
Science and Faith to Understand Milk Bioactivity for Infants


Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction and Rationale
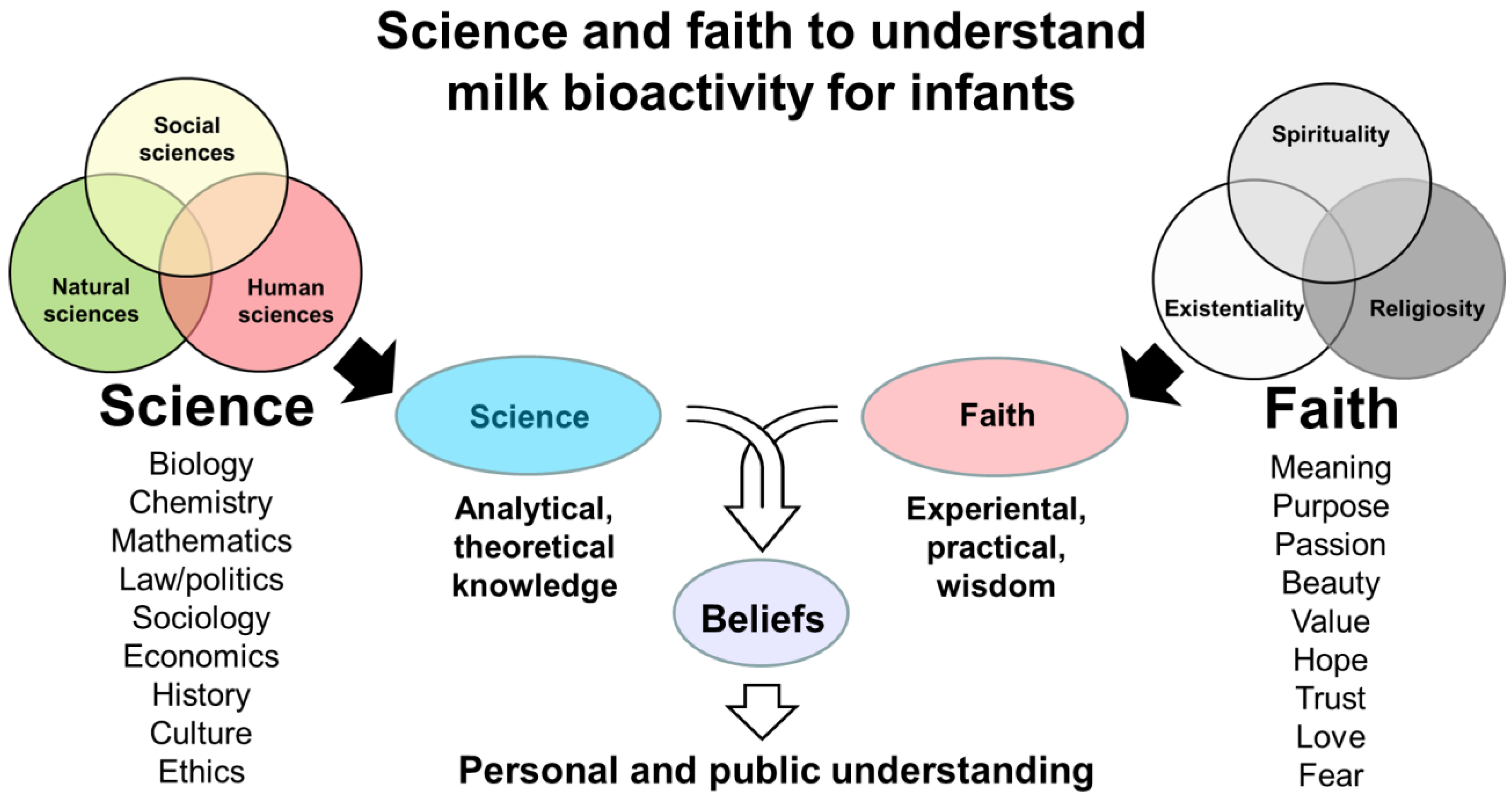
2. Academic Sciences Related to Milk Bioactivity
3. Beliefs and Faiths Related to Milk Bioactivity
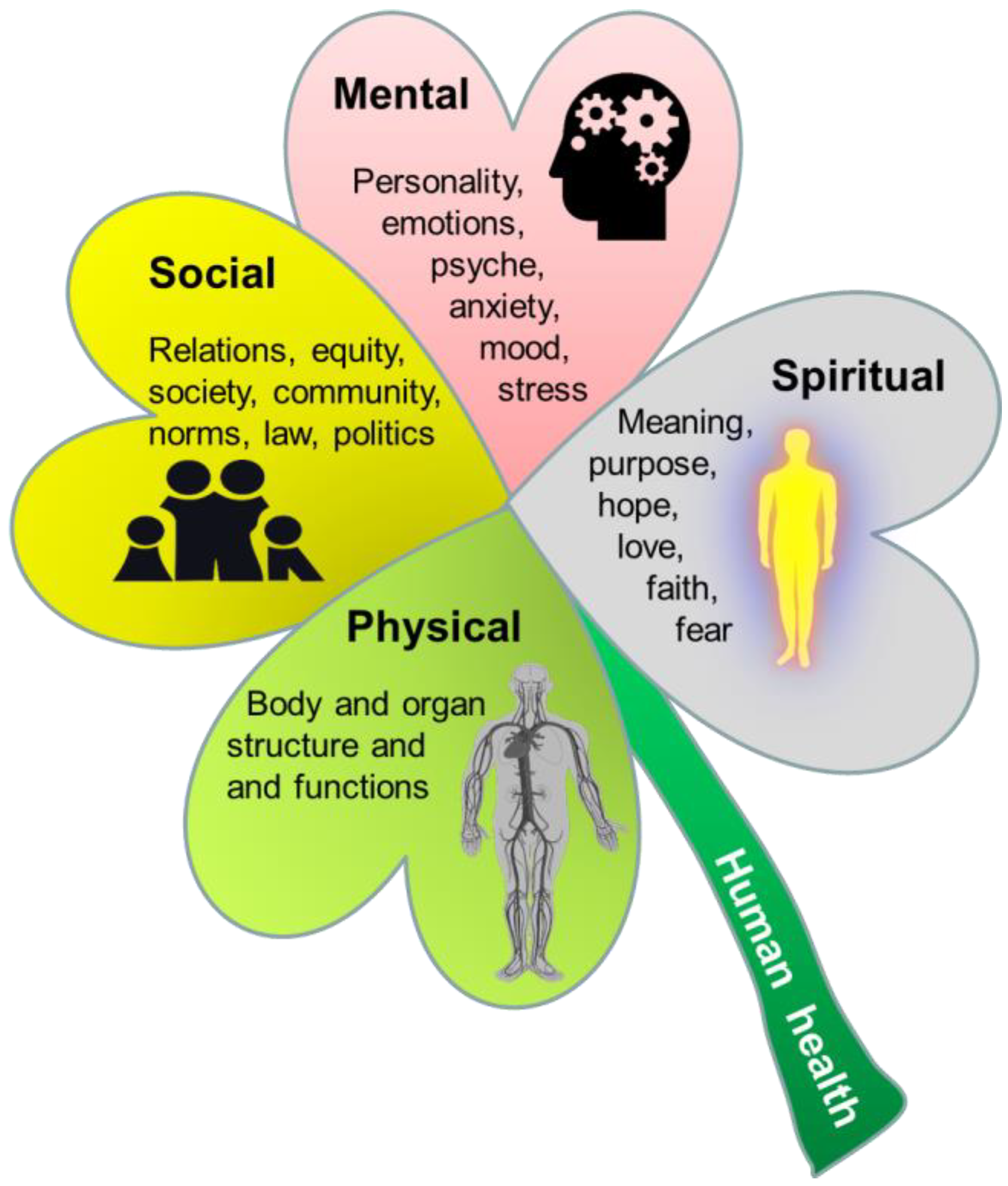
4. Physical, Social, Mental, and Spiritual Dimensions of Human Health
5. Milk Bioactivity in Religions
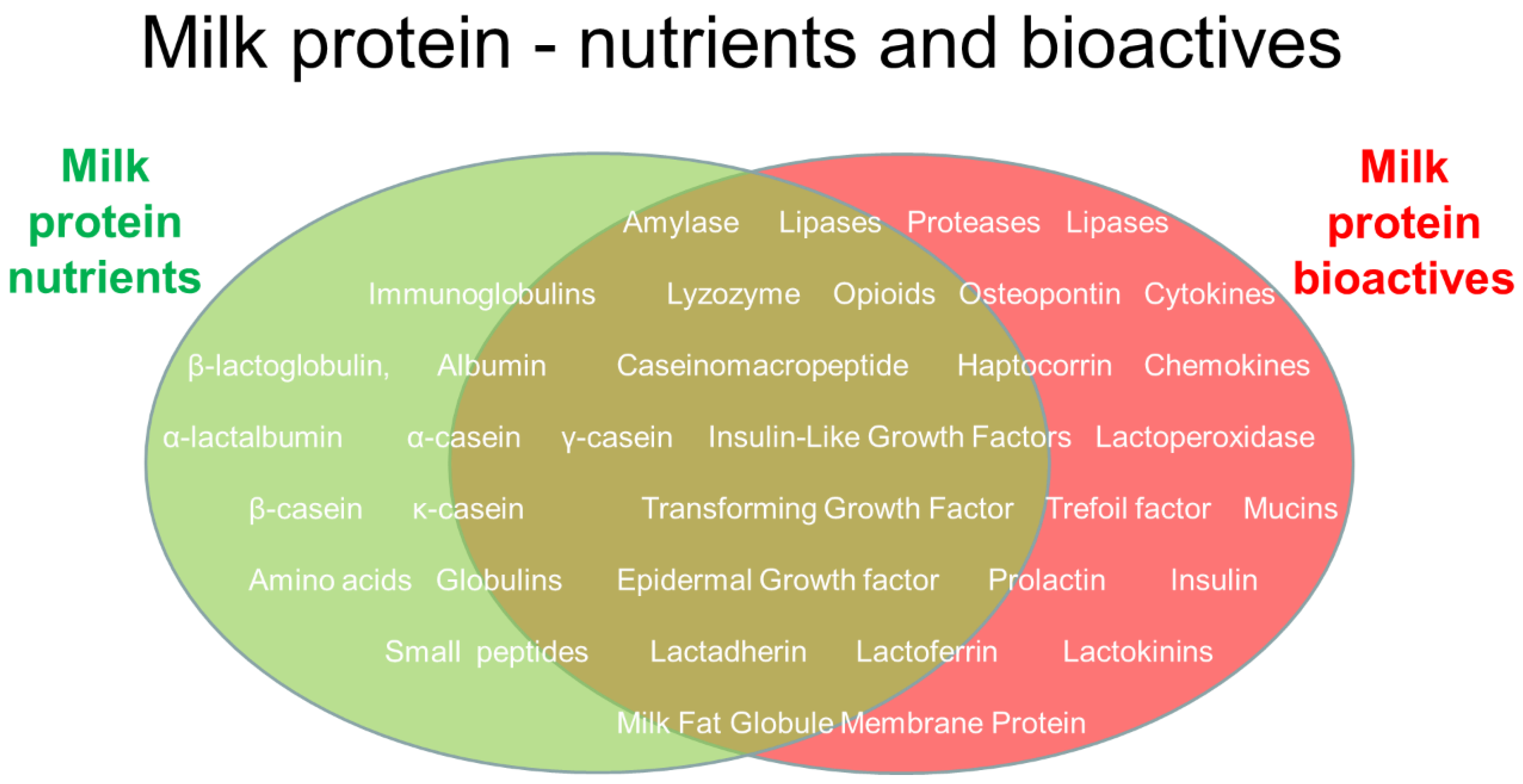
6. Milk Protein Bioactivity and Human Health Interactions
7. Colostrum Bioactivity
8. Infant Formula Bioactivity
9. Bioactivity of Isolated Milk Fractions or Proteins
10. Science, Faith, and Breastfeeding
11. Conflict or Synergy between Scientific Knowledge and Faith Convictions
12. Conclusions and Perspectives
Supplementary Materials
Funding
Acknowledgments
Conflicts of Interest
References
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.E.; Virmani, M.D.; Rosa, F.; Munblit, D.; Matazel, K.S.; Elolimy, A.A.; Yeruva, L. Role of human milk bioactives on infants’ gut and immune health. Front. Immunol. 2021, 12, 604080. [Google Scholar] [CrossRef] [PubMed]
- Chatterton, D.E.; Nguyen, D.N.; Bering, S.B.; Sangild, P.T. Anti-inflammatory mechanisms of bioactive milk proteins in the intestine of newborns. Int. J. Biochem. Cell Biol. 2013, 45, 1730–1747. [Google Scholar] [CrossRef] [PubMed]
- Runehov, A.L.C.; Oviedo, L. (Eds.) Enclocypedia of Sciences and Religion; Springer: Dordrecht, The Netherlands, 2013; p. 2372. [Google Scholar] [CrossRef]
- Kappel, S.S.; Sangild, P.T.; Ahnfeldt, A.M.; Jóhannsdóttir, V.; Soernsen, L.J.; Bak, L.B.; Friborg, C.; Möller, S.; Zachariassen, G.; Aunsholt, L. A randomized, controlled study to investigate how bovine colostrum fortification of human milk affects bowel habits in preterm infants (Forticolos study). Nutrients 2022, 14, 4756. [Google Scholar] [CrossRef] [PubMed]
- Navis, M.; Muncan, V.; Sangild, P.T.; Møller Willumsen, L.; Koelink, P.J.; Wildenberg, M.E.; Abrahamse, E.; Thymann, T.; van Elburg, R.M.; Renes, I.B. Beneficial Effect of Mildly Pasteurized Whey Protein on Intestinal Integrity and Innate Defense in Preterm and Near-Term Piglets. Nutrients 2020, 12, 1125. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, C.H.; Hui, Y.; Nguyen, D.N.; Ahnfeldt, A.M.; Burrin, D.G.; Hartmann, B.; Heckmann, A.B.; Sangild, P.T.; Thymann, T.; Bering, S.B. Alpha-lactalbumin enriched whey protein concentrate to improve gut, immunity and brain development in preterm pigs. Nutrients 2020, 12, 245. [Google Scholar] [CrossRef]
- Obelitz-Ryom, K.; Bering, S.B.; Overgaard, S.H.; Eskildsen, S.F.; Ringgaard, S.; Olesen, J.L.; Skovgaard, K.; Pankratova, S.; Wang, B.; Brunse, A.; et al. Bovine Milk Oligosaccharides with Sialyllactose Improves Cognition in Preterm Pigs. Nutrients 2019, 11, 1335. [Google Scholar] [CrossRef] [PubMed]
- Obelitz-Ryom, K.; Rendboe, A.K.; Nguyen, D.N.; Rudloff, S.; Brandt, A.B.; Nielsen, D.S.; Heckmann, A.B.; Chichlowski, M.; Sangild, P.T.; Thymann, T.; et al. Bovine Milk Oligosaccharides with Sialyllactose for Preterm Piglets. Nutrients 2018, 10, 1489. [Google Scholar] [CrossRef] [PubMed]
- Sangild, P.T.; Vonderohe, C.; Melendez Hebib, V.; Burrin, D.G. Potential benefits of bovine colostrum in pediatric nutrition and health. Nutrients 2021, 13, 2551. [Google Scholar] [CrossRef]
- Wang, X.; Jing, J.; Huang, S.; He, X.; Gao, P.; Li, H.; Lin, Z.; Sangild, P.T.; Zhu, Y. Relationship of Early Anemia with Neurodevelopment and Brain Injury in Very Low Birth Weight Preterm Infants-A Prospective Cohort Study. Nutrients 2022, 14, 4931. [Google Scholar] [CrossRef]
- Aasmul-Olsen, K.; Henriksen, N.L.; Nguyen, D.N.; Heckmann, A.B.; Thymann, T.; Sangild, P.T.; Bering, S.B. Milk osteopontin for gut, immunity and brain development in preterm pigs. Nutrients 2021, 13, 2675. [Google Scholar] [CrossRef] [PubMed]
- Ahnfeldt, A.M.; Aunsholt, L.; Hansen, B.M.; Hoest, B.; Jóhannsdóttir, V.; Kappel, S.S.; Klamer, A.; Möller, S.; Moeller, B.K.; Sangild, P.T.; et al. Bovine colostrum as a fortifier to human milk in very preterm infants—A randomized controlled trial (FortiColos). Clin. Nutr. 2023, 42, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Alinaghi, M.; Jiang, P.P.; Brunse, A.; Sangild, P.T.; Bertram, H.C. Rapid Cerebral Metabolic Shift during Neonatal Sepsis Is Attenuated by Enteral Colostrum Supplementation in Preterm Pigs. Metabolites 2019, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Aunsholt, L.; Jeppesen, P.B.; Lund, P.; Sangild, P.T.; Ifaoui, I.B.; Qvist, N.; Husby, S. Bovine colostrum to children with short bowel syndrome: A randomized, double-blind, crossover pilot study. JPEN J. Parenter. Enter. Nutr. 2014, 38, 99–106. [Google Scholar] [CrossRef]
- Jensen, M.L.; Sangild, P.T.; Lykke, M.; Schmidt, M.; Boye, M.; Jensen, B.B.; Thymann, T. Similar efficacy of human banked milk and bovine colostrum to decrease incidence of necrotizing enterocolitis in preterm piglets. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 305, R4–R12. [Google Scholar] [CrossRef]
- Jiang, P.P.; Muk, T.; Krych, L.; Nielsen, D.S.; Khakimov, B.; Li, Y.; Juhl, S.M.; Greisen, G.; Sangild, P.T. Gut colonization in preterm infants supplemented with bovine colostrum in the first week of life: An explorative pilot study. JPEN J. Parenter. Enter. Nutr. 2022, 46, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Juhl, S.M.; Ye, X.; Zhou, P.; Li, Y.; Iyore, E.O.; Zhang, L.; Jiang, P.; van Goudoever, J.B.; Greisen, G.; Sangild, P.T. Bovine colostrum for preterm infants in the first days of life: A randomized controlled pilot trial. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 471–478. [Google Scholar] [CrossRef]
- Li, Y.; Juhl, S.M.; Ye, X.; Shen, R.L.; Iyore, E.O.; Dai, Y.; Sangild, P.T.; Greisen, G.O. A stepwise, pilot study of bovine colostrum to supplement the first enteral feeding in preterm infants (precolos): Study protocol and initial results. Front. Pediatr. 2017, 5, 42. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Pan, X.; Nguyen, D.N.; Ren, S.; Moodley, A.; Sangild, P.T. Bovine Colostrum Before or After Formula Feeding Improves Systemic Immune Protection and Gut Function in Newborn Preterm Pigs. Front. Immunol. 2019, 10, 3062. [Google Scholar] [CrossRef]
- Lund, P.; Sangild, P.T.; Aunsholt, L.; Hartmann, B.; Holst, J.J.; Mortensen, J.; Mortensen, P.B.; Jeppesen, P.B. Randomised controlled trial of colostrum to improve intestinal function in patients with short bowel syndrome. Eur. J. Clin. Nutr. 2012, 66, 1059–1065. [Google Scholar] [CrossRef]
- Møller, H.K.; Thymann, T.; Fink, L.N.; Frokiaer, H.; Kvistgaard, A.S.; Sangild, P.T. Bovine colostrum is superior to enriched formulas in stimulating intestinal function and necrotising enterocolitis resistance in preterm pigs. Br. J. Nutr. 2011, 105, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.O.; Martin, L.; Østergaard, M.V.; Rudloff, S.; Li, Y.; Roggenbuck, M.; Bering, S.B.; Sangild, P.T. Bovine colostrum improves neonatal growth, digestive function, and gut immunity relative to donor human milk and infant formula in preterm pigs. Am. J. Physiol. Gastrointest. Liver Physiol. 2016, 311, G480–G491. [Google Scholar] [CrossRef] [PubMed]
- Rathe, M.; De Pietri, S.; Wehner, P.S.; Frandsen, T.L.; Grell, K.; Schmiegelow, K.; Sangild, P.T.; Husby, S.; Müller, K. Bovine Colostrum against Chemotherapy-Induced Gastrointestinal Toxicity in Children With Acute Lymphoblastic Leukemia: A Randomized, Double-Blind, Placebo-Controlled Trial. JPEN J. Parenter. Enter. Nutr. 2020, 44, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Rathe, M.; Müller, K.; Sangild, P.T.; Husby, S. Clinical applications of bovine colostrum therapy: A systematic review. Nutr. Rev. 2014, 72, 237–254. [Google Scholar] [CrossRef] [PubMed]
- Shen, R.L.; Thymann, T.; Østergaard, M.V.; Støy, A.C.; Krych, Ł.; Nielsen, D.S.; Lauridsen, C.; Hartmann, B.; Holst, J.J.; Burrin, D.G.; et al. Early gradual feeding with bovine colostrum improves gut function and NEC resistance relative to infant formula in preterm pigs. Am. J. Physiol. Gastrointest. Liver Physiol. 2015, 309, G310–G323. [Google Scholar] [CrossRef] [PubMed]
- Støy, A.C.; Heegaard, P.M.; Thymann, T.; Bjerre, M.; Skovgaard, K.; Boye, M.; Stoll, B.; Schmidt, M.; Jensen, B.B.; Sangild, P.T. Bovine colostrum improves intestinal function following formula-induced gut inflammation in preterm pigs. Clin. Nutr. 2014, 33, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Li, Y.; Pan, X.; Nguyen, D.N.; Brunse, A.; Bojesen, A.M.; Rudloff, S.; Mortensen, M.S.; Burrin, D.G.; Sangild, P.T. Human milk fortification with bovine colostrum is superior to formula-based fortifiers to prevent gut dysfunction, necrotizing enterocolitis, and systemic infection in preterm pigs. JPEN J. Parenter. Enter. Nutr. 2019, 43, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Pan, X.; Ding, L.; Dai, Y.; Chen, J.; Yang, Y.; Li, Y.; Hao, H.; Qiu, H.; Ye, Z.; et al. Bovine colostrum to supplement the first feeding of very preterm infants: The PreColos randomized controlled trial. Clin. Nutr. 2023, 42, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Aasmul-Olsen, K.; Akillioglu, H.G.; Christiansen, L.I.; Engholm-Keller, K.; Brunse, A.; Stefanova, D.V.; Bjornshave, A.; Bechshoft, M.R.; Skovgaard, K.; Thymann, T.; et al. A Gently Processed Skim Milk-Derived Whey Protein Concentrate for Infant Formula: Effects on Gut Development and Immunity in Preterm Pigs. Mol. Nutr. Food. Res. 2024, 68, e2300458. [Google Scholar] [CrossRef]
- Chatterton, D.E.W.; Aagaard, S.; Hesselballe Hansen, T.; Nguyen, D.N.; De Gobba, C.; Lametsch, R.; Sangild, P.T. Bioactive proteins in bovine colostrum and effects of heating, drying and irradiation. Food Funct. 2020, 11, 2309–2327. [Google Scholar] [CrossRef]
- Li, Y.; Nguyen, D.N.; Obelitz-Ryom, K.; Andersen, A.D.; Thymann, T.; Chatterton, D.E.W.; Purup, S.; Heckmann, A.B.; Bering, S.B.; Sangild, P.T. Bioactive Whey Protein Concentrate and Lactose Stimulate Gut Function in Formula-fed Preterm Pigs. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Nguyen, D.N.; de Waard, M.; Christensen, L.; Zhou, P.; Jiang, P.; Sun, J.; Bojesen, A.M.; Lauridsen, C.; Lykkesfeldt, J.; et al. Pasteurization Procedures for Donor Human Milk Affect Body Growth, Intestinal Structure, and Resistance against Bacterial Infections in Preterm Pigs. J. Nutr. 2017, 147, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.N.; Jiang, P.; Stensballe, A.; Bendixen, E.; Sangild, P.T.; Chatterton, D.E. Bovine lactoferrin regulates cell survival, apoptosis and inflammation in intestinal epithelial cells and preterm pig intestine. J. Proteom. 2016, 139, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.N.; Sangild, P.T.; Li, Y.; Bering, S.B.; Chatterton, D.E.W. Processing of whey modulates proliferative and immune functions in intestinal epithelial cells. J. Dairy Sci. 2016, 99, 959–969. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ostergaard, M.V.; Jiang, P.; Chatterton, D.E.; Thymann, T.; Kvistgaard, A.S.; Sangild, P.T. Whey protein processing influences formula-induced gut maturation in preterm pigs. J. Nutr. 2013, 143, 1934–1942. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.N.; Li, Y.; Sangild, P.T.; Bering, S.B.; Chatterton, D.E. Effects of bovine lactoferrin on the immature porcine intestine. Br. J. Nutr. 2014, 111, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Hui, Y.; Goericke-Pesch, S.; Pankratova, S.; Kot, W.; Pan, X.; Thymann, T.; Sangild, P.T.; Nguyen, D.N. Gut and immune effects of bioactive milk factors in preterm pigs exposed to prenatal inflammation. Am. J. Physiol. Gastrointest. Liver Physiol. 2019, 317, G67–G77. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.N.; Sangild, P.T.; Ostergaard, M.V.; Bering, S.B.; Chatterton, D.E. Transforming growth factor-beta2 and endotoxin interact to regulate homeostasis via interleukin-8 levels in the immature intestine. Am. J. Physiol. Gastrointest. Liver Physiol. 2014, 307, G689–G699. [Google Scholar] [CrossRef] [PubMed]
- Sangild, P.T.; Mei, J.; Fowden, A.L.; Xu, R.J. The prenatal porcine intestine has low transforming growth factor-beta ligand and receptor density and shows reduced trophic response to enteral diets. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 296, R1053–R1062. [Google Scholar] [CrossRef]
- Sangild, P.T.; Siggers, R.H.; Schmidt, M.; Elnif, J.; Bjornvad, C.R.; Thymann, T.; Grondahl, M.L.; Hansen, A.K.; Jensen, S.K.; Boye, M.; et al. Diet- and colonization-dependent intestinal dysfunction predisposes to necrotizing enterocolitis in preterm pigs. Gastroenterology 2006, 130, 1776–1792. [Google Scholar] [CrossRef]
- Rasmussen, M.B.; Holgersen, K.; Pankratova, S.; Baek, O.; Burrin, D.G.; Thymann, T.; Sangild, P.T. Gut development following insulin-like growth factor-1 supplementation to preterm pigs. Pediatr. Res. 2023, 95, 1528–1535. [Google Scholar] [CrossRef] [PubMed]
- Holgersen, K.; Rasmussen, M.B.; Carey, G.; Burrin, D.G.; Thymann, T.; Sangild, P.T. Clinical outcome and gut development after insulin-like growth factor-1 supplementation to preterm pigs. Front. Pediatr. 2022, 10, 868911. [Google Scholar] [CrossRef]
- Calnan, M.; Kirchin, S.; Roberts, D.L.; Wass, M.N.; Michaelis, M. Understanding and tackling the reproducibility crisis—Why we need to study scientists’ trust in data. Pharmacol. Res. 2024, 199, 107043. [Google Scholar] [CrossRef]
- Hoekstra, R.; Vazire, S. Aspiring to greater intellectual humility in science. Nat. Hum. Behav. 2021, 5, 1602–1607. [Google Scholar] [CrossRef] [PubMed]
- Popper, K.R. Conjectures and Refutations: The Growth of Scientific Knowledge; first published 1963; Routledge & Psychology Press: London, UK, 2002. [Google Scholar]
- Kaiser, M. Uncertainty and Precaution 1: Certainty and uncertainty in science. Glob. Bioeth. 2004, 17, 71–80. [Google Scholar] [CrossRef]
- Lonnerdal, B. Bioactive proteins in breast milk. J. Paediatr. Child Health 2013, 49 (Suppl. 1), 1–7. [Google Scholar] [CrossRef]
- Nielsen, S.D.; Beverly, R.L.; Qu, Y.; Dallas, D.C. Milk bioactive peptide database: A comprehensive database of milk protein-derived bioactive peptides and novel visualization. Food Chem. 2017, 232, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Latour, B. From the World of Science to the World of Research? Science 1998, 280, 208–209. [Google Scholar] [CrossRef]
- Dressel, M. Models of science and society: Transcending the antagonism. Hum. Soc. Sci. Comm. 2022, 9, 241. [Google Scholar] [CrossRef]
- Brussow, H. What is truth—In science and beyond. Environ. Microbiol. 2022, 24, 2895–2906. [Google Scholar] [CrossRef]
- Preston, J.; Epley, N. Explanations versus applications: The explanatory power of valuable beliefs. Psychol. Sci. 2005, 16, 826–832. [Google Scholar] [CrossRef] [PubMed]
- Wrathall, M. Religion after Metaphysics; Cambridge University Press: Cambridge, UK, 2004; p. 204. [Google Scholar]
- Smith, W.C. Faith and Belief: The Difference between Them; Oneworld Publications: London, UK, 1998; p. 368. [Google Scholar]
- Farias, M.; Newheiser, A.K.; Kahane, G.; de Toledo, Z. Scientific faith: Belief in science increases in the face of stress and existential anxiety. J. Exp. Soc. Psychol. 2013, 49, 1210–1213. [Google Scholar] [CrossRef] [PubMed]
- Stenmark, M. What is scientism? Relig. Stud. 1997, 33, 15–32. [Google Scholar] [CrossRef]
- Beck, J.; Forstmeier, W. Superstition and belief as inevitable by-products of an adaptive learning strategy. Hum. Nat. 2007, 18, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Loke, A. The Teleological and Kalam Cosmological Arguments Revisited; Springer Nature: Cham, Switzerland, 2022. [Google Scholar]
- McKinnon, A. Kierkegaard and “The Leap of Faith”. Kierkegaardiana 1993, 16, 107–125. [Google Scholar] [CrossRef]
- Carlisle, C. Philosopher of the Heart: The Restless Life of Søren Kierkegaard; Allan Lane: London, UK, 2019; p. 288. [Google Scholar]
- Ewans, C.S. Faith Beyond Reason: A Kierkegaardian Account; Edinburgh University Press: Edinburgh, UK, 1998. [Google Scholar]
- Fremstedal, R. Kierkegaard on Self, Ethics, and Religion: Purity or Despair. In Kierkegaard on Self, Ethics, and Religion: Purity or Despair; Cambridge University Press: Cambridge, UK, 2022. [Google Scholar] [CrossRef]
- Ferreira, M.J.; Ferreira, M. Kierkegaardian faith: The condition and the response. Int. J. Philos. Relig. 1990, 28, 63–79. [Google Scholar] [CrossRef]
- Frankl, V.E. Man’s Search for Meaning; Beacon Press: Boston, MA, USA, 1959. [Google Scholar]
- Løgstrup, K.E. Controverting Kierkegaard; Oxford University Press: Oxford, UK, 2023. [Google Scholar] [CrossRef]
- Audi, R. Faith, Belief, and Rationality. Philos. Perspect. 1991, 5, 213–239. [Google Scholar] [CrossRef]
- Clegg, J.S. Faith. Am. Philos. Q. 1979, 16, 225–232. [Google Scholar]
- Howard-Snyder, D. Does faith entail belief? Faith Philos. 2016, 33, 142–162. [Google Scholar] [CrossRef]
- Pojrnan, L. Faith without belief? Faith Philos. 1986, 3, 157–176. [Google Scholar]
- Joas, K. Faith and knowledge: Habermas’ alternative history of philosophy. Theory Cult. Soc. 2020, 37, 47–52. [Google Scholar] [CrossRef]
- Rapport, N. The truth is alive: Kierkegaard’s anthropology of dualism, subjectivity and somatic knowledge. Anthropol. Theory 2002, 2, 165–183. [Google Scholar] [CrossRef]
- Rogers, C.D. Schleiermacher, Kierkegaard and the problem of first immediacy. Int. J. Philos. Relig. 2016, 80, 259–278. [Google Scholar] [CrossRef]
- WHO. Constitution for World Health Organization. Available online: https://www.who.int/about/accountability/governance/constitution (accessed on 20 November 2023).
- Isaac, M. Role of humanities in modern medical education. Curr. Opin. Psychiatry 2023, 36, 347–351. [Google Scholar] [CrossRef]
- O’Mathuna, D.P. Nursing ethics education: Thinking, feeling, and technology. Nurs. Clin. N. Am. 2022, 57, 613–625. [Google Scholar] [CrossRef]
- Puchalski, C.M.; Vitillo, R.; Hull, S.K.; Reller, N. Improving the spiritual dimension of whole person care: Reaching national and international consensus. J. Palliat. Med. 2014, 17, 642–656. [Google Scholar] [CrossRef]
- Peng-Keller, S.; Winiger, F.; Rauch, R. The Spirit of Global Health: The World Health Organization and the ‘Spiritual Dimension’ of Health, 1946–2021; Oxford University Press: Oxford, UK, 2022. [Google Scholar]
- Koenig, H.G. Research on religion, spirituality, and mental health: A review. Can. J. Psychiatry 2009, 54, 283–291. [Google Scholar] [CrossRef] [PubMed]
- So, H.; Mackenzie, L.; Chapparo, C.; Ranka, J.; McColl, M.A. Spirituality in Australian health professional practice: A scoping review and qualitative synthesis of findings. J. Relig. Health 2023, 62, 2297–2322. [Google Scholar] [CrossRef]
- Gu, S.; Sokolovskiy, K.; Evreeva, O.; Ivleva, S. Religious beliefs shaping health care and transforming health concepts: The case of Shanghai. J. Relig. Health 2023. [Google Scholar] [CrossRef]
- Stripp, T.A.; Wehberg, S.; Bussing, A.; Koenig, H.G.; Balboni, T.A.; VanderWeele, T.J.; Sondergaard, J.; Hvidt, N.C. Spiritual needs in Denmark: A population-based cross-sectional survey linked to Danish national registers. Lancet Reg. Health Eur. 2023, 28, 100602. [Google Scholar] [CrossRef]
- Hayward, R.D.; Krause, N.; Ironson, G.; Hill, P.C.; Emmons, R. Health and well-being among the non-religious: Atheists, agnostics, and no preference compared with religious group members. J. Relig. Health 2016, 55, 1024–1037. [Google Scholar] [CrossRef] [PubMed]
- Dhar, N.; Chaturvedi, S.K.; Nandan, D. Spiritual health, the fourth dimension: A public health perspective. WHO South East Asia J. Public Health 2013, 2, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Canda, E.R.; Furman, L.D. Spiritual Diversity in Social Work Practice: The Heart of Helping; Oxford University Press: Oxford, UK, 2009. [Google Scholar]
- Lv, W. Understanding traditional Chinese medicine. Hepatobiliary Surg. Nutr. 2021, 10, 846–848. [Google Scholar] [CrossRef] [PubMed]
- Giovanni, M.C. The Psyche in Chinese Medicine: Treatment of Emotional and Mental Disharmonies with Acupuncture and Chinese Herbs; Elsevier: Amsterdam, The Netherlands; Churchill Livingstone: London, UK, 2009. [Google Scholar]
- Ghaderi, A.; Tabatabaei, S.M.; Nedjat, S.; Javadi, M.; Larijani, B. Explanatory definition of the concept of spiritual health: A qualitative study in Iran. J. Med. Ethics Hist. Med. 2018, 11, 3. [Google Scholar] [PubMed]
- de Oliveira Maraldi, E. Response bias in research on religion, spirituality and mental health: A critical review of the literature and methodological recommendations. J. Relig. Health 2020, 59, 772–783. [Google Scholar] [CrossRef] [PubMed]
- Koenig, H.G. Religion, spirituality, and health: A review and update. Adv. Mind Body Med. 2015, 29, 19–26. [Google Scholar] [PubMed]
- Daria, S.; Islam, M.R. The use of cow dung and urine to cure COVID-19 in India: A public health concern. Int. J. Health Plann. Manage. 2021, 36, 1950–1952. [Google Scholar] [CrossRef] [PubMed]
- Manokara, K.; Lee, A.; Kamble, S.V.; Krumhuber, E.G. Mind your meat: Religious differences in the social perception of animals. Int. J. Psychol. 2021, 56, 466–477. [Google Scholar] [CrossRef] [PubMed]
- D’Silva, J. Animal Welfare in World Religion Teaching and Practice; Routledge: New York, NY, USA, 2023. [Google Scholar]
- Subudhi, S.; Sriraman, N. Islamic beliefs about milk kinship and donor human milk in the United States. Pediatrics 2021, 147, e20200441. [Google Scholar] [CrossRef]
- Khalil, A.; Buffin, R.; Sanlaville, D.; Picaud, J.C. Milk kinship is not an obstacle to using donor human milk to feed preterm infants in Muslim countries. Acta Paediatr. 2016, 105, 462–467. [Google Scholar] [CrossRef]
- Ozkan, H.; Tuzun, F.; Kumral, A.; Duman, N. Milk kinship hypothesis in light of epigenetic knowledge. Clin. Epigenet. 2012, 4, 14. [Google Scholar] [CrossRef] [PubMed]
- Melnik, B.C.; Schmitz, G. MicroRNAs: Milk’s epigenetic regulators. Best Pract. Res. Clin. Endocrinol. Metab. 2017, 31, 427–442. [Google Scholar] [CrossRef] [PubMed]
- Ahlberg, E.; Al-Kaabawi, A.; Thune, R.; Simpson, M.R.; Pedersen, S.A.; Cione, E.; Jenmalm, M.C.; Tingo, L. Breast milk microRNAs: Potential players in oral tolerance development. Front. Immunol. 2023, 14, 1154211. [Google Scholar] [CrossRef] [PubMed]
- Adamkin, D.H. Use of human milk and fortification in the NICU. J. Perinatol. 2023, 43, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Ludwig, D.S. Milk and health. N. Engl. J. Med. 2020, 382, 644–654. [Google Scholar] [CrossRef]
- Marangoni, F.; Pellegrino, L.; Verduci, E.; Ghiselli, A.; Bernabei, R.; Calvani, R.; Cetin, I.; Giampietro, M.; Perticone, F.; Piretta, L.; et al. Cow’s Milk Consumption and Health: A Health Professional’s Guide. J. Am. Coll. Nutr. 2019, 38, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Rowe, P.C.; Marden, C.L.; Jasion, S.E.; Cranston, E.M.; Flaherty, M.A.; Kelly, K.J. Cow’s milk protein intolerance in adolescents and young adults with chronic fatigue syndrome. Acta Paediatr. 2016, 105, e412–e418. [Google Scholar] [CrossRef] [PubMed]
- Rowe, K.S. Long term follow up of young people with chronic fatigue syndrome attending a pediatric outpatient service. Front. Pediatr. 2019, 7, 21. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, X.; Mi, L.; Li, C.; Zhang, Y.; Bi, R.; Pang, J.; Li, Y. Comparative proteomic analysis of proteins in breast milk during different lactation periods. Nutrients 2022, 14, 3648. [Google Scholar] [CrossRef]
- Zhao, H.; Li, M.; Zhu, Q.; Liu, A.; Bi, J.; Quan, Z.; Luo, X.; Zheng, Y.; Yang, N.; Yue, X.; et al. Label-free quantitative proteomic analysis of milk fat globule membrane proteins in porcine colostrum and mature milk. Food Chem. 2023, 426, 136447. [Google Scholar] [CrossRef]
- Yang, M.; Cong, M.; Peng, X.; Wu, J.; Wu, R.; Liu, B.; Ye, W.; Yue, X. Quantitative proteomic analysis of milk fat globule membrane (MFGM) proteins in human and bovine colostrum and mature milk samples through iTRAQ labeling. Food Funct. 2016, 7, 2438–2450. [Google Scholar] [CrossRef] [PubMed]
- Marcone, S.; Belton, O.; Fitzgerald, D.J. Milk-derived bioactive peptides and their health promoting effects: A potential role in atherosclerosis. Br. J. Clin. Pharmacol. 2017, 83, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Mayes, C.R.; Thompson, D.B. What should we eat? Biopolitics, ethics, and nutritional scientism. J. Bioeth. Inq. 2015, 12, 587–599. [Google Scholar] [CrossRef] [PubMed]
- Hayek, F.A. The counter-revolution of science: Studies on the abuse of reason. Ann. Am. Acad. Polit. Soc. Sci. 1952, 284, 208–209. [Google Scholar]
- Kumari, P.; Raval, A.; Rana, P.; Mahto, S.K. Regenerative potential of human breast milk: A natural reservoir of nutrients, bioactive components and stem cells. Stem Cell Rev. Rep. 2023, 19, 1307–1327. [Google Scholar] [CrossRef] [PubMed]
- Ning, J.; Yang, M.; Liu, W.; Luo, X.; Yue, X. Proteomics and peptidomics as a tool to compare the proteins and endogenous peptides in human, cow, and donkey milk. J. Agric. Food Chem. 2023, 71, 16435–16451. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Gong, D.; Gao, F.; Sangild, P.T. Diet-dependent changes in the intestinal DNA methylome after introduction of enteral feeding in preterm pigs. Epigenomics 2018, 10, 395–408. [Google Scholar] [CrossRef] [PubMed]
- Lemas, D.J.; Du, X.; Dado-Senn, B.; Xu, K.; Dobrowolski, A.; Magalhaes, M.; Aristizabal-Henao, J.J.; Young, B.E.; Francois, M.; Thompson, L.A.; et al. Untargeted metabolomic analysis of lactation-stage-matched human and bovine milk samples at 2 weeks postnatal. Nutrients 2023, 15, 3768. [Google Scholar] [CrossRef] [PubMed]
- Moossavi, S.; Miliku, K.; Sepehri, S.; Khafipour, E.; Azad, M.B. The prebiotic and probiotic properties of human milk: Implications for infant immune development and pediatric asthma. Front. Pediatr. 2018, 6, 197. [Google Scholar] [CrossRef]
- Albright, J.R. God of the Gaps. In Encyclopedia of Sciences and Religions; Runehov, A.L.C., Oviedo, L., Eds.; Springer: Dordrecht, The Netherlands, 2013; pp. 955–956. [Google Scholar] [CrossRef]
- Ng, S.; Strunk, T.; Jiang, P.; Muk, T.; Sangild, P.T.; Currie, A. Precision Medicine for Neonatal Sepsis. Front. Mol. Biosci. 2018, 5, 70. [Google Scholar] [CrossRef]
- D’Alessandro, A.; Scaloni, A.; Zolla, L. Human milk proteins: An interactomics and updated functional overview. J. Proteome Res. 2010, 9, 3339–3373. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Stanstrup, J.; Thymann, T.; Sangild, P.T.; Dragsted, L.O. Progressive Changes in the Plasma Metabolome during Malnutrition in Juvenile Pigs. J. Proteome Res. 2016, 15, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Muk, T.; Ren, S.; Nguyen, D.N.; Shen, R.L.; Gao, F.; Sangild, P.T. Blood transcriptomic markers of necrotizing enterocolitis in preterm pigs. Pediatr. Res. 2022, 91, 1113–1120. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Pan, X.; Hui, Y.; Kot, W.; Gao, F.; Sangild, P.T.; Nguyen, D.N. Subclinical necrotizing enterocolitis-induced systemic immune suppression in neonatal preterm pigs. Am. J. Physiol. Gastrointest. Liver Physiol. 2021, 321, G18–G28. [Google Scholar] [CrossRef] [PubMed]
- Willems, R.; Krych, L.; Rybicki, V.; Jiang, P.; Sangild, P.T.; Shen, R.L.; Hensel, K.O.; Wirth, S.; Postberg, J.; Jenke, A.C. Introducing enteral feeding induces intestinal subclinical inflammation and respective chromatin changes in preterm pigs. Epigenomics 2015, 7, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Sangild, P.T. Intestinal proteomics in pig models of necrotising enterocolitis, short bowel syndrome and intrauterine growth restriction. Proteom. Clin. Appl. 2014, 8, 700–714. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Siggers, J.L.; Ngai, H.H.; Sit, W.H.; Sangild, P.T.; Wan, J.M. The small intestine proteome is changed in preterm pigs developing necrotizing enterocolitis in response to formula feeding. J. Nutr. 2008, 138, 1895–1901. [Google Scholar] [CrossRef]
- Jiang, P.; Wan, J.M.; Sit, W.H.; Lee, C.L.; Schmidt, M.; Sangild, P.T. Enteral feeding in utero induces marked intestinal structural and functional proteome changes in pig fetuses. Pediatr. Res. 2011, 69, 123–128. [Google Scholar] [CrossRef]
- Sharma, I.K.; Byrne, A. Early initiation of breastfeeding: A systematic literature review of factors and barriers in South Asia. Int. Breastfeed. J. 2016, 11, 17. [Google Scholar] [CrossRef]
- Huo, M.; Liu, C.; Mei, H.; Zhang, Y.; Liu, C.; Song, D.; Zhang, Y.; Zhang, Y.; Xin, C. Intervention effect of oropharyngeal administration of colostrum in preterm infants: A meta-analysis. Front. Pediatr. 2022, 10, 895375. [Google Scholar] [CrossRef]
- Slouha, E.; Anderson, Z.S.; Ankrah, N.M.N.; Kalloo, A.E.; Gorantla, V.R. Colostrum and preterm babies: A systematic review. Cureus 2023, 15, e42021. [Google Scholar] [CrossRef] [PubMed]
- Garofoli, F.; Civardi, E.; Pisoni, C.; Angelini, M.; Ghirardello, S. Anti-Inflammatory and anti-allergic properties of colostrum from mothers of full-term and preterm babies: The importance of maternal lactation in the first days. Nutrients 2023, 15, 4249. [Google Scholar] [CrossRef] [PubMed]
- Nasuf, A.W.A.; Ojha, S.; Dorling, J. Oropharyngeal colostrum in preventing mortality and morbidity in preterm infants. Cochrane Database Syst. Rev. 2018, 9, CD011921. [Google Scholar] [CrossRef]
- Kersin, S.G.; Ozek, E. Breast milk stem cells: Are they magic bullets in neonatology? Turk. Arch. Pediatr. 2021, 56, 187–191. [Google Scholar] [CrossRef]
- Kaplan, M.; Arslan, A.; Duman, H.; Karyelioglu, M.; Baydemir, B.; Gunar, B.B.; Alkan, M.; Bayraktar, A.; Tosun, H.I.; Erturk, M.; et al. Production of bovine colostrum for human consumption to improve health. Front. Pharmacol. 2021, 12, 796824. [Google Scholar] [CrossRef] [PubMed]
- Dziewiecka, H.; Buttar, H.S.; Kasperska, A.; Ostapiuk-Karolczuk, J.; Domagalska, M.; Cichon, J.; Skarpanska-Stejnborn, A. A systematic review of the influence of bovine colostrum supplementation on leaky gut syndrome in athletes: Diagnostic biomarkers and future directions. Nutrients 2022, 14, 2512. [Google Scholar] [CrossRef] [PubMed]
- Linehan, K.; Ross, R.P.; Stanton, C. Bovine colostrum for veterinary and human health applications: A critical review. Annu. Rev. Food Sci. Technol. 2023, 14, 387–410. [Google Scholar] [CrossRef]
- Mehra, R.; Garhwal, R.; Sangwan, K.; Guine, R.P.F.; Lemos, E.T.; Buttar, H.S.; Visen, P.K.S.; Kumar, N.; Bhardwaj, A.; Kumar, H. Insights into the research trends on bovine colostrum: Beneficial health perspectives with special reference to manufacturing of functional foods and feed supplements. Nutrients 2022, 14, 659. [Google Scholar] [CrossRef]
- Ghosh, S.; Lacucci, M. Diverse immune effects of bovine colostrum and benefits in human health and disease. Nutrients 2021, 13, 3798. [Google Scholar] [CrossRef]
- Playford, R.J. The Useof bovine colostrum in medical practice and human health: Current evidence and areas requiring further examination. Nutrients 2021, 14, 92. [Google Scholar] [CrossRef]
- Gao, X.; Li, Y.; Olin, A.B.; Nguyen, D.N. Fortification with bovine colostrum enhances antibacterial activity of human milk. JPEN J. Parenter. Enter. Nutr. 2021, 45, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, B.; Dutta, S.; Singh, R.; Prasad, R.; Kumar, P. Bovine colostrum in prevention of necrotizing enterocolitis and sepsis in very low birth weight neonates: A randomized, double-blind, placebo-controlled pilot trial. J. Trop. Pediatr. 2017, 63, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Ismail, R.I.H.; Awad, H.A.; Imam, S.S.; Gad, G.I.; Aboushady, N.M.; Abdou, R.M.; Eissa, D.S.; Azzam, N.T.; Barakat, M.M.; Yassin, M.M.; et al. Gut priming with bovine colostrum and T regulatory cells in preterm neonates: A randomized controlled trial. Pediatr. Res. 2021, 90, 650–656. [Google Scholar] [CrossRef]
- Akhter, S. Multinational corporations and the impact of public advocacy on corporate strategy: Nestlé and the infant formula controversy. J. Int. Bus. Stud. 1994, 25, 658–660. [Google Scholar] [CrossRef]
- Wei, Y.; Liu, D. Review of melamine scandal: Still a long way ahead. Toxicol. Ind. Health 2012, 28, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Walker, A. Breast milk as the gold standard for protective nutrients. J. Pediatr. 2010, 156, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Luo, G.; Zhu, Y.; Ni, D.; Chen, J.; Zhang, W.; Mu, W. Infant formulae—Key components, nutritional value, and new perspectives. Food Chem. 2023, 424, 136393. [Google Scholar] [CrossRef]
- Lajnaf, R.; Feki, S.; Ben Ameur, S.; Attia, H.; Kammoun, T.; Ayadi, M.A.; Masmoudi, H. Recent advances in selective allergies to mammalian milk proteins not associated with Cow’s Milk Proteins Allergy. Food Chem. Toxicol. 2023, 178, 113929. [Google Scholar] [CrossRef] [PubMed]
- Nebbia, S.; Deglaire, A.; Menard, O.; Henry, G.; Barberis, E.; Manfredi, M.; Bertino, E.; Coscia, A.; Dupont, D.; Giribaldi, M.; et al. Supplementing human milk with a donkey or bovine milk derived fortifier: Consequences on proteolysis, lipolysis and particle structure under in vitro dynamic digestion. Food Chem. 2022, 395, 133579. [Google Scholar] [CrossRef]
- Sun, J.; Akıllıoğlu, H.G.; Aasmul-Olsen, K.; Ye, Y.; Lund, P.; Zhao, X.; Brunse, A.; Nielsen, C.F.; Chatterton, D.E.W.; Sangild, P.T.; et al. Ultra-high temperature treatment and storage of infant formula induces dietary protein modifications, gut dysfunction, and inflammation in preterm pigs. Mol. Nutr. Food Res. 2022, 66, e2200132. [Google Scholar] [CrossRef]
- Ahern, G.J.; Hennessy, A.A.; Ryan, C.A.; Ross, R.P.; Stanton, C. Advances in infant formula science. Annu. Rev. Food Sci. Technol. 2019, 10, 75–102. [Google Scholar] [CrossRef] [PubMed]
- Embleton, N.D.; Berrington, J.E. Milk-based bionutrient trials to improve outcomes in preterm infants: Challenges and opportunities. Am. J. Perinatol. 2022, 39, S68–S72. [Google Scholar] [CrossRef] [PubMed]
- Timby, N.; Domellof, M.; Lonnerdal, B.; Hernell, O. Supplementation of infant formula with bovine milk fat globule membranes. Adv. Nutr. 2017, 8, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Nie, C.; Zhao, Y.; Wang, X.; Li, Y.; Fang, B.; Wang, R.; Wang, X.; Liao, H.; Li, G.; Wang, P.; et al. Structure, Biological Functions, Separation, Properties, and Potential Applications of Milk Fat Globule Membrane (MFGM): A Review. Nutrients 2024, 16, 587. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Jia, Q.; Chen, Z.; You, Y.; Liu, Y.; Zhao, J.; Chen, L.; Ma, D.; Xing, Y. Comparative evaluation of enriched formula milk powder with OPO and MFGM vs. breastfeeding and regular formula milk powder in full-term infants: A comprehensive study on gut microbiota, neurodevelopment, and growth. Food Funct. 2024, 15, 1417–1430. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo-Ospina, A.M.; Mujica-Coopman, M.F.; Murguia-Peniche, T.; Wampler, J.L.; Wu, S.S.; Berseth, C.L.; Weisstaub, S.G.; Uauy, R. Micronutrient, Metabolic, and Inflammatory Biomarkers through 24 Months of Age in Infants Receiving Formula with Added Bovine Milk Fat Globule Membrane through the First Year of Life: A Randomized Controlled Trial. J. Nutr. 2023, 153, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Ambrozej, D.; Dumycz, K.; Dziechciarz, P.; Ruszczynski, M. Milk fat globule membrane supplementation in children: Systematic review with meta-analysis. Nutrients 2021, 13, 714. [Google Scholar] [CrossRef] [PubMed]
- Best, K.P.; Yelland, L.N.; Collins, C.T.; McPhee, A.J.; Rogers, G.B.; Choo, J.; Gibson, R.A.; Murguia-Peniche, T.; Varghese, J.; Cooper, T.R.; et al. Growth of late preterm infants fed nutrient-enriched formula to 120 days corrected age—A randomized controlled trial. Front. Pediatr. 2023, 11, 1146089. [Google Scholar] [CrossRef] [PubMed]
- Sangild, P.T.; Strunk, T.; Currie, A.J.; Nguyen, D.N. Editorial: Immunity in compromised newborns. Front. Immunol. 2021, 12, 732332. [Google Scholar] [CrossRef]
- Yan, X.; Sangild, P.T.; Peng, Y.; Li, Y.; Bering, S.B.; Pan, X. Supplementary bovine colostrum feedings to formula-fed preterm pigs improve gut function and reduce necrotizing enterocolitis. J. Pediatr. Gastroenterol. Nutr. 2021, 73, e39–e46. [Google Scholar] [CrossRef]
- Ulfman, L.H.; Leusen, J.H.W.; Savelkoul, H.F.J.; Warner, J.O.; van Neerven, R.J.J. Effects of bovine immunoglobulins on immune function, allergy, and infection. Front. Nutr. 2018, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Walsh, V.; McGuire, W. Immunonutrition for preterm infants. Neonatology 2019, 115, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Tinghall Nilsson, U.; Hernell, O.; Lonnerdal, B.; Hartvigsen, M.L.; Jacobsen, L.N.; Kvistgaard, A.S.; Karlsland Akeson, P. Low-protein formulas with alpha-lactalbumin-enriched or glycomacropeptide-reduced whey: Effects on growth, nutrient intake and protein metabolism during early infancy: A randomized, double-blinded controlled trial. Nutrients 2023, 15, 1010. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, L.; Worku, M. Recent perspective on cow’s milk allergy and dairy nutrition. Crit. Rev. Food Sci. Nutr. 2022, 62, 7503–7517. [Google Scholar] [CrossRef] [PubMed]
- Kouwenhoven, S.M.P.; Muts, J.; Finken, M.J.J.; Goudoever, J.B.V. Low-protein infant formula and obesity risk. Nutrients 2022, 14, 2728. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, E.S.; Christensen, B. Milk Osteopontin and Human Health. Nutrients 2023, 15, 2423. [Google Scholar] [CrossRef] [PubMed]
- Christensen, B.; Buitenhuis, A.J.; Jacobsen, L.N.; Ostenfeld, M.S.; Sorensen, E.S. The effect of human and bovine milk osteopontin on intestinal caco-2 cells: A transcriptome comparison. Nutrients 2023, 15, 1166. [Google Scholar] [CrossRef] [PubMed]
- Sodek, J.; Da Silva, A.P.B.; Zohar, R. Osteopontin and Mucosal Protection. J. Dent. Res. 2006, 85, 404–415. [Google Scholar] [CrossRef] [PubMed]
- Jiang, R.; Prell, C.; Lonnerdal, B. Milk osteopontin promotes brain development by up-regulating osteopontin in the brain in early life. FASEB J. 2019, 33, 1681–1694. [Google Scholar] [CrossRef]
- Berrington, J.E.; McGuire, W.; Embleton, N.D. ELFIN, the United Kingdom preterm lactoferrin trial: Interpretation and future questions (1). Biochem. Cell Biol. 2021, 99, 1–6. [Google Scholar] [CrossRef]
- Corpeleijn, W.E.; van Vliet, I.; de Gast-Bakker, D.A.; van der Schoor, S.R.; Alles, M.S.; Hoijer, M.; Tibboel, D.; van Goudoever, J.B. Effect of enteral IGF-1 supplementation on feeding tolerance, growth, and gut permeability in enterally fed premature neonates. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 184–190. [Google Scholar] [CrossRef] [PubMed]
- York, D.J.; Smazal, A.L.; Robinson, D.T.; De Plaen, I.G. Human milk growth factors and their role in NEC prevention: A narrative review. Nutrients 2021, 13, 3751. [Google Scholar] [CrossRef] [PubMed]
- Holgersen, K.; Gao, X.; Narayanan, R.; Gaur, T.; Carey, G.; Barton, N.; Pan, X.; Muk, T.; Thymann, T.; Sangild, P.T. Supplemental Insulin-Like Growth Factor-1 and necrotizing enterocolitis in preterm pigs. Front. Pediatr. 2020, 8, 602047. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.K.; Monaco, M.M.; Donovan, S.M. Delivery of total parenteral nutrition (TPN) via umbilical catheterization: Development of a piglet model to investigate therapies to improve gastrointestinal structure and enzyme activity during TPN. Biol. Neonate 1998, 73, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.N.; Jiang, P.; Jacobsen, S.; Sangild, P.T.; Bendixen, E.; Chatterton, D.E. Protective effects of transforming growth factor β2 in intestinal epithelial cells by regulation of proteins associated with stress and endotoxin responses. PLoS ONE 2015, 10, e0117608. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, A.; Kelly, D.R.; Nicola, T.; Ambalavanan, N.; Jain, S.K.; Murphy-Ullrich, J.; Athar, M.; Shimamura, M.; Bhandari, V.; Aprahamian, C.; et al. TGF-beta2 suppresses macrophage cytokine production and mucosal inflammatory responses in the developing intestine. Gastroenterology 2011, 140, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Coursodon, C.F.; Dvorak, B. Epidermal growth factor and necrotizing enterocolitis. Curr. Opin. Pediatr. 2012, 24, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, M.A.; Haymond, M.W. The magic of mother’s milk. Diabetes 2012, 61, 3076–3077. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.; Sauve, R.S. Breast is best for babies. J. Natl. Med. Assoc. 2005, 97, 1010–1019. [Google Scholar]
- Reid, L. Scientism in medical education and the improvement of medical care: Opioids, competencies, and social accountability. Health Care Anal. 2018, 26, 155–170. [Google Scholar] [CrossRef]
- Liu, C.; Pan, M.; Lu, X.; Gao, Y.; Xu, J.; Chen, X. Breastfeeding Barriers for Preterm Infants in Neonatal Intensive Care Unit Environments: A Systematic Assessment and Meta-Analysis. Breastfeed. Med. 2024. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.K.; Kim, J.H.; Baek, H.S.; Lee, E.; Baek, J.H.; Shim, S.; Kim, Y.H.; Moreno, L.A.; Lee, S.W.; Han, M.Y. Association between complementary food introduction before age 4 months and body mass index at age 5–7 years: A retrospective population-based longitudinal cohort study. J. Hum. Nutr. Diet 2023, 36, 787–797. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.K.; Kim, J.H.; Cha, H.R.; Lee, W.S.; Lee, S.W.; Han, M.Y. Relationship Between Feeding to Sleep During Infancy and Subsequent Childhood Disease Burden. J. Pediatr. 2023, 256, 85–91.e3. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.K.; Lee, S.W.; Kim, J.H.; Lee, E.; Cha, H.R.; Han, B.E.; Shin, J.; Han, M.Y. Associations between Delayed Introduction of Complementary Foods and Childhood Health Consequences in Exclusively Breastfed Children. Nutrients 2023, 15, 3410. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Shin, J.I.; Kim, S.; Choi, Y.S.; Shin, Y.H.; Hwang, J.; Shin, J.U.; Koyanagi, A.; Jacob, L.; Smith, L.; et al. Breastfeeding and impact on childhood hospital admissions: A nationwide birth cohort in South Korea. Nat. Commun. 2023, 14, 5819. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guideline: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services. Available online: https://www.ncbi.nlm.nih.gov/books/NBK487814/ (accessed on 20 November 2023).
- Lewis, M.; Freedle, R. Mother–Infant Dyad: The Cradle of Meaning. In Communication and Affect; Pliner, P., Krames, L., Alloway, T., Eds.; Academic Press: Cambridge, MA, USA, 1973; pp. 127–155. [Google Scholar] [CrossRef]
- Tsang, L.P.M.; Ng, D.C.C.; Chan, Y.H.; Chen, H.Y. Caring for the mother-child dyad as a family physician. Singap. Med. J. 2019, 60, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Subramani, S. Beyond Public Health and Private Choice: Breastfeeding, Embodiment and Public Health Ethics. Asian Bioeth. Rev. 2024, 16, 249–266. [Google Scholar] [CrossRef] [PubMed]
- Martucci, J.; Barnhill, A. Examining the use of ‘natural’ in breastfeeding promotion: Ethical and practical concerns. J. Med. Ethics 2018, 44, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Colodro-Conde, L.; Liminana-Gras, R.M.; Sanchez-Lopez, M.P.; Ordonana, J.R. Gender, health, and initiation of breastfeeding. Women Health 2015, 55, 22–41. [Google Scholar] [CrossRef]
- Beltran-Silva, F.; McInnis, N. Relationship Between Sex-Specific Labor Market Performance and Breastfeeding Prevalence. J. Hum. Lact. 2024, 40, 318–327. [Google Scholar] [CrossRef]
- Santacruz-Salas, E.; Aranda-Reneo, I.; Hidalgo-Vega, A.; Blanco-Rodriguez, J.M.; Segura-Fragoso, A. The Economic Influence of Breastfeeding on the Health Cost of Newborns. J. Hum. Lact. 2019, 35, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Nagel, E.M.; Howland, M.A.; Pando, C.; Stang, J.; Mason, S.M.; Fields, D.A.; Demerath, E.W. Maternal Psychological Distress and Lactation and Breastfeeding Outcomes: A Narrative Review. Clin. Ther. 2022, 44, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Bernard, J.Y.; Rifas-Shiman, S.L.; Cohen, E.; Lioret, S.; de Lauzon-Guillain, B.; Charles, M.A.; Kramer, M.S.; Oken, E. Maternal religion and breastfeeding intention and practice in the US Project Viva cohort. Birth 2020, 47, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Burdette, A.M.; Pilkauskas, N.V. Maternal religious involvement and breastfeeding initiation and duration. Am. J. Public Health 2012, 102, 1865–1868. [Google Scholar] [CrossRef] [PubMed]
- Bensaid, B. Breastfeeding as a fundamental islamic human right. J. Relig. Health 2021, 60, 362–373. [Google Scholar] [CrossRef]
- Kowalski, C.J.; Mrdjenovich, A.J.; Redman, R.W. Scientism recognizes evidence only of the quantitative/general variety. J. Eval. Clin. Pract. 2020, 26, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Loughlin, M.; Lewith, G.; Falkenberg, T. Science, practice and mythology: A definition and examination of the implications of scientism in medicine. Health Care Anal. 2013, 21, 130–145. [Google Scholar] [CrossRef]
- Werth, A.J.; Allchin, D. How we Think About Human Nature: Cognitive Errors and Concrete Remedies. Found. Sci. 2021, 26, 825–846. [Google Scholar] [CrossRef]
- Taher, M.; Pashaeypoor, S.; Cheraghi, M.A.; Karimy, M.; Hoseini, A.S.S. Superstition in health beliefs: Concept exploration and development. J. Fam. Med. Prim. Care 2020, 9, 1325–1330. [Google Scholar] [CrossRef]
- Wold, A.E. Why is there still confusion about the impact of breast-feeding on the risk of allergy development? Scand. J. Food Nutr. 2006, 50, 35–41. [Google Scholar] [CrossRef]
- Nuzzi, G.; Di Cicco, M.E.; Peroni, D.G. Breastfeeding and allergic diseases: What’s new? Children 2021, 8, 330. [Google Scholar] [CrossRef] [PubMed]
- Matheson, M.C.; Allen, K.J.; Tang, M.L. Understanding the evidence for and against the role of breastfeeding in allergy prevention. Clin. Exp. Allergy 2012, 42, 827–851. [Google Scholar] [CrossRef]
- Rafaelsen, O.J. Steno in Six Languages; Rhodos International Publishers: Humlebaek, Denmark, 1986; p. 95. [Google Scholar]
- Tubbs, R.S.; Gianaris, N.; Shoja, M.M.; Loukas, M.; Cohen Gadol, A.A. “The heart is simply a muscle” and first description of the tetralogy of “Fallot”. Early contributions to cardiac anatomy and pathology by bishop and anatomist Niels Stensen (1638–1686). Int. J. Cardiol. 2012, 154, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Feingold, M. The religion of the young Isaac Newton. Ann. Sci. 2019, 76, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Cortes, M.E.; Del Rio, J.P.; Vigil, P. The harmonious relationship between faith and science from the perspective of some great saints: A brief comment. Linacre Q. 2015, 82, 3–7. [Google Scholar] [CrossRef]
- Steno, N. Prooemium or Preface to a Demonstration in Copenhagen Anatomical Theater in the Year 1673 (translation from Latin). In Steno: Life, Science, Philosophy: Acta Historica Scientarium naturalium et Medicinalium; Kardel, T., Ed.; National Library of Science: Copenhagen, Denmark, 1994; Volume 42, p. 159. [Google Scholar]
- Boss, J. The medical philosophy of Francis Bacon (1561–1626). Med. Hypotheses 1978, 4, 208–220. [Google Scholar] [CrossRef]
- Upton, J.; Janeka, I.; Ferraro, N. The whole is more than the sum of its parts: Aristotle, metaphysical. J. Craniofac. Surg. 2014, 25, 59–63. [Google Scholar] [CrossRef]
- Vallish, B.N.; Dang, D.; Dang, A. Nature and mechanism of immune boosting by Ayurvedic medicine: A systematic review of randomized controlled trials. World J. Methodol. 2022, 12, 132–147. [Google Scholar] [CrossRef] [PubMed]
- Subbarayappa, B.V. Siddha medicine: An overview. Lancet 1997, 350, 1841–1844. [Google Scholar] [CrossRef]
- Matos, L.C.; Machado, J.P.; Monteiro, F.J.; Greten, H.J. Understanding Traditional Chinese Medicine Therapeutics: An Overview of the Basics and Clinical Applications. Healthcare 2021, 9, 257. [Google Scholar] [CrossRef]
- Patwardhan, B.; Warude, D.; Pushpangadan, P.; Bhatt, N. Ayurveda and traditional Chinese medicine: A comparative overview. Evid. Based Complement. Alternat. Med. 2005, 2, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Catlin, E.A.; Cadge, W.; Ecklund, E.H.; Gage, E.A.; Zollfrank, A.A. The spiritual and religious identities, beliefs, and practices of academic pediatricians in the United States. Acad. Med. 2008, 83, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Ecklund, E.H.; Johnson, D.R.; Scheitle, C.P.; Matthews, K.R.W.; Lewis, S.W. Religion among Scientists in International Context:A New Study of Scientists in Eight Regions. Socius 2016, 2, 2378023116664353. [Google Scholar] [CrossRef]
- Johnson, D.R.; Ecklund, E.H.; Di, D.; Matthews, K.R.W. Responding to Richard: Celebrity and (mis)representation of science. Public Underst. Sci. 2018, 27, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.M. On the origin of natural history: Steno’s modern, but forgotten philosophy of science. Bull. Geologic. Soc. Den. 2009, 57, 1–24. [Google Scholar] [CrossRef]
- Gould, S.J. Nonoverlapping magisteria. Nat. Hist. 1997, 106, 16–22. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sangild, P.T. Science and Faith to Understand Milk Bioactivity for Infants. Nutrients 2024, 16, 1676. https://doi.org/10.3390/nu16111676
Sangild PT. Science and Faith to Understand Milk Bioactivity for Infants. Nutrients. 2024; 16(11):1676. https://doi.org/10.3390/nu16111676
Chicago/Turabian StyleSangild, Per T. 2024. "Science and Faith to Understand Milk Bioactivity for Infants" Nutrients 16, no. 11: 1676. https://doi.org/10.3390/nu16111676
APA StyleSangild, P. T. (2024). Science and Faith to Understand Milk Bioactivity for Infants. Nutrients, 16(11), 1676. https://doi.org/10.3390/nu16111676