
High-Protein Processed Foods: Impact on Diet, Nutritional Status, and Possible Effects on Health

 , ,
, ,  , ,
, ,  ,
,  , , and
, , and 
Highlights
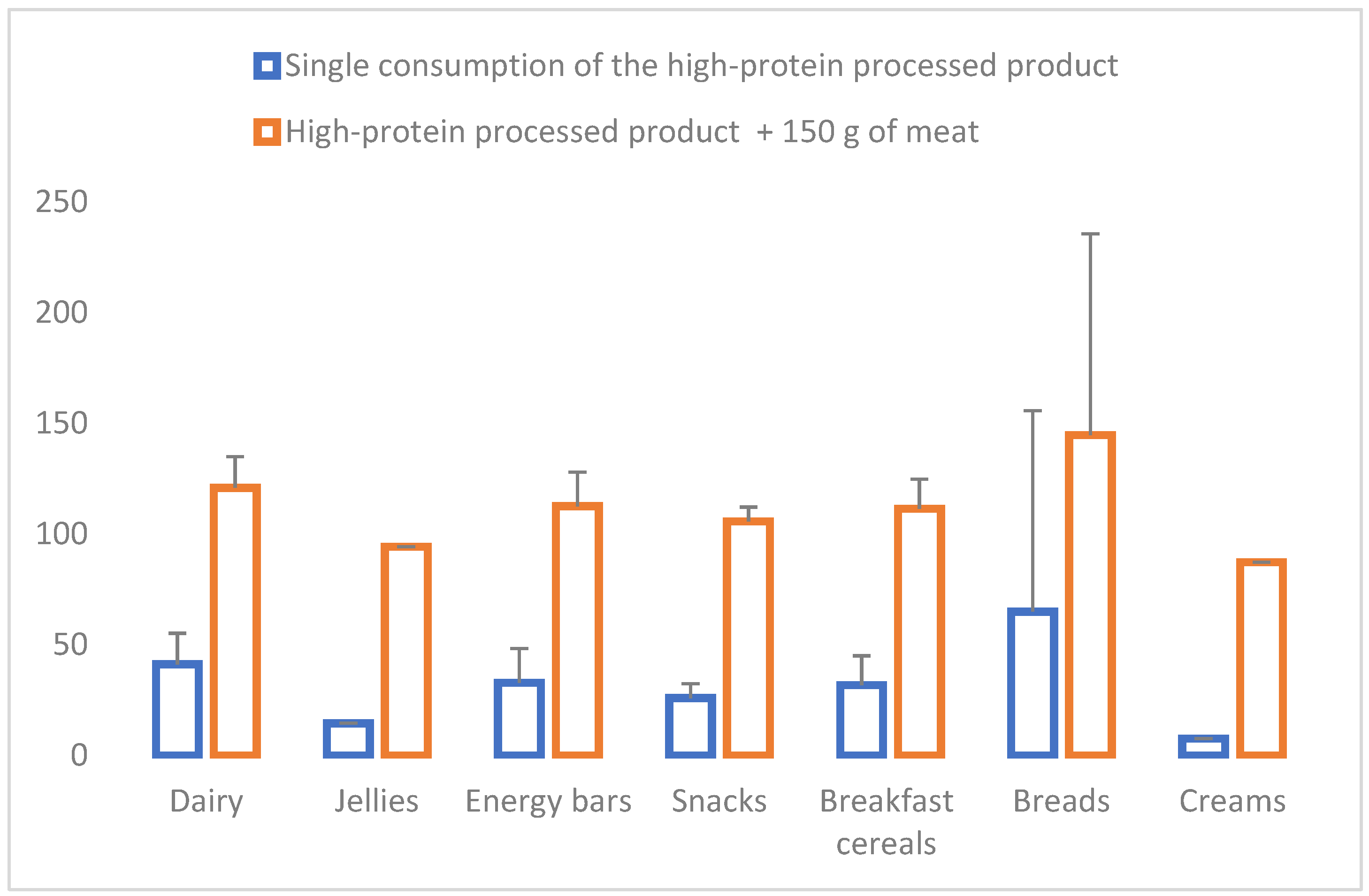
- The massive number of high-protein-enriched foods on offer in supermarket chains may lead to protein overconsumption.
- The increase in protein consumption can cause an imbalance in our diet, possibly negatively affecting health.
- It is relevant to warn consumers about the effect of overconsuming high-protein-enriched foods to ensure that they make informed choices.
- There is a need for authorities to regulate the mass sale of high-protein-enriched foods.
- Health professionals and nutritional advisors should advise on the consumption of high-protein-enriched foods according to needs.
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruiz, E.; Ávila, J.M.; Valero, T.; Del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; et al. Energy Intake, Profile, and Dietary Sources in the Spanish Population: Findings of the ANIBES Study. Nutrients 2015, 7, 4739–4762. [Google Scholar] [CrossRef]
- Winkvist, A.; Klingberg, S.; Nilsson, L.M.; Wennberg, M.; Renström, F.; Hallmans, G.; Boman, K.; Johansson, I. Longitudinal 10-year changes in dietary intake and associations with cardio-metabolic risk factors in the Northern Sweden Health and Disease Study. Nutr. J. 2017, 16, 20. [Google Scholar] [CrossRef]
- Narasaki, Y.; Okuda, Y.; Moore, L.W.; You, A.S.; Tantisattamo, E.; Inrig, J.K.; Miyagi, T.; Nakata, T.; Kovesdy, C.P.; Nguyen, D.V.; et al. Dietary protein intake, kidney function, and survival in a nationally representative cohort. Am. J. Clin. Nutr. 2021, 114, 303–313. [Google Scholar] [CrossRef]
- Norton, V.; Lignou, S.; Methven, L. Influence of Age and Individual Differences on Mouthfeel Perception of Whey Protein-Fortified Products: A Review. Foods 2021, 10, 433. [Google Scholar] [CrossRef]
- Prokopidis, K.; Mazidi, M.; Sankaranarayanan, R.; Tajik, B.; McArdle, A.; Isanejad, M. Effects of whey and soy protein supplementation on inflammatory cytokines in older adults: A systematic review and meta-analysis. Br. J. Nutr. 2023, 129, 759–770. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary Reference Values for protein EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). EFSA J. 2012, 10, 2557. [Google Scholar] [CrossRef]
- Darling, A.L.; Millward, D.J.; Lanham-New, S.A. Dietary Protein and Bone Health: Towards a Synthesised View. Proc. Nutr. Soc. 2021, 80, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Mittendorfer, B.; Klein, S.; Fontana, L. A word of caution against excessive protein intake. Nat. Rev. Endocrinol. 2020, 16, 59–66. [Google Scholar] [CrossRef]
- Martin-Hadmaș, R.M.; Martin Ștefan, A.; Romonți, A.; Mărginean, C.O. The Effect of Dietary Intake and Nutritional Status on Anthropometric Development and Systemic Inflammation: An Observational Study. Int. J. Environ. Res. Public. Health 2021, 18, 5635. [Google Scholar] [CrossRef]
- Blachier, F.; Beaumont, M.; Portune, K.J.; Steuer, N.; Lan, A.; Audebert, M.; Khodorova, N.; Andriamihaja, M.; Airinei, G.; Benamouzig, R.; et al. High-protein diets for weight management: Interactions with the intestinal microbiota and consequences for gut health. A position paper by the my new gut study group. Clin. Nutr. 2019, 38, 1012–1022. [Google Scholar] [CrossRef]
- Rendón Rodríguez, R. Efectos de las dietas hiperproteicas sobre la función renal: Una controversia actual. Nutr. Clínica En Med. 2018, 12, 149–162. [Google Scholar]
- Bilancio, G.; Cavallo, P.; Ciacci, C.; Cirillo, M. Dietary Protein, Kidney Function and Mortality: Review of the Evidence from Epidemiological Studies. Nutrients 2019, 11, 196. [Google Scholar] [CrossRef]
- Rafieian-Kopaei, M.; Beigrezaei, S.; Nasri, H.; Kafeshani, M. Soy Protein and Chronic Kidney Disease: An Updated Review. Int. J. Prev. Med. 2017, 8, 105. [Google Scholar]
- Tahreem, A.; Rakha, A.; Rabail, R.; Nazir, A.; Socol, C.T.; Maerescu, C.M.; Aadil, R.M. Fad Diets: Facts and Fiction. Front. Nutr. 2022, 9, 960922. [Google Scholar] [CrossRef]
- Teymoori, F.; Asghari, G.; Mirmiran, P.; Azizi, F. Dietary amino acids and incidence of hyper-tension: A principle component analysis approach. Sci. Rep. 2017, 7, 16838. [Google Scholar] [CrossRef]
- Varela-Moreiras, G.; Ruiz, E.; Valero, T.; Ávila, J.M.; del Pozo, S. The Spanish diet: An update. Nutr. Hosp. 2013, 28, 13–20. [Google Scholar]
- López-Sobaler, A.M.; Aparicio, A.; Rubio, J.; Marcos, V.; Sanchidrian, R.; Santos, S.; Pérez-Farinós, N.; Dal-Re, M.A.; Villar-Villalba, C.; Yusta-Boyo, M.J.; et al. Adequacy of usual macronutrient intake and macronutrient distribution in children and adolescents in Spain: A National Dietary Survey on the Child and Adolescent Population, ENALIA 2013-2014. Eur. J. Nutr. 2019, 58, 705–719. [Google Scholar] [CrossRef]
- Madrigal, C.; Soto-Méndez, M.J.; Hernández-Ruiz, Á.; Valero, T.; Villoslada, F.L.; Leis, R.; Martínez de Victoria, E.; Moreno, J.M.; Ortega, R.M.; Ruiz-López, M.D.; et al. Dietary Intake, Nutritional Adequacy, and Food Sources of Protein and Relationships with Personal and Family Factors in Spanish Children Aged One to <10 Years: Findings of the EsNuPI Study. Nutrients 2021, 13, 1062. [Google Scholar] [CrossRef]
- Jabeen, S.; Javed, F.; Hettiarachchy, N.S.; Sahar, A.; Sameen, A.; Khan, M.R.; Siddeeg, A.; Riaz, A.; Aadil, R.M. Development of energy-rich protein bars and in vitro determination of angiotensin I-converting enzyme inhibitory antihypertensive activities. Food Sci. Nutr. 2022, 10, 1239–1247. [Google Scholar] [CrossRef]
- Arenas-Jal, M.; Suñé-Negre, J.M.; Pérez-Lozano, P.; García-Montoya, E. Trends in the food and sports nutrition industry: A review. Crit. Rev. Food Sci. Nutr. 2020, 60, 2405–2421. [Google Scholar] [CrossRef]
- Ortega, R.M.; Requejo, A.M.; Navia, B.; López Sobaler, A.M.; Aparicio, A. Ingestas Diarias Recomendadas de Energía y Nutrientes Para la Población Española; Departamento de Nutrición y Ciencia de los Alimentos, Facultad de Farmacia: Madrid, Spain, 2019. [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Ingestas Diarias Recomendadas de Energía y Nutrientes Para la Población Española. In Tablas de Composición de Alimentos, 18th ed.; Grupo Anaya: Madrid, Spain, 2016. [Google Scholar]
- European Food Safety Authority. Dietary Reference Intakes (VDR). 2019. Available online: https://www.efsa.europa.eu/en/interactive-pages/drvs (accessed on 10 July 2023).
- Tuni, O.M.; Carbajal, Á.; Forneiro, L.C.; Vives, C.C. Tablas de Composición de Alimentos; Grupo Anaya: Madrid, España, 2022; pp. 1–520. [Google Scholar]
- EU Parliament. C1 Regulation (EC) No 1924/2006 of the European Parliament and of the Council of 20 December 2006 on Nutrition and Health Claims made on Foods; EU Parliament: Strasbourg, France, 2006. [Google Scholar]
- Ly, J.L.; Wu, Q.J.; Li, X.Y.; Gao, C.; Xu, M.Z.; Yang, J.; Zang, S.T.; Luan, J.; Cai, D.Z.; Chang, Q.; et al. Dietary protein and multiple health outcomes: An umbrella review of systematic reviews and meta-analyses of observational studies. Clin. Nutr. 2022, 41, 759–1769. [Google Scholar]
- Chen, Z.; Glisic, M.; Song, M.; Aliahmad, H.A.; Zhang, X.; Moumdjian, A.C.; Gonzalez-Jaramillo, V.; van der Schaft, N.; Bramer, W.M.; Ikram, M.A.; et al. Dietary protein intake and all-cause and cause-specific mortality: Results from the Rotterdam Study and a meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2020, 35, 411–429. [Google Scholar] [CrossRef]
- Santesso, N.; Akl, E.A.; Bianchi, M.; Mente, A.; Mustafa, R.; Heels-Ansdell, D.; Schünemann, H.J. Effects of higher- versus lower-protein diets on health outcomes: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 780–788. [Google Scholar] [CrossRef]
- Vogtschmidt, Y.D.; Raben, A.; Faber, I.; de Wilde, C.; Lovegrove, J.A.; Givens, D.I.; Pfeiffer, A.F.H.; Soedamah-Muthu, S.S. Is protein the forgotten ingredient: Effects of higher compared to lower protein diets on cardiometabolic risk factors. A systematic review and meta-analysis of randomised controlled trials. Atherosclerosis 2021, 328, 124–135. [Google Scholar] [CrossRef]
- Rabassa-Blanco, J.; Palma-Linares, I. Efectos de los suplementos de proteína y aminoácidos de cadena ramificada en entrenamiento de fuerza: Revisión bibliográfica. Rev. Esp. Nutr. Hum. Diet. 2017, 21, 55–73. [Google Scholar] [CrossRef]
- Guefai, F.Z.; Martínez-Rodríguez, A.; Grindlay, G.; Mora, J.; Gras, L. Elemental bioavailability in whey protein supplements. J. Food Compos. Anal. 2022, 112, 104696. [Google Scholar] [CrossRef]
- Sepandi, M.; Samadi, M.; Shirvani, H.; Alimohamadi, Y.; Taghdir, M.; Goudarzi, F.; Akbarzadeh, I. Effect of whey protein supplementation on weight and body composition indicators: A meta-analysis of randomized clinical trials. Clin. Nutr. ESPEN 2022, 50, 74–83. [Google Scholar] [CrossRef]
- Li, M.L.; Zhang, F.; Luo, H.Y.; Quan, Z.W.; Wang, Y.F.; Huang, L.T.; Wang, J.H. Improving sarcopenia in older adults: A systematic review and meta-analysis of randomized controlled trials of whey protein supplementation with or without resistance training. J. Nutr. Health Aging 2024, 28, 100184. [Google Scholar] [CrossRef] [PubMed]
- Cava, E.; Padua, E.; Campaci, D.; Bernardi, M.; Muthanna, F.M.S.; Caprio, M.; Lombardo, M. Investigating the Health Implications of Whey Protein Consumption: A Narrative Review of Risks, Adverse Effects, and Associated Health Issues. Healthcare 2024, 12, 246. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Kind of Product | Brand | Proteins (g/100 g EP) | Proteins (g/100 g NEP) | Container/Serving Size (g or mL) | Proteins (g/Container or Serving) | Energy/Container or Serving (kcal) | Energy (from Proteins)/Container or Serving (kcal) | Energy (from Proteins)/Container or Serving (%) | RDI Proteins/Container or Serving (%) 3 | PRI Proteins/Container or Serving (%) 4 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Woman | Man | Woman | Man | |||||||||
| Dairy | ||||||||||||
| Yoghurts | LIDL 1 | 10.0 | 3.3 | 200.0 | 20.0 | 130.0 | 80.0 | 61.5 | 48.8 | 37.0 | 43.8 | 34.4 |
| Mercadona 2 | 8.3 | 120.0 | 10.0 | 64.0 | 40.0 | 62.5 | 24.4 | 18.5 | 21.9 | 17.2 | ||
| Yopro | 9.4 | 160.0 | 15.0 | 88.0 | 60.0 | 68.2 | 36.6 | 27.8 | 32.9 | 25.8 | ||
| Milkshakes | LIDL 1 | 10.5 | 3.9 | 166.0 | 17.4 | 109.0 | 69.6 | 63.8 | 42.4 | 32.2 | 38.1 | 29.9 |
| Mercadona 2 | 7.9 | 330.0 | 26.0 | 151.0 | 104.0 | 68.9 | 63.4 | 48.1 | 57.0 | 44.7 | ||
| Yopro | 6.0 | 330.0 | 15.0 | 118.0 | 60.0 | 50.8 | 36.6 | 27.8 | 32.9 | 25.8 | ||
| Prozis | 6.0 | 250.0 | 15.0 | 90.0 | 60.0 | 66.7 | 36.6 | 27.8 | 32.9 | 25.8 | ||
| Drinkable yoghurt | Mercadona 2 | 7.1 | 3.0 | 280.0 | 20.0 | 143.0 | 80.0 | 55.9 | 48.8 | 37.0 | 43.8 | 34.4 |
| Yopro | 8.3 | 300.0 | 25.0 | 177.0 | 100.0 | 56.5 | 61.0 | 46.3 | 54.8 | 43.0 | ||
| Ice creams | LIDL 1 | 7.6 | 3.5 | 45.5 | 3.5 | 116.0 | 14.0 | 12.1 | 8.5 | 6.5 | 7.7 | 6.0 |
| Mercadona 2 | 9.3 | 265.0 | 24.6 | 389.0 | 98.4 | 25.3 | 60.0 | 45.6 | 53.9 | 42.3 | ||
| Mousses | Mercadona 2 | 10.0 | 4.1 | 200.0 | 20.0 | 152.0 | 80.0 | 52.6 | 48.8 | 37.0 | 43.8 | 34.4 |
| Yopro | 10.1 | 200.0 | 20.0 | 155.0 | 80.0 | 51.6 | 48.8 | 37.0 | 43.8 | 34.4 | ||
| Valio profeel | 12.0 | 150.0 | 18.0 | 130.5 | 72.0 | 55.2 | 43.9 | 33.3 | 39.4 | 31.0 | ||
| Reina | 10.0 | 100.0 | 10.0 | 123.0 | 40.0 | 32.5 | 24.4 | 18.5 | 21.9 | 17.2 | ||
| Milk | Mercadona 2 | 6. 0 | 3.9 | 250.0 | 15.0 | 142.0 | 60.0 | 42.2 | 36.6 | 27.8 | 32.9 | 25.8 |
| Custards | Mercadona 2 | 10.0 | 5.0 | 120.0 | 12.0 | 92.0 | 48.0 | 52.2 | 29.3 | 22.2 | 26.3 | 20.6 |
| Pudding | Yopro | 10.0 | 3.2 | 180.0 | 18.0 | 82.0 | 72.0 | 87.8 | 43.9 | 33.3 | 39.4 | 31.0 |
| Jellies | ||||||||||||
| Jelly | Carrefour | 6.0 | 0.0 | 100.0 | 6.00 | 30.0 | 24.0 | 80.0 | 14.6 | 11.1 | 13.1 | 10.3 |
| Mercadona | 6.0 | 100.0 | 6.00 | 39.0 | 24.0 | 61.5 | 14.6 | 11.1 | 13.1 | 10.3 | ||
| Energy bars | ||||||||||||
| Bar | LIDL | 50.0 | 5.7 | 45.0 | 22.5 | 164.0 | 90.0 | 54.9 | 54.9 | 41.7 | 49.3 | 38.7 |
| Prozis | 30.0 | 35.0 | 10.5 | 140.0 | 42.0 | 30.0 | 25.6 | 19.4 | 23.0 | 18.1 | ||
| Foodspring | 29.0 | 45.0 | 13.0 | 157.0 | 52.0 | 33.1 | 31.7 | 24.1 | 28.5 | 22.4 | ||
| El almendro | 24.0 | 35.0 | 8.0 | 180.0 | 32.0 | 17.8 | 19.5 | 14.8 | 17.5 | 13.8 | ||
| Snacks | ||||||||||||
| Chips | PROZIS | 45.0 | 6.5 | 25.0 | 11.2 | 100.7 | 45.0 | 44.7 | 27.4 | 20.8 | 24.64 | 19.36 |
| Muffin | Prozis | 13.0 | 3.5 | 60.00 | 7.80 | 175.2 | 31.2 | 17.8 | 19.0 | 14.4 | 17.1 | 13.4 |
| Cookie | Foodspring | 26.0 | 6.0 | 50.0 | 13.0 | 227.0 | 52.0 | 22.9 | 31.7 | 24.1 | 28.5 | 22.4 |
| Breakfast cereal | ||||||||||||
| Muesli | Prozis | 23.0 | 7.0 | 40.0 | 9.2 | 159.4 | 36.8 | 23.1 | 22.4 | 17.0 | 20.1 | 15.8 |
| Foodspring | 28.2 | 7.0 | 60.0 | 16.9 | 263.0 | 67.6 | 25.7 | 41.2 | 31.3 | 37.0 | 29.1 | |
| Breads | ||||||||||||
| Bread | Prozis | 17.0 | 11.0 | 30.0 | 5.1 | 73.5 | 20.4 | 27.7 | 12.4 | 9.4 | 11.2 | 8.8 |
| Keto protein | 27.0 | 50.0 | 13.5 | 116.0 | 54.0 | 46.5 | 32.9 | 25.0 | 29.6 | 23.2 | ||
| Toasts | Mercadona | 46.5 | 10.0 | 200.0 | 93.0 | 818.0 | 186.0 | 22.7 | 226.8 | 172.2 | 203.7 | 160.1 |
| Wheat tortillas | Keto protein | 22.0 | 7.0 | 40.0 | 8.8 | 127.0 | 35.2 | 27.7 | 21.5 | 16.3 | 19.3 | 15.1 |
| Pizza dough | Keto protein | 28.0 | 6.50 | 45.0 | 13.0 | 110.0 | 52.0 | 47.3 | 31.7 | 24.1 | 28.5 | 22.4 |
| Creams | ||||||||||||
| Cocoa cream | Prozis | 21.0 | 6.3 | 15.0 | 3.1 | 77.4 | 12.6 | 16.3 | 7.7 | 5.8 | 6.9 | 5.4 |
| Hazelnut cream | Foodspring | 21.0 | 6.3 | 15.0 | 3.1 | 79.5 | 12.6 | 15.8 | 7.7 | 5.8 | 6.9 | 5.4 |
| Kind of Product | Brand | Type of Added Protein | Claim/Statement | Indication of Whom the Product Is Intended for (Yes/No) |
|---|---|---|---|---|
| Dairy | ||||
| Yoghurts | LIDL 1 | DWP | Lactose-free and low in fat | NO |
| Mercadona 2 | DWP | 0% fat, gluten free | NO | |
| Yopro | DWP | 0% fat, 0% added sugar, without artificial colourings or preservatives | Athletes, it indicates that it is ideal to enhance training | |
| Milkshakes | LIDL 1 | DWP | Gluten-free, no added sugar, and low in fat | NO |
| Mercadona 2 | DWP | Source of vitamin B6, lactose-free, and without added sugars | NO | |
| Yopro | DWP | 0% fat, 0% added sugar, without colourings or preservatives | Athletes, it indicates that it is ideal to enhance training | |
| Prozis | DWP | Low fat | Children, seniors, athletes, busy professionals, and weight loss programs | |
| Drinkable yoghurt o | Mercadona 2 | DWP | 0% fat, gluten free | NO |
| Yopro | DWP | 0% fat, 0% added sugar, without artificial colourings or preservatives, without lactose | Athletes, it indicates that it is ideal to enhance training | |
| Ice creams | LIDL 1 | DWP | No added sugars | NO |
| Mercadona 2 | DWP | NO | NO | |
| Mousses | Mercadona 2 | DWP, animal jelly | Lactose-free | NO |
| Yopro | DWP, animal jelly | Low fat, 0% added sugars | Athletes, it indicates that it is ideal to enhance training | |
| Valio profeel | DWP | Rich in protein, added sugars free and lactose-free | NO | |
| Reina | DWP | High in protein, low fat, 0% added sugar | NO | |
| Milk | Mercadona 2 | DWP | Lactose-free. Enriched with protein and calcium | NO |
| Custards | Mercadona 2 | DWP | Gluten-free. Source of protein and calcium | NO |
| Pudding | Yopro | DWP | Lactose-free and low in fat | NO |
| Jellies | ||||
| Jelly | Carrefour | Hydrolyzed collagen protein, jelly | High protein content, 0% fat, gluten free | NO |
| Mercadona | Hydrolyzed collagen protein, jelly | Gluten free, 0% fat | NO | |
| Energy bars | ||||
| Bar | LIDL | Mix of proteins 1 | 50% proteins | NO |
| Prozis | DWP | 30% proteins, source of fibre, GMO-free | People who control their diet, athletes, busy people | |
| Foodspring | DWP | No added sugars | Athletes | |
| El almendro | Pea protein extruded 2 | Source of protein, with almonds, source of fibre, gluten-free, palm oil-free | NO | |
| Snacks | ||||
| Chips | Prozis | Soy protein concentrate | High protein content (45%), no added sugars, high fiber content | Athletes, busy people, and people who control their diet |
| Muffin | Prozis | DWP | Low in sugar, source of protein, without aspartame, without artificial colourings | Suitable for all persons |
| Cookie | Foodspring | Wheat protein (gluten) | Low sugar, high protein | NO |
| Breakfast cereal | ||||
| Muesli | Prozis | DWP | High protein content and high fiber content | NO |
| Foodspring | Soybean flakes, almond flakes, extruded soybeans, cashews, toasted hazelnuts, protein sunflower seeds (sunflower protein, rice flour) | High protein content, 100% organic, GMO-free, rich in fibre | NO | |
| Breads | ||||
| Bread | Prozis | Whole wheat flour (gluten), wheat flour, wheat gluten, wheat bran, soybean flakes, barley malt flour | High protein and low carbohydrate | Athletes and weight control |
| Keto protein | Whole wheat flour (gluten), wheat flour, wheat gluten, wheat bran, soybean flakes, barley malt flour | Low in carbohydrates, rich in protein, fibre contribution | Healthy lifestyle, weight control or weight maintenance, sport/bodybuilding | |
| Toasts | Mercadona | Vegetable flours (rice protein, whole rye flour (gluten), whole chickpea flour, hydrolyzed wheat protein (gluten) | Low carb | NO |
| Wheat tortillas | Keto protein | Wheat protein, pea protein, rice protein | Low in carbohydrates, high in protein, low in sugar and high in fibre | Healthy lifestyle, weight control or weight maintenance, sport/bodybuilding |
| Pizza dough | Keto protein | Wheat protein, sunflower seed meal, soy protein | Low in carbohydrates, high in protein, low in sugar and high in fibre | Healthy lifestyle, weight control or weight maintenance, sport/bodybuilding |
| Creams | ||||
| Cocoa cream | Prozis | DWP | No palm oil, reduced salt content, no added sugar, no aspartame, no artificial colourings or preservatives, GMO-free | NO |
| Hazelnut cream | Foodspring | DWP | No added sugar, no palm oil, high protein, and low carbohydrate | NO |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega, R.M.; Arribas-López, N.; Salas-González, M.D.; Aparicio, A.; González-Rodríguez, L.G.; Bermejo, L.M.; Lozano-Estevan, M.D.C.; Cuadrado-Soto, E.; López-Sobaler, A.M.; Loria-Kohen, V. High-Protein Processed Foods: Impact on Diet, Nutritional Status, and Possible Effects on Health. Nutrients 2024, 16, 1697. https://doi.org/10.3390/nu16111697
Ortega RM, Arribas-López N, Salas-González MD, Aparicio A, González-Rodríguez LG, Bermejo LM, Lozano-Estevan MDC, Cuadrado-Soto E, López-Sobaler AM, Loria-Kohen V. High-Protein Processed Foods: Impact on Diet, Nutritional Status, and Possible Effects on Health. Nutrients. 2024; 16(11):1697. https://doi.org/10.3390/nu16111697
Chicago/Turabian StyleOrtega, Rosa M., Nerea Arribas-López, María Dolores Salas-González, Aránzazu Aparicio, Liliana Guadalupe González-Rodríguez, Laura M. Bermejo, María Del Carmen Lozano-Estevan, Esther Cuadrado-Soto, Ana M. López-Sobaler, and Viviana Loria-Kohen. 2024. "High-Protein Processed Foods: Impact on Diet, Nutritional Status, and Possible Effects on Health" Nutrients 16, no. 11: 1697. https://doi.org/10.3390/nu16111697
APA StyleOrtega, R. M., Arribas-López, N., Salas-González, M. D., Aparicio, A., González-Rodríguez, L. G., Bermejo, L. M., Lozano-Estevan, M. D. C., Cuadrado-Soto, E., López-Sobaler, A. M., & Loria-Kohen, V. (2024). High-Protein Processed Foods: Impact on Diet, Nutritional Status, and Possible Effects on Health. Nutrients, 16(11), 1697. https://doi.org/10.3390/nu16111697