
Eating Behaviours of Polish and Portuguese Adults—Cross-Sectional Surveys


Abstract
1. Introduction
1.1. Body Mass Index as a Health-Related Indicator
- Underweight, BMI score < 18.5 kg/m2;
- Normal weight (optimal), 18.5–24.9 kg/m2;
- Overweight (pre-obese), 25–29.9 kg/m2;
- Obese type I ≥ 30–34.9 kg/m2;
- Obese type II 35–39.9 kg/m2;
- Obese type III ≥ 40 kg/m2 [13].
1.2. Poland and Portugal, Nutritional- and Health-Status Characteristics
1.3. Portugal
1.4. Poland
1.5. Similarities in Nutrition and Health Status in Portugal and Poland
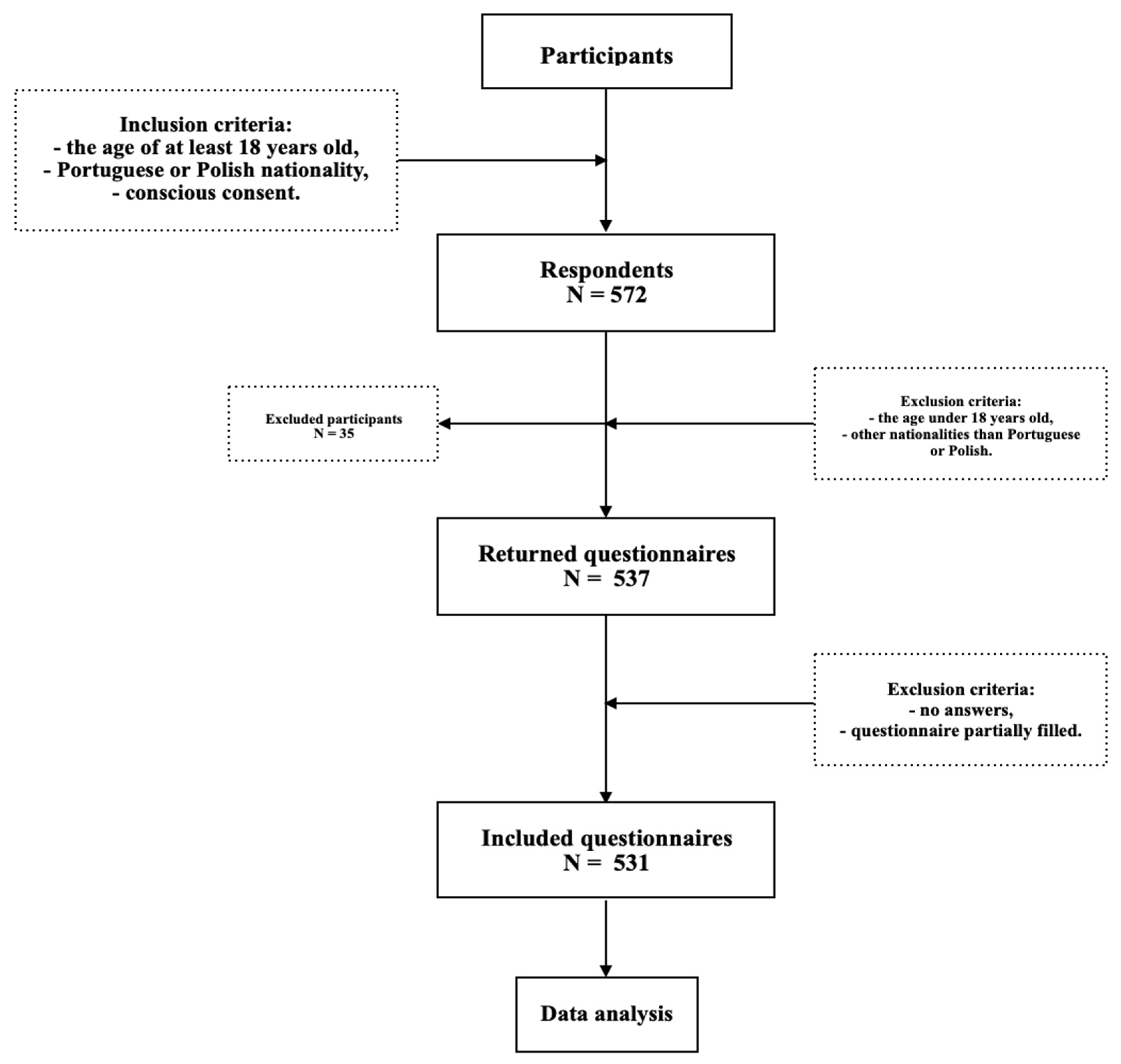
2. Materials and Methods
3. Results
3.1. Study Group
3.2. Health-Related Measurements
3.3. Daily Behaviours
3.4. Eating Behaviours
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- La Caille, L. Eating Behavior. In Encyclopedia of Behavioral Medicine; Gellman Marc, D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 641–642. ISBN 978-1-4419-1005-9. [Google Scholar]
- Ludwig, D.S.; Aronne, L.J.; Astrup, A.; De Cabo, R.; Cantley, L.C.; Friedman, M.I.; Heymsfield, S.B.; Johnson, J.D.; King, J.C.; Krauss, R.M.; et al. The Carbohydrate-Insulin Model: A Physiological Perspective on the Obesity Pandemic. Am. J. Clin. Nutr. 2021, 114, 1873–1885. [Google Scholar] [CrossRef] [PubMed]
- Warkentin, S.; Costa, A.; Oliveira, A. Validity of the Adult Eating Behavior Questionnaire and Its Relationship with Parent-Reported Eating Behaviors among Adolescents in Portugal. Nutrients 2022, 14, 1301. [Google Scholar] [CrossRef] [PubMed]
- Braden, A.; Musher-Eizenman, D.; Watford, T.; Emley, E. Eating When Depressed, Anxious, Bored, or Happy: Are Emotional Eating Types Associated with Unique Psychological and Physical Health Correlates? Appetite 2018, 125, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed]
- González-Monroy, C.; Gómez-Gómez, I.; Olarte-Sánchez, C.M.; Motrico, E. Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies. Int. J. Environ. Res. Public Health 2021, 18, 11130. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Simeone, M.; Scarpato, D. Sustainable Consumption: How Does Social Media Affect Food Choices? J. Clean. Prod. 2020, 277, 124036. [Google Scholar] [CrossRef]
- Rounsefell, K.; Gibson, S.; McLean, S.; Blair, M.; Molenaar, A.; Brennan, L.; Truby, H.; McCaffrey, T.A. Social Media, Body Image and Food Choices in Healthy Young Adults: A Mixed Methods Systematic Review. Nutr. Diet. 2020, 77, 19–40. [Google Scholar] [CrossRef]
- Fox, A.; Feng, W.; Asal, V. What Is Driving Global Obesity Trends? Globalization or “Modernization”? Glob. Health 2019, 15, 32. [Google Scholar] [CrossRef]
- De Andrade, P. Globalization of Consumption, Lifestyles and ‘Viral Society’. Rev. Estud. Intercult. REI 2021, 1–25. [Google Scholar] [CrossRef]
- Ng, C.D.; Elliott, M.R.; Riosmena, F.; Cunningham, S.A. Beyond Recent BMI: BMI Exposure Metrics and Their Relationship to Health. SSM-Popul. Health 2020, 11, 100547. [Google Scholar] [CrossRef]
- Simkova, S.; Dvorackova, O.; Velemínsky, M. Assessment of Healthy Lifestyles in Relation to BMI. Neuro Endocrinol. Lett. 2022, 43, 393–399. [Google Scholar]
- World Health Organization. Body Mass Index among Adults. Available online: https://www.who.int/data/gho/data/themes/topics/indicator-groups/indicator-group-details/GHO/bmi-among-adults (accessed on 11 February 2023).
- Jarosz, M.; Rychlik, E.; Stoś, K.; Charzewska, J. Normy Żywienia Dla Populacji Polski i Ich Zastosowanie; National Insitute of Public Health: Warsaw, Poland, 2020. [Google Scholar]
- Lopes, C.; Torres, D.; Oliveira, A.; Severo, M.; Guiomar, S.; Alarcão, V.; Ramos, E.; Rodrigues, S.; Vilela, S.; Oliveira, L.; et al. National Food, Nutrition, and Physical Activity Survey of the Portuguese General Population, IAN-AF 2015–2016. JMIR Res. Protoc. 2018, 7, e8990. [Google Scholar]
- Gregório, M.J.; Afonso Henriques, A.D.; da Graça Freitas, M.; Mestre, R.; Teixeira, D.; Salvador, C.; Graça, P. Programa Nacional Para a Promoção da Alimentação Saudável 2022–2030; Direção-Geral da Saúde: Lisboa, Portugal, 2023. [Google Scholar]
- Wojtyniak, B.; Goryński, P. (Eds.) Health Status of Polish Population and Its Determinants 2022; National Insitute of Public Health: Warsaw, Poland, 2022. [Google Scholar]
- Moraes, M.M.; Oliveira, B.; Afonso, C.; Santos, C.; Miranda, R.C.; Rauber, F.; Levy, R.B.; Rodrigues, S. Mediterranean Diet, Sociodemographic Factors and Ultra-Processed Food Consumption in Portugal. Eur. J. Public Health 2020, 30, ckaa165.434. [Google Scholar] [CrossRef]
- Real, H.; Dias, R.R.; Graça, P. Mediterranean Diet Conceptual Model and Future Trends of Its Use in Portugal. Health Promot. Int. 2021, 36, 548–560. [Google Scholar] [CrossRef]
- Marinho, A.R.; Severo, M.; Correia, D.; Lobato, L.; Vilela, S.; Oliveira, A.; Ramos, E.; Torres, D.; Lopes, C. Total, Added and Free Sugar Intakes, Dietary Sources and Determinants of Consumption in Portugal: The National Food, Nutrition and Physical Activity Survey (IAN-AF 2015–2016). Public Health Nutr. 2020, 23, 869–881. [Google Scholar] [CrossRef]
- Poínhos, R.; Oliveira, B.M.P.M.; Correia, F. Eating Behavior in Portuguese Higher Education Students: The Effect of Social Desirability. Nutrition 2015, 31, 310–314. [Google Scholar] [CrossRef]
- ISE. Balança Alimentar Portuguesa: 2020; Institute of Education and Sciences: Lisboa, Portugal, 2021. [Google Scholar]
- Our World in Data Daily Supply of Calories per Person, 2015 to 2018. Available online: https://ourworldindata.org/food-supply (accessed on 18 February 2023).
- Destri, K.; Alves, J.; Gregório, M.J.; Dias, S.S.; Henriques, A.R.; Mendonça, N.; Canhão, H.; Rodrigues, A.M. Obesity- Attributable Costs of Absenteeism among Working Adults in Portugal. BMC Public Health 2022, 22, 978. [Google Scholar] [CrossRef]
- Borusiak, B.; Szymkowiak, A.; Kucharska, B.; Gálová, J.; Mravcová, A. Predictors of Intention to Reduce Meat Consumption Due to Environmental Reasons—Results from Poland and Slovakia. Meat Sci. 2022, 184, 108674. [Google Scholar] [CrossRef]
- Hannah, R. Roser Max Obesity. Available online: https://ourworldindata.org/obesity (accessed on 18 February 2023).
- Guzek, D.; Skolmowska, D.; Głąbska, D. Appetitive Traits in a Population-Based Study of Polish Adolescents within the Place-19 Study: Validation of the Adult Eating Behavior Questionnaire. Nutrients 2020, 12, 3889. [Google Scholar] [CrossRef]
- Lopes, C.; Aro, A.; Azevedo, A.; Ramos, E.; Barros, H. Intake and Adipose Tissue Composition of Fatty Acids and Risk of Myocardial Infarction in a Male Portuguese Community Sample. J. Am. Diet. Assoc. 2007, 107, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Bedyńska, S.; Książek, M. Statystyczny Drogowskaz: Praktyczny Przewodnik Wykorzystania Modeli Regresji Oraz Równań Strukturalnych; Wydawnictwo Akademickie Sedno: Warsaw, Poland, 2012. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; Sage Publications Ltd.: London, UK, 2009. [Google Scholar]
- Bhurosy, T.; Jeewon, R. Overweight and Obesity Epidemic in Developing Countries: A Problem with Diet, Physical Activity, or Socioeconomic Status? Sci. World J. 2014, 2014, 964236. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.; Khurana, L. Obesity and the Metabolic Syndrome in Developing Countries. J. Clin. Endocrinol. Metab. 2008, 93, s9–s30. [Google Scholar] [CrossRef] [PubMed]
- Sardinha, L.B.; Santos, D.A.; Silva, A.M.; Coelho-e-Silva, M.J.; Raimundo, A.M.; Moreira, H.; Santos, R.; Vale, S.; Baptista, F.; Mota, J. Prevalence of Overweight, Obesity, and Abdominal Obesity in a Representative Sample of Portuguese Adults. PLoS ONE 2012, 7, e47883. [Google Scholar] [CrossRef]
- Okati-Aliabad, H.; Ansari-Moghaddam, A.; Kargar, S.; Jabbari, N. Prevalence of Obesity and Overweight among Adults in the Middle East Countries from 2000 to 2020: A Systematic Review and Meta-Analysis. J. Obes. 2022, 2022, 8074837. [Google Scholar] [CrossRef]
- Albury, C.; Strain, W.D.; Brocq, S.L.; Logue, J.; Lloyd, C.; Tahrani, A. The Importance of Language in Engagement between Health-Care Professionals and People Living with Obesity: A Joint Consensus Statement. Lancet Diabetes Endocrinol. 2020, 8, 447–455. [Google Scholar] [CrossRef]
- Dietz, W.H.; Baur, L.A.; Hall, K.; Puhl, R.M.; Taveras, E.M.; Uauy, R.; Kopelman, P. Management of Obesity: Improvement of Health-Care Training and Systems for Prevention and Care. Lancet 2015, 385, 2521–2533. [Google Scholar] [CrossRef]
- Kahleova, H.; Lloren, J.I.; Mashchak, A.; Hill, M.; Fraser, G.E. Meal Frequency and Timing Are Associatedwith Changes in Body Mass Index in Adventist Health Study 2. J. Nutr. 2017, 147, 1722–1728. [Google Scholar] [CrossRef]
- Barrington, W.E.; Beresford, S.A.A. Eating Occasions, Obesity and Related Behaviors in Working Adults: Does It Matter When You Snack? Nutrients 2019, 11, 2320. [Google Scholar] [CrossRef]
- Lopez-Minguez, J.; Gómez-Abellán, P.; Garaulet, M. Timing of Breakfast, Lunch, and Dinner. Effects on Obesity and Metabolic Risk. Nutrients 2019, 11, 2624. [Google Scholar] [CrossRef]
- Baron, K.G.; Reid, K.J.; Van Horn, L.; Zee, P.C. Contribution of Evening Macronutrient Intake to Total Caloric Intake and Body Mass Index. Appetite 2013, 60, 246–251. [Google Scholar] [CrossRef]
- Kuntsche, E.; Rehm, J.; Gmel, G. Characteristics of Binge Drinkers in Europe. Soc. Sci. Med. 2004, 59, 113–127. [Google Scholar] [CrossRef]
- Lannoy, S.; Duka, T.; Carbia, C.; Billieux, J.; Fontesse, S.; Dormal, V.; Gierski, F.; López-Caneda, E.; Sullivan, E.V.; Maurage, P. Emotional Processes in Binge Drinking: A Systematic Review and Perspective. Clin. Psychol. Rev. 2021, 84, 101971. [Google Scholar] [CrossRef]
- Shelton, N.J.; Knott, C.S. Association Between Alcohol Calorie Intake and Overweight and Obesity in English Adults. Am. J. Public Health 2014, 104, 629–631. [Google Scholar] [CrossRef]
- Tran, E.; Dale, H.F.; Jensen, C.; Lied, G.A. Effects of Plant-Based Diets on Weight Status: A Systematic Review. Diabetes Metab. Syndr. Obes. 2020, 13, 3433–3448. [Google Scholar] [CrossRef]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Personal, Population, and Planetary Health. Adv. Nutr. 2019, 10, S275–S283. [Google Scholar] [CrossRef]
- Pfeiler, T.M.; Egloff, B. Personality and Eating Habits Revisited: Associations between the Big Five, Food Choices, and Body Mass Index in a Representative Australian Sample. Appetite 2020, 149, 104607. [Google Scholar] [CrossRef]
- Coakley, K.E.; Lardier, D.T.; Le, H.; Wilks, A. Food Approach and Avoidance Appetitive Traits in University Students: A Latent Profile Analysis. Appetite 2022, 168, 105667. [Google Scholar] [CrossRef]
- Hunot, C.; Fildes, A.; Croker, H.; Llewellyn, C.H.; Wardle, J.; Beeken, R.J. Appetitive Traits and Relationships with BMI in Adults: Development of the Adult Eating Behaviour Questionnaire. Appetite 2016, 105, 356–363. [Google Scholar] [CrossRef]
- Mallan, K.M.; Fildes, A.; de la Piedad Garcia, X.; Drzezdzon, J.; Sampson, M.; Llewellyn, C. Appetitive Traits Associated with Higher and Lower Body Mass Index: Evaluating the Validity of the Adult Eating Behaviour Questionnaire in an Australian Sample. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 130. [Google Scholar] [CrossRef]
- Dorosh, N.; Boyko, O.; Kleszczewska, E.; Łogwiniuk, K.; Andryszczyk, M.; Wyższa Szkoła Zawodowa Suwałkach, P.; Marketingu Przedsiębiorczości, K.; Zarządzania, W.; Białostocka, P. Porównanie Nawyków Żywieniowych Studentów Na Ukrainie i w Polsce. Część I. Badania Ankietowe Comparison of Dietary Habits of Students in Ukraine and Poland. Part I. Survey Data; Uniwersytet Medyczny We Lwowie: Lviv, Ukraine, 2013; Volume 48. [Google Scholar]
- Hunot-Alexander, C.; Arellano-Gómez, L.P.; Smith, A.D.; Kaufer-Horwitz, M.; Vásquez-Garibay, E.M.; Romero-Velarde, E.; Fildes, A.; Croker, H.; Llewellyn, C.H.; Beeken, R.J. Examining the Validity and Consistency of the Adult Eating Behaviour Questionnaire-Español (AEBQ-Esp) and Its Relationship to BMI in a Mexican Population. Eat. Weight. Disord. 2022, 27, 651–663. [Google Scholar] [CrossRef] [PubMed]
- Viana, V.; Sinde, S.; Saxton, J.C. Children’s Eating Behaviour Questionnaire: Associations with BMI in Portuguese Children. Br. J. Nutr. 2008, 100, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Poínhos, R.; Oliveira, B.M.P.M.; Correia, F. Eating Behaviour Patterns and BMI in Portuguese Higher Education Students. Appetite 2013, 71, 314–320. [Google Scholar] [CrossRef]
- Zickgraf, H.F.; Rigby, A. The Adult Eating Behaviour Questionnaire in a Bariatric Surgery-Seeking Sample: Factor Structure, Convergent Validity, and Associations with BMI. Eur. Eat. Disord. Rev. 2019, 27, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Verzijl, C.L.; Ahlich, E.; Schlauch, R.C.; Rancourt, D. The Role of Craving in Emotional and Uncontrolled Eating. Appetite 2018, 123, 146–151. [Google Scholar] [CrossRef]
- van Strien, T. Causes of Emotional Eating and Matched Treatment of Obesity. Curr. Diab. Rep. 2018, 18, 35. [Google Scholar] [CrossRef]
- Kaźmierczak-Wojtaś, N.; Niedzielski, A.; Drozd, M. Orthorexic Tendencies and the Structure of Achievement Motivation in Young People in Poland. Nutrition 2022, 103–104, 111795. [Google Scholar] [CrossRef]
- Torres, S.J.; Nowson, C.A. Relationship between Stress, Eating Behavior, and Obesity. Nutrition 2007, 23, 887–894. [Google Scholar] [CrossRef]
- Yau, Y.H.C.; Potenza, M.N. Stress and Eating Behaviors. Minerva Endocrinol. 2013, 138, 255–267. [Google Scholar]
- Robinson, E.; Marty, L.; Higgs, S.; Jones, A. Interoception, Eating Behaviour and Body Weight. Physiol. Behav. 2021, 237, 113434. [Google Scholar] [CrossRef]
- Quick, V.M.; Byrd-Bredbenner, C. Disordered Eating, Socio-Cultural Media Influencers, Body Image, and Psychological Factors among a Racially/Ethnically Diverse Population of College Women. Eat. Behav. 2014, 15, 37–41. [Google Scholar] [CrossRef]
- Walsh, B.T. The Importance of Eating Behavior in Eating Disorders. Physiol. Behav. 2011, 104, 525–529. [Google Scholar] [CrossRef]
- Washburn, J.J.; Soto, D.; Osorio, C.A.; Slesinger, N.C. Eating Disorder Behaviors as a Form of Non-Suicidal Self-Injury. Psychiatry Res. 2023, 319, 115002. [Google Scholar] [CrossRef]
- Smink, F.R.E.; Van Hoeken, D.; Hoek, H.W. Epidemiology of Eating Disorders: Incidence, Prevalence and Mortality Rates. Curr. Psychiatry Rep. 2012, 14, 406–414. [Google Scholar] [CrossRef]
- Campos, M.B.; Menezes, I.H.C.F.; do Rosário Gondim Peixoto, M.; Schincaglia, R.M. Intuitive Eating in General Aspects of Eating Behaviors in Individuals with Obesity: Randomized Clinical Trial. Clin. Nutr. ESPEN 2022, 50, 24–32. [Google Scholar] [CrossRef]
- Lowe, M.R.; Doshi, S.D.; Katterman, S.N.; Feig, E.H. Dieting and Restrained Eating as Prospective Predictors of Weight Gain. Front. Psychol. 2013, 4, 577. [Google Scholar] [CrossRef]
- Benton, D.; Young, H.A. Reducing Calorie Intake May Not Help You Lose Body Weight. Perspect. Psychol. Sci. 2017, 12, 703–714. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| R | M | SD | Mdn | Sk | Kurt | D | |
|---|---|---|---|---|---|---|---|
| total | |||||||
| age | 18–78 | 25.84 | 8.91 | 23 | 2.09 | 5.13 | 0.23 ** |
| weight | 40–124 | 64.75 | 13.37 | 62 | 1.11 | 1.87 | 0.10 ** |
| height | 145–198 | 168.39 | 8.99 | 168 | 0.53 | 0.11 | 0.09 ** |
| Portuguese | |||||||
| age | 18–66 | 23.79 | 7.40 | 22 | 2.51 | 7.45 | 0.24 ** |
| weight | 40–115 | 62.74 | 11.84 | 60 | 0.86 | 0.90 | 0.11 ** |
| height | 145–192 | 166.58 | 8.35 | 165 | 0.46 | −0.16 | 0.11 ** |
| BMI | 15.06–34.72 | 22.52 | 3.33 | 22.04 | 0.91 | 1.09 | 0.08 ** |
| Polish | |||||||
| age | 18–78 | 28.62 | 9.98 | 24 | 1.74 | 3.54 | 0.21 ** |
| weight | 43–124 | 67.49 | 14.80 | 64 | 1.14 | 1.74 | 0.11 ** |
| height | 151–198 | 170.86 | 9.26 | 170 | 0.54 | 0.11 | 0.07 ** |
| BMI | 15.32–41.52 | 22.99 | 3.99 | 22.49 | 1.52 | 4.19 | 0.09 ** |
| men | |||||||
| age | 18.00–78.00 | 27.56 | 10.63 | 23.00 | 2.04 | 4.80 | 0.20 ** |
| weight | 48.00–121.00 | 77.29 | 13.20 | 77.00 | 0.55 | 1.04 | 0.10 ** |
| height | 164.00–198.00 | 179.04 | 7.13 | 179.00 | 0.41 | −0.07 | 0.08 |
| BMI | 15.32–36.93 | 24.03 | 3.37 | 23.91 | 0.62 | 1.58 | 0.07 |
| women | |||||||
| age | 18.00–71.00 | 25.32 | 8.29 | 23.00 | 1.99 | 4.29 | 0.24 ** |
| weight | 40.00–124.00 | 60.82 | 10.82 | 59.00 | 1.52 | 5.01 | 0.10 ** |
| height | 145.00–183.00 | 165.07 | 6.67 | 164.00 | 0.22 | −0.17 | 0.08 ** |
| BMI | 15.06–41.52 | 22.30 | 3.62 | 21.71 | 1.61 | 4.53 | 0.10 ** |
| Variables | Portuguese (n = 306) | Polish (n = 225) | |||||
|---|---|---|---|---|---|---|---|
| Mdn | Mrang | Mdn | Mrang | U | p | Rg | |
| age | 22.00 | 220.49 | 24.00 | 327.90 | 20498.00 | <0.001 | 0.40 |
| weight | 60.00 | 245.52 | 64.00 | 293.86 | 28157.00 | <0.001 | 0.18 |
| height | 165.00 | 235.95 | 170.00 | 306.86 | 25230.50 | <0.001 | 0.27 |
| BMI | 22.04 | 259.78 | 22.49 | 274.46 | 32522.50 | 0.276 | 0.06 |
| Source of Variation | F | p | η2 |
|---|---|---|---|
| nationality | 0.63 | 0.427 | 0.00 |
| gender | 4.96 | 0.026 | 0.01 |
| age | 21.94 | <0.001 | 0.04 |
| nationality × gender | 0.05 | 0.818 | 0.00 |
| nationality × age | 1.25 | 0.265 | 0.00 |
| gender × age | 0.64 | 0.423 | 0.00 |
| nationality × gender × age | 0.03 | 0.857 | 0.00 |
| Variable | BMI |
|---|---|
| age | 0.16 ** |
| weekly frequency: breakfast | −0.01 |
| weekly frequency: second breakfast/morning snack | −0.02 |
| weekly frequency: lunch | −0.04 |
| weekly frequency: dessert/afternoon snack | −0.05 |
| weekly frequency: dinner | −0.01 |
| weekly frequency: dessert/night snack | 0.00 |
| time (hour): breakfast | 0.03 |
| time (hour): second breakfast/morning snack | 0.01 |
| time (hour): lunch | −0.01 |
| time (hour): dessert/afternoon snack | −0.03 |
| time (hour): dinner | 0.00 |
| time (hour): dessert/night snack | −0.03 |
| number of skipped meals | 0.02 |
| binge drinking | 0.14 ** |
| Group | Mdn | Mrang | H (2) | p | Post-Hoc | |
|---|---|---|---|---|---|---|
| Dietary pattern | ||||||
| I | omnivore | 22.41 | 280.00 | 10.26 * | 0.016 | II < I * |
| II | vegetarian/vegan | 21.10 | 225.51 | III < I * | ||
| III | flexitarian | 21.84 | 235.38 |
| Variables | Portuguese (n = 298) | Polish (n = 222) | |||||
|---|---|---|---|---|---|---|---|
| Mdn | Mrang | Mdn | Mrang | U | p | Rg | |
| weekly frequency: breakfast | 4 | 255.38 | 4 | 267.37 | 31,552.50 | 0.258 | 0.05 |
| weekly frequency: second breakfast/morning snack | 2 | 233.91 | 2 | 305.02 | 24,748.00 | <0.001 | 0.27 |
| weekly frequency: lunch | 4 | 289.24 | 4 | 226.62 | 25,547.00 | <0.001 | 0.24 |
| Weekly frequency: dessert/afternoon snack | 3 | 311.93 | 2 | 200.13 | 19,628.50 | <0.001 | 0.42 |
| weekly frequency: dinner | 4 | 286.33 | 4 | 237.26 | 27,958.50 | <0.001 | 0.19 |
| weekly frequency: dessert/night snack | 1 | 262.82 | 1 | 264.43 | 33,577.00 | 0.898 | 0.01 |
| time (hour): breakfast | 8 | 233.85 | 8 | 248.58 | 26,183.50 | 0.237 | 0.06 |
| time (hour): second breakfast/morning snack | 11 | 171.59 | 11 | 203.84 | 14,217.50 | 0.002 | 0.17 |
| time (hour): lunch | 13 | 195.42 | 14 | 335.49 | 13,369.50 | <0.001 | 0.56 |
| time (hour): dessert/afternoon snack | 17 | 230.63 | 17 | 224.71 | 23,322.50 | 0.632 | 0.03 |
| time (hour): dinner | 20 | 299.39 | 20 | 210.71 | 22,064.50 | <0.001 | 0.34 |
| time (hour): dessert/night. snack | 23 | 181.05 | 21 | 89.38 | 3582.50 | <0.001 | 0.64 |
| number of skipped meals | 1 | 251.61 | 1 | 284.48 | 30,020.50 | 0.010 | 0.12 |
| binge drinking | 0 | 253.13 | 1 | 278.94 | 30,539.00 | 0.038 | 0.10 |
| Portuguese | Polish | All Sample | |||||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | α | M | SD | α | M | SD | α | |
| food approach | 2.88 | 0.60 | 0.84 | 2.89 | 0.62 | 0.86 | 2.88 | 0.60 | 0.84 |
| hunger | 2.58 | 0.71 | 0.65 | 2.66 | 0.76 | 0.69 | 2.62 | 0.73 | 0.66 |
| food responsiveness | 2.66 | 0.76 | 0.69 | 2.68 | 0.79 | 0.72 | 2.67 | 0.77 | 0.70 |
| emotional overeating | 2.85 | 1.08 | 0.89 | 2.63 | 1.05 | 0.88 | 2.75 | 1.07 | 0.89 |
| enjoyment of food | 3.73 | 0.75 | 0.75 | 3.95 | 0.95 | 0.92 | 3.82 | 0.85 | 0.78 |
| food avoidance | 2.52 | 0.59 | 0.82 | 2.55 | 0.54 | 0.82 | 2.53 | 0.57 | 0.82 |
| satiety responsiveness | 2.47 | 0.74 | 0.66 | 2.47 | 0.75 | 0.68 | 2.47 | 0.74 | 0.67 |
| emotional undereating | 2.56 | 1.03 | 0.89 | 2.82 | 1.01 | 0.86 | 2.67 | 1.03 | 0.88 |
| food fussiness | 2.37 | 0.98 | 0.89 | 2.16 | 0.86 | 0.85 | 2.28 | 0.94 | 0.88 |
| slowness in eating | 2.70 | 1.08 | 0.88 | 2.78 | 1.00 | 0.85 | 2.73 | 1.05 | 0.87 |
| Variables | Portuguese (n = 306) | Polish (n = 225) | |||||
|---|---|---|---|---|---|---|---|
| Mdn | Mrang | Mdn | Mrang | U | p | rg | |
| food approach | 2.88 | 266.14 | 2.88 | 265.81 | 34,381.50 | 0.980 | 0.00 |
| hunger | 2.60 | 261.32 | 2.60 | 272.36 | 32,994.00 | 0.411 | 0.04 |
| food responsiveness | 2.50 | 264.77 | 2.75 | 267.68 | 34,047.50 | 0.828 | 0.01 |
| emotional overeating | 2.80 | 280.65 | 2.40 | 246.08 | 29,942.00 | 0.010 | 0.13 |
| enjoyment of food | 3.67 | 242.56 | 4.00 | 296.83 | 27,253.50 | <0.001 | 0.20 |
| food avoidance | 2.50 | 261.29 | 2.56 | 272.41 | 32,983.00 | 0.409 | 0.04 |
| satiety responsiveness | 2.50 | 266.97 | 2.50 | 264.68 | 34,129.00 | 0.865 | 0.01 |
| emotional undereating | 2.55 | 249.38 | 2.80 | 288.60 | 29,339.00 | 0.004 | 0.15 |
| food fussiness | 2.20 | 279.35 | 2.00 | 247.84 | 30,339.00 | 0.019 | 0.12 |
| slowness in eating | 2.50 | 259.98 | 2.75 | 274.19 | 32,581.50 | 0.290 | 0.05 |
| Variables | Food Approach | Food Avoidance |
|---|---|---|
| age | −0.02 | −0.04 |
| weekly frequency: breakfast | 0.05 | −0.03 |
| weekly frequency: second breakfast/morning snack | 0.02 | −0.03 |
| weekly frequency: lunch | 0.02 | −0.10 ** |
| weekly frequency: dessert/afternoon snack | 0.03 | −0.04 |
| weekly frequency: dinner | −0.00 | −0.06 |
| weekly frequency: dessert/night snack | 0.13 ** | 0.01 |
| time (hour): breakfast | 0.02 | 0.03 |
| time (hour): second breakfast/morning snack | 0.01 | 0.07 |
| time (hour): lunch | −0.01 | 0.03 |
| time (hour): dessert/afternoon breakfast | −0.01 | 0.06 |
| time (hour): dinner | −0.01 | 0.03 |
| time (hour): dessert/night snack | −0.05 | 0.01 |
| number of skipped meals | −0.12 ** | −0.00 |
| binge drinking | 0.11 ** | −0.10 ** |
| BMI | 0.09 ** | −0.19 ** |
| I: Underweight (n = 32) | II: Normal Weight (n = 303) | III: Overweight (n = 173) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mdn | Mrang | Mdn | Mrang | Mdn | Mrang | H (2) | p | ε2 | Post-Hoc | ||
| A | food approach | 2.76 | 228.00 | 2.82 | 236.43 | 3.00 | 291.05 | 16.37 | <0.001 | 0.03 | A.II < A.III ** |
| B | hunger | 2.90 | 301.81 | 2.60 | 247.28 | 2.60 | 258.40 | 4.21 | 0.122 | 0.01 | n.i. |
| C | food responsiveness | 2.50 | 229.95 | 2.50 | 246.09 | 2.75 | 273.77 | 4.92 | 0.085 | 0.01 | n.i. |
| D | emotional overeating | 2.23 | 209.97 | 2.40 | 226.48 | 3.20 | 311.81 | 40.53 | <0.001 | 0.08 | D.I < D.III ** D.II < D.III ** |
| E | enjoyment of food | 3.67 | 217.91 | 4.00 | 262.77 | 3.67 | 245.27 | 3.71 | 0.157 | 0.01 | n.i. |
| F | food avoidance | 2.81 | 305.56 | 2.56 | 265.11 | 2.44 | 226.48 | 11.77 | 0.003 | 0.02 | F.III < F.I * F.III < F.II * |
| G | satiety responsiveness | 2.50 | 262.56 | 2.50 | 250.39 | 2.50 | 260.20 | 0.60 | 0.740 | 0.00 | n.i. |
| H | emotional undereating | 3.00 | 307.91 | 2.80 | 264.49 | 2.20 | 227.13 | 11.72 | 0.003 | 0.02 | H.III < H.I * H.III < H.II * |
| I | food fussiness | 2.40 | 269.63 | 2.00 | 248.32 | 2.20 | 262.52 | 1.40 | 0.496 | 0.00 | n.i. |
| J | slowness in eating | 3.00 | 296.44 | 2.75 | 272.14 | 2.25 | 215.85 | 19.08 | <0.001 | 0.04 | J.III < J.I * J.III < J.II ** |
| Variables | I: Negative (n = 172) | II: Neutral (n = 183) | III: Positive (n = 169) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mdn | Mrang | Mdn | Mrang | Mdn | Mrang | H (2) | p | ε2 | Post-Hoc | ||
| A | food approach | 3.06 | 306.87 | 2.88 | 250.78 | 2.71 | 230.03 | 23.65 | <0.001 | 0.05 | A.II < A.I ** A.III < A.I ** |
| B | hunger | 2.60 | 280.03 | 2.60 | 266.42 | 2.40 | 240.42 | 6.07 | 0.048 | 0.01 | B.III < B.I * |
| C | food responsiveness | 2.75 | 285.34 | 2.50 | 257.35 | 2.50 | 244.83 | 6.49 | 0.039 | 0.01 | C.III < C.I * |
| D | emotional overeating | 3.20 | 323.30 | 2.40 | 236.69 | 2.40 | 228.57 | 41.72 | <0.001 | 0.08 | D.II < D.I ** D.III < D.I ** |
| E | enjoyment of food | 3.67 | 252.71 | 3.67 | 258.02 | 4.00 | 275.71 | 2.21 | 0.332 | 0.00 | n.i. |
| F | food avoidance | 2.44 | 247.08 | 2.61 | 289.20 | 2.50 | 249.28 | 8.77 | 0.012 | 0.02 | F.I < F.II * F.III < F.II * |
| G | satiety responsiveness | 2.50 | 276.02 | 2.50 | 267.80 | 2.25 | 243.00 | 4.45 | 0.108 | 0.01 | n.i. |
| H | emotional undereating | 2.40 | 236.49 | 2.80 | 290.49 | 2.60 | 258.66 | 11.50 | 0.003 | 0.02 | H.I < H.II ** |
| I | food fussiness | 2.20 | 273.77 | 2.20 | 280.05 | 2.00 | 232.03 | 10.32 | 0.006 | 0.02 | I.III < I.I * I.III < I.II ** |
| J | slowness in eating | 2.50 | 238.40 | 2.67 | 269.34 | 2.75 | 279.62 | 6.93 | 0.031 | 0.01 | J.I < J.III * |
| Variables | I: No (n = 76) | II: Yes, Reduce Body Weight (n = 198) | III: Yes, Change the Appearance of the Body Shape, without Significantly Changing the Body Weight (n = 202) | IV: Yes, Gain Body Weight (n = 43) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mdn | Mrang | Mdn | Mrang | Mdn | Mrang | Mdn | Mrang | H (3) | p | ε2 | Post-Hoc | ||
| A | food approach | 2.71 | 236.27 | 3.00 | 289.57 | 2.82 | 243.39 | 2.81 | 243.84 | 12.59 | 0.006 | 0.02 | A.III < A.II * |
| B | hunger | 2.60 | 268.33 | 2.60 | 250.00 | 2.60 | 258.50 | 2.60 | 298.36 | 3.98 | 0.264 | 0.01 | n.i. |
| C | food responsiveness | 2.50 | 236.25 | 2.75 | 273.30 | 2.50 | 256.40 | 2.50 | 257.66 | 3.63 | 0.305 | 0.01 | n.i. |
| D | emotional overeating | 2.40 | 231.84 | 3.20 | 309.54 | 2.60 | 233.25 | 2.20 | 207.31 | 36.17 | <0.001 | 0.07 | D.I < D.II ** D.III < D.II ** D.IV < D.II ** |
| E | enjoyment of food | 4.00 | 255.40 | 4.00 | 263.02 | 4.00 | 254.82 | 4.00 | 272.62 | 0.71 | 0.872 | 0.00 | n.i. |
| F | food avoidance | 2.56 | 273.32 | 2.43 | 229.40 | 2.61 | 273.97 | 2.72 | 311.71 | 15.71 | 0.001 | 0.03 | F.II < F.III * F.II < F.IV ** |
| G | satiety responsiveness | 2.50 | 263.23 | 2.50 | 254.49 | 2.50 | 270.11 | 2.25 | 232.15 | 2.74 | 0.434 | 0.01 | n.i. |
| H | emotional undereating | 2.45 | 255.09 | 2.40 | 235.89 | 2.80 | 269.31 | 3.20 | 335.97 | 17.11 | 0.001 | 0.03 | H.I < H.IV * H.II < H.IV ** H.III < H.IV * |
| I | food fussiness | 2.20 | 264.30 | 2.00 | 255.34 | 2.00 | 262.15 | 2.20 | 263.76 | 0.32 | 0.955 | 0.00 | n.i. |
| J | slowness in eating | 2.88 | 277.13 | 2.50 | 232.16 | 2.75 | 270.46 | 3.00 | 308.77 | 13.41 | 0.004 | 0.03 | J.II < J.IV * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bober, J.; Wiśniewska, K.; Okręglicka, K. Eating Behaviours of Polish and Portuguese Adults—Cross-Sectional Surveys. Nutrients 2023, 15, 1934. https://doi.org/10.3390/nu15081934
Bober J, Wiśniewska K, Okręglicka K. Eating Behaviours of Polish and Portuguese Adults—Cross-Sectional Surveys. Nutrients. 2023; 15(8):1934. https://doi.org/10.3390/nu15081934
Chicago/Turabian StyleBober, Julia, Klaudia Wiśniewska, and Katarzyna Okręglicka. 2023. "Eating Behaviours of Polish and Portuguese Adults—Cross-Sectional Surveys" Nutrients 15, no. 8: 1934. https://doi.org/10.3390/nu15081934
APA StyleBober, J., Wiśniewska, K., & Okręglicka, K. (2023). Eating Behaviours of Polish and Portuguese Adults—Cross-Sectional Surveys. Nutrients, 15(8), 1934. https://doi.org/10.3390/nu15081934