Prolonged Fasting Induces Histological and Ultrastructural Changes in the Intestinal Mucosa That May Reduce Absorption and Revert after Enteral Refeeding

 , ,
, , 
Abstract
:1. Introduction
- Analyze the histological and ultrastructural changes in the intestinal mucosa of malnourished patients referred and submitted to endoscopic gastrostomy after a significant fasting period.
- Assess if these changes are reverted after refeeding through enteral nutrition by PEG.
2. Material and Methods
2.1. Study Design
2.2. Patients
- Nutritional anamnesis performed by a trained dietitian through a dietary recall.
- Estimation of energy needs according to age, gender, height, weight, and clinical setting to assess the reduction in food ingestion in the last month before PEG.
- Prospective clinical and demographic database registry that includes age, gender, clinical indication for PEG, anthropometry, laboratory parameters, and survival.
- PEG was performed by two gastroenterologists using the “pull” method described by Gauderer-Ponsky, with the patients under deep sedation. Antithrombotic therapy was managed according to international guidelines [21].
- The collection of 4–6 duodenal biopsies (second portion) at the time of the gastrostomy procedure (T0) and after 3–6 months of PEG feeding at endoscopic tube replacement (T1).
2.3. Anthropometric Evaluation
2.4. Laboratory Evaluation
2.5. Duodenal Biopsy Analysis
2.6. Statistical Analysis
3. Results
3.1. Patients
3.2. Nutritional Assessment: NRS 2002, Anthropometry, and Laboratory Data
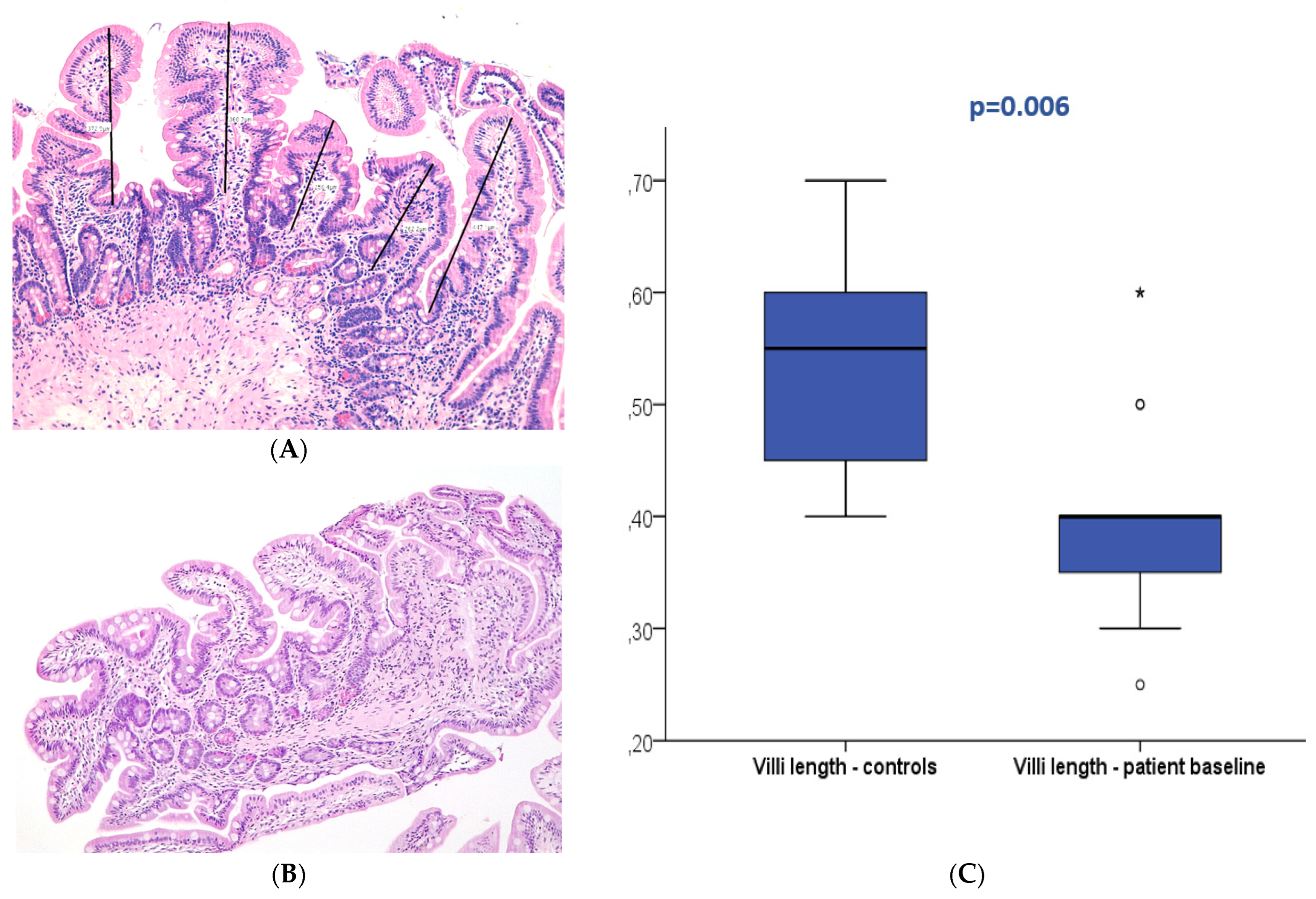
3.3. Duodenal Mucosa Histology
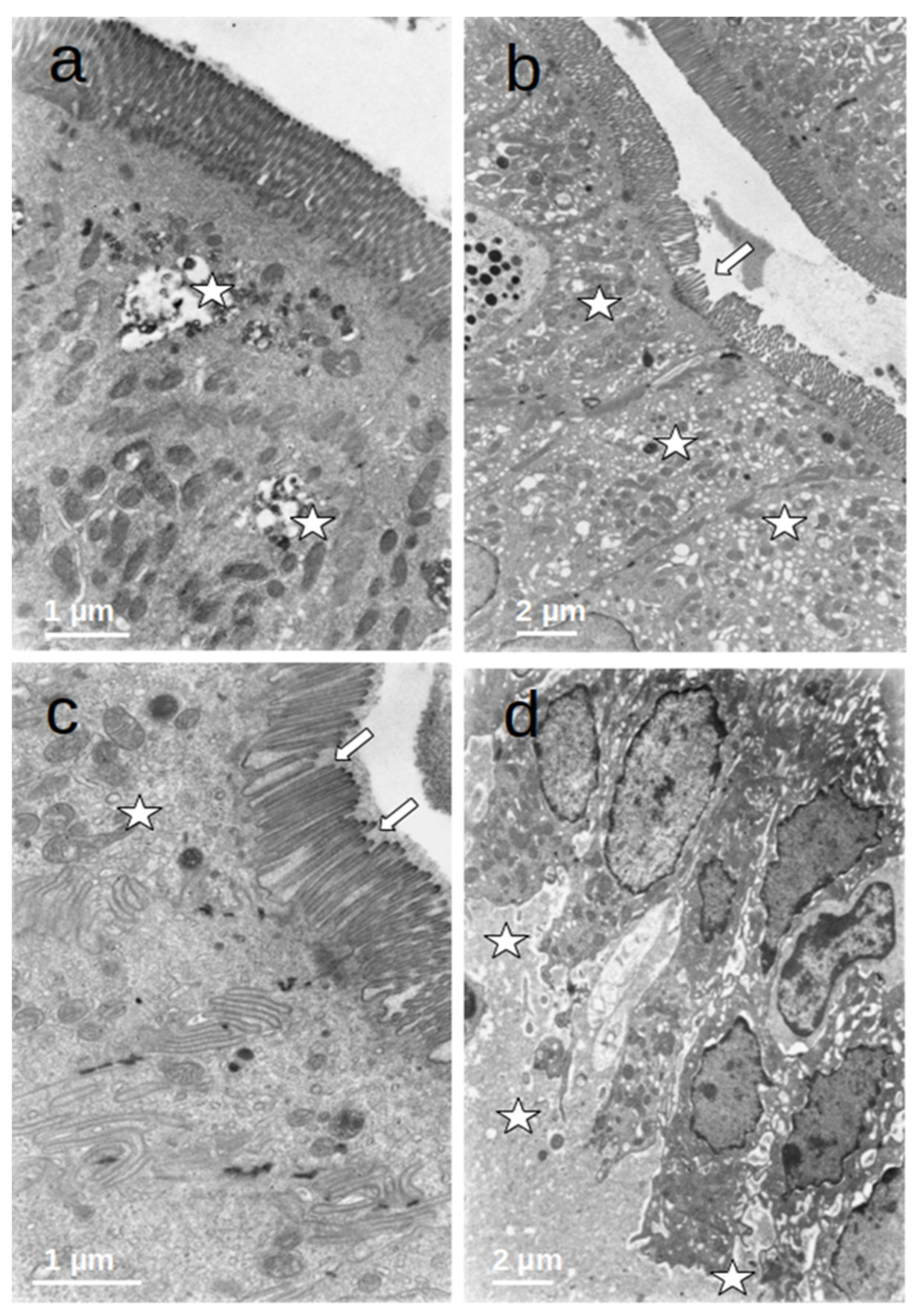
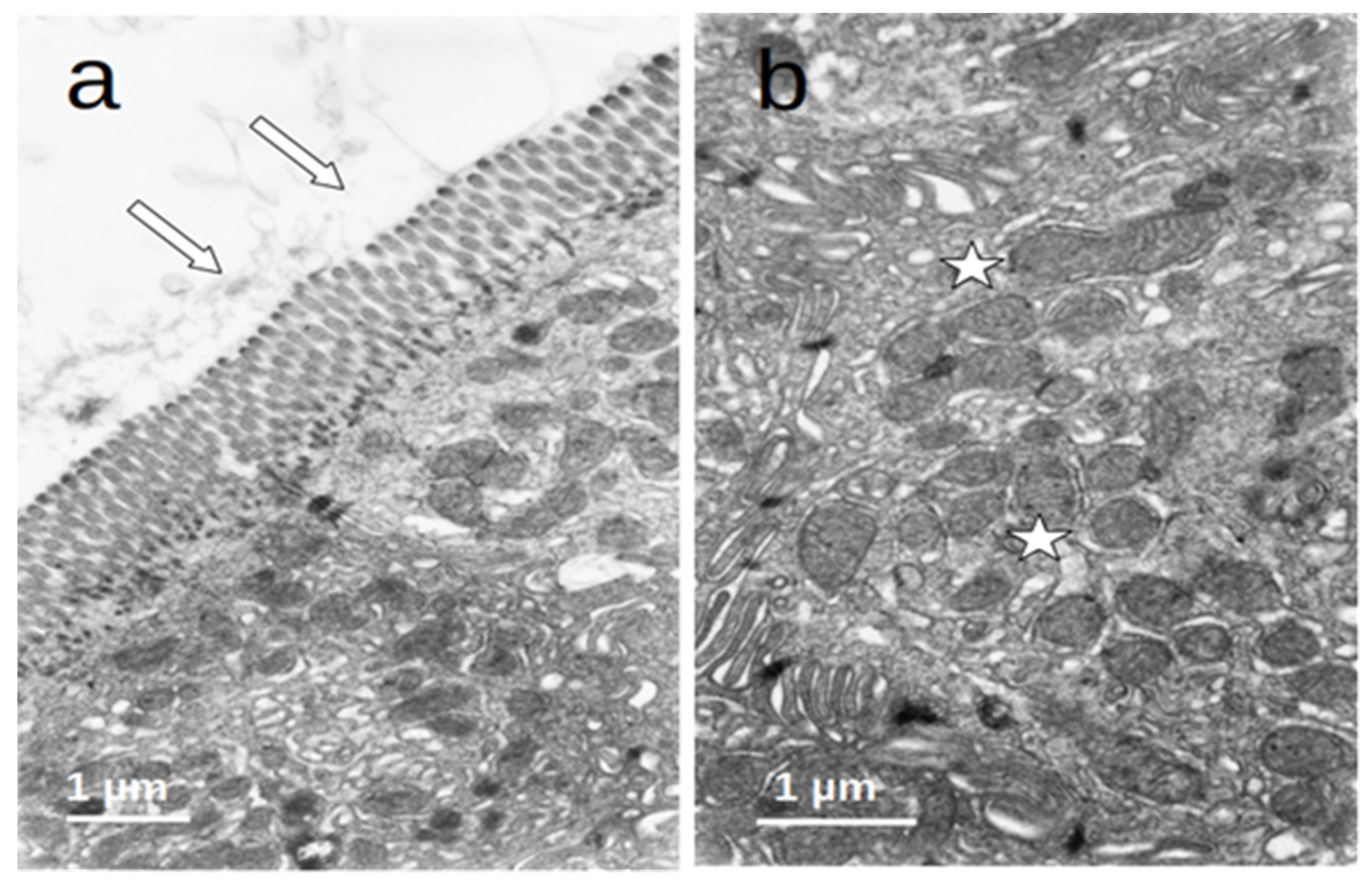
3.4. Duodenal Mucosa Ultrastructure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Isabelle Cremers, M. The European Section and Board of Gastroenterology and Hepatology: What’s new? GE Port. J. Gastroenterol. 2017, 24, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Nunes, G.; Brito, M.; Santos, C.A.; Fonseca, J. Refeeding syndrome in the gastroenterology practice how concerned should we be? Eur. J. Gastroenterol. Hepatol. 2018, 30, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Crook, M.A. Refeeding syndrome problems with definition and management. Nutrition 2014, 30, 1448–1455. [Google Scholar] [CrossRef] [PubMed]
- da Silva, J.S.V.; Seres, D.S.; Sabino, K.; Adams, S.C.; Berdahl, G.J.; Citty, S.W.; Cober, M.P.; Evans, D.C.; Greaves, J.R.; Gura, K.M.; et al. Parenteral Nutrition Safety and Clinical Practice Committees, American Society for Parenteral and Enteral Nutrition. ASPEN Consensus Recommendations for Refeeding Syndrome. Nutr. Clin. Pract. 2020, 35, 178–195. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Clinical Excellence. Nutrition Support in Adults: Oral Nutrition Support, Enteral Tube Feeding and Parenteral Nutrition; Clinical Guideline CG32; National Institute for Health and Clinical Excellence: London, UK, 2006; Available online: www.nice.org.uk/page.aspx?o=cg032 (accessed on 30 November 2023).
- Cioffi, I.; Ponzo, V.; Pellegrini, M.; Evangelista, A.; Bioletto, F.; Ciccone, G.; Pasanisi, F.; Ghigo, E.; Bo, S. The incidence of the refeeding syndrome. A systematic review and meta-analyses of literature. Clin. Nutr. 2021, 40, 3688–3701. [Google Scholar] [CrossRef] [PubMed]
- Friedli, N.; Stanga, Z.; Sobotka, L.; Culkin, A.; Kondrup, J.; Laviano, A.; Mueller, B.; Schuetz, P. Revisiting the refeeding syndrome: Results of a systematic review. Nutrition 2017, 35, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.J.Y.; Pang, J.G.T.; Li, Y.Y.; Lew, C.C.H. Refeeding Hypophosphatemia in Patients Receiving Parenteral Nutrition: Prevalence, Risk Factors, and Predicting Its Occurrence. Nutr. Clin. Pract. 2021, 36, 679–688. [Google Scholar] [CrossRef]
- Arvanitakis, M.; Gkolfakis, P.; Despott, E.J.; Ballarin, A.; Beyna, T.; Boeykens, K.; Elbe, P.; Gisbertz, I.; Hoyois, A.; Mosteanu, O.; et al. Endoscopic management of enteral tubes in adult patients—Part 1: Definitions and indications. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021, 53, 81–92. [Google Scholar] [CrossRef]
- Gkolfakis, P.; Arvanitakis, M.; Despott, E.J.; Ballarin, A.; Beyna, T.; Boeykens, K.; Elbe, P.; Gisbertz, I.; Hoyois, A.; Mosteanu, O.; et al. Endoscopic management of enteral tubes in adult patients—Part 2: Peri- and post-procedural management. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021, 53, 178–195. [Google Scholar] [CrossRef]
- Nunes, G.; Santos, C.A.; Grunho, M.; Fonseca, J. Enteral feeding through endoscopic gastrostomy in amyotrophic lateral sclerosis patients. Nutr. Hosp. 2016, 33, 561. [Google Scholar] [CrossRef]
- Lubart, E.; Leibovitz, A.; Dror, Y.; Katz, E.; Segal, R. Mortality after nasogastric tube feeding initiation in long-term care elderly with oropharyngeal dysphagia -the contribution of refeeding syndrome. Gerontology 2009, 55, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Nunes, G.; Brito, M.; Patita, M.; Santos, C.A.; Fonseca, J. Hypophosphatemia before endoscopic gastrostomy predicts higher mortality during the first week and first month post-gastrostomy a risk marker of refeeding syndrome in gastrostomy-fed patients. Nutr. Hosp. 2019, 36, 247–252. [Google Scholar] [PubMed]
- Ito, J.; Uchida, H.; Yokote, T.; Ohtake, K.; Kobayashi, J. Fasting-induced intestinal apoptosis is mediated by inducible nitric oxide synthase and interferon-{gamma} in rat. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 298, G916–G926. [Google Scholar] [CrossRef] [PubMed]
- Chappell, V.L.; Thompson, M.D.; Jeschke, M.G.; Chung, D.H.; Thompson, J.C.; Wolf, S.E. Effects of incremental starvation on gut mucosa. Dig. Dis. Sci. 2003, 48, 765–769. [Google Scholar] [CrossRef] [PubMed]
- Habold, C.; Reichardt, F.; Foltzer-Jourdainne, C.; Lignot, J.H. Morphological changes of the rat intestinal lining in relation to body stores depletion during fasting and after refeeding. Pflug. Arch. 2007, 455, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Gorostiza, E.; Poullain, M.G.; Marche, C.; Gobert, J.G.; Broyart, J.P.; Macry, J.; Cezard, J.P. Effect of fasting and refeeding on the adaptation of the small intestine in rats. A model for physiopathologic studies. Gastroenterol. Clin. Biol. 1985, 9, 790–796. [Google Scholar] [PubMed]
- Song, J.; Wolf, S.E.; Wu, X.W.; Finnerty, C.C.; Herndon, D.N.; Jeschke, M.G. Proximal gut mucosal epithelial homeostasis in aged IL-1 type I receptor knockout mice after starvation. J. Surg. Res. 2011, 169, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Dou, Y.; Gregersen, S.; Zhao, J.; Zhuang, F.; Gregersen, H. Morphometric and biomechanical intestinal remodeling induced by fasting in rats. Dig. Dis. Sci. 2002, 47, 1158–1168. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L. To Create a Consensus on Malnutrition Diagnostic Criteria. JPEN J. Parenter. Enter. Nutr. 2017, 41, 311–314. [Google Scholar] [CrossRef]
- Veitch, A.M.; Radaelli, F.; Alikhan, R.; Dumonceau, J.M.; Eaton, D.; Jerrome, J.; Lester, W.; Nylander, D.; Thoufeeq, M.; Vanbiervliet, G.; et al. Endoscopy in patients on antiplatelet or anticoagulant therapy: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guideline update. Endoscopy 2021, 53, 947–969. [Google Scholar] [CrossRef]
- Stewart, A.; Marfell-Jones, M.; Olds, T. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Lower Hutt, New Zealand, 2011. [Google Scholar]
- Powell-Tuck, J.; Hennessy, E. A comparison of mid upper arm circumference, body mass index and weight loss as indices of undernutrition in acutely hospitalized patients. Clin. Nutr. 2003, 22, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Barosa, R.; Roque Ramos, L.; Santos, C.A.; Pereira, M.; Fonseca, J. Mid upper arm circumference and Powell-Tuck and Hennessy’s equation correlate with body mass index and can be used sequentially in gastrostomy fed patients. Clin. Nutr. 2018, 37, 1584–1588. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C.; Austin, P.; Boeykens, K.; Chourdakis, M.; Cuerda, C.; Jonkers-Schuitema, C.; Lichota, M.; Nyulasi, I.; Schneider, S.M.; Stanga, Z.; et al. ESPEN practical guideline: Home enteral nutrition. Clin. Nutr. 2022, 41, 468–488. [Google Scholar] [CrossRef]
- López-Gómez, J.J.; Ballesteros-Pomar, M.D.; Torres-Torres, B.; Pintor-De la Maza, B.; Penacho-Lázaro, M.A.; Palacio-Mures, J.M.; Abreu-Padín, C.; Sanz-Gallego, I.; De Luis-Román, D.A. Impact of Percutaneous Endoscopic Gastrostomy (PEG) on the Evolution of Disease in Patients with Amyotrophic Lateral Sclerosis (ALS). Nutrients 2021, 13, 2765. [Google Scholar] [CrossRef] [PubMed]
- Lanyero, B.; Grenov, B.; Barungi, N.N.; Namusoke, H.; Michaelsen, K.F.; Mupere, E.; Mølgaard, C.; Jiang, P.; Frøkiær, H.; Wiese, M.; et al. Correlates of Gut Function in Children Hospitalized for Severe Acute Malnutrition, a Cross-sectional Study in Uganda. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 292–298. [Google Scholar] [CrossRef]
- Hasan, M.; Ferguson, A. Measurements of intestinal villi non-specific and ulcer-associated duodenitis-correlation between area of microdissected villus and villus epithelial cell count. J. Clin. Pathol. 1981, 34, 1181–1186. [Google Scholar] [CrossRef]
- Kai, Y. Intestinal villus structure contributes to even shedding of epithelial cells. Biophys. J. 2021, 120, 699–710. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics—Count (%) | ||
|---|---|---|
| Age | M = 67.1 ± 13.5 years | |
| Gender | Male: 16 Female: 14 | (53.3) (46.7) |
| Indication for PEG | Amyotrophic lateral sclerosis: 27 Post-stroke: 2 Esophageal dysmotility: 1 | (90) (6.7) (3.3) |
| Body Mass Index | Low: 12 Normal: 18 | (40) (60) |
| Albumin | Low: 1 Normal: 29 | (3.3) (96.7) |
| Transferrin | Low: 9 Normal: 21 | (30) (70) |
| Total Cholesterol | Low: 8 Normal: 22 | (26.7) (73.3) |
| Duodenal Histology | Normal: 27 Marsh 3A: 2 Marsh 3B: 1 | (90) (6.7) (3.3) |
| Duodenal Villi Length | M = 0.4 ± 0.09 mm | |
| <0.5 mm: 22 ≥0.5 mm: 8 | (73.3) (26.7) | |
| Duodenal Ultrastructure | Shortening, bending, and disruption of microvilli Autophagic vacuoles Dilation and vesiculation of the ER Dilated intercellular spaces Basal membrane detachment | |
| Patient | Histology (T0) | Villi Length (T0) | Villi Length (T1) | Histology (T1) |
|---|---|---|---|---|
| 1 | Normal | 0.6 | 0.6 | Normal |
| 2 | Marsh IIIB | 0.25 | 0.4 | Marsh IIIA |
| 3 | Normal | 0.6 | 0.85 | Normal |
| 4 | Normal | 0.4 | 0.6 | Normal |
| 5 | Marsh IIIA | 0.3 | 0.35 | Normal |
| 6 | Normal | 0.3 | 0.5 | Normal |
| 7 | Normal | 0.4 | 0.45 | Normal |
| 8 | Normal | 0.35 | 0.5 | Normal |
| 9 | Normal | 0.4 | 0.7 | Normal |
| 10 | Normal | 0.3 | 0.6 | Normal |
| 11 | Normal | 0.4 | 0.5 | Normal |
| 12 | Marsh IIIA | 0.3 | 0.5 | Normal |
| 13 | Normal | 0.35 | 0.5 | Normal |
| 14 | Normal | Artefact | 0.5 | Normal |
| 15 | Normal | 0.4 | PEG removed | |
| 16 | Normal | 0.5 | Deceased | |
| 17 | Normal | 0.4 | Deceased | |
| 18 | Normal | 0.6 | Deceased | |
| 19 | Normal | 0.4 | Deceased | |
| 20 | Normal | 0.4 | Deceased | |
| 21 | Normal | 0.3 | Deceased | |
| 22 | Normal | 0.4 | Deceased | |
| 23 | Normal | 0.4 | Deceased | |
| 24 | Normal | Artefact | Deceased | |
| 25 | Normal | 0.35 | Lost for follow-up | |
| 26 | Normal | 0.4 | Lost for follow-up | |
| 27 | Normal | 0.4 | Lost for follow-up | |
| 28 | Normal | 0.5 | Lost for follow-up | |
| 29 | Normal | 0.4 | Lost for follow-up | |
| 30 | Normal | 0.4 | Lost for follow-up | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nunes, G.; Guimarães, M.; Coelho, H.; Carregosa, R.; Oliveira, C.; Pereira, S.S.; Alves de Matos, A.; Fonseca, J. Prolonged Fasting Induces Histological and Ultrastructural Changes in the Intestinal Mucosa That May Reduce Absorption and Revert after Enteral Refeeding. Nutrients 2024, 16, 128. https://doi.org/10.3390/nu16010128
Nunes G, Guimarães M, Coelho H, Carregosa R, Oliveira C, Pereira SS, Alves de Matos A, Fonseca J. Prolonged Fasting Induces Histological and Ultrastructural Changes in the Intestinal Mucosa That May Reduce Absorption and Revert after Enteral Refeeding. Nutrients. 2024; 16(1):128. https://doi.org/10.3390/nu16010128
Chicago/Turabian StyleNunes, Gonçalo, Marta Guimarães, Hélder Coelho, Ricardo Carregosa, Cátia Oliveira, Sofia S. Pereira, António Alves de Matos, and Jorge Fonseca. 2024. "Prolonged Fasting Induces Histological and Ultrastructural Changes in the Intestinal Mucosa That May Reduce Absorption and Revert after Enteral Refeeding" Nutrients 16, no. 1: 128. https://doi.org/10.3390/nu16010128
APA StyleNunes, G., Guimarães, M., Coelho, H., Carregosa, R., Oliveira, C., Pereira, S. S., Alves de Matos, A., & Fonseca, J. (2024). Prolonged Fasting Induces Histological and Ultrastructural Changes in the Intestinal Mucosa That May Reduce Absorption and Revert after Enteral Refeeding. Nutrients, 16(1), 128. https://doi.org/10.3390/nu16010128