Infant Formula with 50% or More of Palmitic Acid Bound to the sn-2 Position of Triacylglycerols Eliminate the Association between Formula-Feeding and the Increase of Fecal Palmitic Acid Levels in Newborns: An Exploratory Study

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Categorization of Infant Formulas
2.2. Study Design and Participants
2.3. Data and Sample Collection
2.4. Anthropometric Data Collection
2.5. Analysis of Total PA and Soaped PA Levels in Stool
2.6. Statistical Analysis
3. Results
3.1. Study Population and Demographic Data
3.2. Association between Feeding Volume of High or Low sn-2 PA Milk and Anthropometric Data
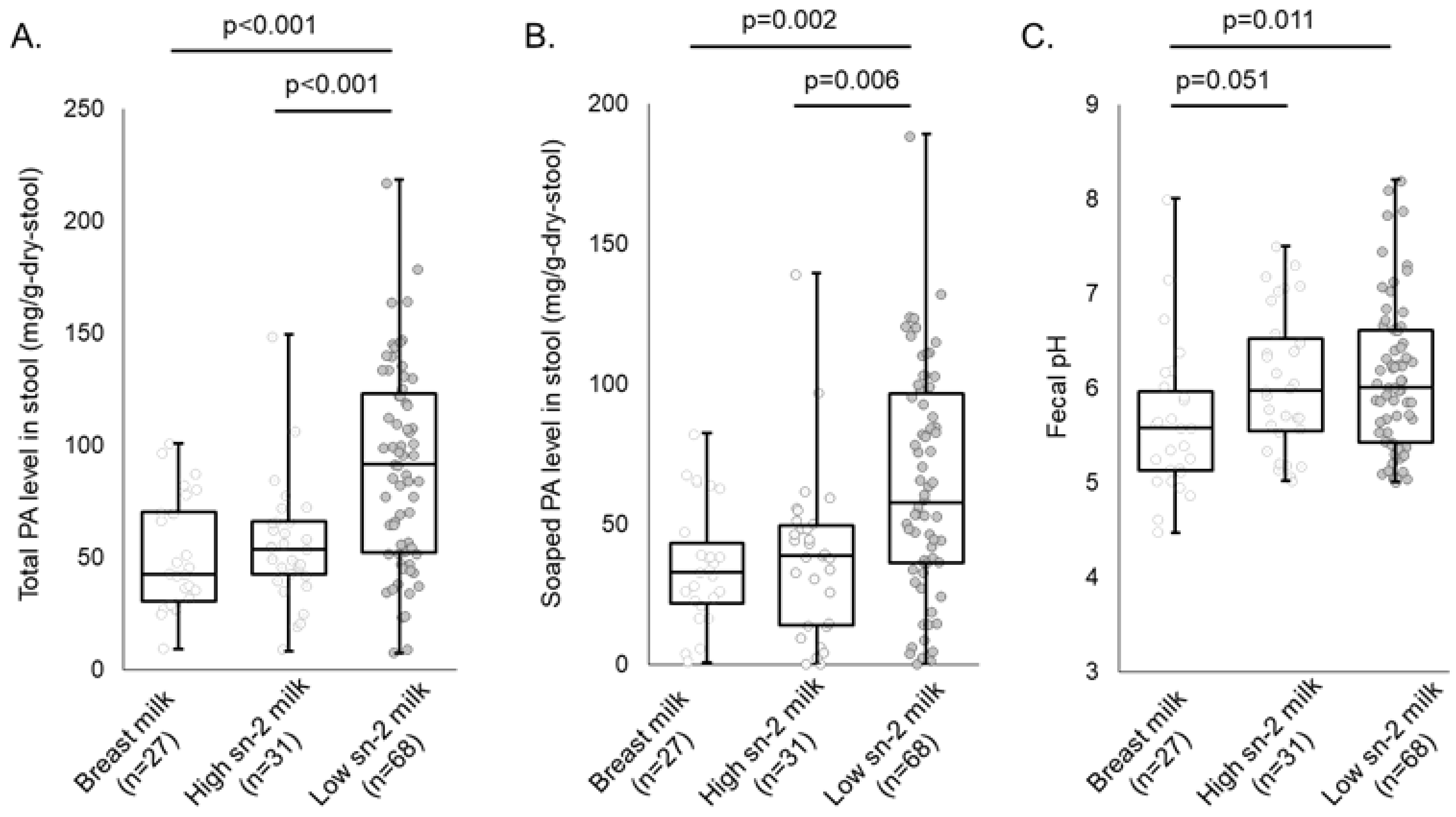
3.3. Association between Feeding Volume of High or Low sn-2 PA Milk and Fecal PA Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Demmelmair, H.; Koletzko, B. Lipids in human milk. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Innis, S.M. Palmitic acid in early human development. Crit. Rev. Food Sci. Nutr. 2016, 56, 1952–1959. [Google Scholar] [CrossRef] [PubMed]
- Havlicekova, Z.; Jesenak, M.; Banovcin, P.; Kuchta, M. Beta-palmitate—A natural component of human milk in supplemental milk formulas. Nutr. J. 2016, 15, 28. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.G.; Ferris, A.M.; Lammi-Keefe, C.J.; Henderson, R.A. Lipids of bovine and human milks: A comparison. J. Dairy Sci. 1990, 73, 223–240. [Google Scholar] [CrossRef] [PubMed]
- Innis, S.M.; Dyer, R.; Nelson, C.M. Evidence that palmitic acid is absorbed as sn-2 monoacylglycerol from human milk by breast-fed infants. Lipids 1994, 29, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Straarup, E.M.; Lauritzen, L.; Faerk, J.; Høy Deceased, C.E.; Michaelsen, K.F. The stereospecific triacylglycerol structures and Fatty Acid profiles of human milk and infant formulas. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.C.; Bougnoux, P.; Antoine, J.M.; Lanson, M.; Couet, C. Triacylglycerol structure of human colostrum and mature milk. Lipids 1993, 28, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Wei, W.; Su, H.; Zou, X.; Wang, X. Evaluation of sn-2 fatty acid composition in commercial infant formulas on the Chinese market: A comparative study based on fat source and stage. Food Chem. 2018, 242, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, P.T.; Lockton, S.; Irwin, J.; Lucas, A.L. The relationship between stool hardness and stool composition in breast- and formula-fed infants. J. Pediatr. Gastroenterol. Nutr. 1995, 20, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Carnielli, V.P.; Luijendijk, I.H.; van Goudoever, J.B.; Sulkers, E.J.; Boerlage, A.A.; Degenhart, H.J.; Sauer, P.J. Feeding premature newborn infants palmitic acid in amounts and stereoisomeric position similar to that of human milk: Effects on fat and mineral balance. Am. J. Clin. Nutr. 1995, 61, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Carnielli, V.P.; Luijendijk, I.H.; Van Goudoever, J.B.; Sulkers, E.J.; Boerlage, A.A.; Degenhart, H.J.; Sauer, P.J. Structural position and amount of palmitic acid in infant formulas: Effects on fat, fatty acid, and mineral balance. J. Pediatr. Gastroenterol. Nutr. 1996, 23, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Lucas, A.; Quinlan, P.; Abrams, S.; Ryan, S.; Meah, S.; Lucas, P.J. Randomised controlled trial of a synthetic triglyceride milk formula for preterm infants. Arch. Dis. Child Fetal. Neonatal. Ed. 1997, 77, F178–F184. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, K.; Fewtrell, M.S.; Morley, R.; Abbott, R.; Quinlan, P.T.; Wells, J.C.; Bindels, J.G.; Lucas, A. Double-blind, randomized trial of a synthetic triacylglycerol in formula-fed term infants: Effects on stool biochemistry, stool characteristics, and bone mineralization. Am. J. Clin. Nutr. 1999, 70, 920–927. [Google Scholar] [CrossRef] [PubMed]
- López-López, A.; Castellote-Bargalló, A.I.; Campoy-Folgoso, C.; Rivero-Urgël, M.; Tormo-Carnicé, R.; Infante-Pina, D.; López-Sabater, M.C. The influence of dietary palmitic acid triacylglyceride position on the fatty acid, calcium and magnesium contents of at term newborn faeces. Early Hum. Dev. 2001, 65 (Suppl. 2), S83–S94. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Lien, E.L.; Capeding, M.R.; Fitzgerald, M.; Ramanujam, K.; Yuhas, R.; Northington, R.; Lebumfacil, J.; Wang, L.; DeRusso, P.A. Effects of term infant formulas containing high sn-2 palmitate with and without oligofructose on stool composition, stool characteristics, and bifidogenicity. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Nowacki, J.; Lee, H.C.; Lien, R.; Cheng, S.W.; Li, S.T.; Yao, M.; Northington, R.; Jan, I.; Mutungi, G. Stool fatty acid soaps, stool consistency and gastrointestinal tolerance in term infants fed infant formulas containing high sn-2 palmitate with or without oligofructose: A double-blind, randomized clinical trial. Nutr. J. 2014, 13, 105. [Google Scholar] [CrossRef] [PubMed]
- Bar-Yoseph, F.; Lifshitz, Y.; Cohen, T.; Malard, P.; Xu, C. SN2-palmitate reduces fatty acid excretion in chinese formula-fed infants. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Manios, Y.; Karaglani, E.; Thijs-Verhoeven, I.; Vlachopapadopoulou, E.; Papazoglou, A.; Maragoudaki, E.; Manikas, Z.; Kampani, T.M.; Christaki, I.; Vonk, M.M.; et al. Effect of milk fat-based infant formulae on stool fatty acid soaps and calcium excretion in healthy term infants: Two double-blind randomised cross-over trials. BMC Nutr. 2020, 6, 46. [Google Scholar] [CrossRef] [PubMed]
- Yaron, S.; Shachar, D.; Abramas, L.; Riskin, A.; Bader, D.; Litmanovitz, I.; Bar-Yoseph, F.; Cohen, T.; Levi, L.; Lifshitz, Y.; et al. Effect of high β-palmitate content in infant formula on the intestinal microbiota of term infants. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Zhao, A.; Liu, B.; Ye, W.H.; Su, H.W.; Li, J.; Zhang, Y.M. Neurodevelopmental outcomes and gut bifidobacteria in term infants fed an infant formula containing high sn-2 palmitate: A cluster randomized clinical trial. Nutrients 2021, 13, 693. [Google Scholar] [CrossRef] [PubMed]
- Béghin, L.; Marchandise, X.; Lien, E.; Bricout, M.; Bernet, J.P.; Lienhardt, J.F.; Jeannerot, F.; Menet, V.; Requillart, J.C.; Marx, J.; et al. Growth, stool consistency and bone mineral content in healthy term infants fed sn-2-palmitate-enriched starter infant formula: A randomized, double-blind, multicentre clinical trial. Clin. Nutr. 2019, 38, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Huang, W.; Xu, X.; Wang, L.; Wang, Q.; Li, S.; Yuan, X. Stool Saponified Fatty acid, behavior, growth, and stool characteristics in infants fed a high-OPO formula: A randomized, double-blind clinical trial. Front. Pediatr. 2021, 9, 712201. [Google Scholar] [CrossRef] [PubMed]
- Litmanovitz, I.; Davidson, K.; Eliakim, A.; Regev, R.H.; Dolfin, T.; Arnon, S.; Bar-Yoseph, F.; Goren, A.; Lifshitz, Y.; Nemet, D. High Beta-palmitate formula and bone strength in term infants: A randomized, double-blind, controlled trial. Calcif. Tissue Int. 2013, 92, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Bronsky, J.; Campoy, C.; Embleton, N.; Fewtrell, M.; Mis, N.F.; Gerasimidis, K.; Hojsak, I.; Hulst, J.; Indrio, F.; Lapillonne, A.; et al. Palm oil and beta-palmitate in infant formula: A position paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 742–760. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, H.; Iseki, K.; Fujita, K. Development and differences of intestinal flora in the neonatal period in breast-fed and bottle-fed infants. Pediatrics 1983, 72, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Balmer, S.E.; Wharton, B.A. Diet and faecal flora in the newborn: Breast milk and infant formula. Arch. Dis. Child. 1989, 64, 1672–1677. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Bravo-Ruiseco, G.; Happe, R.; He, T.; van Dijl, J.M.; Harmsen, H.J.M. The effect of calcium palmitate on bacteria associated with infant gut microbiota. Microbiologyopen 2021, 10, e1187. [Google Scholar] [CrossRef] [PubMed]
- Guo, D.; Li, F.; Zhao, J.; Zhang, H.; Liu, B.; Pan, J.; Zhang, W.; Chen, W.; Xu, Y.; Jiang, S.; et al. Effect of an infant formula containing sn-2 palmitate on fecal microbiota and metabolome profiles of healthy term infants: A randomized, double-blind, parallel, controlled study. Food Funct. 2022, 13, 2003–2018. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, Y.; Zakharova, I.; Dmitrieva, Y. Oligosaccharides in infant formula: More evidence to validate the role of prebiotics. Br. J. Nutr. 2015, 113, 1339–1344. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, Y.; De Greef, E.; Veereman, G. Prebiotics in infant formula. Gut Microbes 2014, 5, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Greer, F.R. Calcium, phosphorus, and magnesium: How much is too much for infant formulas? J. Nutr. 1989, 119, 1846–1851. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.M.; Innis, S.M. Plasma lipoprotein fatty acids are altered by the positional distribution of fatty acids in infant formula triacylglycerols and human milk. Am. J. Clin. Nutr. 1999, 70, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare, Japan. National Growth Survey on Preschool Children. 2016. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000134208.html (accessed on 20 December 2023).
- Watanabe, Y.; Sato, S.; Asada, M.; Arishima, T.; Iida, Y.; Imagi, J.; Saito, K.; Sano, T.; Sasaki, A.; Sasaki, R.; et al. Enzymatic Analysis of Positional Fatty Acid Distributions in Triacylglycerols by 1(3)-Selective Transesterification with Candida antarctica Lipase B: A Collaborative Study. J. Oleo Sci. 2015, 64, 1193–1205. [Google Scholar] [CrossRef] [PubMed]
- Bligh, E.G.; Dyer, W.J. A rapid method of total lipid extraction and purification. Can. J. Biochem. Physiol. 1959, 37, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Bekkali, N.; Hamers, S.L.; Reitsma, J.B.; Van Toledo, L.; Benninga, M.A. Infant stool form scale: Development and results. J. Pediatr. 2009, 154, 521–526.e521. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Infant Formula | Sn-2 PA in Total PA | Category |
|---|---|---|
| (%) | ||
| A | 55.3 | High sn-2 PA milk |
| B | 52.9 | |
| C | 39.5 | Low sn-2 PA milk |
| D | 37.5 | |
| E | 11.9 | |
| F | 11.7 | |
| G | 11.4 | |
| H | 10.3 | |
| I | 6.4 | |
| J | 6.1 |
| Unit | Total (n = 149) | Sub-Grouped by Feeding Types | ||||
|---|---|---|---|---|---|---|
| Exclusively Breastfed Infants (n = 31) | Formula-Fed Infants | p Value * | ||||
| High sn-2 PA Milk-Fed (n = 40) | Low sn-2 PA Milk-Fed (n = 78) | |||||
| Maternal data | ||||||
| Age at birth | days | 34.4 ± 5.4 | 32.9 ± 4.8 | 34.5 ± 5.3 | 35.0 ± 5.5 | 0.172 |
| BMI before pregnancy | kg/m2 | 21.5 ± 3.5 | 21.1 ± 3.0 | 21.5 ± 3.5 | 21.6 ± 3.7 | 0.816 |
| Maximum BMI during pregnancy | kg/m2 | 25.5 ± 3.3 | 25.1 ± 2.7 | 25.6 ± 3.6 | 25.6 ± 3.4 | 0.749 |
| Nationality (not Japanese) | person | 2 (1.3%) | 0 (0%) | 1 (2.5%) | 1 (1.3%) | 0.667 |
| Missing | 1 (0.7%) | 1 (3.2%) | 0 (0%) | 0 (0%) | ||
| History of prior births before | person | 69 (46.3%) | 15 (48.4%) | 17 (42.5%) | 37 (47.4%) | 0.849 |
| C-section (yes) | person | 47 (31.5%) | 8 (25.8%) | 14 (35.0%) | 25 (32.1%) | 0.704 |
| Administration of antimicrobials before birth (yes) | person | 25 (16.8%) | 6 (19.4%) | 6 (15.0%) | 13 (16.7%) | 0.856 |
| Missing | 1 (0.7%) | 1 (3.2%) | 0 (0%) | 0 (0%) | ||
| Intake of lactobacillus/bifidobacteria supplements during pregnancy (yes) | person | 8 (5.4%) | 1 (3.2%) | 2 (5.0%) | 5 (6.4%) | 0.811 |
| Missing | 1 (0.7%) | 1 (3.2%) | 0 (0%) | 0 (0%) | ||
| Paternal data | ||||||
| Nationality (not Japanese) | person | 5 (3.4%) | 1 (3.2%) | 2 (5.0%) | 2 (2.6%) | 0.786 |
| Missing | 1 (0.7%) | 1 (3.2%) | 0 (0%) | 0 (0%) | ||
| Infant data | ||||||
| Sex (girls) | person | 80 (53.7%) | 16 (51.6%) | 24 (60.0%) | 40 (51.3%) | 0.665 |
| Missing | 1 (0.7%) | 1 (3.2%) | 0 (0%) | 0 (0%) | ||
| Gestational age at birth | weeks | 39.3 ± 1.1 | 39.3 ± 0.9 | 39.3 ± 1.2 | 39.2 ± 1.2 | 0.928 |
| Weight at birth | g | 3058.5 ± 304.9 | 3059.7 ± 280.9 | 3070.6 ± 295.1 | 3051.7 ± 321.9 | 0.951 |
| Length at birth | cm | 48.7 ± 2.9 | 48.6 ± 1.5 | 48.6 ± 1.6 | 48.8 ± 3.8 | 0.907 |
| Head circumference at birth | cm | 33.6 ± 1.2 | 33.4 ± 1.2 | 33.7 ± 1.1 | 33.7 ± 1.2 | 0.452 |
| Age at the 1-month clinical visit | days | 33.6 ± 5.3 | 33.9 ± 5.6 | 33.9 ± 4.0 | 33.3 ± 5.7 | 0.790 |
| Use of antimicrobials until 1 month (yes) | person | 3 (2.0%) | 0 (0%) | 0 (0%) | 3 (3.8%) | 0.248 |
| Feeding volume of infant formula | mL/day/kg | - | - | 67.4 ± 57.3 | 84.7 ± 61.8 | 0.143 |
| Formula-Fed | p-Value * | |||
|---|---|---|---|---|
| Exclusively Breastfed | High sn-2 PA Milk-Fed | Low sn-2 PA Milk-Fed | ||
| (n = 31) | (n = 40) | (n = 78) | ||
| At 1 month | ||||
| Weight (kg) | 4.4 ± 0.5 | 4.3 ± 0.4 | 4.3 ± 0.4 | 0.630 |
| Length (cm) | 53.9 ± 1.7 | 53.9 ± 1.8 | 53.6 ± 1.9 | 0.629 |
| Head circumference (cm) | 37.0 ± 1.2 | 37.0 ± 1.3 | 37.0 ± 1.1 | 0.990 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shoji, H.; Arai, H.; Kakiuchi, S.; Ito, A.; Sato, K.; Jinno, S.; Takahashi, N.; Masumoto, K.; Yoda, H.; Shimizu, T. Infant Formula with 50% or More of Palmitic Acid Bound to the sn-2 Position of Triacylglycerols Eliminate the Association between Formula-Feeding and the Increase of Fecal Palmitic Acid Levels in Newborns: An Exploratory Study. Nutrients 2024, 16, 1558. https://doi.org/10.3390/nu16111558
Shoji H, Arai H, Kakiuchi S, Ito A, Sato K, Jinno S, Takahashi N, Masumoto K, Yoda H, Shimizu T. Infant Formula with 50% or More of Palmitic Acid Bound to the sn-2 Position of Triacylglycerols Eliminate the Association between Formula-Feeding and the Increase of Fecal Palmitic Acid Levels in Newborns: An Exploratory Study. Nutrients. 2024; 16(11):1558. https://doi.org/10.3390/nu16111558
Chicago/Turabian StyleShoji, Hiromichi, Hiroko Arai, Satsuki Kakiuchi, Atsushi Ito, Keigo Sato, Shinji Jinno, Naoto Takahashi, Kenichi Masumoto, Hitoshi Yoda, and Toshiaki Shimizu. 2024. "Infant Formula with 50% or More of Palmitic Acid Bound to the sn-2 Position of Triacylglycerols Eliminate the Association between Formula-Feeding and the Increase of Fecal Palmitic Acid Levels in Newborns: An Exploratory Study" Nutrients 16, no. 11: 1558. https://doi.org/10.3390/nu16111558
APA StyleShoji, H., Arai, H., Kakiuchi, S., Ito, A., Sato, K., Jinno, S., Takahashi, N., Masumoto, K., Yoda, H., & Shimizu, T. (2024). Infant Formula with 50% or More of Palmitic Acid Bound to the sn-2 Position of Triacylglycerols Eliminate the Association between Formula-Feeding and the Increase of Fecal Palmitic Acid Levels in Newborns: An Exploratory Study. Nutrients, 16(11), 1558. https://doi.org/10.3390/nu16111558