
Assessment of the Use of Food Supplements by Military Personnel: Study Protocol and Results

 ,
,  ,
,  , ,
, ,  ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Survey Instrument
- -
- The section on the use of FSSPs (3) was divided into three subsections:
- -
- (3A) The subjects were first introduced to a definition of an FSSP. Following the protocol of Zdešar Kotnik et al. [31,32], the subjects were then asked whether they had consumed any such products within the last 12 months. We also asked them where they purchased the FSSPs (multiple answers were possible). Only the users of FSSPs were asked to continue to the next subsection.
- -
- (3B) The table collection of all consumed FSSPs included: the product and manufacturer’s name, the product form (capsule, powder; tablet; syrup; gel; bar; fizzy tablet; drops; spray; plastic bottle/can; other), daily dose (e.g., 2 capsules), a URL link to the product details, and the availability of a product photo (yes/no).
- -
- (3C) Details were collected for each reported FSSP. The subjects were asked to provide the frequency of the consumption of a specific product during each season (daily, 4–6 times per week, 1–3 times per week, 1–3 times per month, less frequently, or never), and their use of the product in specific situations (during a period which required greater physical capability, during a military operation abroad, during the assessment of movement skills, and during illness). The subjects were further asked to identify the reasons for using specific products (multiple answers were possible), who recommended they use the products, and their self-reported observations of any positive or negative effects of the use of the FSSPs.
2.2. Administration of Survey Tool
2.3. Study Sample and Enrolment Details
2.4. Data Extraction
- (A)
- A spreadsheet was developed to house data about the study subjects. This spreadsheet included all the data from sections 1–2 of the survey tool. Each subject was inserted in a new line with a unique subject identification number (SID).
- (B)
- A spreadsheet was developed for data on the composition of all the reported food supplements and similar products. Different participants may have reported the use of the same FSSP, but each product was inserted into this spreadsheet only once. Each product was inserted in a new line with a unique food supplements identification number (FSID). These data originated from section 3A of the survey tool and were supplemented with detailed product compositions with the use of product labelling pictures (obtained from descriptions on the provided URL links) and from the national branded foods composition database, CLAS (Composition and Labelling Information System) [33]. Each FSSP was manually categorized. In the absence of an internationally harmonized categorization system for food supplements, a previously used categorization [13] was adapted and modified to include products similar to food supplements (vitamin–mineral supplements, vitamin supplements, mineral supplements, protein supplements, fatty acid supplements, energy drinks and caffeine supplements, sports drinks and similar creatine, herbal supplements, and other supplements). It should be noted that the food supplements were not subjected to laboratory analyses, and thus, the exact composition of the FSSP could not be verified. Altogether, 467 products were recorded, but 5 were designated as out of scope because they did not meet our definition of an FSSP (these included peanut butter, soya nuts, oatmeal, and two brands of baking powder). For the remaining 462 products, we were able to obtain detailed labelled composition data.
- (C)
- A spreadsheet was developed for data on the use of food supplements and similar products. This spreadsheet presented a link between the specific subjects (SID) and the supplements used (FSID). Each reported use of a food supplement or similar product was recorded in a separate line. For example, if subject ID1 reported using two products, two lines were inserted—each specifying details of the FSSP, including daily dosage and seasonal frequency, the origin of the recommendation, and self-reported positive/negative effects of the FSSP.
2.5. Data Analysis
3. Results and Discussion
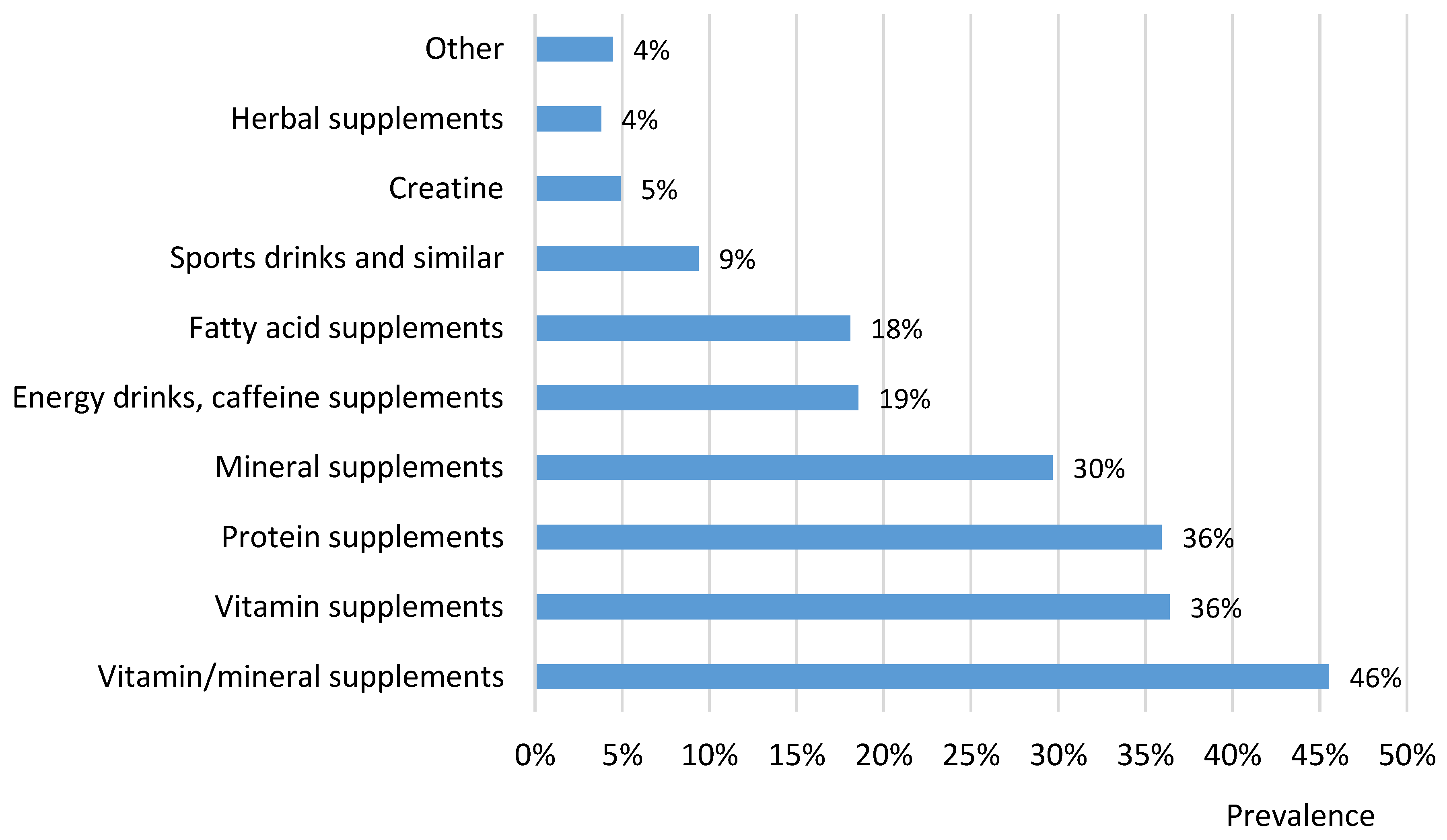
3.1. Use of Different Types of Food Supplements and Similar Products
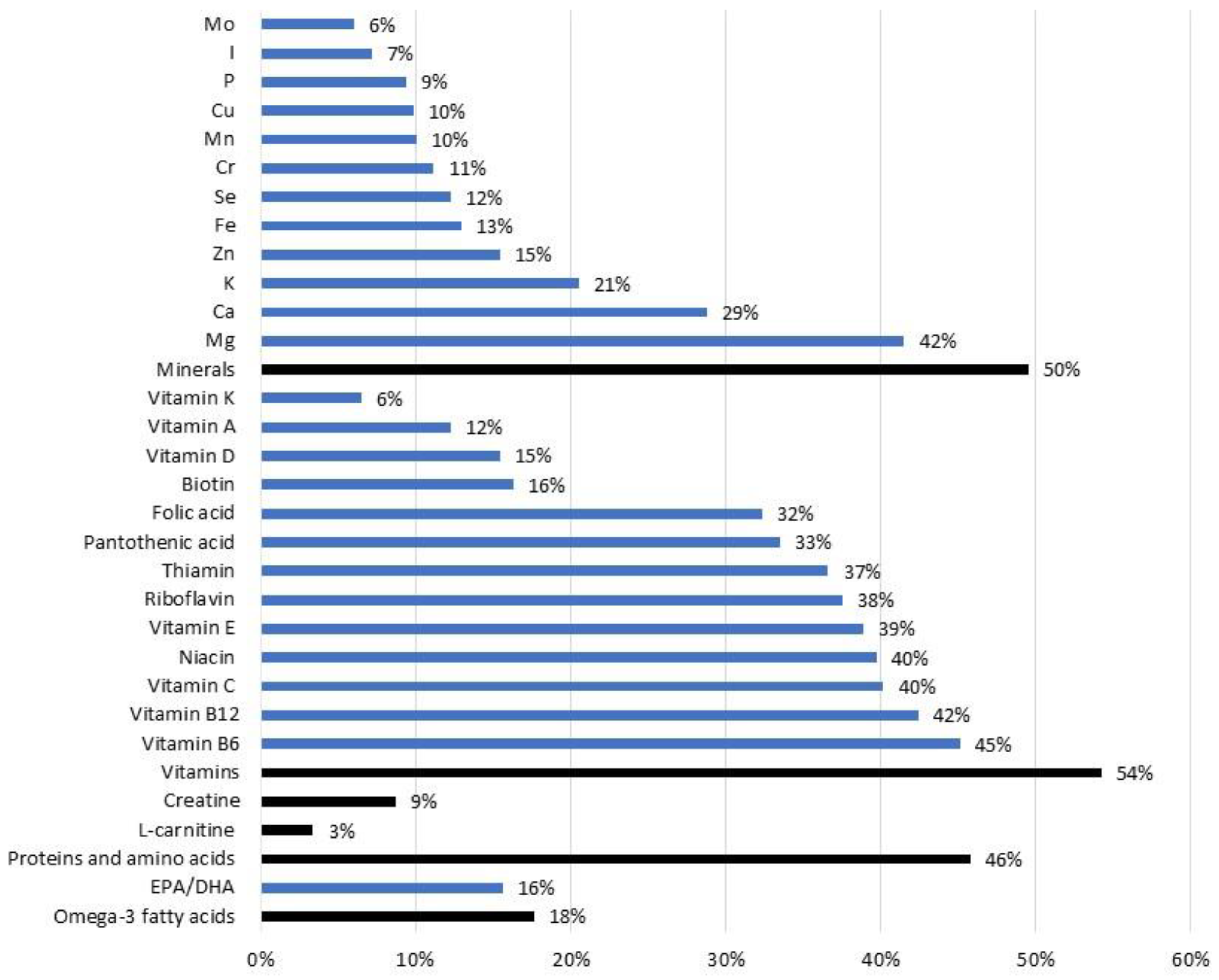
3.2. Food Supplements and Similar Products as Sources of Nutrients and Other Biologically Active Ingredients
3.3. Study Strengths and Limitations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reinert, A.; Rohrmann, S.; Becker, N.; Linseisen, J. Lifestyle and diet in people using dietary supplements: A German cohort study. Eur. J. Nutr. 2007, 46, 165–173. [Google Scholar] [CrossRef]
- Kiely, M.; Flynn, A.; Harrington, K.E.; Robson, P.; O’Connor, N.; Hannon, E.M.; O’Brien, M.M.; Bell, S.; Strain, J.J. The efficacy and safety of nutritional supplement use in a representative sample of adults in the North/South Ireland Food Consumption Survey. Public Health Nutr. 2001, 4, 1089–1097. [Google Scholar] [CrossRef]
- Grm, H.Š.; Ars, M.S.; Besednjak-Kocijančič, L.; Golja, P. Nutritional supplement use among Slovenian adolescents. Public Health Nutr. 2011, 15, 587–593. [Google Scholar]
- Eisenberg, D.M.; Davis, R.B.; Ettner, S.L.; Appel, S.; Wilkey, S.; Van Rompay, M.; Kessler, R.C. Trends in alternative medicine use in the United States, 1990–1997: Results of a follow-up national survey. JAMA 1998, 280, 1569–1575. [Google Scholar] [CrossRef] [PubMed]
- Coulter, I.D.; Newberry, S.J.; Hilton, L. Regulation of Dietary Supplements in the Military: Report of an Expert Panel; RAND Corporation: Santa Monica, CA, USA, 2011. [Google Scholar]
- IoM. Institute of Medicine: Use of Dietary Supplements by Military Personnel; Greenwood, M.R.C., Oria, M., Eds.; The National Academies Press: Washington, DC, USA, 2008; pp. 1–458. [Google Scholar]
- Gahche, J.J.; Bailey, R.L.; Potischman, N.; Dwyer, J.T. Dietary Supplement Use Was Very High among Older Adults in the United States in 2011–2014. J. Nutr. 2017, 147, 1968–1976. [Google Scholar] [CrossRef]
- Qato, D.M.; Alexander, G.C.; Guadamuz, J.S.; Lindau, S.T. Prevalence of Dietary Supplement Use in US Children and Adolescents, 2003–2014. JAMA Pediatr. 2018, 172, 780–782. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.W.; Kelly, J.P.; Rosenberg, L.; Anderson, T.E.; Mitchell, A.A. Recent patterns of medication use in the ambulatory adult population of the United States: The Slone survey. JAMA 2002, 287, 337–344. [Google Scholar] [CrossRef]
- Neuhouser, M.L.; Patterson, R.E.; Levy, L. Motivations for Using Vitamin and Mineral Supplements. J. Acad. Nutr. Diet. 1999, 99, 851–854. [Google Scholar] [CrossRef]
- MZ RS. Raziskava Javnega Mnenja o Uporabi Prehranskih Dopolnil 2010. Available online: http://mz.arhiv-spletisc.gov.si/fileadmin/mz.gov.si/pageuploads/zakonodaja/mednarodna_zakonodaja/VARNOST_%C5%BDIVIL/PARSIFAL-porocilo_raziskave.pdf (accessed on 11 April 2023).
- Knapik, J.J.; Steelman, R.A.; Hoedebecke, S.S.; Farina, E.K.; Austin, K.G.; Lieberman, H.R. A systematic review and meta-analysis on the prevalence of dietary supplement use by military personnel. BMC Complement. Altern. Med. 2014, 14, 143. [Google Scholar] [CrossRef]
- Lieberman, H.R.; Stavinoha, T.B.; McGraw, S.M.; White, A.; Hadden, L.S.; Marriott, B.P. Use of dietary supplements among active-duty US Army soldiers. Am. J. Clin. Nutr. 2010, 92, 985–995. [Google Scholar] [CrossRef]
- Casey, A.; Hughes, J.; Izard, R.M.; Greeves, J.P. Supplement use by UK-based British Army soldiers in training. Br. J. Nutr. 2014, 112, 1175–1184. [Google Scholar] [CrossRef] [PubMed]
- Daher, J.; Mallick, M.; El Khoury, D. Prevalence of Dietary Supplement Use among Athletes Worldwide: A Scoping Review. Nutrients 2022, 14, 4109. [Google Scholar] [CrossRef] [PubMed]
- Chmielewska, A.; Regulska-Ilow, B. Evaluation of Supplement Use in Sport Climbers at Different Climbing Levels. Nutrients 2023, 15, 100. [Google Scholar] [CrossRef]
- Ficarra, G.; Rottura, M.; Irrera, P.; Bitto, A.; Trimarchi, F.; Di Mauro, D. Use of Drugs and Dietary Supplements in University Students of Sports Science: Results of a Survey-Based Cross-Sectional Study. Nutrients 2022, 14, 4267. [Google Scholar] [CrossRef] [PubMed]
- Austin, K.G.; Price, L.L.; McGraw, S.M.; McLellan, T.M.; Lieberman, H.R. Longitudinal trends in use of dietary supplements by U.S. Army personnel differ from those of civilians. Appl. Physiol. Nutr. Metab. 2016, 41, 1217–1224. [Google Scholar] [CrossRef]
- Ministrstvo za Obrambo RS. Prehranska Priporočila za Slovensko Vojsko; MORS: Ljubljana, Slovenia, 2017; pp. 1–12. [Google Scholar]
- Pograjc, L.; Stibilj, V.; Ščančar, J.; Jamnik, M. Determination of macronutrients and some essential elements in the slovene military diet. Food Chem. 2010, 122, 1235–1240. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Military Nutrition Research: Not Eating Enough: Overcoming Underconsumption of Military Operational Rations—Overview of Dietary Intakes during Military Exercises. 1995. Available online: https://www.ncbi.nlm.nih.gov/books/NBK232462/ (accessed on 6 January 2023).
- EFSA. Food Supplements. 2020. Available online: https://www.efsa.europa.eu/en/topics/topic/food-supplements (accessed on 20 January 2020).
- EC. Directive 2002/46/EC on the Approximation of the Laws of the Member States Relating to Food Supplements. 2002. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32002L0046 (accessed on 15 February 2021).
- Jovanov, P.; Sakač, M.; Jurdana, M.; Pražnikar, Z.J.; Kenig, S.; Hadnađev, M.; Jakus, T.; Petelin, A.; Škrobot, D.; Marić, A. High-Protein Bar as a Meal Replacement in Elite Sports Nutrition: A Pilot Study. Foods 2021, 10, 2628. [Google Scholar] [CrossRef]
- Duchan, E.; Patel, N.D.; Feucht, C. Energy Drinks: A Review of Use and Safety for Athletes. Physician Sportsmed. 2010, 38, 171–179. [Google Scholar] [CrossRef]
- Caldwell, J.A.; McGraw, S.M.; Thompson, L.A.; Lieberman, H.R. A Survey Instrument to Assess Intake of Dietary Supplements, Related Products, and Caffeine in High-Use Populations. J. Nutr. 2018, 148, 1445S–1451S. [Google Scholar] [CrossRef]
- van der Pols, J.C.; Kanesarajah, J.; Bell, A.; Lui, C.W. Current dietary supplement use of Australian military veterans of Middle East operations. Public Health Nutr. 2017, 20, 3156–3165. [Google Scholar] [CrossRef]
- Sammito, S.; Erley, O.M.; Rose, D.-M.; Güttler, N. The Prevalence of Dietary Supplement Usage in Military Aviators. Int. J. Environ. Res. Public Health 2022, 19, 5017. [Google Scholar] [CrossRef]
- MORS, Navodilo za Preverjanje Gibalnih Sposobnosti Vojaških oseb v Slovenski Vojski in MORS. 2020. Available online: https://www.slovenskavojska.si/fileadmin/user_upload/Dokumenti/Karierne_poti/2_Program_in_kriteriji_selekcije_2020.pdf (accessed on 11 April 2023).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Kotnik, K.Z.; Jurak, G.; Starc, G.; Golja, P. Faster, Stronger, Healthier: Adolescent-Stated Reasons for Dietary Supplementation. J. Nutr. Educ. Behav. 2017, 49, 817–826. [Google Scholar] [CrossRef] [PubMed]
- KOTNIK, K.Z.; Jurak, G.; Starc, G.; Puc, M.; Golja, P. Use of dietary supplements in differently physically active adolescents. J. Food Nutr. Res. 2018, 57, 231–241. [Google Scholar]
- Pravst, I.; Hribar, M.; Žmitek, K.; Blažica, B.; Koroušić Seljak, B.; Kušar, A. Branded foods databases as a tool to support nutrition research and monitoring of the food supply: Insights from the Slovenian Composition and Labelling Information System (CLAS). Front. Nutr. 2022, 8, 1077. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.E.; MacInnis, R.J.; Wattanapenpaiboon, N.; Nowson, C.A. BMI and all-cause mortality. Am. J. Clin. Nutr. 2014, 99, 875–890. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Physical Activity Terms. 2007. Available online: http://www.cdc.gov/nccdphp/dnpa/physical/terms/ (accessed on 20 January 2020).
- Wong, S.L.; Leatherdale, S.T. Association between sedentary behavior, physical activity, and obesity: Inactivity among active kids. Prev. Chronic. Dis. 2009, 6, A26. [Google Scholar]
- Wright, S.P. Adjusted P-Values for Simultaneous Inference. Biometrics 1992, 48, 1005–1013. [Google Scholar] [CrossRef]
- Knapik, J.J.; Austin, K.G.; Farina, E.K.; Lieberman, H.R. Dietary Supplement Use in a Large, Representative Sample of the US Armed Forces. J. Acad. Nutr. Diet. 2018, 118, 1370–1388. [Google Scholar] [CrossRef]
- Bovill, M.E.; Tharion, W.J.; Lieberman, H.R. Nutrition knowledge and supplement use among elite U.S. army soldiers. Mil. Med. 2003, 168, 997–1000. [Google Scholar] [CrossRef]
- Hatch, A.M.; Cole, R.E.; DiChiara, A.J.; McGraw, S.M.; Merrill, E.P.; Wright, A.O.; Lieberman, H.R.; Bukhari, A.S. Personality Traits and Occupational Demands Are Linked to Dietary Supplement Use in Soldiers: A Cross-sectional Study of Sensation Seeking Behaviors. Mil. Med. 2019, 184, e253–e262. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, A.; Blatman, J.; El-Dash, N.; Franco, J.C. Consumer usage and reasons for using dietary supplements: Report of a series of surveys. J. Am. Coll. Nutr. 2014, 33, 176–182. [Google Scholar] [CrossRef]
- Bailey, R.L.; Gahche, J.J.; Miller, P.E.; Thomas, P.R.; Dwyer, J.T. Why US Adults Use Dietary Supplements. JAMA Intern. Med. 2013, 173, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Vesela, K.; Navratilova, M.; Beranova, M. Evaluation of Consumer Behaviour on the Food Suplements Market. In Proceedings of the 15th Annual International Scientific Conference on Marketing Identity—Digital Mirrors, Slovak Acad Sci, Smolenice, Slovakia, 6–7 November 2018. [Google Scholar]
- EC. EU Register of Nutrition and Health Claims Made on Foods. 2022. Available online: https://ec.europa.eu/food/food-feed-portal/screen/health-claims/eu-register (accessed on 17 February 2022).
- Rowe, S.; Carr, A.C. Global Vitamin C Status and Prevalence of Deficiency: A Cause for Concern? Nutrients 2020, 12, 2008. [Google Scholar] [CrossRef] [PubMed]
- Hribar, M.; Benedik, E.; Gregorič, M.; Blaznik, U.; Kukec, A.; Hristov, H.; Žmitek, K.; Pravst, I. A systematic review of vitamin D status and dietary intake in various Slovenian populations. Zdr. Varst. 2022, 61, 55–72. [Google Scholar] [CrossRef] [PubMed]
- Hribar, M.; Hristov, H.; Lavriša, Ž.; Seljak, B.K.; Gregorič, M.; Blaznik, U.; Žmitek, K.; Pravst, I. Vitamin D intake in Slovenian adolescents, adults, and the elderly population. Nutrients 2021, 13, 3528. [Google Scholar] [CrossRef]
- Hribar, M.; Hristov, H.; Gregorič, M.; Blaznik, U.; Zaletel, K.; Oblak, A.; Osredkar, J.; Kušar, A.; Žmitek, K.; Rogelj, I.; et al. Nutrihealth Study: Seasonal Variation in Vitamin D Status Among the Slovenian Adult and Elderly Population. Nutrients 2020, 12, 1838. [Google Scholar] [CrossRef]
- Žmitek, K.; Hribar, M.; Lavriša, Ž.; Hristov, H.; Kušar, A.; Pravst, I. Socio-demographic and knowledge-related determinants of vitamin D supplementation in the context of the COVID-19 pandemic: Assessment of an educational intervention. Front. Nutr. 2021, 8, 648450. [Google Scholar] [CrossRef]
- Steward, C.J.; Zhou, Y.; Keane, G.; Cook, M.D.; Liu, Y.; Cullen, T. One week of magnesium supplementation lowers IL-6, muscle soreness and increases post-exercise blood glucose in response to downhill running. Eur. J. Appl. Physiol. 2019, 119, 2617–2627. [Google Scholar] [CrossRef]
- Pasiakos, S.M.; Sepowitz, J.J.; Deuster, P.A. US Military Dietary Protein Recommendations: A Simple but Often Confused Topic. J. Spec. Oper. Med. 2015, 15, 89–95. [Google Scholar] [CrossRef]
- Carbone, J.W.; Pasiakos, S.M. Dietary Protein and Muscle Mass: Translating Science to Application and Health Benefit. Nutrients 2019, 11, 1136. [Google Scholar] [CrossRef] [PubMed]
- NIJZ. Referenčne Vrednosti za Energijski Vnos ter Vnos Hranil (Engl. Reference Values for Intake of Energy and Nutrients). 2020. Available online: https://www.nijz.si/sites/www.nijz.si/files/uploaded/referencne_vrednosti_2020_3_2.pdf (accessed on 12 January 2023).
- Havenetidis, K. The use of creatine supplements in the military. J. R. Army Med. Corps 2016, 162, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Bjelica, A.; Aleksić, S.; Goločorbin-Kon, S.; Sazdanić, D.; Torović, L.; Cvejić, J. Internet Marketing of Cardioprotective Dietary Supplements. J. Altern. Complement. Med. 2020, 26, 204–211. [Google Scholar] [CrossRef]
- Lavriša, Ž.; Hristov, H.; Hribar, M.; Žmitek, K.; Kušar, A.; Seljak, B.K.; Gregorič, M.; Blaznik, U.; Gregorič, N.; Zaletel, K.; et al. Dietary Intake and Status of Vitamin B12 in Slovenian Population. Nutrients 2022, 14, 334. [Google Scholar] [CrossRef] [PubMed]
- EC. Regulation (EU) no 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the Provision of Food Information to Consumers, Amending Regulations (EC) No 1924/2006 and (EC) No 1925/2006 of the European Parliament and of the Council, and Repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004. 2011. Available online: http://data.europa.eu/eli/reg/2011/1169/2018-01-01 (accessed on 27 September 2021).
- SCF. Tolerable Upper Intake Levels for Vitamins and Minerals. 2006. Available online: https://www.efsa.europa.eu/sites/default/files/efsa_rep/blobserver_assets/ndatolerableuil.pdf (accessed on 17 February 2021).
- Crawford, C.; Teo, L.; Lafferty, L.; Drake, A.; Bingham, J.J.; Gallon, M.D.; O’Connell, M.L.; Chittum, H.K.; Arzola, S.M.; Berry, K. Caffeine to optimize cognitive function for military mission-readiness: A systematic review and recommendations for the field. Nutr. Rev. 2017, 75, 17–35. [Google Scholar] [CrossRef]
- Stephens, M.B.; Attipoe, S.; Jones, D.; Ledford, C.J.W.; Deuster, P. Energy drink and energy shot use in the military. Nutr. Rev. 2014, 72, 72–77. [Google Scholar] [CrossRef]
- Echavarria Cross, A.; Escobar Gil, T.; Jones Segura, M.; Monroy Gomez, M.C.; Restrepo Botero, M.; Rodriguez, M.I.; Cadavid Mazo, S.Y. Energy Drinks in Military Personnel. Rev. Ces Salud Publica 2018, 9, 18–35. [Google Scholar]
- Reissig, C.J.; Strain, E.C.; Griffiths, R.R. Caffeinated energy drinks—A growing problem. Drug Alcohol Depend. 2009, 99, 1–10. [Google Scholar] [CrossRef]
- Gunja, N.; Brown, J.A. Energy drinks: Health risks and toxicity. Med. J. Aust. 2012, 196, 46–49. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies. Scientific opinion on the safety of caffeine. EFSA J. 2015, 13, 4102. [Google Scholar]
- Sekhri, K.; Kaur, K. Public knowledge, use and attitude toward multivitamin supplementation: A cross-sectional study among general public. Int. J. Appl. Basic Med. Res. 2014, 4, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Guallar, E.; Stranges, S.; Mulrow, C.; Appel, L.J.; Miller, E.R. Enough is enough: Stop wasting money on vitamin and mineral supplements. Ann. Intern. Med. 2013, 159, 850–851. [Google Scholar] [CrossRef] [PubMed]
- Wheatley, V.M.; Spink, J. Defining the public health threat of dietary supplement fraud. Compr. Rev. Food Sci. Food Saf. 2013, 12, 599–613. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Participants | Use of: Any FSSP | Vitamin and Mineral FSSPs | Protein FSSPs | Energy Drinks and Caffeine FSSPs | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | n (%) | n | n (%) | Odds Ratio | n | n (%) | Odds Ratio | n | n (%) | Odds Ratio | n | n (%) | Odds Ratio | ||
| Overall | 448 | 304 | 68 | 204 | 46 | 163 | 36 | 83 | 19 | ||||||
| Age | 18–29 | 85 | 19 | 65 | 76 | 1 | 42 | 39 | 1 | 36 | 35 | 1 | 20 | 29 b | 1 |
| 30–39 | 196 | 44 | 149 | 76 | 1.30 (0.71–2.36) | 88 | 54 | 0.95 (0.55–1.65) | 77 | 32 | 1.02 (0.59–1.78) | 42 | 21 b | 0.64 (0.32–1.26) | |
| ≥40 | 167 | 37 | 90 | 54 | 1.69 (0.84–3.39) | 74 | 39 | 1.12 (0.60–2.13) | 50 | 41 | 0.75 (0.39–1.45) | 21 | 10 a | 0.39 (0.17–0.93) | |
| Sex | Male | 399 | 89 | 269 | 67 | 1 | 184 | 45 | 1 | 146 | 37 | 1 | 74 | 19 | 1 |
| Female | 49 | 11 | 35 | 71 | 0.85 (0.43–1.66) | 20 | 53 | 0.77 (0.40–1.47) | 17 | 31 | 0.88 (0.45–1.73) | 9 | 12 | 0.87 (0.37–2.03) | |
| Education | Lower secondary school | 44 | 10 | 29 | 66 | 1 | 20 | 30 | 1 | 15 | 39 | 1 | 16 | 25 b | 1 |
| Secondary school | 287 | 64 | 189 | 66 | 1.02 (0.49–2.16) | 133 | 44 | 1.10 (0.56–2.15) | 110 | 37 | 1.39 (0.69–2.82) | 49 | 17 a | 0.40 (0.18–0.84) | |
| Higher education | 117 | 26 | 86 | 74 | 0.92 (0.37–2.25) | 51 | 55 | 1.11 (0.49–2.53) | 38 | 33 | 0.93 (0.39–2.25) | 18 | 20 b | 0.51 (0.19–1.36) | |
| Rank | Private | 244 | 54 | 176 | 72 b | 1 | 121 | 44 | 1 | 100 | 32 b | 1 | 53 | 21 | 1 |
| Non-commissioned officer | 128 | 29 | 74 | 58 a | 0.38 (0.22–0.67) | 51 | 43 | 0.63 (0.37–1.06) | 35 | 43 a | 0.57 (0.33–0.99) | 21 | 13 | 1.12 (0.56–2.29) | |
| Higher ranks/Others | 76 | 17 | 54 | 71 b | 0.49 (0.22–1.07) | 32 | 54 | 0.71 (0.34–1.46) | 28 | 37 b | 1.25 (0.58–2.69) | 9 | 21 | 0.62 (0.22–1.76) | |
| Operation abroad | Yes | 229 | 51 | 141 | 62 | 1 | 95 | 36 b | 1 | 84 | 29 | 1 | 42 | 25 a | 1 |
| No | 219 | 49 | 163 | 74 | 1.06 (0.70–1.62) | 109 | 55 a | 1.47 (0.99–2.18) | 79 | 43 | 0.95 (0.63–1.43) | 41 | 11 b | 1.16 (0.69–1.95) | |
| APFT score | 3 or less | 89 | 20 | 49 | 55 | 1 | 36 | 39 b | 1 | 37 | 39 | 1 | 18 | 11 | 1 |
| 4 | 102 | 23 | 60 | 59 | 0.87 (0.46–1.64) | 44 | 40 ab | 1.36 (0.74–2.50) | 31 | 32 | 0.70 (0.37–1.32) | 22 | 18 | 1.14 (0.53–2.48) | |
| 5 | 257 | 57 | 159 | 62 | 1.15 (0.65–2.03) | 124 | 50 a | 1.75 (1.02–2.98) | 95 | 37 | 1.02 (0.59–1.75) | 43 | 21 | 0.87 (0.43–1.75) | |
| BMI | <25 | 127 | 28 | 91 | 72 | 1 | 44 | 50 | 1 | 32 | 36 | 1 | 20 | 17 | 1 |
| 25–30 | 260 | 58 | 174 | 67 | 1.36 (0.78–2.22) | 129 | 43 | 1.01 (0.61–1.68) | 103 | 35 | 1.09 (0.64–1.85) | 55 | 19 | 0.91 (0.48–1.71) | |
| >30 | 61 | 14 | 39 | 64 | 1.57 (0.74–3.36) | 31 | 48 | 1.12 (0.49–2.53) | 28 | 41 | 1.28 (0.62–2.63) | 8 | 20 | 0.44 (0.16–1.21) | |
| Physical activity | Low | 54 | 12 | 37 | 69 | 1 | 19 | 35 | 1 | 25 | 54 | 1 | 20 | 37 b | 1 |
| Moderate | 335 | 75 | 222 | 66 | 0.88 (0.47–1.67) | 155 | 46 | 1.44 (0.78–2.66) | 115 | 34 | 0.58 (0.32–1.06) | 58 | 17 a | 0.29 (0.15–0.57) | |
| High | 59 | 13 | 45 | 76 | 1.33 (0.56–3.18) | 30 | 51 | 1.51 (0.68–3.33) | 23 | 39 | 0.66 (0.30–1.46) | 5 | 8 a | 0.13 (0.04–0.41) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pravst, I.; Lavriša, Ž.; Hristov, H.; Hribar, M.; Krušič, S.; Žmitek, K.; Kušar, A.; Zdešar Kotnik, K.; Golja, P.; Čibej Andlovec, A.; et al. Assessment of the Use of Food Supplements by Military Personnel: Study Protocol and Results. Nutrients 2023, 15, 1902. https://doi.org/10.3390/nu15081902
Pravst I, Lavriša Ž, Hristov H, Hribar M, Krušič S, Žmitek K, Kušar A, Zdešar Kotnik K, Golja P, Čibej Andlovec A, et al. Assessment of the Use of Food Supplements by Military Personnel: Study Protocol and Results. Nutrients. 2023; 15(8):1902. https://doi.org/10.3390/nu15081902
Chicago/Turabian StylePravst, Igor, Živa Lavriša, Hristo Hristov, Maša Hribar, Sanja Krušič, Katja Žmitek, Anita Kušar, Katja Zdešar Kotnik, Petra Golja, Anja Čibej Andlovec, and et al. 2023. "Assessment of the Use of Food Supplements by Military Personnel: Study Protocol and Results" Nutrients 15, no. 8: 1902. https://doi.org/10.3390/nu15081902
APA StylePravst, I., Lavriša, Ž., Hristov, H., Hribar, M., Krušič, S., Žmitek, K., Kušar, A., Zdešar Kotnik, K., Golja, P., Čibej Andlovec, A., & Pograjc, L. (2023). Assessment of the Use of Food Supplements by Military Personnel: Study Protocol and Results. Nutrients, 15(8), 1902. https://doi.org/10.3390/nu15081902