | |
|---|---|---|---|---|
| Model 1 | 0.87 [0.74, 1.00] | 0.94 [0.79, 1.08] | 0.93 [0.89, 0.97] | 0.001 |
| Model 2 | 0.86 [0.72, 1.00] | 0.93 [0.78, 1.08] | 0.93 [0.88, 0.97] | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Couch, C.A.; Ament, Z.; Patki, A.; Kijpaisalratana, N.; Bhave, V.; Jones, A.C.; Armstrong, N.D.; Cheung, K.L.; Kimberly, W.T.; Tiwari, H.K.; et al. The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet and Metabolites in Chronic Kidney Disease. Nutrients 2024, 16, 2458. https://doi.org/10.3390/nu16152458
Couch CA, Ament Z, Patki A, Kijpaisalratana N, Bhave V, Jones AC, Armstrong ND, Cheung KL, Kimberly WT, Tiwari HK, et al. The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet and Metabolites in Chronic Kidney Disease. Nutrients. 2024; 16(15):2458. https://doi.org/10.3390/nu16152458
Chicago/Turabian StyleCouch, Catharine A., Zsuzsanna Ament, Amit Patki, Naruchorn Kijpaisalratana, Varun Bhave, Alana C. Jones, Nicole D. Armstrong, Katharine L. Cheung, W. Taylor Kimberly, Hemant K. Tiwari, and et al. 2024. "The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet and Metabolites in Chronic Kidney Disease" Nutrients 16, no. 15: 2458. https://doi.org/10.3390/nu16152458
APA StyleCouch, C. A., Ament, Z., Patki, A., Kijpaisalratana, N., Bhave, V., Jones, A. C., Armstrong, N. D., Cheung, K. L., Kimberly, W. T., Tiwari, H. K., & Irvin, M. R. (2024). The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet and Metabolites in Chronic Kidney Disease. Nutrients, 16(15), 2458. https://doi.org/10.3390/nu16152458