
Morphofunctional Assessment beyond Malnutrition: Fat Mass Assessment in Adult Patients with Phenylketonuria—Systematic Review
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Selection Criteria
2.2. Search Strategy, Study Selection, and Data Collecction
2.3. Assessment of Risk of Bias in Individual Studies
3. Results
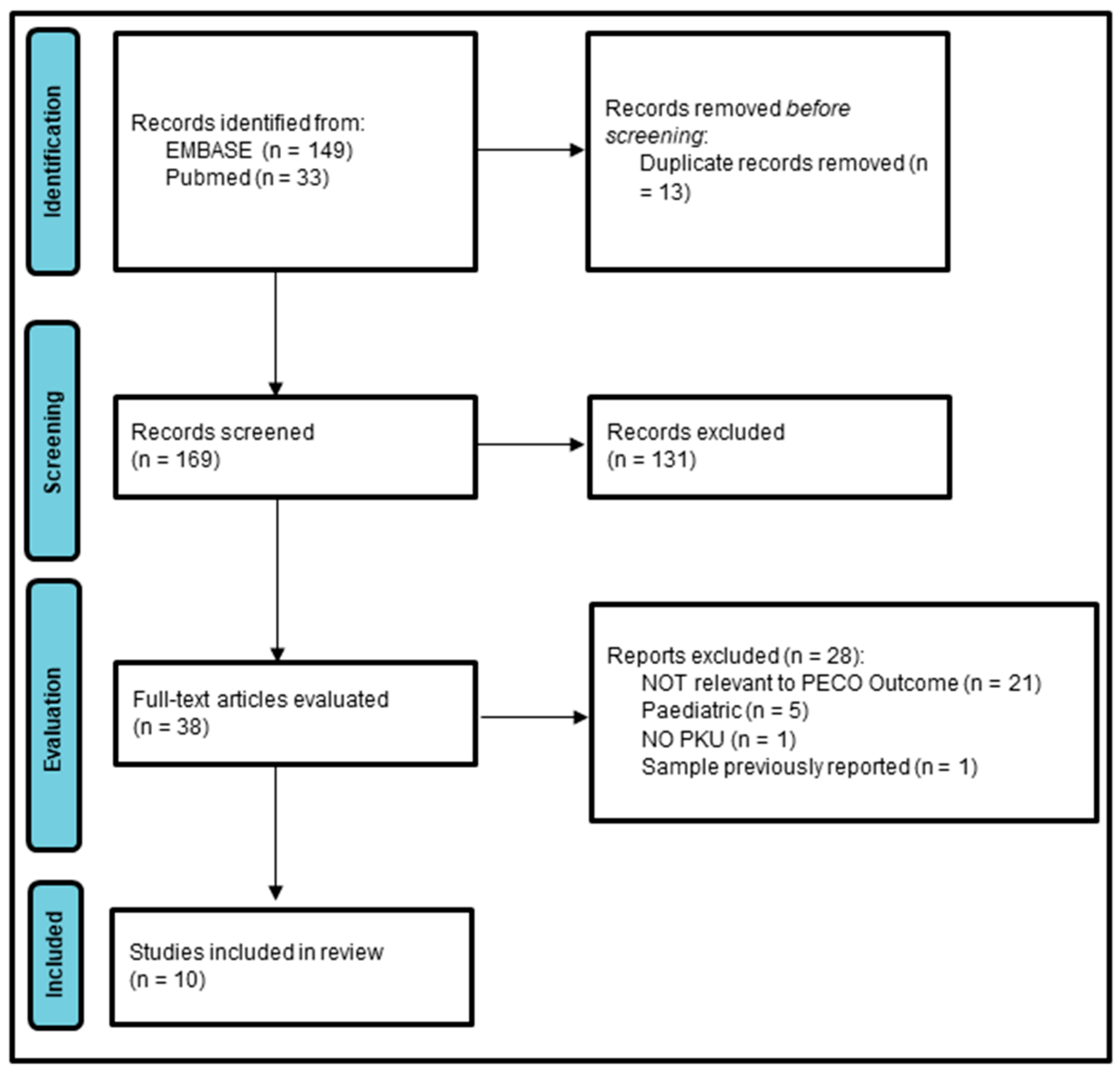
3.1. Study Selection
3.2. Study Characteristics
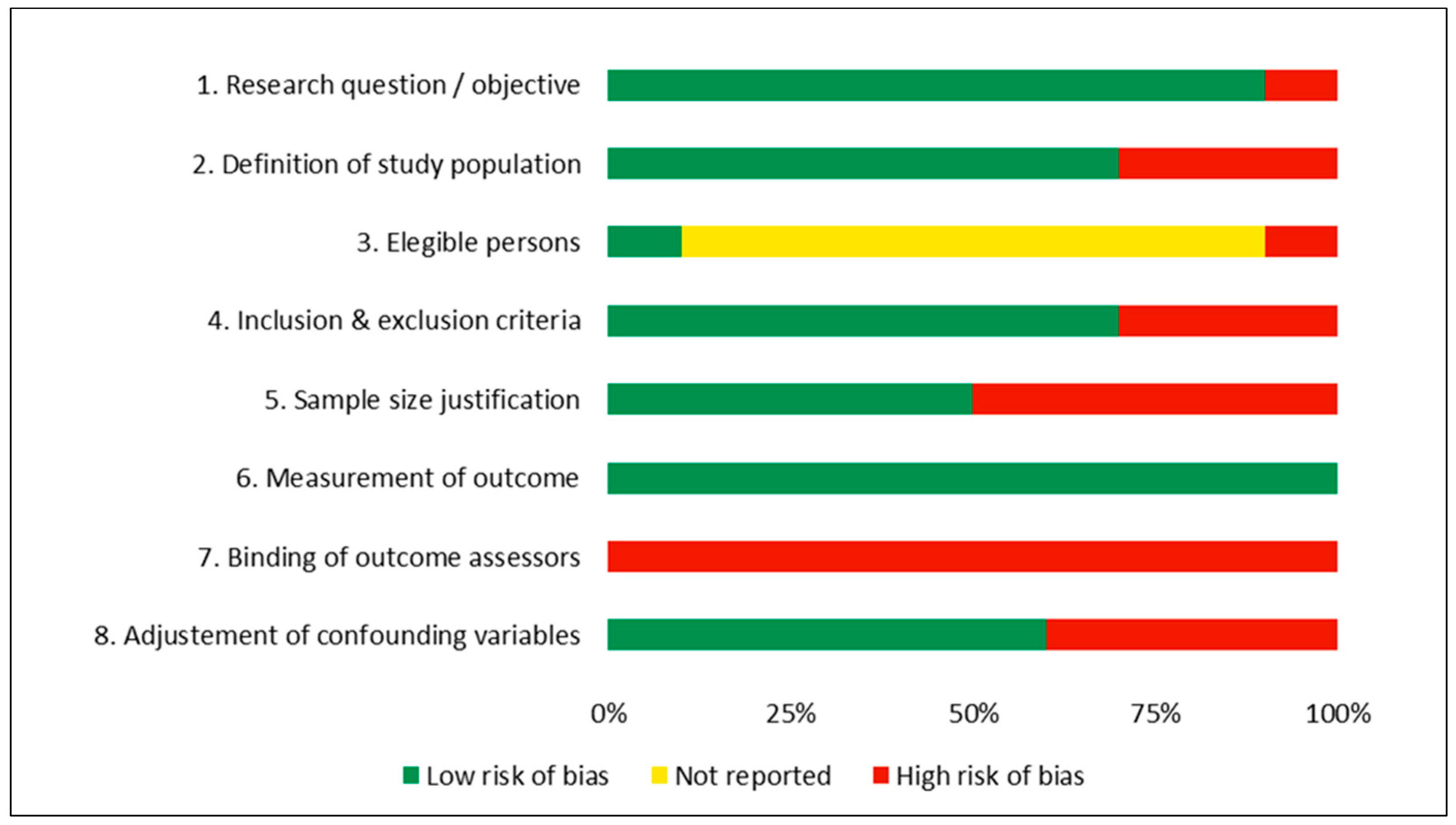
3.3. Risk of Bias Assessment
3.4. Synthesis of Results
3.4.1. Patients with PKU vs. Controls
3.4.2. Patients with PKU without Control Group
3.4.3. Metabolic Control
3.4.4. Sex
3.4.5. Body Fat Mass
3.4.6. Moderate vs. Poor Risk of Bias Studies
4. Discussion
4.1. Inherited Metabolic Diseases with Known Higher Cardiovascular Risk
- vascular endothelial injury and dysfunction, with less release of nitric oxide, thus favoring endothelial dysfunction and the atherothrombotic process [30];
- a prothrombotic state favored by an increase in the activity of coagulation factors V and XII and a higher production of thromboxane A2 (a potent platelet aggregator), favoring the genesis of vascular disease [33];
- intraluminal venous thrombi formation [34].
4.2. Adipose Tissue and Cardiometabolic Risk
4.3. Morphofunctional Assessment of Cardiometabolic Risk
4.4. Summary of Evidence
4.5. Strengths and Limitations of This Study
- Followed the PRISMA guidelines
- Clearly defined the objective of this review
- Defined inclusion and exclusion criteria according to the PECO format
- Included both PubMed and EMBASE databases in the search strategy
- Presented the full search strategies for both databases, including any filters and limits used
- Searched the reference lists of the included studies
- Described the study selection process using the PRISMA-model flow diagram
- Provided the list of excluded studies and the reasons for their exclusion in the Supplementary Material
- Provided a table with the main characteristics of the included studies
- Study selection, data search, and assessment of risk of bias and quality of evidence were performed by two independent authors
- Described the rationale for the review in the context of existing knowledge
- Provided an interpretation of the results in the context of the evidence
- Discussed the limitations of the evidence included in the review and the limitations of the review process itself.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Almeida, J.M.G.; García, C.G.; Castañeda, V.B.; Guerrero, D.B. Nuevo enfoque de la nutrición. Valoración del estado nutricional del paciente: Función y composición corporal. Nutr. Hosp. 2018, 35, 1–14. [Google Scholar] [CrossRef]
- García, C.G.; Almeida, J.M.G.; Aguilar, I.M.V.; Castañeda, V.B.; Guerrero, D.B. Morphofunctional assessment of patient nutritional status: A global approach. Nutr. Hosp. 2021, 38, 592–600. [Google Scholar] [CrossRef]
- Rocha, J.C.; MacDonald, A.; Trefz, F. Is overweight an issue in phenylketonuria? Mol. Genet. Metab. 2013, 110, S18–S24. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Pinto, A.; Faria, A.; Teixeira, D.; van Wegberg, A.M.J.; Ahring, K.; Feillet, F.; Calhau, C.; MacDonald, A.; Moreira-Rosário, A.; et al. Is the Phenylalanine-Restricted Diet a Risk Factor for Overweight or Obesity in Patients with Phenylketonuria (PKU)? A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3443. [Google Scholar] [CrossRef]
- Tankeu, A.T.; Pavlidou, D.C.; Superti-Furga, A.; Gariani, K.; Tran, C. Overweight and obesity in adult patients with phenylketonuria: A systematic review. Orphanet J. Rare Dis. 2023, 18, 37. [Google Scholar] [CrossRef] [PubMed]
- Coelho, M.; Oliveira, T.; Fernandes, R. Biochemistry of adipose tissue: An endocrine organ. Arch. Med. Sci. 2013, 9, 191–200. [Google Scholar] [CrossRef]
- Koenen, M.; Hill, M.A.; Cohen, P.; Sowers, J.R. Obesity, Adipose Tissue and Vascular Dysfunction. Circ. Res. 2021, 128, 951–968. [Google Scholar] [CrossRef]
- Oikonomou, E.K.; Antoniades, C. The role of adipose tissue in cardiovascular health and disease. Nat. Rev. Cardiol. 2018, 16, 83–99. [Google Scholar] [CrossRef]
- Compher, C.; Cederholm, T.; Correia, M.I.T.D.; Gonzalez, M.C.; Higashiguch, T.; Shi, H.P.; Bischoff, S.C.; Boirie, Y.; Carrasco, F.; Cruz-Jentoft, A.; et al. Guidance for assessment of the muscle mass phenotypic criterion for the Global Leadership Initiative on Malnutrition diagnosis of malnutrition. J. Parenter. Enter. Nutr. 2022, 46, 1232–1242. [Google Scholar] [CrossRef]
- Luengo-Pérez, L.M.; Fernández-Bueso, M.; Ambrojo, A.; Guijarro, M.; Ferreira, A.C.; Pereira-Da-Silva, L.; Moreira-Rosário, A.; Faria, A.; Calhau, C.; Daly, A.; et al. Body Composition Evaluation and Clinical Markers of Cardiometabolic Risk in Patients with Phenylketonuria. Nutrients 2023, 15, 5133. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Atkins, D.; Brozek, J.; Vist, G.; Alderson, P.; Glasziou, P.; Falck-Ytter, Y.; Schünemann, H.J. GRADE guidelines: 2. Framing the question and deciding on important outcomes. J. Clin. Epidemiology 2011, 64, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute (NHLBI) Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 23 February 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. he PRISMA 2020 statement: An updated guideline for reporting systematic reviews Systematic reviews and Meta-Analyses. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, N.; Alfheeaid, H.; Cochrane, B.; Adam, S.; Galloway, P.; Cozens, A.; Preston, T.; Malkova, D.; Gerasimidis, K. Mechanisms of obesity in children and adults with phenylketonuria on contemporary treatment. Clin. Nutr. ESPEN 2021, 46, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Barta, A.G.; Becsei, D.; Kiss, E.; Sumánszki, C.; Simonová, E.; Reismann, P. The Impact of Phenylketonuria on Body Composition in Adults. Ann. Nutr. Metab. 2021, 78, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Jani, R.; Coakley, K.; Douglas, T.; Singh, R. Protein intake and physical activity are associated with body composition in individuals with phenylalanine hydroxylase deficiency. Mol. Genet. Metab. 2017, 121, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Mezzomo, T.R.; Dias, M.R.M.G.; Pereira, R.M. Adults with early diagnosis of phenylketonuria have higher resting energy expenditure than adults with late diagnosis. Clin. Nutr. ESPEN 2023, 56, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Montanari, C.; Ceccarani, C.; Corsello, A.; Zuvadelli, J.; Ottaviano, E.; Cas, M.D.; Banderali, G.; Zuccotti, G.; Borghi, E.; Verduci, E. Glycomacropeptide Safety and Its Effect on Gut Microbiota in Patients with Phenylketonuria: A Pilot Study. Nutrients 2022, 14, 1883. [Google Scholar] [CrossRef] [PubMed]
- Rocha, J.C.; van Spronsen, F.J.; Almeida, M.F.; Soares, G.; Quelhas, D.; Ramos, E.; Guimarães, J.T.; Borges, N. Dietary treatment in phenylketonuria does not lead to increased risk of obesity or metabolic syndrome. Mol. Genet. Metab. 2012, 107, 659–663. [Google Scholar] [CrossRef]
- Rojas-Agurto, E.; Leal-Witt, M.J.; Arias, C.; Cabello, J.F.; Bunout, D.; Cornejo, V. Muscle and Bone Health in Young Chilean Adults with Phenylketonuria and Different Degrees of Compliance with the Phenylalanine Restricted Diet. Nutrients 2023, 15, 2939. [Google Scholar] [CrossRef] [PubMed]
- Stroup, B.M.; Hansen, K.E.; Krueger, D.; Binkley, N.; Ney, D.M. Sex differences in body composition and bone mineral density in phenylketonuria: A cross-sectional study. Mol. Genet. Metab. Rep. 2018, 15, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Weng, H.-L.; Yang, F.-J.; Chen, P.-R.; Hwu, W.-L.; Lee, N.-C.; Chien, Y.-H. Dietary intake and nutritional status of patients with phenylketonuria in Taiwan. Sci. Rep. 2020, 10, 14537. [Google Scholar] [CrossRef] [PubMed]
- Tansek, M.Z.; Bertoncel, A.; Sebez, B.; Zibert, J.; Groselj, U.; Battelino, T.; Stefanija, M.A. Anthropometry and bone mineral density in treated and untreated hyperphenylalaninemia. Endocr. Connect. 2020, 9, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Ney, D.M.; Stroup, B.M.; Clayton, M.K.; Murali, S.G.; Rice, G.M.; Rohr, F.; Levy, H.L. Glycomacropeptide for nutritional management of phenylketonuria: A randomized, controlled, crossover trial. Am. J. Clin. Nutr. 2016, 104, 334–345. [Google Scholar] [CrossRef] [PubMed]
- McCully, K.S.; Wilson, R.B. Homocysteine theory of arteriosclerosis. Atherosclerosis 1975, 22, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Daly, L.; Robinson, K.; Naughten, E.; Cahalane, S.; Fowler, B.; Graham, I. Hyperhomocysteinemia: An Independent Risk Factor for Vascular Disease. N. Engl. J. Med. 1991, 324, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Verhoef, P.; Stampfer, M.J. Prospective Studies of Homocysteine and Cardiovascular Disease. Nutr. Rev. 2009, 53, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.L.; Jacobsen, D.W.; Robinson, K. Homocysteine and coronary atherosclerosis. Circ. 1996, 27, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.C.; A Perrella, M.; Yoshizumi, M.; Hsieh, C.M.; Haber, E.; Schlegel, R.; E Lee, M. Promotion of vascular smooth muscle cell growth by homocysteine: A link to atherosclerosis. Proc. Natl. Acad. Sci. USA 1994, 91, 6369–6373. [Google Scholar] [CrossRef]
- Hirano, K.; Ogihara, T.; Miki, M.; Yasuda, H.; Tamai, H.; Kawamura, N.; Mino, M. Homocysteine Induces Iron-Catalyzed Lipid Peroxidation of Low-Density Lipoprotein that is Prevented by Alpha-Tocopherol. Free. Radic. Res. 1994, 21, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Di Minno, G.; Davì, G.; Margaglione, M.; Cirillo, F.; Grandone, E.; Ciabattoni, G.; Catalano, I.; Strisciuglio, P.; Andria, G.; Patrono, C. Abnormally high thromboxane biosynthesis in homozygous homocystinuria. Evidence for platelet involvement and probucol-sensitive mechanism. J. Clin. Investig. 1993, 92, 1400–1406. [Google Scholar] [CrossRef] [PubMed]
- Magner, M.; Krupková, L.; Honzík, T.; Zeman, J.; Hyánek, J.; Kožich, V. Vascular presentation of cystathionine beta-synthase deficiency in adulthood. J. Inherit. Metab. Dis. 2010, 34, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Morris, J.K.; Wald, N.J. Reconciling the Evidence on Serum Homocysteine and Ischaemic Heart Disease: A Meta-Analysis. PLoS ONE 2011, 6, e16473. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Law, M.; Morris, J.K. Homocysteine and cardiovascular disease: Evidence on causality from a meta-analysis. BMJ 2002, 325, 1202–1206. [Google Scholar] [CrossRef] [PubMed]
- Rake, J.; Visser, G.; Labrune, P.; Leonard, J.V.; Ullrich, K.; Smit, P.G. Glycogen storage disease type I: Diagnosis, management, clinical course and outcome. Results of the European Study on Glycogen Storage Disease Type I (ESGSD I). Eur. J. Pediatr. 2002, 161, S20–S34. [Google Scholar] [CrossRef] [PubMed]
- Bandsma, R.H.; Smit, P.G.; Kuipers, F. Disturbed lipid metabolism in glycogen storage disease type 1. Eur. J. Pediatr. 2002, 161, S65–S69. [Google Scholar] [CrossRef]
- Wierzbicki, A.S.; Watts, G.F.; Lynas, J.; Winder, A.F.; Wray, R. Very low-density lipoprotein apolipoprotein B-100 turnover in glycogen storage disease type Ia (von Gierke disease). J. Inherit. Metab. Dis. 2001, 24, 527–534. [Google Scholar] [CrossRef]
- Bernier, A.V.; Correia, C.E.; Haller, M.J.; Theriaque, D.W.; Shuster, J.J.; Weinstein, D.A. Vascular Dysfunction in Glycogen Storage Disease Type I. J. Pediatr. 2009, 154, 588–591. [Google Scholar] [CrossRef]
- Xue, Y.; Petrovic, N.; Cao, R.; Larsson, O.; Lim, S.; Chen, S.; Feldmann, H.M.; Liang, Z.; Zhu, Z.; Nedergaard, J.; et al. Hypoxia-Independent Angiogenesis in Adipose Tissues during Cold Acclimation. Cell Metab. 2009, 9, 99–109. [Google Scholar] [CrossRef]
- Després, J.-P. Body Fat Distribution and Risk of Cardiovascular Disease: An update. Circulation 2012, 126, 1301–1313. [Google Scholar] [CrossRef] [PubMed]
- Recinella, L.; Orlando, G.; Ferrante, C.; Chiavaroli, A.; Brunetti, L.; Leone, S. Adipokines: New Potential Therapeutic Target for Obesity and Metabolic, Rheumatic, and Cardiovascular Diseases. Front. Physiol. 2020, 11, 578966. [Google Scholar] [CrossRef] [PubMed]
- Farkhondeh, T.; Llorens, S.; Pourbagher-Shahri, A.M.; Ashrafizadeh, M.; Talebi, M.; Shakibaei, M.; Samarghandian, S. An Overview of the Role of Adipokines in Cardiometabolic Diseases. Molecules 2020, 25, 5218. [Google Scholar] [CrossRef] [PubMed]
- Smekal, A.; Vaclavik, J. Adipokines and cardiovascular disease: A comprehensive review. Biomed. Pap. 2017, 161, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Shibata, R.; Ouchi, N.; Ohashi, K.; Murohara, T. The role of adipokines in cardiovascular disease. J. Cardiol. 2017, 70, 329–334. [Google Scholar] [CrossRef]
- Javed, A.; Jumean, M.; Murad, M.H.; Okorodudu, D.; Kumar, S.; Somers, V.K.; Sochor, O.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity in children and adolescents: A systematic review and meta-analysis. Pediatr. Obes. 2014, 10, 234–244. [Google Scholar] [CrossRef]
- Zimmet, P.; Magliano, D.; Matsuzawa, Y.; Alberti, G.; Shaw, J. The Metabolic Syndrome: A Global Public Health Problem and A New Definition. J. Atheroscler. Thromb. 2005, 12, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Gaskill, S.P.; Haffner, S.M.; Stern, M.P. Waist Circumference as the Best Predictor of Noninsulin Dependent Diabetes Mellitus (NIDDM) Compared to Body Mass Index, Waist/hip Ratio and Other Anthropometric Measurements in Mexican Americans—A 7-Year Prospective Study. Obes. Res. 1997, 5, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Van Der Kooy, K.; Leenen, R.; Seidell, J.C.; Deurenberg, P.; Visser, M. Abdominal diameters as indicators of visceral fat: Comparison between magnetic resonance imaging and anthropometry. Br. J. Nutr. 1993, 70, 47–58. [Google Scholar] [CrossRef] [PubMed]
- De La Torre, M.L.; Guerrero, D.B.; Cortada, J.V.; González, A.S.; Malpartida, K.G.; Hernandez-Mijares, A. Distribución de la circunferencia de la cintura y de la relación circunferencia de la cintura con respecto a la talla según la categoría del índice de masa corporal en los pacientes atendidos en consultas de endocrinología y nutrición. Endocrinol. Nutr. 2010, 57, 479–485. [Google Scholar] [CrossRef]
- Rodea-Montero, E.R.; Evia-Viscarra, M.L.; Apolinar-Jiménez, E. Waist-to-Height Ratio Is a Better Anthropometric Index than Waist Circumference and BMI in Predicting Metabolic Syndrome among Obese Mexican Adolescents. Int. J. Endocrinol. 2014, 2014, 195407. [Google Scholar] [CrossRef]
- Woolcott, O.O.; Bergman, R.N. Relative fat mass (RFM) as a new estimator of whole-body fat percentage—A cross-sectional study in American adult individuals. Sci. Rep. 2018, 8, 10980. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, C.R.; Formolo, N.P.S.; Dezanetti, T.; Speretta, G.F.F.; Nunes, E.A. Relative fat mass is a better tool to diagnose high adiposity when compared to body mass index in young male adults: A cross-section study. Clin. Nutr. ESPEN 2020, 41, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.C.; Giordano, C.; Pitrone, M.; Galluzzo, A. Cut-off points of the visceral adiposity index (VAI) identifying a visceral adipose dysfunction associated with cardiometabolic risk in a Caucasian Sicilian population. Lipids Health Dis. 2011, 10, 183. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Ge, L.; Yang, H.; He, Y.; Wang, Y. Chinese Visceral Adipose Index Shows Superior Diagnostic Performance in Predicting the Risk of Metabolic Dysfunction Associated Fatty Liver Disease in Early Postmenopausal Chinese Women. Diabetes Metab. Syndr. Obes. Targets Ther. 2023, 2023, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Fosbøl, M.O.; Zerahn, B. Contemporary methods of body composition measurement. Clin. Physiol. Funct. Imaging 2015, 35, 81–97. [Google Scholar] [CrossRef]
- Ceniccola, G.D.; Castro, M.G.; Piovacari, S.M.F.; Horie, L.M.; Corrêa, F.G.; Barrere, A.P.N.; Toledo, D.O. Current technologies in body composition assessment: Advantages and disadvantages. Nutrition 2018, 62, 25–31. [Google Scholar] [CrossRef]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the Bedside. Nutr. Clin. Pract. 2015, 30, 180–193. [Google Scholar] [CrossRef] [PubMed]
- Price, K.L.; Earthman, C.P. Update on body composition tools in clinical settings: Computed tomography, ultrasound, and bioimpedance applications for assessment and monitoring. Eur. J. Clin. Nutr. 2018, 73, 187–193. [Google Scholar] [CrossRef]
- García-Almeida, J.M.; García-García, C.; Vegas-Aguilar, I.M.; Pomar, M.D.B.; Cornejo-Pareja, I.M.; Medina, B.F.; Román, D.A.d.L.; Guerrero, D.B.; Lesmes, I.B.; Madueño, F.J.T. Nutritional ultrasound®: Conceptualisation, technical considerations and standardisation. Endocrinol. Diabetes Y Nutr. 2023, 70, 74–84. [Google Scholar] [CrossRef]
- Walker, F. Neuromuscular ultrasound. Neurol. Clin. 2004, 22, 563–590. [Google Scholar] [CrossRef] [PubMed]
- Mayans, D.; Cartwright, M.S.; Walker, F.O. Neuromuscular Ultrasonography: Quantifying Muscle and Nerve Measurements. Phys. Med. Rehabil. Clin. N. Am. 2012, 23, 133–148. [Google Scholar] [CrossRef]
- Casey, P.; Alasmar, M.; McLaughlin, J.; Ang, Y.; McPhee, J.; Heire, P.; Sultan, J. The current use of ultrasound to measure skeletal muscle and its ability to predict clinical outcomes: A systematic review. J. Cachex Sarcopenia Muscle 2022, 13, 2298–2309. [Google Scholar] [CrossRef]
- Hernández-Socorro, C.R.; Saavedra, P.; López-Fernández, J.C.; Ruiz-Santana, S. Assessment of Muscle Wasting in Long-Stay ICU Patients Using a New Ultrasound Protocol. Nutrients 2018, 10, 1849. [Google Scholar] [CrossRef]
- Figueiredo, P.; Marques, E.A.; Gudnason, V.; Lang, T.; Sigurdsson, S.; Jonsson, P.V.; Aspelund, T.; Siggeirsdottir, K.; Launer, L.; Eiriksdottir, G.; et al. Computed tomography-based skeletal muscle and adipose tissue attenuation: Variations by age, sex, and muscle. Exp. Gerontol. 2021, 149, 111306. [Google Scholar] [CrossRef]
- Amini, B.; Boyle, S.P.; Boutin, R.D.; Lenchik, L. Approaches to Assessment of Muscle Mass and Myosteatosis on Computed Tomography: A Systematic Review. J. Gerontol. Ser. A 2019, 74, 1671–1678. [Google Scholar] [CrossRef]
- Correa-De-Araujo, R.; Addison, O.; Miljkovic, I.; Goodpaster, B.H.; Bergman, B.C.; Clark, R.V.; Elena, J.W.; Esser, K.A.; Ferrucci, L.; Harris-Love, M.O.; et al. Myosteatosis in the Context of Skeletal Muscle Function Deficit: An Interdisciplinary Workshop at the National Institute on Aging. Front. Physiol. 2020, 11, 963. [Google Scholar] [CrossRef] [PubMed]
- Rosenquist, K.J.; Pedley, A.; Massaro, J.M.; Therkelsen, K.E.; Murabito, J.M.; Hoffmann, U.; Fox, C.S. Visceral and Subcutaneous Fat Quality and Cardiometabolic Risk. JACC Cardiovasc. Imaging 2013, 6, 762–771. [Google Scholar] [CrossRef] [PubMed]
- Brennan, D.D.; Whelan, P.F.; Robinson, K.; Ghita, O.; O’Brien, J.M.; Sadleir, R.; Eustace, S.J. Rapid Automated Measurement of Body Fat Distribution from Whole-Body MRI. Am. J. Roentgenol. 2005, 185, 418–423. [Google Scholar] [CrossRef]
- Borga, M.; West, J.; Bell, J.D.; Harvey, N.C.; Romu, T.; Heymsfield, S.B.; Leinhard, O.D. Advanced body composition assessment: From body mass index to body composition profiling. J. Investig. Med. 2018, 66, 1–9. [Google Scholar] [CrossRef]
- Zaffina, C.; Wyttenbach, R.; Pagnamenta, A.; Grasso, R.F.; Biroli, M.; Del Grande, F.; Rizzo, S. Body composition assessment: Comparison of quantitative values between magnetic resonance imaging and computed tomography. Quant. Imaging Med. Surg. 2022, 12, 1450–1466. [Google Scholar] [CrossRef] [PubMed]
- Lehr, S.; Hartwig, S.; Lamers, D.; Famulla, S.; Müller, S.; Hanisch, F.-G.; Cuvelier, C.; Ruige, J.; Eckardt, K.; Ouwens, D.M.; et al. Identification and Validation of Novel Adipokines Released from Primary Human Adipocytes. Mol. Cell. Proteom. 2012, 11. [Google Scholar] [CrossRef]
- Kahn, C.R.; Wang, G.; Lee, K.Y. Altered adipose tissue and adipocyte function in the pathogenesis of metabolic syndrome. J. Clin. Investig. 2019, 129, 3990–4000. [Google Scholar] [CrossRef] [PubMed]
- van de Woestijne, A.P.; Monajemi, H.; Kalkhoven, E.; Visseren, F.L.J. Adipose tissue dysfunction and hypertriglyceridemia: Mechanisms and management. Obes. Rev. 2011, 12, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Luengo-Pérez, L.M.; Ambrojo, A.; Fernández-Bueso, M.; Guijarro, M.; Ferreira, A.; Luzes, G.; Pereira, M.; Calhau, C.; Rocha, J.C. Muscle Quality and Risk of Metabolic Syndrome in Adult Patients with Inherited Metabolic Diseases. Endocr. Metab. Immune Disord. Drug Targets 2023, 24, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Sena, B.d.S.; de Andrade, M.I.S.; da Silva, A.P.F.; Dourado, K.F.; Silva, A.L.F. Overweight and associated factors in children and adolescents with phenylketonuria: A systematic review. Rev. Paul. Pediatr. 2020, 38, e2018201. [Google Scholar] [CrossRef]
- Aldámiz-Echevarría, L.; Bueno, M.A.; Couce, M.L.; Lage, S.; Dalmau, J.; Vitoria, I.; Andrade, F.; Blasco, J.; Alcalde, C.; Gil, D.; et al. Anthropometric characteristics and nutrition in a cohort of PAH-deficient patients. Clin. Nutr. 2013, 33, 702–717. [Google Scholar] [CrossRef] [PubMed]
- Burrage, L.C.; McConnell, J.; Haesler, R.; O’Riordan, M.A.; Sutton, V.R.; Kerr, D.S.; McCandless, S.E. High prevalence of overweight and obesity in females with phenylketonuria. Mol. Genet. Metab. 2012, 107, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Camatta, G.C.; Kanufre, V.d.C.; Alves, M.R.A.; Soares, R.D.L.; Norton, R.D.C.; de Aguiar, M.J.B.; Starling, A.L.P. Body fat percentage in adolescents with phenylketonuria and associated factors. Mol. Genet. Metab. Rep. 2020, 23, 100595. [Google Scholar] [CrossRef]
- Couce, M.L.; Vitoria, I.; Aldámiz-Echevarría, L.; Fernández-Marmiesse, A.; Roca, I.; Llarena, M.; Sánchez-Pintos, P.; Leis, R.; Hermida, A. Lipid profile status and other related factors in patients with Hyperphenylalaninaemia. Orphanet J. Rare Dis. 2016, 11, 123. [Google Scholar] [CrossRef]
- Daly, A.; Evans, S.; Pinto, A.; Jackson, R.; Ashmore, C.; Rocha, J.C.; MacDonald, A. The Impact of the Use of Glycomacropeptide on Satiety and Dietary Intake in Phenylketonuria. Nutrients 2020, 12, 2704. [Google Scholar] [CrossRef] [PubMed]
- Dios-Fuentes, E.; Marin, M.G.; Remón-Ruiz, P.; Avila, R.B.; Delgado, M.A.B.; Alonso, J.B.; Gamgaram, V.K.D.; Olveira, G.; Soto-Moreno, A.; Venegas-Moreno, E. Cardiometabolic and Nutritional Morbidities of a Large, Adult, PKU Cohort from Andalusia. Nutrients 2022, 14, 1311. [Google Scholar] [CrossRef] [PubMed]
- Enns, G.; Koch, R.; Brumm, V.; Blakely, E.; Suter, R.; Jurecki, E. Suboptimal outcomes in patients with PKU treated early with diet alone: Revisiting the evidence. Mol. Genet. Metab. 2010, 101, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Ozel, H.G.; Ahring, K.; Bélanger-Quintana, A.; Dokoupil, K.; Lammardo, A.; Robert, M.; Rocha, J.; Almeida, M.; van Rijn, M.; MacDonald, A. Overweight and obesity in PKU: The results from 8 centres in Europe and Turkey. Mol. Genet. Metab. Rep. 2014, 1, 483–486. [Google Scholar] [CrossRef]
- Gramer, G.; Haege, G.; Langhans, C.-D.; Schuhmann, V.; Burgard, P.; Hoffmann, G.F. Long-chain polyunsaturated fatty acid status in children, adolescents and adults with phenylketonuria. Prostaglandins Leukot. Essent. Fat. Acids 2016, 109, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Hochuli, M.; Bollhalder, S.; Thierer, C.; Refardt, J.; Gerber, P.; Baumgartner, M.R. Effects of Inadequate Amino Acid Mixture Intake on Nutrient Supply of Adult Patients with Phenylketonuria. Ann. Nutr. Metab. 2017, 71, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Htun, P.; Nee, J.; Ploeckinger, U.; Eder, K.; Geisler, T.; Gawaz, M.; Bocksch, W.; Fateh-Moghadam, S. Fish-Free Diet in Patients with Phenylketonuria Is Not Associated with Early Atherosclerotic Changes and Enhanced Platelet Activation. PLoS ONE 2015, 10, e0135930. [Google Scholar] [CrossRef]
- Leiva, C.; Bravo, P.; Arias, C.; Cabello, J.; Leal-Witt, M.; Salazar, F.; Cornejo, V. 25 Hydroxy Vitamin D Level, Bone Health, Vitamin D and Calcium Intake in Chilean Patients with Phenylketonuria and Hyperphenylalaninemias. J. Inborn Errors Metab. Screen. 2021, 9. [Google Scholar] [CrossRef]
- MacLeod, E.L.; Gleason, S.T.; van Calcar, S.C.; Ney, D.M. Reassessment of phenylalanine tolerance in adults with phenylketonuria is needed as body mass changes. Mol. Genet. Metab. 2009, 98, 331–337. [Google Scholar] [CrossRef]
- Mazzola, P.N.; Teixeira, B.C.; Schirmbeck, G.H.; Reischak-Oliveira, A.; Derks, T.G.; van Spronsen, F.J.; Dutra-Filho, C.S.; Schwartz, I.V.D. Acute exercise in treated phenylketonuria patients: Physical activity and biochemical response. Mol. Genet. Metab. Rep. 2015, 5, 55–59. [Google Scholar] [CrossRef]
- Okano, Y.; Hattori, T.; Fujimoto, H.; Noi, K.; Okamoto, M.; Watanabe, T.; Watanabe, R.; Fujii, R.; Tamaoki, T. Nutritional status of patients with phenylketonuria in Japan. Mol. Genet. Metab. Rep. 2016, 8, 103–110. [Google Scholar] [CrossRef] [PubMed]
- van Calcar, S.C.; MacLeod, E.L.; Gleason, S.T.; Etzel, M.R.; Clayton, M.K.; A Wolff, J.; Ney, D.M. Improved nutritional management of phenylketonuria by using a diet containing glycomacropeptide compared with amino acids. Am. J. Clin. Nutr. 2009, 89, 1068–1077. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Agra, N.; Fernandez-Crespo, S.; Marques-Afonso, A.-T.; Cruces-Sande, A.; Barbosa-Gouveia, S.; Martinez-Olmos, M.-A.; Hermida-Ameijeiras, A. The correlation of lipid profile and waist circumference with phenylalanine levels in adult patients with classical phenylketonuria. Med. Clin. 2023, 160, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Viau, K.; Wessel, A.; Martell, L.; Sacharow, S.; Rohr, F. Nutrition status of adults with phenylketonuria treated with pegvaliase. Mol. Genet. Metab. 2021, 133, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Wernlund, P.G.; Hvas, C.L.; Dahlerup, J.F.; Bahl, M.I.; Licht, T.R.; Knudsen, K.E.B.; Agnholt, J.S. Casein glycomacropeptide is well tolerated in healthy adults and changes neither high-sensitive C-reactive protein, gut microbiota nor faecal butyrate: A restricted randomised trial. Br. J. Nutr. 2021, 125, 1374–1385. [Google Scholar] [CrossRef] [PubMed]
- de Castro, M.-J.; Sánchez-Pintos, P.; Abdelaziz-Salem, N.; Leis, R.; Couce, M.L. Evaluation of Body Composition, Physical Activity, and Food Intake in Patients with Inborn Errors of Intermediary Metabolism. Nutrients 2021, 13, 2111. [Google Scholar] [CrossRef] [PubMed]
- Doulgeraki, A.; Skarpalezou, A.; Theodosiadou, A.; Monopolis, I.; Schulpis, K. Body Composition Profile of Young Patients With Phenylketonuria and Mild Hyperphenylalaninemia. Int. J. Endocrinol. Metab. 2014, 12, e16061. [Google Scholar] [CrossRef]
- Evans, M.; Truby, H.; Boneh, A. The relationship between dietary intake, growth and body composition in Phenylketonuria. Mol. Genet. Metab. 2017, 122, 36–42. [Google Scholar] [CrossRef]
- Evans, M.; Nguo, K.; Boneh, A.; Truby, H. The Validity of Bioelectrical Impedance Analysis to Measure Body Composition in Phenylketonuria. JIMD Rep. 2018, 42, 37–45. [Google Scholar] [CrossRef]
- Mazzola, P.N.; Nalin, T.; Castro, K.; van Rijn, M.; Derks, T.G.; Perry, I.D.; Mainieri, A.S.; Schwartz, I.V.D. Analysis of body composition and nutritional status in Brazilian phenylketonuria patients. Mol. Genet. Metab. Rep. 2016, 6, 16–20. [Google Scholar] [CrossRef]
- Alfheeaid, H.; Gerasimidis, K.; Năstase, A.-M.; Elhauge, M.; Cochrane, B.; Malkova, D. Impact of phenylketonuria type meal on appetite, thermic effect of feeding and postprandial fat oxidation. Clin. Nutr. 2018, 37, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Rocha, J.C.; van Spronsen, F.J.; Almeida, M.F.; Ramos, E.; Guimarães, J.T.; Borges, N. Early dietary treated patients with phenylketonuria can achieve normal growth and body composition. Mol. Genet. Metab. 2013, 110, S40–S43. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Reference (Country) | Study Design (Duration of Follow-Up) | Sample Size (Age) | Controls (Age) | Sex (F/M) | Other | Risk of Bias 1 |
|---|---|---|---|---|---|---|
| Alghamdi et al. 2021 (UK) [16] | Cross-sectional | 10 (33.9 ± 5.0) | 9 (28.8 ± 5.9) | P: 6/4 C: 6/3 | Mixed pediatric and adult sample | High |
| Barta et al. 2022 (Hungary) [17] | Cross-sectional | 50 (F 31 ± 7.8, M 26.6 ± 7.6) | 40 (F 26.5, M 24) | P: 27/23 C: 20/20 | - | High |
| Jani et al. 2017 (USA) [18] | Cross-sectional | 27 (28.8, [19.5–54.6]) | NO | 18/9 | Mixed pediatric and adult sample, compared with reference US population | High |
| Mezzomo et al. 2023 (Brazil) [19] | Cross-sectional | 36 (25.36 ± 5.14) | 33 (28.27 ± 6.15) | P: 16/20 C: 21/12 | - | Moderate |
| Montanari et al. 2022 (Italy) [20] | Longitudinal (6 months) | 4 (n.a.) | NO | n.a. | Mixed pediatric and adult sample | High |
| Rocha et al. 2012 (Portugal) [21] | Cross-sectional | 26 (22.8 ± 3.0) | 29 (23.6 ± 4.7) | n.a. | Mixed pediatric and adult sample | Moderate |
| Rojas Agurto et al. 2023 (Chile) [22] | Cross-sectional | 24 (39.3) | 24 (38.4) | P: 10/14 C: 10/14 | High | |
| Stroup et al. 2018 (USA) [23] | Cross-sectional | 15 (15–50) | NO | 9/6 | Included 3 adolescents (15–17 y) | High |
| Weng et al. 2020 (Taiwan) [24] | Cross-sectional | 22 (15.23 ± 5.23 [8–27]) | 22 (19.73 ± 10.6 [8–39]) | P: 12/10 C: 12/10 | Correlates inversely with protein intake Adult subjects number not shown | High |
| Zerjav Tansek et al. 2020 (Slovenia) [25] | Cross-sectional | 96 (48 adults) (22.2 ± 11.4) | NO/62 mild HPA (14.4 ± 6.8) | P: 50/46 HPA: 22/40 | Compared with mild HPA, not healthy controls | High |
| Reference (Country) | Parameter, Technique | PKU | Control | Difference | p |
|---|---|---|---|---|---|
| Alghamdi et al. 2021 (UK) [16] | FM (%) FMI Deuterium | 39.4 ± 8.2 12.9 ± 4.6 | 34.3 ± 11.1 11.0 ± 5.8 | +5.1 +1.8 | n.a. n.a. |
| Rocha et al. 2012 (Portugal) [21] | FM (%), BIA | 23.8 (13.9, 35.5) | 23.8 (17.9, 34.3) | 0 | 0.964 |
| Rojas Agurto et al. 2023 (Chile) [22] | FM (kg), DXA | 23.15 | 24.56 | −1.41 | n.a. |
| Weng et al. 2020 (Taiwan) [24] | FM (%), BIA | 20.74 ± 8.9 | 18.67 ± 7.52 | +2.07 | 0.4635 |
| Zerjav Tansek et al. 2020 (Slovenia) [25] | FM (%) AFM (%) DXA | 25.8 ± 6.8 22.7 ± 7.8 | 25.4 ± 6.7 21.1 ± 7.2 (HPA) | +0.4 +1.6 | 0.758 0.204 |
| Reference (Country) | Parameter, Technique | Female PKU | Female Control | Difference | Male PKU | Male Control | Difference |
|---|---|---|---|---|---|---|---|
| Barta et al. 2022 (Hungary) [17] | FM (%), BIA | 36.7 (30.6, 40.2) | 24.7 (22.2, 30.8) | +12.0 * | 18.7 (14.3, 29.8) | 19.4 (15.07, 24.5) | −0.7 |
| Jani et al. 2017 (USA) [18] | FMI, DXA | 38.9 *** (30.8, 64.3) | 40.7 ** | −1.8 | 23.4 *** (13.8, 81.4) | 28.7 ** | +5.3 |
| Mezzomo et al. 2023 (Brazil) [19] | FM (%), BIA | 36.2 (20.1, 49.0) | 28.4 (15.9, 46.4) | +7.2 | 17.4 (10.1, 29.5) | 23.3 (12.1, 27.2) | −5.9 |
| Stroup et al. 2018 (USA) [23] | FM (%), DXA | 36.5 ± 2.5 | - | - | 24.5 ± 4.8 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luengo-Pérez, L.M.; Fernández-Bueso, M.; Guzmán-Carmona, C.; López-Navia, A.; García-Lobato, C. Morphofunctional Assessment beyond Malnutrition: Fat Mass Assessment in Adult Patients with Phenylketonuria—Systematic Review. Nutrients 2024, 16, 1833. https://doi.org/10.3390/nu16121833
Luengo-Pérez LM, Fernández-Bueso M, Guzmán-Carmona C, López-Navia A, García-Lobato C. Morphofunctional Assessment beyond Malnutrition: Fat Mass Assessment in Adult Patients with Phenylketonuria—Systematic Review. Nutrients. 2024; 16(12):1833. https://doi.org/10.3390/nu16121833
Chicago/Turabian StyleLuengo-Pérez, Luis M., Mercedes Fernández-Bueso, Carlos Guzmán-Carmona, Ana López-Navia, and Claudia García-Lobato. 2024. "Morphofunctional Assessment beyond Malnutrition: Fat Mass Assessment in Adult Patients with Phenylketonuria—Systematic Review" Nutrients 16, no. 12: 1833. https://doi.org/10.3390/nu16121833
APA StyleLuengo-Pérez, L. M., Fernández-Bueso, M., Guzmán-Carmona, C., López-Navia, A., & García-Lobato, C. (2024). Morphofunctional Assessment beyond Malnutrition: Fat Mass Assessment in Adult Patients with Phenylketonuria—Systematic Review. Nutrients, 16(12), 1833. https://doi.org/10.3390/nu16121833