
Association between Dietary Patterns during Pregnancy and Children’s Neurodevelopment: A Birth Cohort Study


Abstract

1. Introduction
2. Methods and Materials
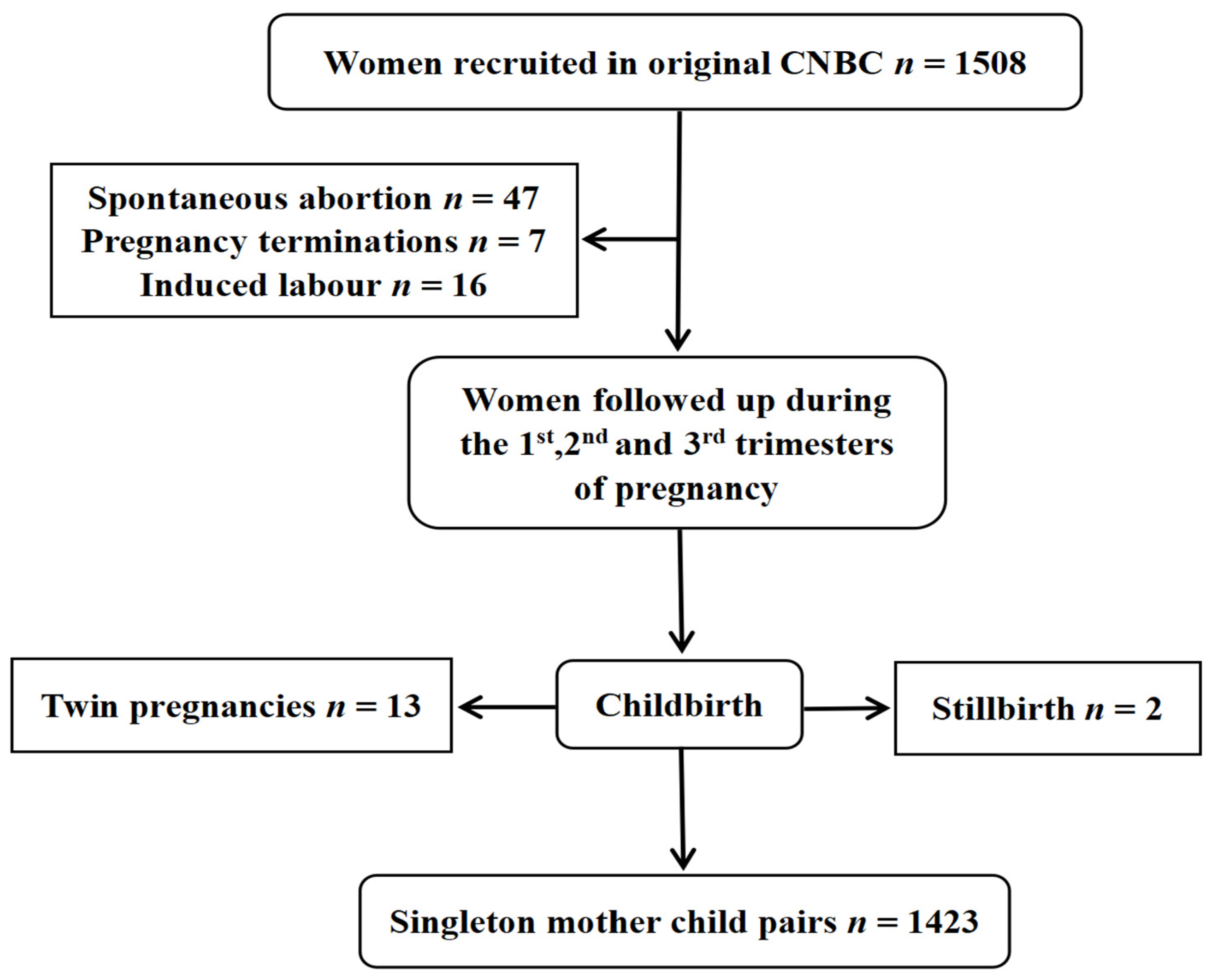
2.1. Study Population
2.2. Dietary Assessment
2.3. Food Pattern Determination
2.4. Evaluation of Children’s Neurodevelopment
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Participants
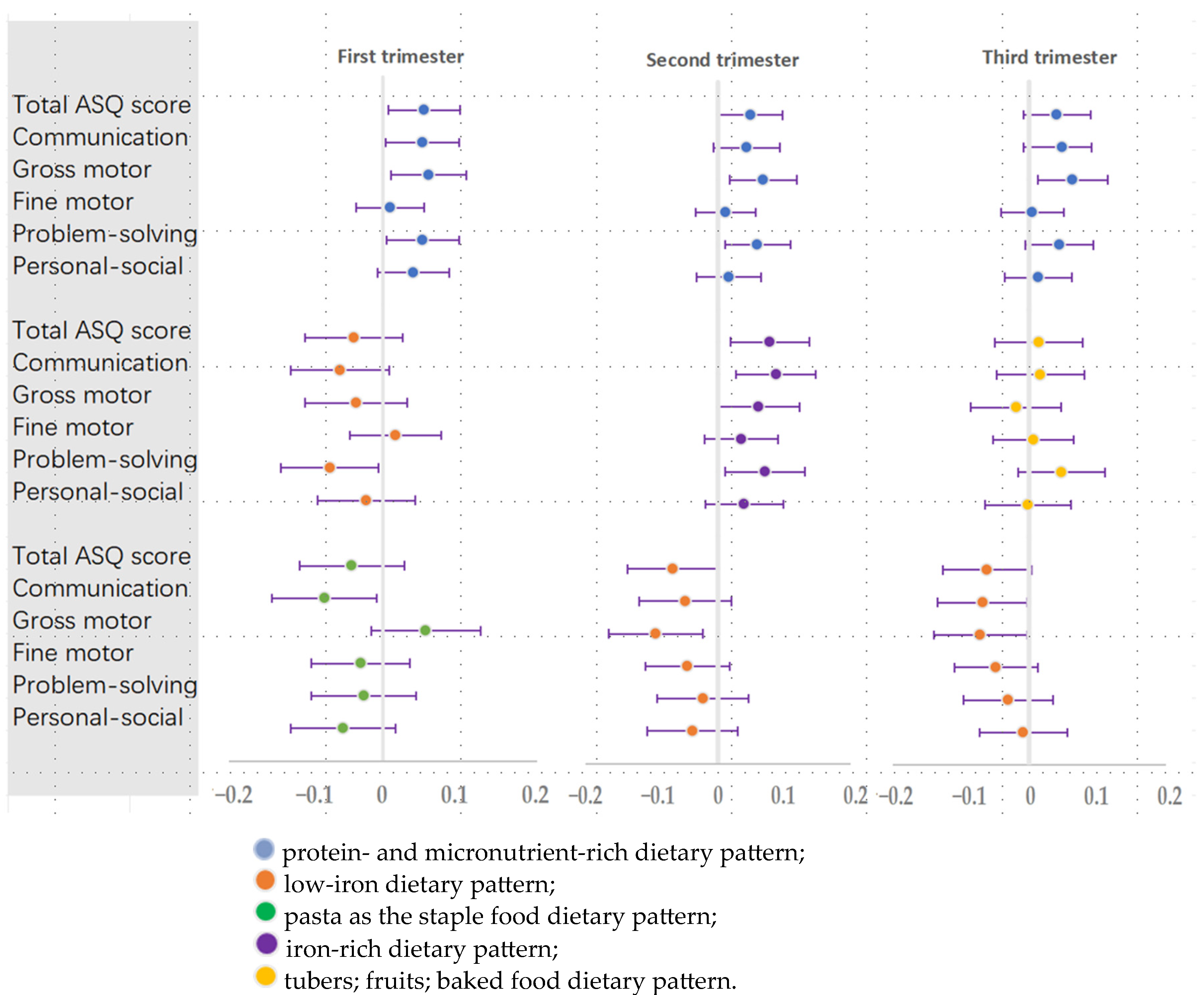
3.2. Association between Dietary Pattern Scores during Pregnancy and Children’s Neurodevelopment
3.3. Characteristics of the Distinct Protein- and Micronutrient-Rich Dietary Pattern Trajectory Groups
3.4. Characteristics of the Distinct Low-Iron Dietary Pattern Trajectory Groups
3.5. Associations between Trajectories of Women’s Protein- and Micronutrient-Rich Dietary Pattern Scores in the Three Periods of Pregnancy and Children’s Neurodevelopment
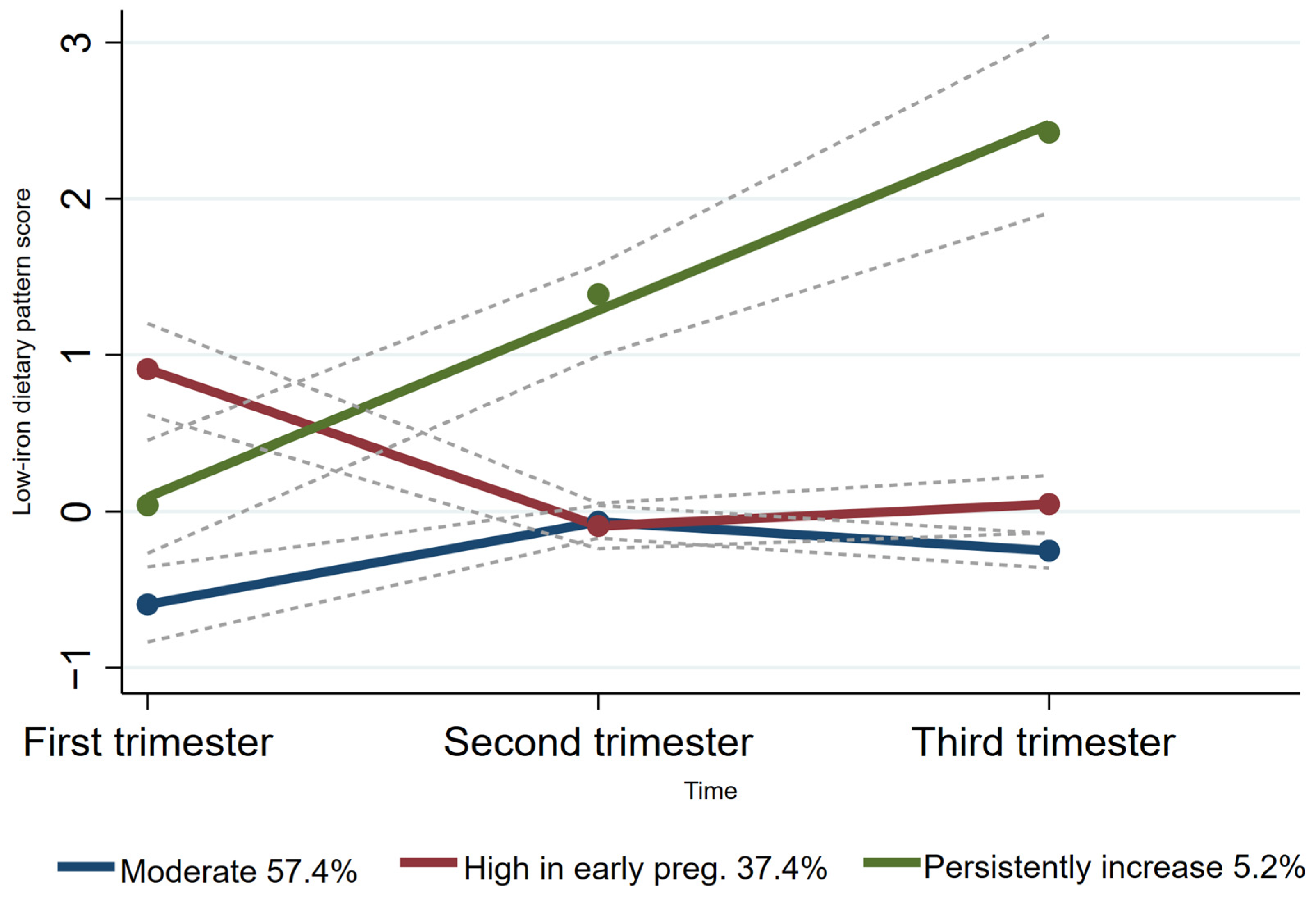
3.6. Associations between Trajectories of Women’s Low-Iron Dietary Pattern Scores in the Three Periods of Pregnancy and Children’s Neurodevelopment
3.7. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barker, D.J.P. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Prado, E.L.; Larson, L.M.; Cox, K.; Bettencourt, K.; Kubes, J.N.; Shankar, A.H. Do effects of early life interventions on linear growth correspond to effects on neurobehavioural development? A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e1398–e1413. [Google Scholar] [CrossRef] [PubMed]
- Fleming, T.P.; Watkins, A.J.; Velazquez, M.A.; Mathers, J.C.; Prentice, A.M.; Stephenson, J.; Barker, M.; Saffery, R.; Yajnik, C.S.; Eckert, J.J.; et al. Origins of lifetime health around the time of conception: Causes and consequences. Lancet 2018, 391, 1842–1852. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Rodrigues, M.; Rosário, R.; Duarte, A.; Silva, M.J.; Augusto, C.; Rodrigues, M.; Padrão, P.; Moreira, P. Neurodevelopment and Dietary Intake in Toddlers—A Cross-Sectional Study from the Healthy Children 2021 Project. Nutrients 2023, 15, 5105. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Brands, B.; Demmelmair, H. The Early Nutrition Programming Project (EARNEST): 5 y of successful multidisciplinary collaborative research. Am. J. Clin. Nutr. 2011, 94, S1749–S1753. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Albornoz, M.C.; García-Guáqueta, D.P.; Velez-van-Meerbeke, A.; Talero-Gutiérrez, C. Maternal Nutrition and Neurodevelopment: A Scoping Review. Nutrients 2021, 13, 3530. [Google Scholar] [CrossRef] [PubMed]
- Basak, S.; Mallick, R.; Duttaroy, A.K. Maternal Docosahexaenoic Acid Status during Pregnancy and Its Impact on Infant Neurodevelopment. Nutrients 2020, 12, 3615. [Google Scholar] [CrossRef]
- Gernand, A.D.; Schulze, K.J.; Stewart, C.P.; West, K.P.; Christian, P. Micronutrient deficiencies in pregnancy worldwide: Health effects and prevention. Nat. Rev. Endocrinol. 2016, 12, 274–289. [Google Scholar] [CrossRef]
- Pitkin, R.M. Folate and neural tube defects. Am. J. Clin. Nutr. 2007, 85, 285S–288S. [Google Scholar] [CrossRef]
- Freitas-Vilela, A.A.; Pearson, R.M.; Emmett, P.; Heron, J.; Smith, A.D.A.C.; Emond, A.; Hibbeln, J.R.; Castro, M.B.T.; Kac, G. Maternal dietary patterns during pregnancy and intelligence quotients in the offspring at 8 years of age: Findings from the ALSPAC cohort. Matern. Child Nutr. 2017, 14, e12431. [Google Scholar] [CrossRef]
- Lv, S.; Qin, R.; Jiang, Y.; Lv, H.; Lu, Q.; Tao, S.; Huang, L.; Liu, C.; Xu, X.; Wang, Q.; et al. Association of Maternal Dietary Patterns during Gestation and Offspring Neurodevelopment. Nutrients 2022, 14, 730. [Google Scholar] [CrossRef] [PubMed]
- Dai, F.; Wang, P.; Li, Q.; Zhang, L.; Yu, L.; Wu, L.; Tao, R.; Zhu, P. Mediterranean diet during pregnancy and infant neurodevelopment: A prospective birth cohort study. Front. Nutr. 2023, 9, 1078481. [Google Scholar] [CrossRef] [PubMed]
- Steenweg-de Graaff, J.; Tiemeier, H.; Steegers-Theunissen, R.P.M.; Hofman, A.; Jaddoe, V.W.V.; Verhulst, F.C.; Roza, S.J. Maternal dietary patterns during pregnancy and child internalising and externalising problems. The Generation R Study. Clin. Nutr. 2014, 33, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Galera, C.; Heude, B.; Forhan, A.; Bernard, J.Y.; Peyre, H.; Van Der Waerden, J.; Pryor, L.; Bouvard, M.P.; Melchior, M.; Lioret, S.; et al. Prenatal diet and children’s trajectories of hyperactivity–inattention and conduct problems from 3 to 8 years: The EDEN mother–child cohort. J. Child Psychol. Psychiatry 2018, 59, 1003–1011. [Google Scholar] [CrossRef]
- Sotres-Alvarez, D.; Herring, A.H.; Siega-Riz, A.-M. Latent Transition Models to Study Women’s Changing of Dietary Patterns from Pregnancy to 1 Year Postpartum. Am. J. Epidemiol. 2013, 177, 852–861. [Google Scholar] [CrossRef]
- Lee, Y.Q.; Colega, M.; Sugianto, R.; Lai, J.S.; Godfrey, K.M.; Tan, K.H.; Shek, L.P.C.; Loy, S.L.; Müller-Riemenschneider, F.; Padmapriya, N.; et al. Tracking of dietary patterns between pregnancy and 6 years post-pregnancy in a multiethnic Asian cohort: The Growing Up in Singapore Towards healthy Outcomes (GUSTO) study. Eur. J. Nutr. 2022, 61, 985–1001. [Google Scholar] [CrossRef]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Laura, S.; Walter C, W. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Hayati Rezvan, P.; Lee, K.J.; Simpson, J.A. The rise of multiple imputation: A review of the reporting and implementation of the method in medical research. BMC Med. Res. Methodol. 2015, 15, 30. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef]
- Kerstjens, J.M.; Bos, A.F. Support for the global feasibility of the Ages and Stages Questionnaire as developmental screener. Early Hum. Dev. 2009, 85, 443–447. [Google Scholar] [CrossRef]
- Manti, F.; Giovannone, F.; Ciancaleoni, M.; De Vita, G.; Fioriello, F.; Gigliotti, F.; Sogos, C. Psychometric Properties and Validation of the Italian Version of Ages & Stages Questionnaires Third Edition. Int. J. Environ. Res. Public Health 2023, 20, 5014. [Google Scholar] [CrossRef] [PubMed]
- Diemer, E.W.; Hudson, J.I.; Javaras, K.N. More (Adjustment) Is Not Always Better: How Directed Acyclic Graphs Can Help Researchers Decide Which Covariates to Include in Models for the Causal Relationship between an Exposure and an Outcome in Observational Research. Psychother. Psychosom. 2021, 90, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Cosco, T.D.; Lachance, C.C.; Blodgett, J.M.; Stubbs, B.; Co, M.; Veronese, N.; Wu, Y.T.; Prina, A.M. Latent structure of the Centre for Epidemiologic Studies Depression Scale (CES-D) in older adult populations: A systematic review. Aging Ment. Health 2020, 24, 700–704. [Google Scholar] [CrossRef] [PubMed]
- Zung, W.W.K. A Rating Instrument for Anxiety Disorders. Psychosomatics 1971, 12, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.L.; Nagin, D.S. A Note on a Stata Plugin for Estimating Group-based Trajectory Models. Sociol. Methods Res. 2013, 42, 608–613. [Google Scholar] [CrossRef]
- Nagin, D.S. Group-Based Trajectory Modeling: An Overview. Ann. Nutr. Metab. 2014, 65, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Dalrymple, K.V.; Vogel, C.; Flynn, A.C.; Seed, P.T.; Godfrey, K.M.; Poston, L.; Inskip, H.M.; Crozier, S.R. Longitudinal dietary trajectories from pregnancy to 3 years post delivery in women with obesity: Relationships with adiposity. Obesity 2023, 31, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Pervin, S.; Emmett, P.; Northstone, K.; Townsend, N.; Fatima, Y.; Huda, M.M.; McIntyre, H.D.; Mamun, A.A. Trajectories of dietary patterns from pregnancy to 12 years post-pregnancy and associated maternal characteristics: Evidence from the Avon Longitudinal Study of Parents and Children. Eur. J. Nutr. 2023, 62, 2763–2777. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-Y. Determining the Number of Latent Classes in Single- and Multiphase Growth Mixture Models. Struct. Equ. Model. Multidiscip. J. 2014, 21, 263–279. [Google Scholar] [CrossRef]
- Xu, J.; Wang, H.; Bian, J.; Xu, M.; Jiang, N.; Luo, W.; Zu, P.; Yin, W.; Zhu, P. Association between the Maternal Mediterranean Diet and Perinatal Outcomes: A Systematic Review and Meta-Analysis. Adv. Nutr. 2024, 15, 100159. [Google Scholar] [CrossRef]
- Perumal, N.; Manji, K.P.; Darling, A.M.; Kisenge, R.R.; Kvestad, I.; Hysing, M.; Belinger, D.C.; Urassa, W.; Strand, T.A.; Duggan, C.P.; et al. Gestational Age, Birth Weight, and Neurocognitive Development in Adolescents in Tanzania. J. Pediatr. 2021, 236, 194–203.e6. [Google Scholar] [CrossRef] [PubMed]
- Koh, K. Maternal breastfeeding and children’s cognitive development. Soc. Sci. Med. 2017, 187, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Amaro, A.; Baptista, F.I.; Matafome, P. Programming of future generations during breastfeeding: The intricate relation between metabolic and neurodevelopment disorders. Life Sci. 2022, 298, 120526. [Google Scholar] [CrossRef] [PubMed]
- Xiang, X.; Yang, T.; Chen, J.; Chen, L.; Dai, Y.; Zhang, J.; Li, L.; Jia, F.; Wu, L.; Hao, Y.; et al. Association of feeding patterns in infancy with later autism symptoms and neurodevelopment: A national multicentre survey. BMC Psychiatry 2023, 23, 174. [Google Scholar] [CrossRef] [PubMed]
- Georgieff, M.K.; Ramel, S.E.; Cusick, S.E. Nutritional influences on brain development. Acta Paediatr. 2018, 107, 1310–1321. [Google Scholar] [CrossRef] [PubMed]
- Belluscio, L.M.; Berardino, B.G.; Ferroni, N.M.; Ceruti, J.M.; Cánepa, E.T. Early protein malnutrition negatively impacts physical growth and neurological reflexes and evokes anxiety and depressive-like behaviors. Physiol. Behav. 2014, 129, 237–254. [Google Scholar] [CrossRef]
- Miyake, K.; Mochizuki, K.; Kushima, M.; Shinohara, R.; Horiuchi, S.; Otawa, S.; Akiyama, Y.; Ooka, T.; Kojima, R.; Yokomichi, H.; et al. Maternal protein intake in early pregnancy and child development at age 3 years. Pediatr. Res. 2023, 94, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Godoy, M.A.D.; Souza, A.S.D.; Lobo, M.A.; Sampaio, O.V.K.; Moraes, L.; Baldanza, M.R.; Magri, T.P.R.; de Castro, J.P.S.W.; do Carmo, M.D.G.T.; Soares-Mota, M.; et al. Effects of protein restriction during gestation and lactation on cell proliferation in the hippocampus and subventricular zone: Functional implications. Protein restriction alters hippocampal/SVZ cell proliferation. Brain Res. 2013, 1496, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Rotta, L.N.; Schmidt, A.P.; Souza, K.B.; Izquierdo, I.A.; Perry, M.L.S.; Souza, D.O. Effects of Undernutrition on Glutamatergic Parameters in Rat Brain. Neurochem. Res. 2003, 28, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Gressens, P.; Muaku, S.M.; Besse, L.; Nsegbe, E.; Gallego, J.; Delpech, B.; Gaultier, C.; Evrard, P.; Ketelslegers, J.M.; Maiter, D. Maternal protein restriction early in rat pregnancy alters brain development in the progeny. Dev. Brain Res. 1997, 103, 21–35. [Google Scholar] [CrossRef]
- Mokler, D.J.; Torres, O.I.; Galler, J.R.; Morgane, P.J. Stress-induced changes in extracellular dopamine and serotonin in the medial prefrontal cortex and dorsal hippocampus of prenatally malnourished rats. Brain Res. 2007, 1148, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Kehoe, P.; Mallinson, K.; Bronzino, J.; McCormick, C.M. Effects of prenatal protein malnutrition and neonatal stress on CNS responsiveness. Dev. Brain Res. 2001, 132, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Resnick, O.; Morgane, P.J. Ontogeny of the levels of serotonin in various parts of the brain in severely protein malnourished rats. Brain Res. 1984, 303, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Amarger, V.; Lecouillard, A.; Ancellet, L.; Grit, I.; Castellano, B.; Hulin, P.; Parnet, P. Protein Content and Methyl Donors in Maternal Diet Interact to Influence the Proliferation Rate and Cell Fate of Neural Stem Cells in Rat Hippocampus. Nutrients 2014, 6, 4200–4217. [Google Scholar] [CrossRef] [PubMed]
- Glinoer, D. Iodine Nutrition Requirements During Pregnancy. Thyroid 2006, 16, 947–948. [Google Scholar] [CrossRef] [PubMed]
- Becker, D.V.; Braverman, L.E.; Delange, F.; Dunn, J.T.; Franklyn, J.A.; Hollowell, J.G.; Lamm, S.H.; Mitchell, M.L.; Pearce, E.; Robbins, J.; et al. Iodine Supplementation for Pregnancy and Lactation—United States and Canada: Recommendations of the American Thyroid Association. Thyroid 2006, 16, 949–951. [Google Scholar] [CrossRef] [PubMed]
- Coker, S.J.; Smith-Díaz, C.C.; Dyson, R.M.; Vissers, M.C.M.; Berry, M.J. The Epigenetic Role of Vitamin C in Neurodevelopment. Int. J. Mol. Sci. 2022, 23, 1208. [Google Scholar] [CrossRef] [PubMed]
- Strain, J.J.; Bonham, M.P.; Duffy, E.M.; Wallace, J.M.W.; Robson, P.J.; Clarkson, T.W.; Shamlaye, C. Nutrition and neurodevelopment: The search for candidate nutrients in the Seychelles Child Development Nutrition Study. Neurotoxicology 2020, 81, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Thilakaratne, R.; Lin, P.-I.D.; Rifas-Shiman, S.L.; Wright, R.O.; Hubbard, A.; Hivert, M.-F.; Bellinger, D.; Oken, E.; Cardenas, A. Mixtures of Metals and Micronutrients in Early Pregnancy and Cognition in Early and Mid-Childhood: Findings from the Project Viva Cohort. Environ. Health Perspect. 2023, 131, 087008. [Google Scholar] [CrossRef] [PubMed]
- Jahan-Mihan, A.; Rodriguez, J.; Christie, C.; Sadeghi, M.; Zerbe, T. The Role of Maternal Dietary Proteins in Development of Metabolic Syndrome in Offspring. Nutrients 2015, 7, 9185–9217. [Google Scholar] [CrossRef]
- Hallam, M.C.; Reimer, R.A. A maternal high-protein diet predisposes female offspring to increased fat mass in adulthood whereas a prebiotic fibre diet decreases fat mass in rats. Br. J. Nutr. 2013, 110, 1732–1741. [Google Scholar] [CrossRef] [PubMed]
- Hua, M.; Shi, D.; Xu, W.; Zhu, L.; Hao, X.; Zhu, B.; Shu, Q.; Lozoff, B.; Geng, F.; Shao, J. Differentiation between fetal and postnatal iron deficiency in altering brain substrates of cognitive control in pre-adolescence. BMC Med. 2023, 21, 167. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, L.; Canals, J.; Arija, V. Effects of prenatal iron status on child neurodevelopment and behavior: A systematic review. Crit. Rev. Food Sci. Nutr. 2018, 58, 1604–1614. [Google Scholar] [CrossRef] [PubMed]
- McCann, J.C.; Ames, B.N. An overview of evidence for a causal relation between iron deficiency during development and deficits in cognitive or behavioral function. Am. J. Clin. Nutr. 2007, 85, 931–945. [Google Scholar] [CrossRef] [PubMed]
- Wu, L. Effect of perinatal iron deficiency on myelination and associated behaviors in rat pups. Behav. Brain Res. 2008, 188, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Arija, V.; Hernández-Martínez, C.; Tous, M.; Canals, J.; Guxens, M.; Fernández-Barrés, S.; Ibarluzea, J.; Babarro, I.; Soler-Blasco, R.; Llop, S.; et al. Association of Iron Status and Intake During Pregnancy with Neuropsychological Outcomes in Children Aged 7 Years: The Prospective Birth Cohort Infancia y Medio Ambiente (INMA) Study. Nutrients 2019, 11, 2999. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Xu, X.; Shi, Z. Trajectories of Dietary Patterns, Sleep Duration, and Body Mass Index in China: A Population-Based Longitudinal Study from China Nutrition and Health Survey, 1991–2009. Nutrients 2020, 12, 2245. [Google Scholar] [CrossRef]
- Wu, F.; Pahkala, K.; Juonala, M.; Rovio, S.P.; Sabin, M.A.; Rönnemaa, T.; Buscot, M.J.; Smith, K.J.; Männistö, S.; Jula, A.; et al. Dietary Pattern Trajectories from Youth to Adulthood and Adult Risk of Impaired Fasting Glucose: A 31-year Cohort Study. J. Clin. Endocrinol. Metab. 2021, 106, e2078–e2086. [Google Scholar] [CrossRef]
- Zhao, Q.; Peng, C.; Wu, X.; Chen, Y.; Wang, C.; You, Z. Maternal sleep deprivation inhibits hippocampal neurogenesis associated with inflammatory response in young offspring rats. Neurobiol. Dis. 2014, 68, 57–65. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Distributions |
|---|---|
| Demographic characteristics | |
| Maternal educational level [n (%)] | |
| Junior high school or below | 8 (0.6) |
| Senior middle school | 507 (35.6) |
| Junior college or above | 908 (63.8) |
| Annual household income (CNY one million) * [n (%)] | |
| <5 | 192 (13.5) |
| 5~10 | 698 (49.1) |
| 10~20 | 412 (29.0) |
| 20~30 | 95 (6.7) |
| >30 | 24 (1.7) |
| Maternal characteristics | |
| Maternal age, years (Mean ± SD) | 28.7 ± 4.0 |
| Body mass index before pregnancy * [n (%)] | |
| Underweight (BMI < 18.5) | 227 (16.0) |
| Normal (18.5 ≤ BMI < 24.9) | 1028 (72.2) |
| Overweight obesity (BMI ≥ 24.9) | 164 (11.5) |
| Maternal occupation [n (%)] | |
| Brain work | 637 (44.8) |
| Manual work | 509 (35.8) |
| Else | 88 (6.2) |
| No work | 189 (13.3) |
| Smoking during pregnancy * [n (%)] | |
| Yes | 30 (2.1) |
| No | 1389 (97.6) |
| Alcohol during pregnancy * [n (%)] | |
| Yes | 352 (24.7) |
| No | 1067 (75.0) |
| Hypertension during pregnancy * [n (%)] | |
| Yes | 13 (0.9) |
| No | 1302 (91.5) |
| Diabetes mellitus during pregnancy * [n (%)] | |
| Yes | 317 (22.3) |
| No | 998 (70.1) |
| Pregnancy anxiety * (Mean ± SD) | 39.5 ± 8.0 |
| Pregnancy depression * (Mean ± SD) | 13.7 ± 7.9 |
| Parity * (Mean ± SD) | |
| 0 | 11 (0.8) |
| 1 | 574 (40.3) |
| 2 | 306 (21.5) |
| 3 | 2 (0.1) |
| Children’s characteristics | |
| Gestational weeks * (Mean ± SD) | 38.9 ± 1.4 |
| Neonatal weight (g) * (Mean ± SD) | 3353 ± 463 |
| Exclusive breastfeeding for 6 months * [n (%)] | |
| Yes | 633 (44.5) |
| No | 603 (49.4) |
| Complementary food within 6 months * [n (%)] | |
| Yes | 524 (36.8) |
| No | 845 (59.4) |
| Maternal Dietary Pattern | Model | Total ASQ Score | Communication | Gross Motor | Fine Motor | Problem-Solving | Personal-Social |
|---|---|---|---|---|---|---|---|
| First trimester | |||||||
| Protein- and micronutrient-rich | 1 | 0.035 (0.005, 0.065) | 0.041 (0.011, 0.072) | 0.021 (−0.010, 0.051) | 0.015 (−0.015, 0.045) | 0.033 (0.002, 0.063) | 0.021 (−0.009, 0.051) |
| 2 | 0.053 (0.006, 0.100) | 0.051 (0.003, 0.098) | 0.059 (0.010, 0.108) | 0.009 (−0.035, 0.053) | 0.051 (0.004, 0.098) | 0.039 (−0.007, 0.086) | |
| Low-iron | 1 | −0.042 (−0.083, 0.001) | −0.056 (−0.097, −0.014) | −0.033 (−0.074, 0.009) | −0.011 (−0.053, 0.030) | −0.062 (−0.104, 0.021) | −0.003 (−0.045, 0.039) |
| 2 | −0.038 (−0.102, 0.025) | −0.056 (−0.120, 0.008) | −0.035 (−0.102, 0.031) | 0.016 (−0.043, 0.075) | −0.069 (−0.133, −0.006) | −0.022 (−0.085, 0.041) | |
| Pasta as the staple food | 1 | −0.028 (−0.074, 0.017) | −0.033 (−0.079, 0.012) | 0.006 (−0.040, 0.052) | −0.021 (−0.067, 0.025) | −0.009 (−0.055, 0.036) | −0.035 (−0.081, 0.011) |
| 2 | −0.041 (−0.109, 0.027) | −0.076 (−0.145, −0.008) | 0.055 (−0.016, 0.126) | −0.029 (−0.093, 0.035) | −0.025 (−0.094, 0.043) | −0.052 (−0.120, 0.016) | |
| Second trimester | |||||||
| Protein- and micronutrient-rich | 1 | 0.021 (−0.012, 0.054) | 0.017 (−0.016, 0.050) | 0.025 (−0.008, 0.059) | 0.006 (−0.027, 0.040) | 0.034 (0.001, 0.067) | 0.001 (−0.033, 0.033) |
| 2 | 0.049 (0.001, 0.098) | 0.043 (−0.007, 0.093) | 0.068 (0.017, 0.119) | 0.011 (−0.035, 0.057) | 0.059 (0.010, 0.109) | 0.016 (−0.033, 0.065) | |
| Iron-rich | 1 | 0.056 (0.015, 0.097) | 0.076 (0.035, 0.117) | 0.036 (−0.005, 0.077) | 0.010 (−0.031, 0.051) | 0.057 (0.016, 0.098) | 0.039 (−0.002, 0.080) |
| 2 | 0.078 (0.018, 0.138) | 0.088 (0.027, 0.148) | 0.061 (−0.002, 0.123) | 0.035 (−0.021, 0.090) | 0.071 (0.011, 0.131) | 0.039 (−0.020, 0.099) | |
| Low-iron | 1 | −0.032 (−0.079, 0.015) | −0.048 (−0.095, −0.001) | −0.049 (−0.096, −0.002) | −0.014 (−0.061, 0.033) | −0.001 (−0.048, 0.046) | −0.017 (−0.064, 0.030) |
| 2 | −0.069 (−0.138, 0.001) | −0.050 (−0.120, 0.020) | −0.095 (−0.167, −0.023) | −0.047 (−0.111, 0.017) | −0.023 (−0.093, 0.046) | −0.039 (−0.108, 0.030) | |
| Third trimester | |||||||
| Protein- and micronutrient-rich | 1 | 0.017 (−0.017, 0.051) | 0.013 (−0.021, 0.047) | 0.028 (−0.006, 0.062) | 0.003 (−0.031, 0.037) | 0.020 (−0.014, 0.054) | 0.006 (−0.028, 0.040) |
| 2 | 0.040 (−0.009, 0.089) | 0.048 (−0.008, 0.091) | 0.063 (0.012, 0.114) | 0.004 (−0.041, 0.050) | 0.044 (−0.006, 0.093) | 0.013 (−0.036, 0.062) | |
| Tubers; fruits; baked food | 1 | 0.004 (−0.036, 0.044) | −0.020 (−0.060, 0.019) | −0.022 (−0.061, 0.018) | 0.004 (−0.036, 0.044) | 0.028 (−0.012, 0.068) | 0.011 (−0.028, 0.051) |
| 2 | 0.014 (−0.050, 0.078) | 0.016 (−0.048, 0.080) | −0.019 (−0.086, 0.047) | 0.006 (−0.053, 0.065) | 0.047 (−0.017, 0.111) | −0.002 (−0.065, 0.061) | |
| Low-iron | 1 | −0.037 (−0.083, 0.009) | −0.055 (−0.101, −0.009) | −0.039 (−0.085, 0.007) | −0.028 (−0.073, 0.018) | −0.014 (−0.059, 0.032) | −0.004 (−0.050, 0.042) |
| 2 | −0.062 (−0.127, 0.003) | −0.068 (−0.134, −0.003) | −0.072 (−0.140, −0.004) | −0.049 (−0.109, 0.012) | −0.031 (−0.096, 0.035) | −0.009 (−0.073, 0.056) |
| Maternal Dietary Pattern Trajectories | Total ASQ Score | Communication | Gross Motor | Fine Motor | Problem-Solving | Personal-Social |
|---|---|---|---|---|---|---|
| Protein- and micronutrient-rich | ||||||
| Model 1 | 3.007 (−0.157, 6.171) | 0.500 (−0.213, 1.213) | 0.725 (0.070, 1.379) | 0.766 (−0.565, 2.097) | 0.897 (0.041, 1.752) | 0.119 (−0.853, 1.092) |
| Model 2 | 5.107 (0.464, 9.750) | 0.939 (−0.109, 1.987) | 1.279 (0.289, 2.269) | 0.994 (−0.837, 2.825) | 1.478 (0.221, 2.735) | 0.417 (−1.004, 1.838) |
| Low-iron | ||||||
| Model 1 | −2.063 (−5.992, 1.866) | −0.040 (−0.921, 0.841) | −0.334 (−1.140, 0.473) | −0.882 (−2.536, 0.772) | −0.478 (−1.537, 0.581) | −0.329 (−1.538, 0.879) |
| Model 2 | −1.032 (−6.670, 4.607) | −0.410 (−1.682, 0.861) | −0.112 (−1.316, 1.091) | −0.854 (−3.071, 1.363) | 0.098 (−1.429, 1.625) | 0.246 (−1.474, 1.967) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ouyang, J.; Cai, W.; Wu, P.; Tong, J.; Gao, G.; Yan, S.; Tao, F.; Huang, K. Association between Dietary Patterns during Pregnancy and Children’s Neurodevelopment: A Birth Cohort Study. Nutrients 2024, 16, 1530. https://doi.org/10.3390/nu16101530
Ouyang J, Cai W, Wu P, Tong J, Gao G, Yan S, Tao F, Huang K. Association between Dietary Patterns during Pregnancy and Children’s Neurodevelopment: A Birth Cohort Study. Nutrients. 2024; 16(10):1530. https://doi.org/10.3390/nu16101530
Chicago/Turabian StyleOuyang, Jiajun, Wenjin Cai, Penggui Wu, Juan Tong, Guopeng Gao, Shuangqin Yan, Fangbiao Tao, and Kun Huang. 2024. "Association between Dietary Patterns during Pregnancy and Children’s Neurodevelopment: A Birth Cohort Study" Nutrients 16, no. 10: 1530. https://doi.org/10.3390/nu16101530
APA StyleOuyang, J., Cai, W., Wu, P., Tong, J., Gao, G., Yan, S., Tao, F., & Huang, K. (2024). Association between Dietary Patterns during Pregnancy and Children’s Neurodevelopment: A Birth Cohort Study. Nutrients, 16(10), 1530. https://doi.org/10.3390/nu16101530