
Body Mass Index Distribution in Female Child, Adolescent and Adult Inpatients with Anorexia Nervosa—A Retrospective Chart Review
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Description
2.2. Data Analyses
3. Results
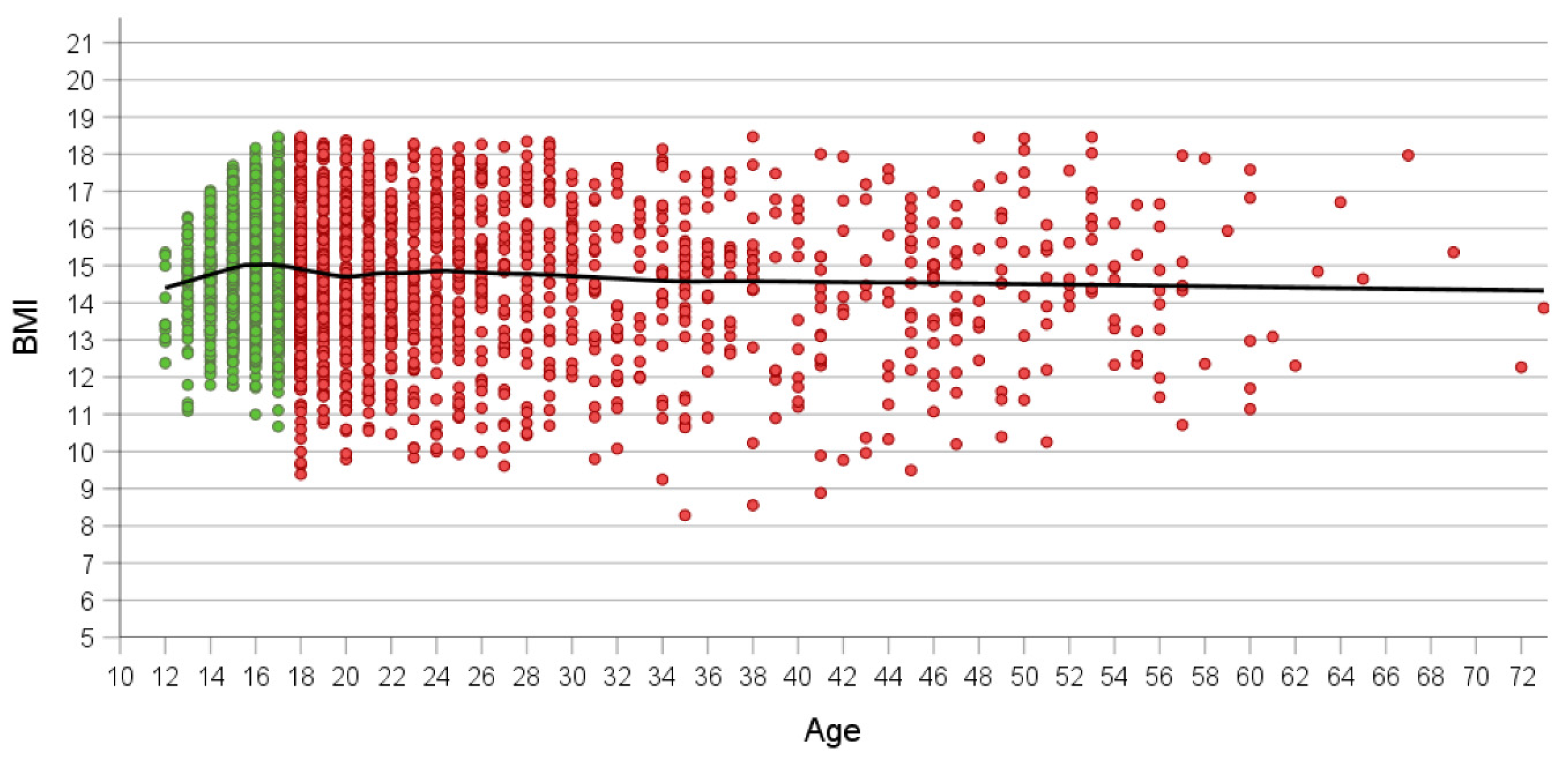
3.1. Relationship between Age and BMI
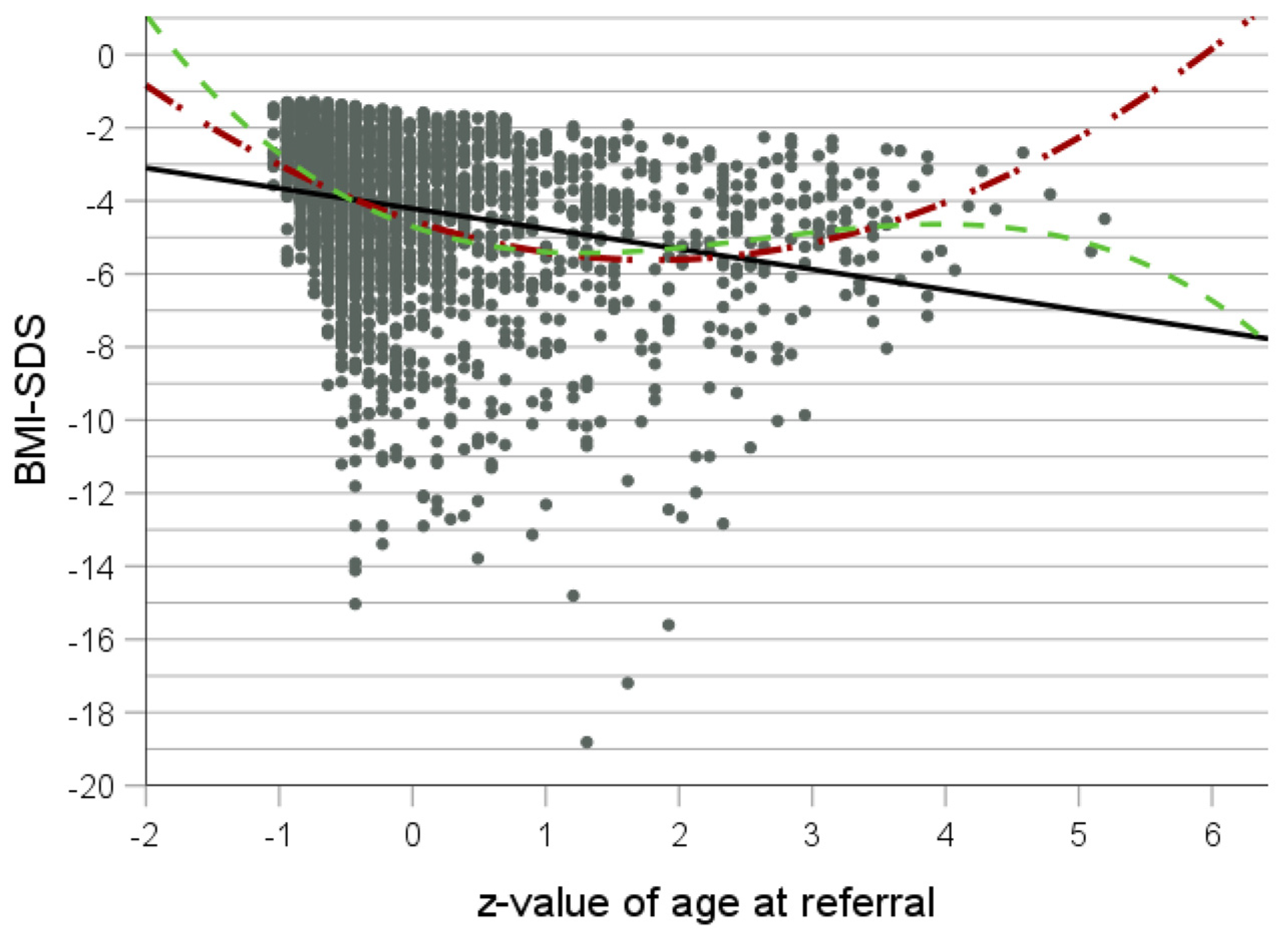
3.2. Curve Fit Analyses
3.3. Association of Height, Height-SDS and BMI in Adolescents
3.4. Association of Height, Height-SDS and BMI in Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Engelhardt, C.; Foecker, M.; Buehren, K.; Dahmen, B.; Becker, K.; Weber, L.; Correll, C.U.; Egberts, K.M.; Ehrlich, S.; Roessner, V.; et al. Age dependency of body mass index distribution in childhood and adolescent inpatients with anorexia nervosa with a focus on DSM-5 and ICD-11 weight criteria and severity specifiers. Eur. Child Adolesc. Psychiatry 2021, 30, 1081–1094. [Google Scholar] [CrossRef] [PubMed]
- Loomba-Albrecht, L.A.; Styne, D.M. Effect of puberty on body composition. Curr. Opin. Endocrinol. Diabetes 2009, 16, 10–15. [Google Scholar] [CrossRef]
- APA. Diagnostic and Statistical Manual of Mental Disorders (DSM-III), 3rd ed.; American Psychiatric Association: Washington, DC, USA, 1980. [Google Scholar]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; de Pablo, G.S.; Shin, J.I.; Kirkbride, J.B.; Jones, P.; Kim, J.H.; et al. Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 2022, 27, 281–295. [Google Scholar] [CrossRef]
- Miller, C.A.; Golden, N.H. An introduction to eating disorders: Clinical presentation, epidemiology, and prognosis. Nutr. Clin. Pract. 2010, 25, 110–115. [Google Scholar] [CrossRef]
- APA. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Modan-Moses, D.; Yaroslavsky, A.; Pinhas-Hamiel, O.; Levy-Shraga, Y.; Kochavi, B.; Iron-Segev, S.; Enoch-Levy, A.; Toledano, A.; Stein, D. Prospective Longitudinal Assessment of Linear Growth and Adult Height in Female Adolescents with Anorexia Nervosa. J. Clin. Endocrinol. Metab. 2021, 106, e1–e10. [Google Scholar] [CrossRef]
- Solmi, M.; Veronese, N.; Correll, C.U.; Favaro, A.; Santonastaso, P.; Caregaro, L.; Vancampfort, D.; Luchini, C.; De Hert, M.; Stubbs, B. Bone mineral density, osteoporosis, and fractures among people with eating disorders: A systematic review and meta-analysis. Acta Psychiatr. Scand. 2016, 133, 341–351. [Google Scholar] [CrossRef]
- Forcinito, P.; Andrade, A.C.; Finkielstain, G.P.; Baron, J.; Nilsson, O.; Lui, J.C. Growth-inhibiting conditions slow growth plate senescence. J. Endocrinol. 2011, 208, 59–67. [Google Scholar] [CrossRef]
- Downey, A.E.; Richards, A.; Tanner, A.B. Linear growth in young people with restrictive eating disorders: “Inching” toward consensus. Front. Psychiatry 2023, 14, 1094222. [Google Scholar] [CrossRef]
- Neale, J.; Pais, S.M.A.; Nicholls, D.; Chapman, S.; Hudson, L.D. What Are the Effects of Restrictive Eating Disorders on Growth and Puberty and Are Effects Permanent? A Systematic Review and Meta-Analysis. J. Adolesc. Health 2020, 66, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Swenne, I. Changes in body weight and body mass index (BMI) in teenage girls prior to the onset and diagnosis of an eating disorder. Acta Paediatr. 2001, 90, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Herpertz-Dahlmann, B.; Dahmen, B. Children in Need-Diagnostics, Epidemiology, Treatment and Outcome of Early Onset Anorexia Nervosa. Nutrients 2019, 11, 1932. [Google Scholar] [CrossRef]
- Cole, T.J.; Green, P.J. Smoothing Reference centile curves: The LMS Method and penelized Likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef]
- Rosario, A.S.; Kurth, B.M.; Stolzenberg, H.; Ellert, U.; Neuhauser, H. Body mass index percentiles for children and adolescents in Germany based on a nationally representative sample (KiGGS 2003–2006). Eur. J. Clin. Nutr. 2010, 64, 341–349. [Google Scholar] [CrossRef]
- Hemmelmann, C.; Brose, S.; Vens, M.; Hebebrand, J.; Ziegler, A. Perzentilen des Body-Mass-Index auch für 18- bis 80-Jährige? Daten der Nationalen Verzehrsstudie II. Dtsch. Med. Wochenschr. 2010, 135, 848–852. [Google Scholar] [CrossRef]
- Kromeyer-Hausschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Percentiles of body mass index in children and adolescents evaluated from different regional German studies. Monatsschrift Kinderheilkd. 2001, 149, 807–818. [Google Scholar]
- Jacobi, W.G. Loess: A nonparametric, graphical tool for depicting relationships between variables. Electroral. Stud. 2000, 19, 577–613. [Google Scholar] [CrossRef]
- Benjamin, D.J.; Berger, J.O.; Johannesson, M.; Nosek, B.A.; Wagenmakers, E.J.; Berk, R.; Bollen, K.A.; Brembs, B.; Brown, L.; Camerer, C.; et al. Redefine statistical significance. Nat. Hum. Behav. 2018, 2, 6–10. [Google Scholar] [CrossRef]
- Fisher, M.; Schneider, M.; Burns, J.; Symons, H.; Mandel, F.S. Differences between adolescents and young adults at presentation to an eating disorders program. J. Adolesc. Health 2001, 28, 222–227. [Google Scholar] [CrossRef]
- Peters, T.; Kolar, D.; Focker, M.; Buhren, K.; Dahmen, B.; Becker, K.; Weber, L.; Correll, C.U.; Jaite, C.; Egberts, K.M.; et al. Reasons for admission and variance of body weight at referral in female inpatients with anorexia nervosa in Germany. Child Adolesc. Psychiatry Ment. Health 2021, 15, 78. [Google Scholar] [CrossRef]
- Yang, Y.C.; Walsh, C.E.; Johnson, M.P.; Belsky, D.W.; Reason, M.; Curran, P.; Aiello, A.E.; Chanti-Ketterl, M.; Harris, K.M. Life-course trajectories of body mass index from adolescence to old age: Racial and educational disparities. Proc. Natl. Acad. Sci. USA 2021, 118, e2020167118. [Google Scholar] [CrossRef]
- Schmidt, U.; Adan, R.; Böhm, I.; Campbell, I.C.; Dingemans, A.; Ehrlich, S.; Elzakkers, I.; Favaro, A.; Giel, K.; Harrison, A.; et al. Eating disorders: The big issue. Lancet Psychiatry 2016, 3, 313–315. [Google Scholar] [CrossRef]
- Arcelus, J.; Bouman, W.P.; Morgan, J.F. Treating young people with eating disorders: Transition from child mental health to specialist adult eating disorder services. Eur. Eat. Disord. Rev. 2008, 16, 30–36. [Google Scholar] [CrossRef]
- Winston, A.P.; Paul, M.; Juanola-Borrat, Y. The same but different? Treatment of anorexia nervosa in adolescents and adults. Eur. Eat Disord. Rev. 2012, 20, 89–93. [Google Scholar] [CrossRef]
- Arcelus, J.; Button, E. Clinical and socio-demographic characteristics of university students referred to an eating disorders service. Eur. Eat. Disord. Rev. 2007, 15, 146–151. [Google Scholar] [CrossRef]
- Glasofer, D.R.; Muratore, A.F.; Attia, E.; Wu, P.; Wang, Y.; Minkoff, H.; Rufin, T.; Walsh, B.T.; Steinglass, J.E. Predictors of illness course and health maintenance following inpatient treatment among patients with anorexia nervosa. J. Eat. Disord. 2020, 8, 69. [Google Scholar] [CrossRef]
- Treasure, J.; Stein, D.; Maguire, S. Has the time come for a staging model to map the course of eating disorders from high risk to severe enduring illness? An examination of the evidence. Early Interv. Psychiatry 2015, 9, 173–184. [Google Scholar] [CrossRef]
- American Psychiatric Association. The American Psychiatric Association Practice Guideline for the Treatment of Patients with Eating Disorders; American Psychiatric Association: Washington, DC, USA, 2023. [Google Scholar]
- Agüera, Z.; Romero, X.; Arcelus, J.; Sánchez, I.; Riesco, N.; Jiménez-Murcia, S.; González-Gómez, J.; Granero, R.; Custal, N.; Montserrat-Gil de Bernabé, M.; et al. Changes in Body Composition in Anorexia Nervosa: Predictors of Recovery and Treatment Outcome. PLoS ONE 2015, 10, e0143012. [Google Scholar] [CrossRef]
- Mika, C.; Herpertz-Dahlmann, B.; Heer, M.; Holtkamp, K. Improvement of nutritional status as assessed by multifrequency BIA during 15 weeks of refeeding in adolescent girls with anorexia nervosa. J. Nutr. 2004, 134, 3026–3030. [Google Scholar] [CrossRef]
- Polito, A.; Cuzzolaro, M.; Raguzzini, A.; Censi, L.; Ferro-Luzzi, A. Body composition changes in anorexia nervosa. Eur. J. Clin. Nutr. 1998, 52, 655–662. [Google Scholar] [CrossRef]
- Yamashita, S.; Kawai, K.; Yamanaka, T.; Inoo, T.; Yokoyama, H.; Morita, C.; Takii, M.; Kubo, C. BMI, body composition, and the energy requirement for body weight gain in patients with anorexia nervosa. Int. J. Eat. Disord. 2010, 43, 365–371. [Google Scholar] [CrossRef]
- Mayer, L.E.; Roberto, C.A.; Glasofer, D.R.; Etu, S.F.; Gallagher, D.; Wang, J.; Heymsfield, S.B.; Pierson, R.N., Jr.; Attia, E.; Devlin, M.J.; et al. Does percent body fat predict outcome in anorexia nervosa? Am. J. Psychiatry 2007, 164, 970–972. [Google Scholar] [CrossRef]
- Hebebrand, J.; Himmelmann, G.W.; Herzog, W.; Herpertz-Dahlmann, B.M.; Steinhausen, H.C.; Amstein, M.; Seidel, R.; Deter, H.C.; Remschmidt, H.; Schäfer, H. Prediction of low body weight at long-term follow-up in acute anorexia nervosa by low body weight at referral. Am. J. Psychiatry 1997, 154, 566–569. [Google Scholar] [CrossRef]
- Huas, C.; Godart, N.; Foulon, C.; Pham-Scottez, A.; Divac, S.; Fedorowicz, V.; Peyracque, E.; Dardennes, R.; Falissard, B.; Rouillon, F. Predictors of dropout from inpatient treatment for anorexia nervosa: Data from a large French sample. Psychiatry Res. 2011, 185, 421–426. [Google Scholar] [CrossRef]
- Dietz, W.H.; Robinson, T.N. Use of the body mass index (BMI) as a measure of overweight in children and adolescents. J. Pediatr. 1998, 132, 191–193. [Google Scholar] [CrossRef]
- Gray, D.S. Diagnosis and prevalence of obesity. Med. Clin. N. Am. 1989, 73, 1–13. [Google Scholar] [CrossRef]
- Watson, P.E.; Watson, I.D.; Batt, R.D. Obesity indices. Am. J. Clin. Nutr. 1979, 32, 736–737. [Google Scholar] [CrossRef]
- Metcalf, B.S.; Hosking, J.; Frémeaux, A.E.; Jeffery, A.N.; Voss, L.D.; Wilkin, T.J. BMI was right all along: Taller children really are fatter (implications of making childhood BMI independent of height) EarlyBird 48. Int. J. Obes. 2011, 35, 541–547. [Google Scholar] [CrossRef]
- Sperrin, M.; Marshall, A.D.; Higgins, V.; Renehan, A.G.; Buchan, I.E. Body mass index relates weight to height differently in women and older adults: Serial cross-sectional surveys in England (1992–2011). J. Public Health 2016, 38, 607–613. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Adolescents | Adults | |
|---|---|---|---|
| n | 2372 | 1001 | 1371 |
| AN (ICD-10: F50.0) | 1454 | 623 | 831 |
| Age (mean ± SD; range) | 22.20 ± 9.78; 12–73 | 15.49 ± 1.26; 12–17 | 27.1 ± 10.36; 18–73 |
| BMI (mean ± SD; range) | 14.77 ± 1.80; 8.28–18.47 | 14.95 ± 1.43; 10.67–18.47 | 14.63 ± 2.02; 8.28–18.47 |
| BMI-SDS | −4.21 ± 2.18; −18.81–−1.29 | −3.39 ± 1.43; −11.21–−1.29 | −4.81 ± 2.44; −18.80–−1.4 |
| Duration of illness (years; mean ± SD; range) * | 5.82 ± 7.49; 0–50 | 2.07 ± 1.26; 0–8 | 8.58 ± 8.70; 0–45 |
| n (%) Adolescents | n (%) Adults | |
|---|---|---|
| BMI 8–9.99 kg/m2 | 0 | 20 (1.5) |
| BMI 10–10.99 kg/m2 | 2 (0.2) | 42 (3.1) |
| BMI 11–11.99 kg/m2 | 16 (1.6) | 96 (7.0) |
| BMI 12–12.99 kg/m2 | 71 (7.1) | 123 (9.0) |
| BMI ≥ 13 kg/m2 | 912 (91.19) | 1090 (79.5) |
| Dependent Variable: BMI-SDS | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Equation | Model Overview | Estimation of Parameters | |||||||
| R2 | F | df1 | df2 | Sig. | Intercept | b1 | b2 | b3 | |
| Linear | 0.06 | 163.3 | 1 | 2370 | 3.3 × 10−36 | −4.21 | −0.555 | ||
| Quadratic | 0.11 | 143.3 | 2 | 2369 | 1.8 × 10−59 | −4.54 | −1.19 | 0.33 | |
| Cubic | 0.12 | 102.8 | 3 | 2368 | 1.5 × 10−62 | −4.70 | −1.26 | 0.65 | 0.08 |
| Total (n = 2372) | Adolescents (n = 1001) | Adults (n = 1371) | Difference between Correlation Coefficients in Adolescents and Adults: (Row Difference, z-Value, p-Value) | |
|---|---|---|---|---|
| BMI kg/m2 | r = −0.05; p = 0.018 | r = 0.12; p = 2.4 × 10−4 | r = −0.03; p = 0.3 | 0.09, z = 2.16, p = 0.030 |
| BMI-SDS | r = −0.36; p = 9.2 × 10−74 | r = −0.35; p = 2.1 × 10−30 | r = −0.09; p = 0.001 | 0.26, z = 6.61, p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gradl-Dietsch, G.; Peters, T.; Meule, A.; Hebebrand, J.; Voderholzer, U. Body Mass Index Distribution in Female Child, Adolescent and Adult Inpatients with Anorexia Nervosa—A Retrospective Chart Review. Nutrients 2024, 16, 1732. https://doi.org/10.3390/nu16111732
Gradl-Dietsch G, Peters T, Meule A, Hebebrand J, Voderholzer U. Body Mass Index Distribution in Female Child, Adolescent and Adult Inpatients with Anorexia Nervosa—A Retrospective Chart Review. Nutrients. 2024; 16(11):1732. https://doi.org/10.3390/nu16111732
Chicago/Turabian StyleGradl-Dietsch, Gertraud, Triinu Peters, Adrian Meule, Johannes Hebebrand, and Ulrich Voderholzer. 2024. "Body Mass Index Distribution in Female Child, Adolescent and Adult Inpatients with Anorexia Nervosa—A Retrospective Chart Review" Nutrients 16, no. 11: 1732. https://doi.org/10.3390/nu16111732
APA StyleGradl-Dietsch, G., Peters, T., Meule, A., Hebebrand, J., & Voderholzer, U. (2024). Body Mass Index Distribution in Female Child, Adolescent and Adult Inpatients with Anorexia Nervosa—A Retrospective Chart Review. Nutrients, 16(11), 1732. https://doi.org/10.3390/nu16111732