
The Role of Artificial Intelligence in Nutrition Research: A Scoping Review

 , ,
, , 
Abstract
1. Introduction
1.1. Defining Artificial Intelligence

{kind=link}
{kind=link}
{kind=link}
| Artificial Narrow Intelligence (ANI) [21] | Artificial General Intelligence (AGI) [21] | Artificial Super Intelligence (ASI) [21] | |||
|---|---|---|---|---|---|
|
|
| |||
|
|
| |||
|
|
| |||
|
| ||||
| Branches of artificial intelligence | |||||
| Natural Language Processing (NLP) [25,26,27,28,29] | Machine Learning (ML) [30,31,32,33] | Deep Learning (DL) [34,35,36,37,38] | Generic Algorithm (GA) [39] | Generative Pre-trained Transformer (GPT) [24,40,41,42] | Latent Dirichlet Allocation (LDA) [43] |
|
|
|
|
|
|
1.2. Applications of Artificial Intelligence
2. Materials and Methods
Quality Assessment
3. Results
3.1. Description of the Included Studies
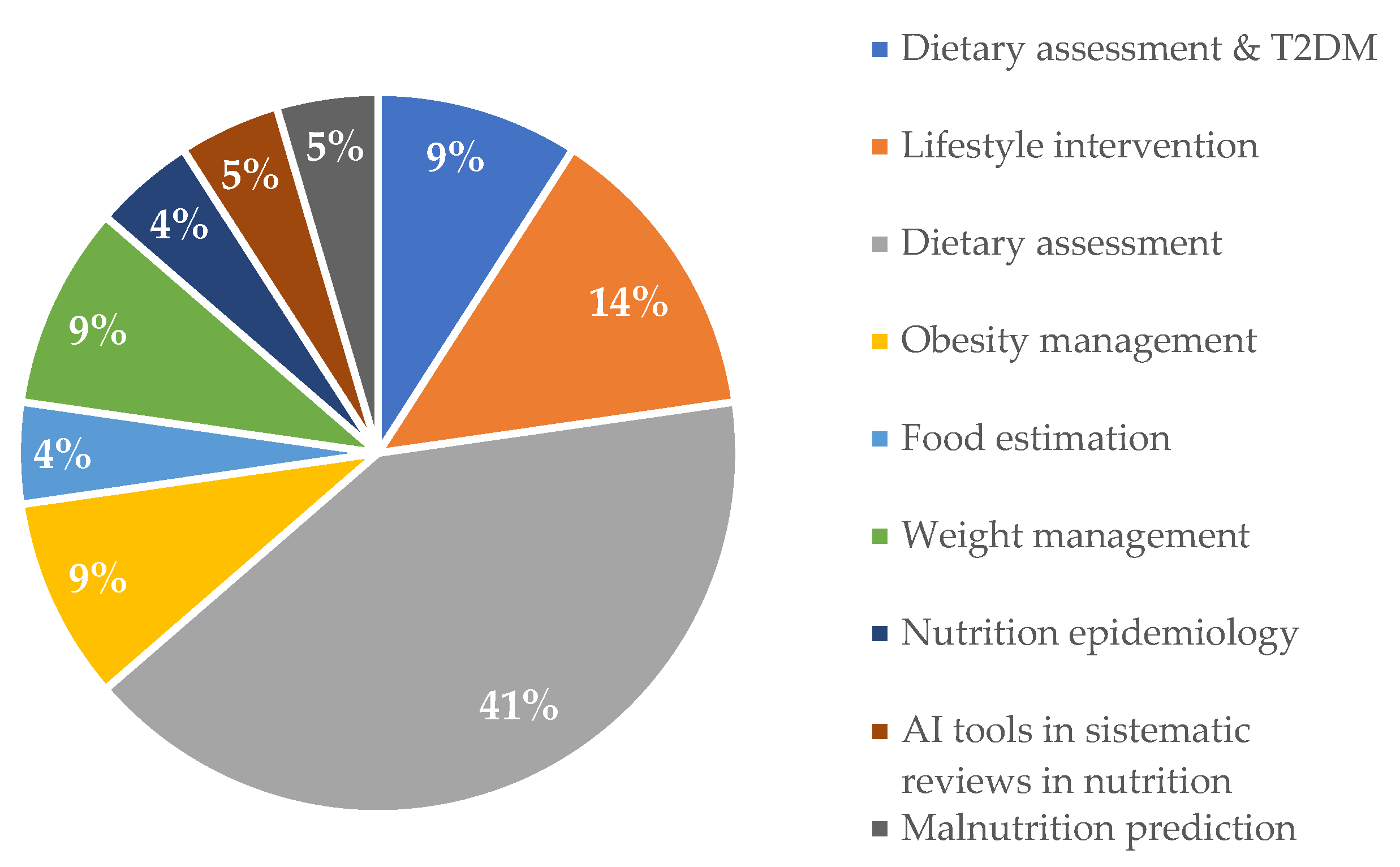
3.2. Applications of AI in Nutrition
3.3. Overview of the Studies
| Five Descriptive Studies (22.73%) [24,30,32,40,44] | Nine ObservationalStudies (40.9%) [31,33,34,35,36,38,39,42,51] | Two Pilot Studies (9.09%) [26,50] | Two SystematicReviews (9.09%) [28,43] | Four Mixed Studies (18.19%) [25,27,29,41] |
|---|---|---|---|---|
|
|
|
|
|
3.4. Testing Stage and Type of AI Used
| Lead Author, Year & Country | Aim & Topic | Study Characteristics | Findings | Limitations | Type of AI | Area in Nutrition | Observations |
|---|---|---|---|---|---|---|---|
| Maharjan, B. (2019) USA [25] | The use and development of an AI tool that is culturally adapted for Native Americans with low computer/technological skills to support diabetes management using people’s voice. |
| Preliminary results showed that Alexa was able to accurately count calories and provide nutrition education. Having the potential to improve health among the target population by recommending meals using ADA’s guidelines. | AI has to learn the needs of the specific target populations to culturally adapt it to other specific groups. | NLP | Dietary assessment for patients with T2DM. | Health improvements, validation and patient’s satisfaction using this technology is yet to be determined. |
| Davis, C.R. (2020) Australia [26] | To evaluate the performance of AI health assistance, and to verify participants’ adherence to physical activity, diet and their engagement |
| Paola (the virtual health-assistant) was successful in behavior change. However, she could not answer questions beyond what she was trained for. | The sample size of the study was too small. Due to data loss, other questions (not related to what AI was trained in) could not be evaluated. Men are underrepresented; thus, the results cannot be generalized. The platform used to launch Paola had issues with 10 min time-outs | NLP | Lifestyle intervention | Paola also provided educational videos and different recipes. Users had weekly exchanges with her for data entry and to obtain her feedback based on their entry |
| Maher, C.A. (2020) Australia [27] | To test the recruitment and retention of a physical activity program that was also based on a Mediterranean diet. The program was delivered by an AI virtual health coach. |
| The virtual-health assistant (Paola) successfully delivered a lifestyle intervention program helping to lose weight and to increase participant’s physical activity. AI virtual coach has room for improvement regarding its connection to people in terms of emotions. | The study was not randomized and the follow up was limited | NLP | Lifestyle intervention | Participants showed enthusiasm using a virtual-health coach. This technology may be used in other nutrition areas, such as weight loss or diabetes management |
| Oh, Y. (2021) USA [28] | To assess the characteristics of chatbots in terms of conversation and function, and to investigate if chatbots interventions were successful in lifestyle changes (healthy eating, exercise, weight control) and health-related outcomes. |
| Chatbots have the potential to change lifestyle and improve access and effectiveness to personalized nutrition. | Sample sizes used by the studies were too small; thus, it is difficult to draw conclusions on employment of chatbots to deliver lifestyle changing programs. | NLP | Lifestyle intervention | Studies did not evaluate side-effects nor the possible harm that users may encounter when using them. Chatbots should be used with caution, and conversations should be monitored to avoid harmful effects. |
| Beyeler, M. (2023) Switzerland [29] | To evaluate the usage of a health bot (HB) and how it is perceived by patients receiving bariatric treatment. |
| The health bot (HB) was assessed by its response to nutrition-related questions. HB was well accepted among patients, and they found it easy to use and understand. Participants had access to useful information through the HB. However, concerns about the replacements of dietitians, personal information and the privacy of the questions were brought up by the participants. | The sample size of the study was too small. AI used for dietary assessment should not be used without supervision of a healthcare professional due to the potential misinterpretation of the HB answers. HB may exclude people with no or limited access to digital resources, and limited literacy. Making an HB easy to use should be considered. | NLP | Dietary assessment | The HB was not meant to replace consultation; instead, it was meant to be used between consultations with a dietitian. |
| Limketkai, B.N. (2021) USA [30] | A review of new technologies (apps, wearable devices, and AI remote nutrition assessment) and their integration in clinical nutrition and patient care. |
| AI-based apps and wearables devices are used by clinicians since they can be used for diet optimization and to find eating patterns, given their real-time data collection. Smartwatches (e.g., Apple watch, Kardia band) have been approved by the FDA for some health uses, shifting from wellness devices to a more medical focus. | Wearable devices are still being developed, as algorithms cannot fully differentiate between different type of foods, portions, and backgrounds. Some technologies that measure body composition have not been tested in clinical trials; thus, the accuracy of the results needs to be assessed. | ML | Dietary assessment | Some apps that offer measurements such as sleeping patterns and heart rate require a monthly subscription and a smartphone. These emerging technologies in clinical nutrition are still in their infancy and need further investigation. There is concern about the information generated and its use in medical decision making. |
| Morgenstern, J.D. (2022) Canada [31] | To create a machine learning prediction model, and to evaluate its efficacy in examining the connection between food intake and CVD risk. |
| The most significant nutritional variables linked to CVD were caffeine, alcohol, supplements and sodium. Without the need of lab tests and anthropometric measurements. | Nutritional variables were used, employing one-time 24 h recall. A larger data set with more frequent dietary assessment is needed. A separate model for dietary variables vs. non-dietary variables is needed to confirm dietary information for CVD prediction. | ML | Nutrition epidemiology | No lab tests and anthropometric variables were used in ML models. |
| Murumkar, A. (2023) India [32] | To develop an AI-based dietician that acts like a real dietitian. It offers diets and diet plans focused on the individual. |
| Feeding AI with appropriate information, such as BMI, allergies, food preferences, physical activity, and type of job; AI has the potential to suggest eating plans according to the user’s need without having to pay for it. | The user will be uploading information (height, weight, allergies, etc.) which is self-reported. | ML | Dietary assessment | No dietitian intervention is encouraged. |
| Fujihara, K. (2023) Japan [33] | To build, develop and evaluate the ability of a ML model to predict variations in body weight over a 3-year period from medical examinations. |
| The system was able to develop 5 different formulas for body weight change prediction over a 3-year span. It successfully identified lifestyle factors that modified body weight. It has the potential to be used in weight management. | The model may not be generalizable because it was developed using a particular ethnic group. Diet and physical activity information used to build the system was self-reported. Environmental and socioeconomic factors were not considered. | ML | Weight management | 5-year data were used to develop the model. Data for 50,000 individuals were used to train the model and 5000 to test it. |
| Yang, Z. (2021) China [34] | To mimic a dietician’s mental process using AI for food size estimation. |
| This technology can be applied to wearable devices for real food volume estimation. | It was assumed that the food on a plate can easily be detected from a real-world image that also contains other things (e.g., table, background of the picture). It relies on high-quality object detection to crop the food plate from image. The volume estimation was limited with the plate having only one type of food; whereas in real life, a plate of food has more than one item. | DL | Food estimation. | Current data sets are designed for food recognition, but not for food volume (portion size) estimation. |
| Taylor, S. (2021) China [35] | To develop an AI-based app to map foods on national (U.S) databases, for calories counting vs. a recommended method. |
| National databases combined with an intelligent app using NLP; can estimate energy intake with no significant difference when compared to the 24HR, which is considered the gold standard for dietary intake. This may be used for weight management. Although participants had the option to speak to the COCO nutritionist to enter their dietary intake; they preferred to type their entries. | COCO nutritionist has limited features (it does not include food photography). The 24 h recall was used; food intake may not reflect complete dietary consumption because it is self-reported. The sample size for preliminary data is small. | DL | Weight management and dietary assessment. | MIT reviewed COCO nutritionist’s data without having access to the 24 h recall. 24 h recall was analyzed using a food processor. |
| Papathanail, I. (2021) Switzerland [36] | To develop and evaluate an AI system that uses input images for energy and macronutrient intake before and after patient’s consumption. |
| The system’s estimation of macronutrients intake performed better than the control (nursing staff and a medical student) in the hospital. The system provides better estimation for individual meal components. AI provides results almost instantly | Meals were not weighted; dietitians and the medical student visually estimated food percentage. | DL | Dietary assessment | This system may be used to prevent malnutrition by monitoring diet among hospitalized older patients |
| Chen, X. (2021) USA [50] | To assess restaurant nutrition at a big scale by using crowdsourcing food images and to develop a restaurant nutrition index (quality of food offered by the restaurant based on calories). |
| DL used the restaurants’ pictures to determine the quality (calorie-based) of their food. Restaurants offering foods with higher calories were found in areas with limited food access and less healthy food retailers. These results may be used in food environment inequality assessment. | The model could not identify pictures with several food items on the same plate—it was able to estimate only one; it could not identify portion sizes derived from the images. Some foods were not accurately identified. Results cannot be generalized to other geographical areas because crowdsourcing images were from food review websites from a particular area. Restaurants with no online presence were excluded. Young adults were most of the raters, and this might have influenced the type of foods that were reviewed. | DL | Dietary assessment and food environment detection | This tool is not meant to replace current dietary assessment methods, it should be used as a complementary tool only. |
| Van Wymelbeke-Delannoy, V. (2022) France [38] | To assess food consumption using an AI system that does not need human interaction to determine food leftovers in a hospital setting. |
| The FoodIntech project was demonstrated to be useful in picture gathering and estimating patient’s food intake by analyzing food leftovers in a hospital setting, providing instant results. With enough pictures the system can learn to recognize new foods. | The camera vision is limited; thus a 100% performance will not be achieved. AI struggles with certain food containers. Thus, food segmentation is hard to achieve. Trained staff are needed to take pictures with good resolution, lighting and clarity, for adequate dietary assessment. | DL | Dietary assessment | Food Intech was evaluated in a hospital setting, but it was not tested with the hospital’s patients. This might allow to determine whether the patient’s food intake and other factors, such as age, gender, and weight, are related to food intake. |
| Jin, B.T. (2022) USA [51] | To evaluate the ability of a malnutrition prediction model using longitudinal patient records. |
| DL is accurate in malnutrition prediction by using patients’ longitudinal data. AI used 3 visits instead of using only the patient’s last visit information for prediction. Neither lab tests nor anthropometric measures are used in this model; (less data collection) was needed, relying only on its capacity of predictive diagnosis. | Patients with minimal records or no records were excluded. This may represent bias towards populations at higher risk. | DL | Malnutrition prediction | This model may be incorporated into current healthcare using demographic and diagnostic data. However, this model still needs to undergo clinical validation. |
| Sefa-Yeboah, S.M. (2021) Ghana [39] | To develop a mobile app for obesity management working both on mobile and on the web; providing personalized meal plans to meet people’s macronutrients and calories needs. |
| AI engine can be used for meals recommendation, and prediction to meet calorie intake for obesity management. It estimates energy intake by selecting the foods from the food record. It also shows how many calories are left to meet the calorie goal. | The system’s overall effectiveness is impacted by the limited method used to assess physical activity, which does not allow to estimate energy expenditure. Additionally, the system is limited to food selection for dietary intake. | GA | Obesity management | This system can also be useful for training those who are in the dietetics field. |
| Niszczota, P. (2023) Poland [40] | To assess the performance of ChatGPT on diet generation by investigating the precision and safety of 56 diets generated by ChatGPT. |
| ChatGPT can generate menus, but it is not always safe; it included allergens for a fictitious allergic woman. It also provided wrong calculations for portion sizes, and it could not provide varied menus, repeating the same food items. This study was carried out in Europe and sometimes the measurements were provided in American units. ChatGPT may mislead people with its dietary suggestions. However, it followed recommendations from different dietary guidelines. | This study used only one prompt (one interaction) instead of a series of interactions. Big language models cannot identify when they are providing wrong information. | GPT | Dietary assessment | Results show that AI can also be misused and needs human interaction to verify that the information provided is correct. In some countries (e.g., Italy) ChatGPT had limited access. |
| Arslan, S. (2023) Turkey [41] | ChatGPT’s potential for treating and managing obesity. Based on the patient’s progress and records, ChatGPT may modify its recommendations. |
| ChatGPT can offer personalized advice such as weight control, physical activity and nutrition and meet individual’s needs. Based on the patient’s progress, recommendations for weight management can be adjusted. | AI’s information might be biased, depending on the type of data that were used to train it. AI-systems do not have emotional intelligence like a human and do not offer emotional support. When GPT provides harmful and inaccurate information, it is not clear who is to blame and who is responsible. | GPT | Obesity management | AI in healthcare must be used with caution and ethical issues must be addressed, since AI systems operate without ethical and professional standards. |
| Sun, H. (2023) China [42] | To develop and validate an AI-nutritionist focused on T2DM. |
| ChatGPT and GPT4 are competent to answer the Chinese Register Dietitian Exam and medical nutrition-related questions. It also identified food using pictures. Endocrinologists’ knowledge regarding nutrition might not be reliable. AI has potential to provide dietary assessment and meet the lack of dietitians in China. | The model was presented only with a limited set of questions that a patient may ask. One of AI’s limitations in the training process is that it can provide several answers for the same question; hence, focusing on specific questions might help to obtain more trustworthy responses. | GPT | Dietary assessment for people with T2DM | The model was not tested, nor has a pilot study been conducted. When testing is performed, the authors recommend reviewing the AI-nutritionist’s answers by a human within 48 h span to ensure no harmful/wrong information is provided to the patient, allowing this to be fixed. |
| Chatelan, A. (2023)Not specified [24] | To provide a guide regarding the potential hazards and benefits of using ChatGPT in clinical, academic and public health contexts. |
| Using ChatGPT has both opportunities and risks. It might be beneficial for people to obtain educational material for free (healthy eating, nutrition). However, ChatGPT is not always accurate and might provide harmful responses. Therefore, it should be supervised. Chatbots do not have soft skills, making it harder to replace RDs. | ChatGPT might provide nutritional advice and diets, nonetheless. It cannot provide emotional and psychological support. ChatGPT does not cite the information sources it uses to provide answers; making it hard to determine whether the sources are factual or not. | GPT | Dietary assessment | ChatGPT trainings are limited. It is not aware of information that happens thereafter (it was last trained in January 2022). Given the quick evolution of chatbots, its potential uses are hard to define. |
| Nunes-Galbez, N. (2022) Brazil [43] | To evaluate AI tools for conducting systematic reviews in the nutrition field |
| The publication dates range from 2015 to 2021. All the retrieved publications are from developed countries. The small number of studies shows that AI is still novel in systematic reviews in nutrition. | The studies that did not address any challenges could be useful when considering the use of these technologies. The review was limited by the number of studies that were included. | LDA | Use of AI tools in systematic reviews in nutrition. | Big data has resulted in an exponential growth in scientific papers. It is hard for scientists to conduct a systematic review without losing data. In consequence, the use of AI has been proposed. |
| Bond, A. (2023) UK [44] | To identify areas and applications in nutrition where AI might play a role. |
| AI can be used to enhance healthcare by interpreting images, making prescriptions, and to provide nutritional advice. In a hospital setting, patients can benefit from these technologies instead of waiting for the dietitian. Other uses in healthcare are expected to be developed. | AI might be biased since it is trained by humans. Thus, training AI should be performed with caution. If not trained properly, AI might face opposition within healthcare. Ethical concerns and how AI deals with personal information are still complex. | DL, ML, NLP | Dietary assessment | Not losing control of AI and how it is used in healthcare is of extreme importance. Healthcare personnel should understand how to use AI |
4. Discussion
4.1. Dietary Assessment
4.2. Dietary Adherence
4.3. Ethical Issues
4.4. Implications for Research
4.5. Limitations
4.6. Recommnedations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vitolins, M.Z.; Case, T.L. What Makes Nutrition Research So Difficult to Conduct and Interpret? Diabetes Spectr. 2020, 33, 113–117. [Google Scholar] [CrossRef]
- Thomas, D.M.; Kleinberg, S.; Brown, A.W.; Crow, M.; Bastian, N.D.; Reisweber, N.; Lasater, R.; Kendall, T.; Shafto, P.; Blaine, R.; et al. Machine learning modeling practices to support the principles of AI and ethics in nutrition research. Nutr. Diabetes 2022, 12, 48. [Google Scholar] [CrossRef] [PubMed]
- American Society for Nutrition. Available online: https://nutrition.org/public-affairs/nutrition-research-agenda/ (accessed on 8 March 2024).
- Kirk, D.; Kok, E.; Tufano, M.; Tekinerdogan, B.; Feskens, E.J.M.; Camps, G. Machine Learning in Nutrition Research. Adv. Nutr. 2022, 13, 2573–2589. [Google Scholar] [CrossRef] [PubMed]
- Côté, M.; Lamarche, B. Artificial intelligence in nutrition research: Perspectives on current and future applications. Appl. Physiol. Nutr. Metab. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Salinari, A.; Machì, M.; Armas Diaz, Y.; Cianciosi, D.; Qi, Z.; Yang, B.; Ferreiro Cotorruelo, M.S.; Villar, S.G.; Dzul Lopez, L.A.; Battino, M.; et al. The Application of Digital Technologies and Artificial Intelligence in Healthcare: An Overview on Nutrition Assessment. Diseases 2023, 11, 97. [Google Scholar] [CrossRef]
- Nutritional Cancer Institute. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/nutritionist (accessed on 9 March 2024).
- Nutritional Cancer Institute. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/dietitian (accessed on 8 March 2024).
- Kelly, J.T.; Collins, P.F.; McCamley, J.; Ball, L.; Roberts, S.; Campbell, K.L. Digital disruption of dietetics: Are we ready? J. Hum. Nutr. Diet. 2021, 34, 134–146. [Google Scholar] [CrossRef]
- Wahl, B.; Cossy-Gantner, A.; Germann, S.; Schwalbe, N.R. Artificial intelligence (AI) and global health: How can AI contribute to health in resource-poor settings? BMJ Glob. Health 2018, 3, e000798. [Google Scholar] [CrossRef] [PubMed]
- Watkins, B.; Odallo, L.; Yu, J. Artificial intelligence for the practical assessment of nutritional status in emergencies. Expert Syst. 2024, 41, e13550. [Google Scholar] [CrossRef]
- Zuhair, V.; Babar, A.; Ali, R.; Oduoye, M.O.; Noor, Z.; Chris, K.; Okon, I.I.; Rehman, L.U. Exploring the Impact of Artificial Intelligence on Global Health and Enhancing Healthcare in Developing Nations. J. Prim. Care Community Health 2024, 15, 21501319241245847. [Google Scholar] [CrossRef]
- Haenlein, M.; Kaplan, A. A Brief History of Artificial Intelligence: On the Past, Present, and Future of Artificial Intelligence. Calif. Manag. Rev. 2019, 61, 5–14. [Google Scholar] [CrossRef]
- Abbass, H. Editorial: What is Artificial Intelligence? IEEE Trans. Artif. Intell. 2021, 2, 94–95. [Google Scholar] [CrossRef]
- McCarthy, J. What Is Artificial Intelligence? Available online: https://www-formal.stanford.edu/jmc/whatisai.pdf (accessed on 10 December 2023).
- Muthukrishnan, N.; Maleki, F.; Ovens, K.; Reinhold, C.; Forghani, B.; Forghani, R. Brief History of Artificial Intelligence. Neuroimaging Clin. N. Am. 2020, 30, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Jarrahi, M.H.; Lutz, C.; Newlands, G. Artificial intelligence, human intelligence and hybrid intelligence based on mutual augmentation. Big Data Soc. 2022, 9. [Google Scholar] [CrossRef]
- Martinez, R. Artificial intelligence: Distinguishing between types & definitions. Nev. Law J. 2019, 19, 9. [Google Scholar]
- Kureshi, R. Artificial Intellligence: How Is It Different from Human Intelligence. Available online: https://online.hull.ac.uk/blog/what-is-artificial-intelligence-and-how-is-it-different-from-human-intelligence#:~:text=While%20artificial%20intelligence%20includes%20technologies,creativity%2C%20perception%2C%20and%20memory (accessed on 10 December 2022).
- Korteling, J.E.; van de Boer-Visschedijk, G.C.; Blankendaal, R.A.M.; Boonekamp, R.C.; Eikelboom, A.R. Human- versus Artificial Intelligence. Front. Artif. Intell. 2021, 4, 622364. [Google Scholar] [CrossRef]
- Moranding-Ahuerma, F. What is Artifiticial Intelligence? Int. J. Res. Publ. Rev. 2022, 3, 1947–1951. [Google Scholar] [CrossRef]
- Wang, P. On defining artificial intelligence. J. Artif. Gen. Intell. 2019, 10, 1–37. [Google Scholar] [CrossRef]
- Lu, Y. Artificial intelligence: A survey on evolution, models, applications and future trends. J. Manag. Anal. 2019, 6, 1–29. [Google Scholar] [CrossRef]
- Chatelan, A.; Clerc, A.; Fonta, P.A. ChatGPT and Future Artificial Intelligence Chatbots: What may be the Influence on Credentialed Nutrition and Dietetics Practitioners? J. Acad. Nutr. Diet 2023, 123, 1525–1531. [Google Scholar] [CrossRef]
- Maharjan, B.; Li, J.; Kong, J.; Tao, C. Alexa, What Should I Eat?: A Personalized Virtual Nutrition Coach for Native American Diabetes Patients Using Amazon’s Smart Speaker Technology. In Proceedings of the 2019 IEEE International Conference on E-Health Networking, Application & Services (HealthCom), Bogota, Colombia, 14–16 October 2019; pp. 1–6. [Google Scholar]
- Davis, C.R.; Murphy, K.J.; Curtis, R.G.; Maher, C.A. A Process Evaluation Examining the Performance, Adherence, and Acceptability of a Physical Activity and Diet Artificial Intelligence Virtual Health Assistant. Int. J. Environ. Res. Public Health 2020, 17, 9137. [Google Scholar] [CrossRef]
- Maher, C.A.; Davis, C.R.; Curtis, R.G.; Short, C.E.; Murphy, K.J. A Physical Activity and Diet Program Delivered by Artificially Intelligent Virtual Health Coach: Proof-of-Concept Study. JMIR Mhealth Uhealth 2020, 8, e17558. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.J.; Zhang, J.; Fang, M.L.; Fukuoka, Y. A systematic review of artificial intelligence chatbots for promoting physical activity, healthy diet, and weight loss. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 160. [Google Scholar] [CrossRef] [PubMed]
- Beyeler, M.; Légeret, C.; Kiwitz, F.; van der Horst, K. Usability and Overall Perception of a Health Bot for Nutrition-Related Questions for Patients Receiving Bariatric Care: Mixed Methods Study. JMIR Hum. Factors 2023, 10, e47913. [Google Scholar] [CrossRef] [PubMed]
- Limketkai, B.N.; Mauldin, K.; Manitius, N.; Jalilian, L.; Salonen, B.R. The Age of Artificial Intelligence: Use of Digital Technology in Clinical Nutrition. Curr. Surg. Rep. 2021, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, J.D.; Rosella, L.C.; Costa, A.P.; Anderson, L.N. Development of machine learning prediction models to explore nutrients predictive of cardiovascular disease using Canadian linked population-based data. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2022, 47, 529–546. [Google Scholar] [CrossRef] [PubMed]
- Murumkar, A.D.; Singh, A.; Chachar, B.R.; Bagade, P.D.; Zaware, G. Artificial Intelligence (AI) based Nutrition Advisorusing an App. In Proceedings of the 2023 International Conference on Sustainable Computing and Smart Systems (ICSCSS), Coimbatore, India, 14–16 June 2023; pp. 586–590. [Google Scholar]
- Fujihara, K.; Yamada Harada, M.; Horikawa, C.; Iwanaga, M.; Tanaka, H.; Nomura, H.; Sui, Y.; Tanabe, K.; Yamada, T.; Kodama, S.; et al. Machine learning approach to predict body weight in adults. Front. Public Health 2023, 11, 1090146. [Google Scholar] [CrossRef]
- Yang, Z.; Yu, H.; Cao, S.; Xu, Q.; Yuan, D.; Zhang, H.; Jia, W.; Mao, Z.H.; Sun, M. Human-Mimetic Estimation of Food Volume from a Single-View RGB Image Using an AI System. Electronics 2021, 10, 1556. [Google Scholar] [CrossRef]
- Taylor, S.; Korpusik, M.; Das, S.; Gilhooly, C.; Simpson, R.; Glass, J.; Roberts, S. Use of Natural Spoken Language with Automated Mapping of Self-reported Food Intake to Food Composition Data for Low-Burden Real-time Dietary Assessment: Method Comparison Study. J. Med. Internet Res. 2021, 23, e26988. [Google Scholar] [CrossRef]
- Papathanail, I.; Brühlmann, J.; Vasiloglou, M.F.; Stathopoulou, T.; Exadaktylos, A.K.; Stanga, Z.; Münzer, T.; Mougiakakou, S. Evaluation of a Novel Artificial Intelligence System to Monitor and Assess Energy and Macronutrient Intake in Hospitalised Older Patients. Nutrients 2021, 13, 4539. [Google Scholar] [CrossRef]
- Chen, A.M.H.; Draime, J.A.; Berman, S.; Gardner, J.; Krauss, Z.; Martinez, J. Food as medicine? Exploring the impact of providing healthy foods on adherence and clinical and economic outcomes. Explor. Res. Clin. Soc. Pharm. 2022, 5, 100129. [Google Scholar] [CrossRef]
- Van Wymelbeke-Delannoy, V.; Juhel, C.; Bole, H.; Sow, A.-K.; Guyot, C.; Belbaghdadi, F.; Brousse, O.; Paindavoine, M. A Cross-Sectional Reproducibility Study of a Standard Camera Sensor Using Artificial Intelligence to Assess Food Items: The FoodIntech Project. Nutrients 2022, 14, 221. [Google Scholar] [CrossRef] [PubMed]
- Sefa-Yeboah, S.M.; Osei Annor, K.; Koomson, V.J.; Saalia, F.K.; Steiner-Asiedu, M.; Mills, G.A. Development of a Mobile Application Platform for Self-Management of Obesity Using Artificial Intelligence Techniques. Int. J. Telemed. Appl. 2021, 2021, 6624057. [Google Scholar] [CrossRef] [PubMed]
- Niszczota, P.; Rybicka, I. The credibility of dietary advice formulated by ChatGPT: Robo-diets for people with food allergies. Nutrition 2023, 112, 112076. [Google Scholar] [CrossRef] [PubMed]
- Arslan, S. Exploring the Potential of Chat GPT in Personalized Obesity Treatment. Ann. Biomed. Eng. 2023, 51, 1887–1888. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Zhang, K.; Lan, W.; Gu, Q.; Jiang, G.; Yang, X.; Qin, W.; Han, D. An AI Dietitian for Type 2 Diabetes Mellitus Management Based on Large Language and Image Recognition Models: Preclinical Concept Validation Study. J. Med. Internet Res. 2023, 25, e51300. [Google Scholar] [CrossRef] [PubMed]
- Nunes-Galbes, N.M. Systematic Reviews in Nutrition Using Artificial Intelligence Tools: A Brief Review; Faculty of Public Health, University of São Paulo: São Paulo, Brazil, 2022. [Google Scholar]
- Bond, A.; Mccay, K.; Lal, S. Artificial intelligence & clinical nutrition: What the future might have in store. Clin. Nutr. ESPEN 2023, 57, 542–549. [Google Scholar]
- Tang, X. The role of artificial intelligence in medical imaging research. BJR Open 2020, 2, 20190031. [Google Scholar] [CrossRef]
- An, R.; Wang, X. Artificial Intelligence Applications to Public Health Nutrition. Nutrients 2023, 15, 4285. [Google Scholar] [CrossRef]
- Sak, J.; Suchodolska, M. Artificial Intelligence in Nutrients Science Research: A Review. Nutrients 2021, 13, 322. [Google Scholar] [CrossRef]
- Kitchenham, K.; Brereton, O.P.; Budnen, D.; Tumer, M.; Bailey, J.; Linkmam, S. Systematic literature reviews in software engineering—A systematic literature review. Inf. Softw. Technol. 2009, 51, 7–15. [Google Scholar] [CrossRef]
- The World Bank. Available online: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html (accessed on 21 March 2024).
- Chen, X.; Johnson, E.; Kulkarni, A.; Ding, C.; Ranelli, N.; Chen, Y.; Xu, R. An Exploratory Approach to Deriving Nutrition Information of Restaurant Food from Crowdsourced Food Images: Case Hartford. Nutrients 2021, 13, 4132. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.T.; Choi, M.H.; Moyer, M.F.; Kim, D.A. Redicting malnutrition from longitudinal patient trajectories with deep learning. PLoS ONE 2022, 17, e0271487. [Google Scholar] [CrossRef] [PubMed]
- Narkhede, S. Understanding auc-roc curve. Towards Data Sci. 2018, 26, 220–227. [Google Scholar]
- Joiner, I.A. Chapter 1—Artificial Intelligence: AI is Nearby. In Emerging Library Technologies; Joiner, I.A., Ed.; Chandos Publishing: Witney, UK, 2018; pp. 1–22. [Google Scholar]
- Roper, J.; Lin, M.H.; Rong, Y. Extensive upfront validation and testing are needed prior to the clinical implementation of AI-based auto-segmentation tools. J. Appl. Clin. Med. Phys. 2023, 24, e13873. [Google Scholar] [CrossRef] [PubMed]
- Kwok, C.S.; Muntean, E.-A.; Mallen, C.D.; Borovac, J.A. Data Collection Theory in Healthcare Research: The Minimum Dataset in Quantitative Studies. Clin. Pract. 2022, 12, 832–844. [Google Scholar] [CrossRef]
- Western Michigan University. Facing the Future: Artificial Intellligence Is Evolving at War Speed-But at What Cost? 2023. Available online: https://wmich.edu/news/2023/05/71771 (accessed on 16 January 2024).
- Larburu, N.; Artola, G.; Kerexeta, J.; Caballero, M.; Ollo, B.; Lando, C.M. Key Factors and AI-Based Risk Prediction of Malnutrition in Hospitalized Older Women. Geriatrics 2022, 7, 105. [Google Scholar] [CrossRef]
- Folson, G.K.; Bannerman, B.; Atadze, V.; Ador, G.; Kolt, B.; McCloskey, P.; Gangupantulu, R.; Arrieta, A.; Braga, B.C.; Arsenault, J.; et al. Validation of Mobile Artificial Intelligence Technology-Assisted Dietary Assessment Tool Against Weighed Records and 24-Hour Recall in Adolescent Females in Ghana. J. Nutr. 2023, 153, 2328–2338. [Google Scholar] [CrossRef] [PubMed]
- Tahir, G.A.; Loo, C.K. A Comprehensive Survey of Image-Based Food Recognition and Volume Estimation Methods for Dietary Assessment. Healthcare 2021, 9, 1676. [Google Scholar] [CrossRef]
- Konstantakopoulos, F.S.; Georga, E.I.; Fotiadis, D.I. A Review of Image-Based Food Recognition and Volume Estimation Artificial Intelligence Systems. IEEE Rev. Biomed. Eng. 2024, 17, 136–152. [Google Scholar] [CrossRef]
- Gibson, A.A.; Sainsbury, A. Strategies to Improve Adherence to Dietary Weight Loss Interventions in Research and Real-World Settings. Behav. Sci. 2017, 7, 44. [Google Scholar] [CrossRef]
- Babel, A.; Taneja, R.; Mondello Malvestiti, F.; Monaco, A.; Donde, S. Artificial Intelligence Solutions to Increase Medication Adherence in Patients with Non-communicable Diseases. Front. Digit. Health 2021, 3, 669869. [Google Scholar] [CrossRef] [PubMed]
- Al-Salmi, N.; Cook, P.; D’Souza, M.S. Diet Adherence among Adults with Type 2 Diabetes Mellitus: A Concept Analysis. Oman Med. J. 2022, 37, e361. [Google Scholar] [CrossRef] [PubMed]
- Kumar, H.; Martin, A. Artificial Emotional Intelligence: Conventional and deep learning approach. Expert Syst. Appl. 2023, 212, 118651. [Google Scholar] [CrossRef]
- Glauberman, G.; Ito-Fujita, A.; Katz, S.; Callahan, J. Artificial Intelligence in Nursing Education: Opportunities and Challenges. Hawaii J. Health Soc. Welf. 2023, 82, 302–305. [Google Scholar] [PubMed]
- World Health Organization. Ethics and Governance of Artificial Intelligence for Health 2021. Available online: https://www.who.int/publications/i/item/9789240029200 (accessed on 19 June 2023).
- Morley, J.; Murphy, L.; Mishra, A.; Joshi, I.; Karpathakis, K. Governing Data and Artificial Intelligence for Health Care: Developing an International Understanding. JMIR Form Res. 2022, 6, e31623. [Google Scholar] [CrossRef] [PubMed]
- Shanklin, R.; Samorani, M.; Harris, S.; Santoro, M.A. Ethical Redress of Racial Inequities in AI: Lessons from Decoupling Machine Learning from Optimization in Medical Appointment Scheduling. Philos. Technol. 2022, 35, 96. [Google Scholar] [CrossRef] [PubMed]
- Detopoulou, P.; Voulgaridou, G.; Moschos, P.; Levidi, D.; Anastasiou, T.; Dedes, V.; Diplari, E.-M.; Fourfouri, N.; Giaginis, C.; Panoutsopoulos, G.I.; et al. Artificial intelligence, nutrition, and ethical issues: A mini-review. Clin. Nutr. Open Sci. 2023, 50, 46–56. [Google Scholar] [CrossRef]
- Makhortykh, M.; Urman, A.; Ulloa, R. Detecting Race and Gender Bias in Visual Representation of AI on Web Search Engines. In Proceedings of the Second International Workshop on Algorithmic Bias in Search and Recommendation, BIAS 2021, Lucca, Italy, 1 April 2021; pp. 36–50. [Google Scholar]
- International Bussiness Machines Corporation. What Is Overfitting. Available online: https://www.ibm.com/topics/overfitting?mhsrc=ibmsearch_a&mhq=what%20is%20overfitting (accessed on 24 January 2024).
- Liu, F.; Panagiotakos, D. Real-world data: A brief review of the methods, applications, challenges and opportunities. BMC Med. Res. Methodol. 2022, 22, 287. [Google Scholar] [CrossRef]
- Alonso, A.; Siracuse, J.J. Protecting patient safety and privacy in the era of artificial intelligence. Semin. Vasc. Surg. 2023, 36, 426–429. [Google Scholar] [CrossRef]
- University of Michigan-Dearborn. AI’s Mysterious “Black Box” Problme, Explained. 2023. Available online: https://umdearborn.edu/news/ais-mysterious-black-box-problem-explained (accessed on 8 January 2023).


| Research Question | What Is the Role of AI in Nutrition Research? | |
|---|---|---|
| Inclusion Criteria | Exclusion Criteria | |
| Population | Studies involved in the human nutrition field, areas within the nutrition field. | Studies involved in any other areas that were not related to human nutrition. |
| Intervention | Studies where AI was used, applied, or implemented in nutrition, or where AI played a main role or was a key part of the research with impact in human nutrition and/or nutrition research. | Studies that did not use AI in their research, studies where AI did not play a main role nor was a key part of the research. Studies that did not focus on human nutrition. |
| Comparison | Not set | None |
| Outcome | AI’s impact in human nutrition, contribution in nutrition research, influence on decision making in nutrition, recommendation of AI’s implementation in nutrition research, prediction of nutritional status, dietary intake, and diet recommendations, how AI is being used in nutrition research. | Studies that did not use AI for human nutrition, studies reporting only AI’s algorithm without emphasizing the use of AI in nutrition. |
| Study Design | Not set | None |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sosa-Holwerda, A.; Park, O.-H.; Albracht-Schulte, K.; Niraula, S.; Thompson, L.; Oldewage-Theron, W. The Role of Artificial Intelligence in Nutrition Research: A Scoping Review. Nutrients 2024, 16, 2066. https://doi.org/10.3390/nu16132066
Sosa-Holwerda A, Park O-H, Albracht-Schulte K, Niraula S, Thompson L, Oldewage-Theron W. The Role of Artificial Intelligence in Nutrition Research: A Scoping Review. Nutrients. 2024; 16(13):2066. https://doi.org/10.3390/nu16132066
Chicago/Turabian StyleSosa-Holwerda, Andrea, Oak-Hee Park, Kembra Albracht-Schulte, Surya Niraula, Leslie Thompson, and Wilna Oldewage-Theron. 2024. "The Role of Artificial Intelligence in Nutrition Research: A Scoping Review" Nutrients 16, no. 13: 2066. https://doi.org/10.3390/nu16132066
APA StyleSosa-Holwerda, A., Park, O.-H., Albracht-Schulte, K., Niraula, S., Thompson, L., & Oldewage-Theron, W. (2024). The Role of Artificial Intelligence in Nutrition Research: A Scoping Review. Nutrients, 16(13), 2066. https://doi.org/10.3390/nu16132066