
The Effects of a High-Carbohydrate versus a High-Fat Shake on Biomarkers of Metabolism and Glycemic Control When Used to Interrupt a 38-h Fast: A Randomized Crossover Study

 , ,
, , 

 , and
, and 
Highlights
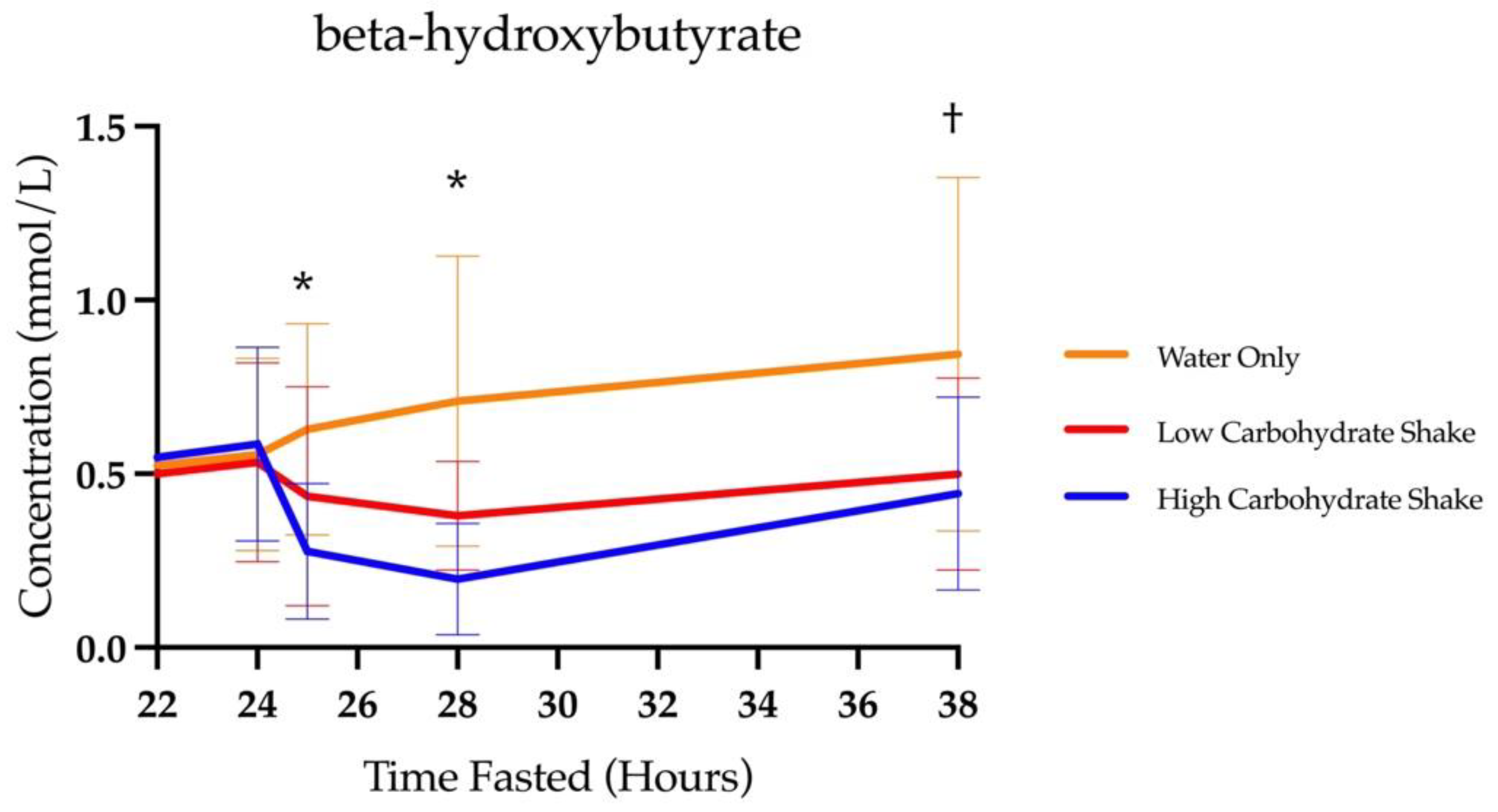
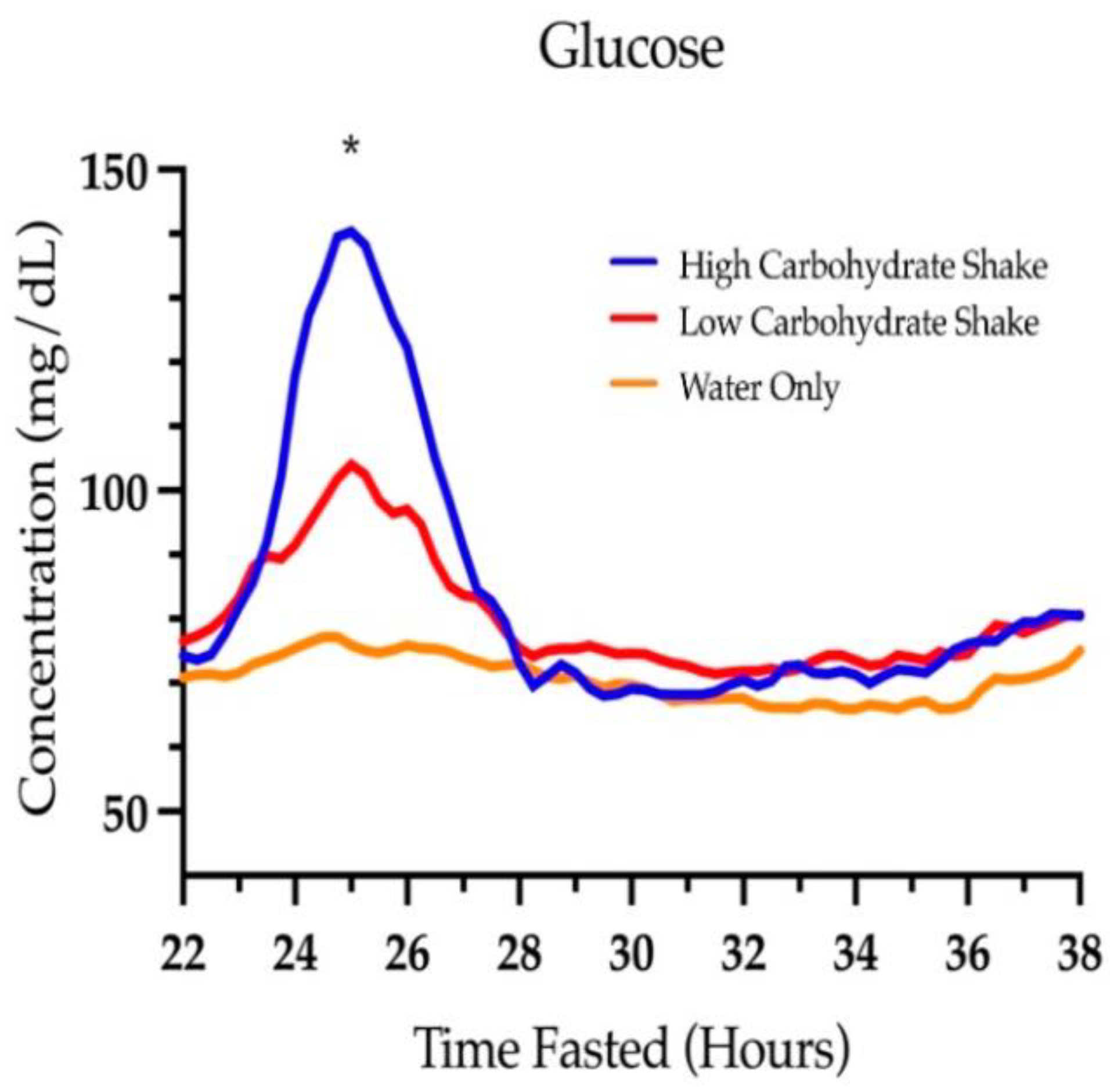
- Breaking a 24-hour fast with a low carbohydrate/high fat (LC/HF) shake maintained higher levels of beta-hydroxybutyrate (BHB), lower glucose, and lower insulin compared to the high carbohydrate/low fat (HC/LF) shake, which more closely mimicked a fasting metabolic state.
- Both shakes increased glucose and insulin levels compared to the water-only fast, but the LC/HF shake resulted in a smaller increase and quicker recovery, while the HC/LF shake caused a more significant disruption in metabolic markers such as insulin and glucagon.
- The LC/HF shake may be a beneficial strategy for those seeking to extend some metabolic benefits of fasting, such as maintaining elevated ketone levels and reducing insulin spikes, which could support metabolic health and flexibility.
- Given the reduced glycemic variability observed with the LC/HF shake, this approach may help minimize the risks associated with high glucose variability, such as insulin resistance, cardiovascular disease, and other metabolic disorders.
Abstract
1. Introduction
2. Materials and Methods
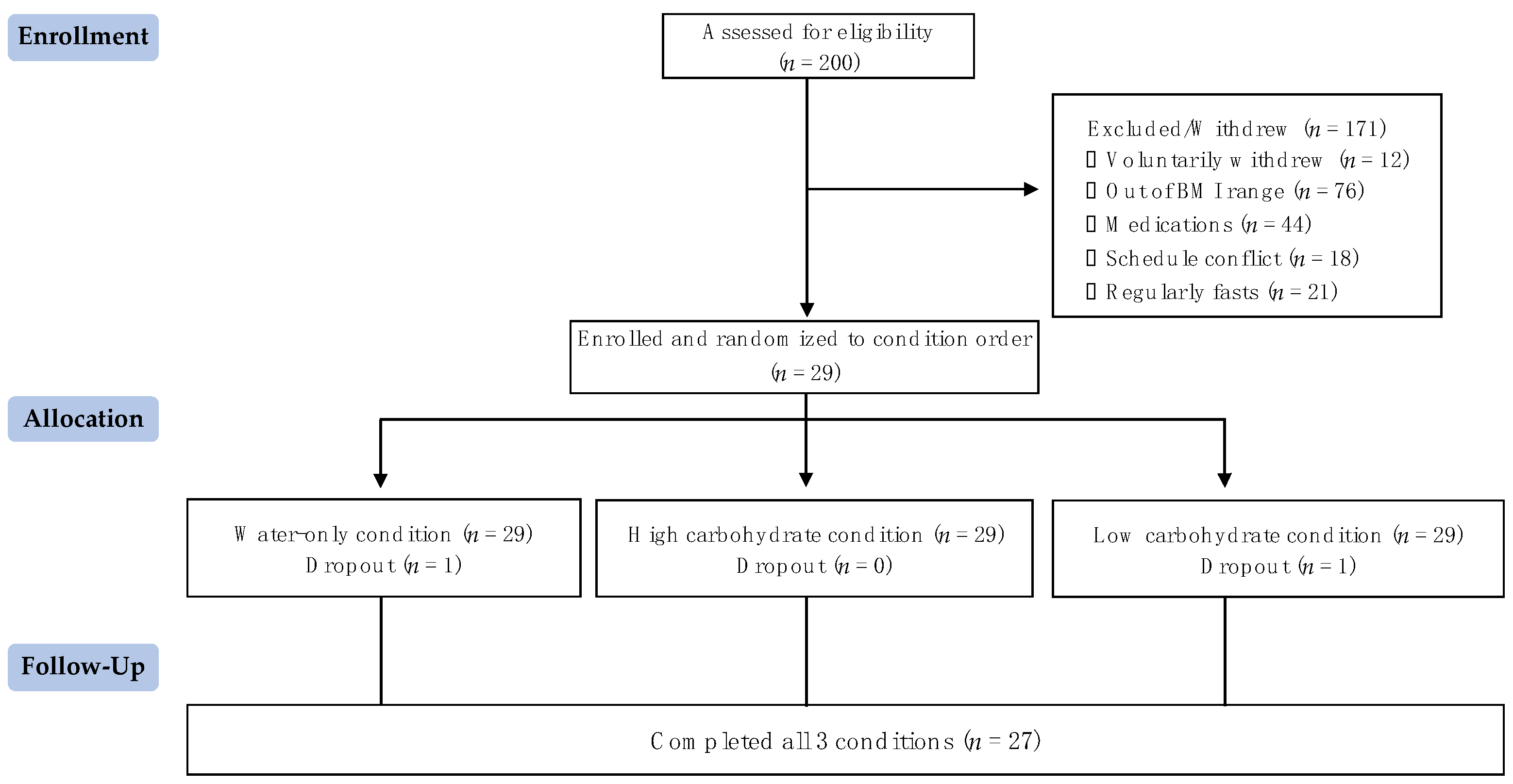
2.1. Participants
- Diagnosed with a chronic disease (i.e., cancer, heart/liver/kidney disease).
- Diagnosed with a metabolic disease (i.e., Type I and Type II diabetes).
- Diagnosed with an eating disorder (i.e., anorexia, bulimia or binge eating disorder).
- Taking medications that alter metabolism, appetite, or neurological function (i.e., insulin, metformin, amphetamine-based ADHD medications, depression, and anxiety medications such as selective serotonin reuptake inhibitors, serotonin and norepinephrine inhibitors, and benzodiazepines) [29].
- Food allergies (i.e.,—nuts, celiac disease, or gluten intolerance, or lactose intolerance).
- Habitually consumption of 60 mg or more of caffeine daily [30].
- Pregnant or lactating.
- Post-menopausal [31].
- Currently participating in ketogenic, carbohydrate, or calorie-restricted diets.
- Regularly exercised more than 225 min per week.
- Fasting more than once per week.
- Irregular sleeping patterns (including graveyard or swing shifts).
2.2. Measurements
2.2.1. Venipuncture
2.2.2. Capillary Ketone Assessment
2.2.3. Continuous Glucose Monitoring
2.3. Procedures
2.3.1. Orientation
2.3.2. Standardized Meals
2.3.3. Standardized Shakes
2.3.4. Treatment Sessions
2.4. Statistical Analysis
3. Results
3.1. Beta-Hydroxybutyrate
3.2. Glucose
3.3. Hormones
3.4. Perceived Difficulty of the Fast
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm (accessed on 30 June 2023).
- Raghupathi, W.; Raghupathi, V. An Empirical Study of Chronic Diseases in the United States: A Visual Analytics Approach to Public Health. Int. J. Envrion. Res. Public Health 2018, 15, 431. [Google Scholar] [CrossRef] [PubMed]
- Rappaport, S.M. Genetic Factors Are Not the Major Causes of Chronic Diseases. PLoS ONE 2016, 11, e0154387. [Google Scholar] [CrossRef] [PubMed]
- Cunliffe, V.T. Experience-sensitive epigenetic mechanisms, developmental plasticity, and the biological embedding of chronic disease risk. Wires Syst. Biol. Med. 2015, 7, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.R.; Kim, S.R.; Cho, W.; Lee, S.G.; Kim, S.H.; Kim, J.H.; Choi, E.; Kim, J.H.; Yu, J.W.; Lee, B.W.; et al. Short Term Isocaloric Ketogenic Diet Modulates NLRP3 Inflammasome Via B-hydroxybutyrate and Fibroblast Growth Factor 21. Front. Immunol. 2022, 13, 843520. [Google Scholar] [CrossRef] [PubMed]
- Castela, I.; Rodrigues, C.; Ismael, S.; Barreiros-Mota, I.; Morais, J.; Araujo, J.R.; Marques, C.; Silvestre, M.P.; Angelo-Dias, M.; Martins, C.; et al. Intermittent energy restriction ameliorates adipose tissue-associated inflammation in adults with obesity: A randomised controlled trial. Clin. Nutr. 2022, 41, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Song, M.; Eliassen, A.H.; Wang, M.; Fung, T.T.; Clinton, S.K.; Rimm, E.B.; Hu, F.B.; Willett, W.C.; Tabung, F.K.; et al. Optimal dietary patterns for prevention of chronic disease. Nat. Med. 2023, 29, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Michailidis, M.; Moraitou, D.; Tata, D.A.; Kalinderi, K.; Papamitsou, T.; Papaliagkas, V. Alzheimer’s Disease as Type 3 Diabetes: Common Pathophysiological Mechanisms between Alzheimer’s Disease and Type 2 Diabetes. Int. J. Mol. Sci. 2022, 23, 2687. [Google Scholar] [CrossRef]
- Pasanisi, P.; Bruno, E.; Manoukian, S.; Berrino, F. A randomized controlled trial of diet and physical activity in BRCA mutation carriers. Fam. Cancer 2014, 13, 181–187. [Google Scholar] [CrossRef]
- Anton, S.D.; Moehl, K.; Donahoo, W.T.; Marosi, K.; Lee, S.A.; Mainous, A.G., 3rd; Leeuwenburgh, C.; Mattson, M.P. Flipping the Metabolic Switch: Understanding and Applying the Health Benefits of Fasting. Obesity 2018, 26, 254–268. [Google Scholar] [CrossRef]
- Mattson, M.P.; Moehl, K.; Ghena, N.; Schmaedick, M.; Cheng, A. Intermittent metabolic switching, neuroplasticity and brain health. Nat. Rev. Neurosci. 2018, 19, 63–80. [Google Scholar] [CrossRef]
- Rein, M.; Ben-Yacov, O.; Godneva, A.; Shilo, S.; Zmora, N.; Kolobkov, D.; Cohen-Dolev, N.; Wolf, B.C.; Kosower, N.; Lotan-Pompan, M.; et al. Effects of personalized diets by prediction of glycemic responses on glycemic control and metabolic health in newly diagnosed T2DM: A randomized dietary intervention pilot trial. BMC Med. 2022, 20, 56. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A. Postprandial hyperglycemia and diabetes complications—Is it time to treat? Diabetes 2005, 54, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Ghani, M.A.; Jenkinson, C.P.; Richardson, D.K.; Tripathy, D.; DeFronzo, R.A. Insulin secretion and action in subjects with impaired fasting glucose and impaired glucose tolerance—Results from the veterans administration genetic epidemiology study. Diabetes 2006, 55, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Khanal, M.K.; Bhandari, P.; Dhungana, R.R.; Gurung, Y.; Rawal, L.B.; Pandey, G.; Bhandari, M.; Devkota, S.; Courten, M.; Courten, B. Poor glycemic control, cardiovascular disease risk factors and their clustering among patients with type 2 diabetes mellitus: A cross-sectional study from Nepal. PLoS ONE 2022, 17, e0271888. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, S.F.; Terada, T.; Chahal, B.S.; Boule, N.G. Exercise lowers postprandial glucose but not fasting glucose in type 2 diabetes: A meta-analysis of studies using continuous glucose monitoring. Diabetes Metab. Res. Rev. 2013, 29, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Fanti, M.; Mishra, A.; Longo, V.D.; Brandhorst, S. Time-Restricted Eating, Intermittent Fasting, and Fasting-Mimicking Diets in Weight Loss. Curr. Obes. Rep. 2021, 10, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Brandhorst, S.; Shelehchi, M.; Mirzaei, H.; Cheng, C.W.; Budniak, J.; Groshen, S.; Mack, W.J.; Guen, E.; Di Biase, S.; et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and cardiovascular disease. Sci. Transl. Med. 2017, 9, eaai8700. [Google Scholar] [CrossRef] [PubMed]
- Brandhorst, S.; Choi, I.Y.; Wei, M.; Cheng, C.W.; Sedrakyan, S.; Navarrete, G.; Dubeau, L.; Yap, L.P.; Park, R.; Vinciguerra, M.; et al. A Periodic Diet that Mimics Fasting Promotes Multi-System Regeneration, Enhanced Cognitive Performance, and Healthspan. Cell Metab. 2015, 22, 86–99. [Google Scholar] [CrossRef]
- Longo, V.D.; Panda, S. Fasting, Circadian Rhythms, and Time-Restricted Feeding in Healthy Lifespan. Cell Metab. 2016, 23, 1048–1059. [Google Scholar] [CrossRef]
- Patterson, R.E.; Sears, D.D. Metabolic Effects of Intermittent Fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef]
- Cheng, C.W.; Villani, V.; Buono, R.; Wei, M.; Kumar, S.; Yilmaz, O.H.; Cohen, P.; Sneddon, J.B.; Perin, L.; Longo, V.D. Fasting-Mimicking Diet Promotes Ngn3-Driven beta-Cell Regeneration to Reverse Diabetes. Cell 2017, 168, 775–788.e12. [Google Scholar] [CrossRef] [PubMed]
- Duregon, E.; Pomatto-Watson, L.C.D.D.; Bernier, M.; Price, N.L.; de Cabo, R. Intermittent fasting: From calories to time restriction. Geroscience 2021, 43, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Balasse, E.O.; Fery, F.; Neef, M.A. Changes induced by exercise in rates of turnover and oxidation of ketone bodies in fasting man. J. Appl. Physiol. Respir. Envrion. Exerc. Physiol. 1978, 44, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Cahill, G.F., Jr. Fuel metabolism in starvation. Annu. Rev. Nutr. 2006, 26, 1–22. [Google Scholar] [CrossRef]
- Browning, J.D.; Baxter, J.; Satapati, S.; Burgess, S.C. The effect of short-term fasting on liver and skeletal muscle lipid, glucose, and energy metabolism in healthy women and men. J. Lipid. Res. 2012, 53, 577–586. [Google Scholar] [CrossRef]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8–11. [Google Scholar] [CrossRef]
- Okura, T.; Nakamura, R.; Fujioka, Y.; Kawamoto-Kitao, S.; Ito, Y.; Matsumoto, K.; Shoji, K.; Sumi, K.; Matsuzawa, K.; Izawa, S.; et al. Body mass index >= 23 is a risk factor for insulin resistance and diabetes in Japanese people: A brief report. PLoS ONE 2018, 13, e0201052. [Google Scholar] [CrossRef]
- Verhaegen, A.A.; Van Gaal, L.F. Drug-induced obesity and its metabolic consequences: A review with a focus on mechanisms and possible therapeutic options. J. Endocrinol. Investig. 2017, 40, 1165–1174. [Google Scholar] [CrossRef]
- Johnston, K.L.; Clifford, M.N.; Morgan, L.M. Coffee acutely modifies gastrointestinal hormone secretion and glucose tolerance in humans: Glycemic effects of chlorogenic acid and caffeine. Am. J. Clin. Nutr. 2003, 78, 728–733. [Google Scholar] [CrossRef]
- Morrow, P.G.; Marshall, W.P.; Kim, H.J.; Kalkhoff, R.K. Metabolic response to starvation. II. Effects of sex steroid administration to pre- and postmenopausal women. Metabolism 1981, 30, 274–278. [Google Scholar] [CrossRef]
- Speakman, J.; Booles, D.; Butterwick, R. Validation of dual energy X-ray absorptiometry (DXA) by comparison with chemical analysis of dogs and cats. Int. J. Obes. 2001, 25, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Tataranni, P.A.; Pettitt, D.J.; Ravussin, E. Dual energy X-ray absorptiometry: Inter-machine variability. Int. J. Obes. 1996, 20, 1048–1050. [Google Scholar]
- Bailey, B.W.; LeCheminant, G.; Hope, T.; Bell, M.; Tucker, L.A. A comparison of the agreement, internal consistency, and 2-day test stability of the InBody 720, GE iDXA, and BOD POD® gold standard for assessing body composition. Meas. Phys. Educ. Exerc. Sci. 2018, 22, 231–238. [Google Scholar] [CrossRef]
- Rothney, M.P.; Xia, Y.; Wacker, W.K.; Martin, F.P.; Beaumont, M.; Rezzi, S.; Giusti, V.; Ergun, D.L. Precision of a new tool to measure visceral adipose tissue (VAT) using dual-energy X-ray absorptiometry (DXA). Obesity 2013, 21, E134–E136. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.; De Lucia Rolfe, E.; Sleigh, A.; Kivisild, T.; Behbehani, K.; Wareham, N.J.; Brage, S.; Mohammad, T. Validity of visceral adiposity estimates from DXA against MRI in Kuwaiti men and women. Nutr. Diabetes 2017, 7, e238. [Google Scholar] [CrossRef] [PubMed]
- Byrne, H.A.; Tieszen, K.L.; Hollis, S.; Dornan, T.L.; New, J.P. Evaluation of an Electrochemical Sensor for Measuring Blood Ketones. Diabetes Care 2000, 23, 500–503. [Google Scholar] [CrossRef]
- Steineck, I.I.K.; Mahmoudi, Z.; Ranjan, A.; Schmidt, S.; Jorgensen, J.B.; Norgaard, K. Comparison of Continuous Glucose Monitoring Accuracy Between Abdominal and Upper Arm Insertion Sites. Diabetes Technol. 2019, 21, 295–302. [Google Scholar] [CrossRef]
- Basu, A.; Dube, S.; Veettil, S.; Slama, M.; Kudva, Y.C.; Peyser, T.; Carter, R.E.; Cobelli, C.; Basu, R. Time lag of glucose from intravascular to interstitial compartment in type 1 diabetes. J. Diabetes Sci. Technol. 2015, 9, 63–68. [Google Scholar] [CrossRef]
- Abbott Diabetes Care Inc. Freestyle Libre Pro Flash Glucose Monitoring System User Manual; Abbott Diabetes Care Inc.: Alameda, CA, USA, 2016; pp. 44–45. [Google Scholar]
- Merino, J.; Linenberg, I.; Bermingham, K.M.; Ganesh, S.; Bakker, E.; Delahanty, L.M.; Chan, A.T.; Pujol, J.C.; Wolf, J.; Al Khatib, H.; et al. Validity of continuous glucose monitoring for categorizing glycemic responses to diet: Implications for use in personalized nutrition. Am. J. Clin. Nutr. 2022, 115, 1569–1576. [Google Scholar] [CrossRef]
- Bailey, T.; Bode, B.W.; Christiansen, M.P.; Klaff, L.J.; Alva, S. The Performance and Usability of a Factory-Calibrated Flash Glucose Monitoring System. Diabetes Technol. Ther. 2015, 17, 787–794. [Google Scholar] [CrossRef]
- Deru, L.S.; Bikman, B.T.; Davidson, L.E.; Tucker, L.A.; Fellingham, G.; Bartholomew, C.L.; Yuan, H.L.; Bailey, B.W. The Effects of Exercise on beta-Hydroxybutyrate Concentrations over a 36-h Fast: A Randomized Crossover Study. Med. Sci. Sports Exerc. 2021, 53, 1987–1998. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. Body Weight Planner. Available online: https://www.niddk.nih.gov/bwp (accessed on 12 October 2022).
- Hall, K.D.; Sacks, G.; Chandramohan, D.; Chow, C.C.; Wang, Y.C.; Gortmaker, S.L.; Swinburn, B.A. Quantification of the effect of energy imbalance on bodyweight. Lancet 2011, 378, 826–837. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Estimates of energy and protein requirements of adults and children. In Energy and Protein Requirements; World Health Organization: Geneva, Switzerland, 1985; pp. 71–112. [Google Scholar]
- Capozzi, M.E.; Coch, R.W.; Koech, J.; Astapova, I.I.; Wait, J.B.; Encisco, S.E.; Douros, J.D.; El, K.; Finan, B.; Sloop, K.W.; et al. The Limited Role of Glucagon for Ketogenesis During Fasting or in Response to SGLT2 Inhibition. Diabetes 2020, 69, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D.; Westman, E.; Mattes, R.D.; Wolfe, R.R.; Astrup, A.; Westerterp-Plantenga, M. Protein, weight management, and satiety. Am. J. Clin. Nutr. 2008, 87, 1558S–1561S. [Google Scholar] [CrossRef] [PubMed]
- Rietman, A.; Schwarz, J.; Tome, D.; Kok, F.J.; Mensink, M. High dietary protein intake, reducing or eliciting insulin resistance? Eur. J. Clin. Nutr. 2014, 68, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B.; Benson, A. Determination of glycaemic fluctuations with continuous glucose monitoring. What is a meaningful difference? J. Sci. Med. Sport 2015, 19, e102. [Google Scholar] [CrossRef]
- Newman, J.C.; Verdin, E. Ketone bodies as signaling metabolites. Trends Endocrin. Met. 2014, 25, 42–52. [Google Scholar] [CrossRef]
- Takao, T.; Ide, T.; Yanagisawa, H.; Kikuchi, M.; Kawazu, S.; Matsuyama, Y. The effect of fasting plasma glucose variability on the risk of retinopathy in type 2 diabetic patients: Retrospective long-term follow-up. Diabetes Res. Clin. Pract. 2010, 89, 296–302. [Google Scholar] [CrossRef]
- Liang, S.; Yin, H.; Wei, C.; Xie, L.; He, H.; Liu, X. Glucose variability for cardiovascular risk factors in type 2 diabetes: A meta-analysis. J. Diabetes Metab. Disord. 2017, 16, 45. [Google Scholar] [CrossRef]
- Klimontov, V.V.; Semenova, J.F. Glucose variability in subjects with normal glucose tolerance: Relations with body composition, insulin secretion and sensitivity. Diabetes Metab. Synd. 2022, 16, 102387. [Google Scholar] [CrossRef]
- Zhao, Q.; Zhou, F.; Zhang, Y.S.; Zhou, X.Y.; Ying, C.J. Fasting plasma glucose variability levels and risk of adverse outcomes among patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2019, 148, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Haak, T.; Hanaire, H.; Ajjan, R.; Hermanns, N.; Riveline, J.P.; Rayman, G. Flash Glucose-Sensing Technology as a Replacement for Blood Glucose Monitoring for the Management of Insulin-Treated Type 2 Diabetes: A Multicenter, Open-Label Randomized Controlled Trial. Diabetes Ther. 2017, 8, 55–73. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.W.; Wei, M.; Caputo, S.; Wilson, M.L.; Antoun, J.; Hsu, W.C. An Intermittent Fasting Mimicking Nutrition Bar Extends Physiologic Ketosis in Time Restricted Eating: A Randomized, Controlled, Parallel-Arm Study. Nutrients 2021, 13, 1523. [Google Scholar] [CrossRef] [PubMed]
- Carroll, K.F.; Nestel, P.J. Diurnal-Variation in Glucose-Tolerance and in Insulin-Secretion in Man. Diabetes 1973, 22, 333–348. [Google Scholar] [CrossRef] [PubMed]
- Deru, L.S.; Chamberlain, C.J.; Lance, G.R.; Gipson, E.Z.; Bikman, B.T.; Davidson, L.E.; Tucker, L.A.; Coleman, J.L.; Bailey, B.W. The Effects of Exercise on Appetite-Regulating Hormone Concentrations over a 36-h Fast in Healthy Young Adults: A Randomized Crossover Study. Nutrients 2023, 15, 1911. [Google Scholar] [CrossRef] [PubMed]
- Betts, G.J.; Desaix, P. Anatomy and Physiology; OpenStax: Houston, TX, USA, 2017. [Google Scholar]
- Brubaker, P.L.; Drucker, D.J. Structure-function of the glucagon receptor family of G protein-coupled receptors: The glucagon, GIP, GLP-1, and GLP-2 receptors. Recept. Channels 2002, 8, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Fisher-Wellman, K.; Bloomer, R.J. Macronutrient specific postprandial oxidative stress: Relevance to the development of insulin resistance. Curr. Diabetes Rev. 2009, 5, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Schirra, J.; Nicolaus, M.; Woerle, H.J.; Struckmeier, C.; Katschinski, M.; Goke, B. GLP-1 regulates gastroduodenal motility involving cholinergic pathways. Neurogastroenterol. Motil. 2009, 21, 609–618, e21–e22. [Google Scholar] [CrossRef]
- Jin, T.; Weng, J. Hepatic functions of GLP-1 and its based drugs: Current disputes and perspectives. Am. J. Physiol. Endocrinol. Metab. 2016, 311, E620–E627. [Google Scholar] [CrossRef]
- Schirra, J.; Nicolaus, M.; Roggel, R.; Katschinski, M.; Storr, M.; Woerle, H.J.; Goke, B. Endogenous glucagon-like peptide 1 controls endocrine pancreatic secretion and antro-pyloro-duodenal motility in humans. Gut 2006, 55, 243–251. [Google Scholar] [CrossRef]
- Reinehr, T.; de Sousa, G.; Roth, C.L. Fasting glucagon-like peptide-1 and its relation to insulin in obese children before and after weight loss. J. Pediatr. Gastr. Nutr. 2007, 44, 608–612. [Google Scholar] [CrossRef] [PubMed]
- Rizi, E.P.; Loh, T.P.; Baig, S.; Chhay, V.; Huang, S.Q.; Quek, J.C.; Tai, E.S.; Toh, S.A.; Khoo, C.M. A high carbohydrate, but not fat or protein meal attenuates postprandial ghrelin, PYY and GLP-1 responses in Chinese men. PLoS ONE 2018, 13, e0191609. [Google Scholar] [CrossRef]
- Gibbons, C.; Caudwell, P.; Finlayson, G.; Webb, D.L.; Hellstrom, P.M.; Naslund, E.; Blundell, J.E. Comparison of postprandial profiles of ghrelin, active GLP-1, and total PYY to meals varying in fat and carbohydrate and their association with hunger and the phases of satiety. J. Clin. Endocrinol. Metab. 2013, 98, E847–E855. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.B. Glucose-dependent insulinotropic polypeptide: Effects on insulin and glucagon secretion in humans. Dan. Med. J. 2016, 63, 3103–3109. [Google Scholar]
- Meier, J.J.; Nauck, M.A. Glucagon-like peptide 1(GLP-1) in biology and pathology. Diabetes Metab. Res. Rev. 2005, 21, 91–117. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Burhol, P.G.; Schulz, T.B. Fasting and postprandial plasma GIP values in man measured with seven different antisera. Regul. Pept. 1983, 7, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Yoder, S.M.; Yang, Q.; Kindel, T.L.; Tso, P. Differential responses of the incretin hormones GIP and GLP-1 to increasing doses of dietary carbohydrate but not dietary protein in lean rats. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 299, G476–G485. [Google Scholar] [CrossRef] [PubMed]
- Paschetta, E.; Hvalryg, M.; Musso, G. Glucose-dependent insulinotropic polypeptide: From pathophysiology to therapeutic opportunities in obesity-associated disorders. Obes. Rev. 2011, 12, 813–828. [Google Scholar] [CrossRef]
- Kwasowski, P.; Flatt, P.R.; Bailey, C.J.; Marks, V. Effects of fatty acid chain length and saturation on gastric inhibitory polypeptide release in obese hyperglycaemic (ob/ob) mice. Biosci. Rep. 1985, 5, 701–705. [Google Scholar] [CrossRef]
- Thomsen, C.; Rasmussen, O.; Lousen, T.; Holst, J.J.; Fenselau, S.; Schrezenmeir, J.; Hermansen, K. Differential effects of saturated and monounsaturated fatty acids on postprandial lipemia and incretin responses in healthy subjects. Am. J. Clin. Nutr. 1999, 69, 1135–1143. [Google Scholar] [CrossRef]
- Johnson, R.E.; Passmore, R. Interrelations among Post-Exercise Ketosis (Courtice-Douglas Effect), Hydration and Metabolic State. Metab. Clin. Exp. 1959, 9, 443–451. [Google Scholar]
- Kanda, A.; Nakayama, K.; Sanbongi, C.; Nagata, M.; Ikegami, S.; Itoh, H. Effects of Whey, Caseinate, or Milk Protein Ingestion on Muscle Protein Synthesis after Exercise. Nutrients 2016, 8, 339. [Google Scholar] [CrossRef] [PubMed]
- Caputo, M.; Pigni, S.; Agosti, E.; Daffara, T.; Ferrero, A.; Filigheddu, N.; Prodam, F. Regulation of GH and GH Signaling by Nutrients. Cells 2021, 10, 1376. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, J.H.; Bell, D.S. Postprandial hyperglycemia/hyperlipidemia (postprandial dysmetabolism) is a cardiovascular risk factor. Am. J. Cardiol. 2007, 100, 899–904. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male (n = 17) | Female (n = 12) | Cumulative (n = 29) | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Age (years) | 36.2 | 15.9 | 35.8 | 8.9 | 36.0 | 13.3 |
| BMI (kg/m2) | 31.8 | 4.6 | 30.5 | 4.5 | 31.2 | 4.5 |
| Percent body fat | 30.5 | 8.14 | 41.5 | 5.2 | 35.4 | 8.8 |
| Visceral Adipose (g) | 1238.8 | 916.1 | 953.6 | 502 | 1120.8 | 773.9 |
| Ethnicity | n | % | n | % | n | % |
| African | 2 | 11.8 | 1 | 8.3 | 3 | 10.3 |
| Caucasian | 13 | 76.4 | 8 | 66.7 | 21 | 72.4 |
| Hispanic/Latino | 2 | 11.8 | 3 | 25 | 5 | 17.3 |
| 0 h * | 24 h * | 25 h † | 28 h † | 38 h ‡ | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Condition | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| HC/LF | 0.13 a | 0.05 | 0.59 b | 0.28 | 0.28 c | 0.19 | 0.19 a,c | 0.16 | 0.44 d | 0.28 |
| LC/HF | 0.14 a | 0.07 | 0.53 b | 0.29 | 0.44 b,c | 0.16 | 0.38 c | 0.16 | 0.51 b | 0.27 |
| Water | 0.18 a | 0.20 | 0.56 b | 0.28 | 0.63 b,c | 0.31 | 0.70 c | 0.42 | 0.85 d | 0.051 |
| Analyte | Condition | 0 h | 24 h | 25 h * | 38 h | F-Value | p-Value |
| Insulin | Water | 3414.4 ± 2635.7 a | 2969.7 ± 2730.5 a | 2955.4 ± 2578.5 a | 2932.9± 2610.7 a | 18.6 | <0.0001 |
| LC/HF | 3614.4 ± 2618.7 a | 3129.8 ± 2650.2 b | 3612.8 ± 3612.8 a | 3172.6 ± 2749.1 b | |||
| HC/LF | 3803.1 ± 3297.8 a | 3112.7 ± 2744.0 a | 8706.7 ± 5615.2 b | 3011.8 ± 2631.1 a | |||
| Analyte | Condition | 0 h ‡ | 24 h | 25 h * | 38 h | F-Value | p-Value |
| GIP | Water | 660.7 ± 420.2 a | 60.2 ± 32.7 b | 64.1 ± 33.3 b | 66.8 ± 35.8 b | 22.1 | <0.0001 |
| LC/HF | 743.4 ± 317.2 a | 67.8 ± 68.9 b | 585.1 ± 178.9 c | 84.6 ± 56.0 bd | |||
| HC/LF | 575.1 ± 314.2 a | 73.2 ± 34.7 b | 704.9 ± 222.9 c | 88.0 ± 51.4 d | |||
| Analyte | Condition | 0 h | 24 h | 25 h ƒ | 38 h | F-Value | p-Value |
| GLP-1 | Water | 442.9 ± 170.1 a | 353.3 ± 161.7 b | 367.7 ± 159.5 bc | 420.4 ± 179.7 c | 4.1 | 0.0006 |
| LC/HF | 442.3 ± 144.8 a | 373.4 ± 153.8 b | 468.3 ± 187.6 ac | 369.6 ± 132.3 cd | |||
| HC/LF | 385.4 ± 122.5 a | 362.2 ± 144.4 b | 411.2 ± 184.7 b | 347.0 ± 126.6 b | |||
| Analyte | Condition | 0 h | 24 h | 25 h † | 38 h | F-Value | p-Value |
| Glucagon | Water | 167.1 ± 66.3 a | 101.3 ± 53.4 b | 105.2 ± 53.3 b | 135.9 ± 64.9 c | 3.4 | 0.0029 |
| LC/HF | 165.8 ± 58.9 a | 122.9 ± 63.5 b | 128.8 ± 68.3 b | 128.9 ± 62.6 b | |||
| HC/LF | 149.6 ± 61.5 a | 112.2 ± 50.8 b | 73.89 ± 60.1 c | 106.37 ± 54.7 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deru, L.S.; Gipson, E.Z.; Hales, K.E.; Bikman, B.T.; Davidson, L.E.; Horne, B.D.; LeCheminant, J.D.; Tucker, L.A.; Bailey, B.W. The Effects of a High-Carbohydrate versus a High-Fat Shake on Biomarkers of Metabolism and Glycemic Control When Used to Interrupt a 38-h Fast: A Randomized Crossover Study. Nutrients 2024, 16, 164. https://doi.org/10.3390/nu16010164
Deru LS, Gipson EZ, Hales KE, Bikman BT, Davidson LE, Horne BD, LeCheminant JD, Tucker LA, Bailey BW. The Effects of a High-Carbohydrate versus a High-Fat Shake on Biomarkers of Metabolism and Glycemic Control When Used to Interrupt a 38-h Fast: A Randomized Crossover Study. Nutrients. 2024; 16(1):164. https://doi.org/10.3390/nu16010164
Chicago/Turabian StyleDeru, Landon S., Elizabeth Z. Gipson, Katelynn E. Hales, Benjamin T. Bikman, Lance E. Davidson, Benjamin D. Horne, James D. LeCheminant, Larry A. Tucker, and Bruce W. Bailey. 2024. "The Effects of a High-Carbohydrate versus a High-Fat Shake on Biomarkers of Metabolism and Glycemic Control When Used to Interrupt a 38-h Fast: A Randomized Crossover Study" Nutrients 16, no. 1: 164. https://doi.org/10.3390/nu16010164
APA StyleDeru, L. S., Gipson, E. Z., Hales, K. E., Bikman, B. T., Davidson, L. E., Horne, B. D., LeCheminant, J. D., Tucker, L. A., & Bailey, B. W. (2024). The Effects of a High-Carbohydrate versus a High-Fat Shake on Biomarkers of Metabolism and Glycemic Control When Used to Interrupt a 38-h Fast: A Randomized Crossover Study. Nutrients, 16(1), 164. https://doi.org/10.3390/nu16010164