
Safety and Suitability of an Infant Formula Manufactured from Extensively Hydrolysed Protein in Healthy Term Infants
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Product
2.3. Anthropometric Measurements
2.4. Infant Formula Intake
2.5. Overall Health and Adverse Events
2.6. Statistical Analysis
2.7. Compliance
3. Results
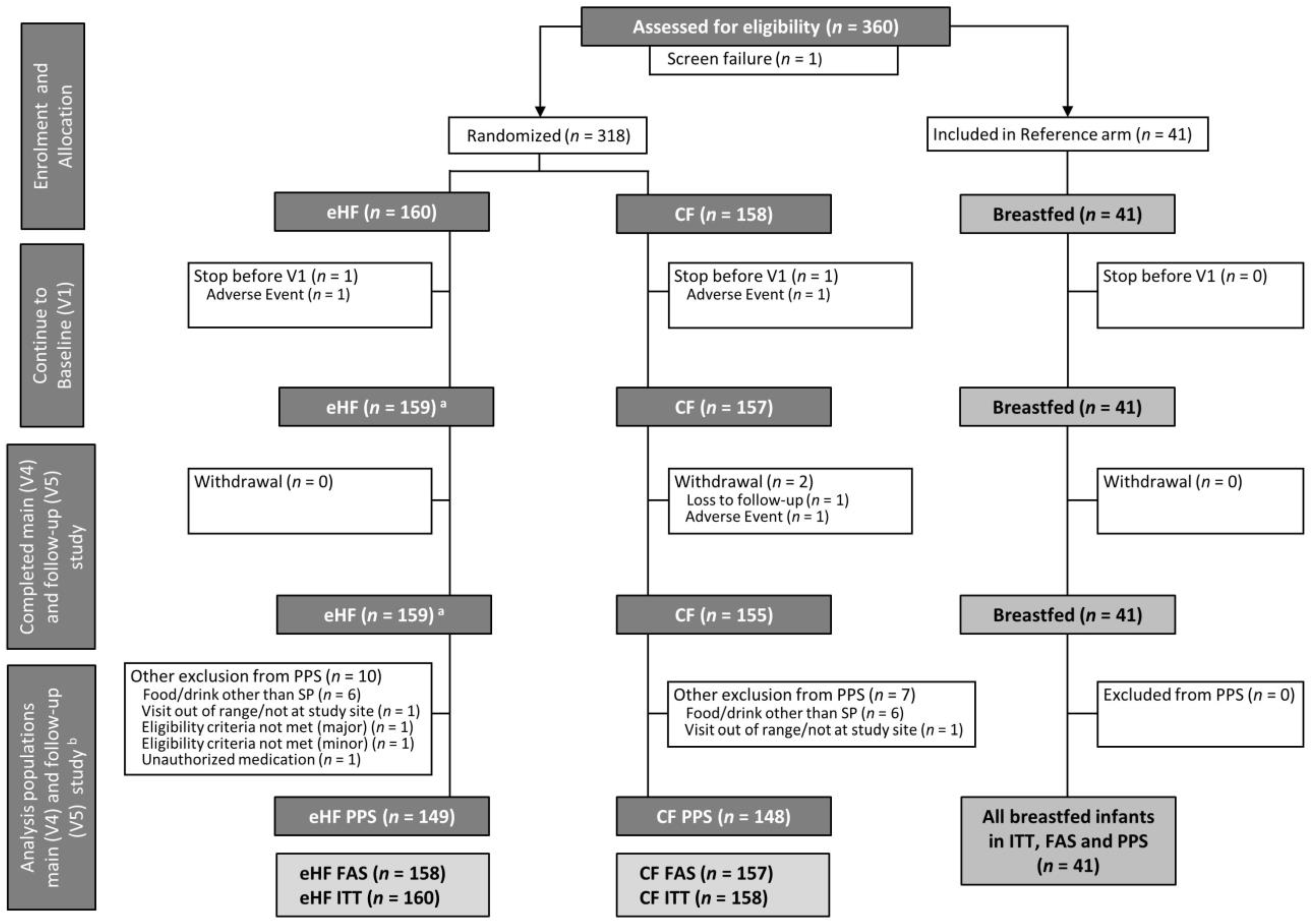
3.1. Study Participants
3.2. Study Population Characteristics
3.3. Primary Outcome: Weight Gain up to V4
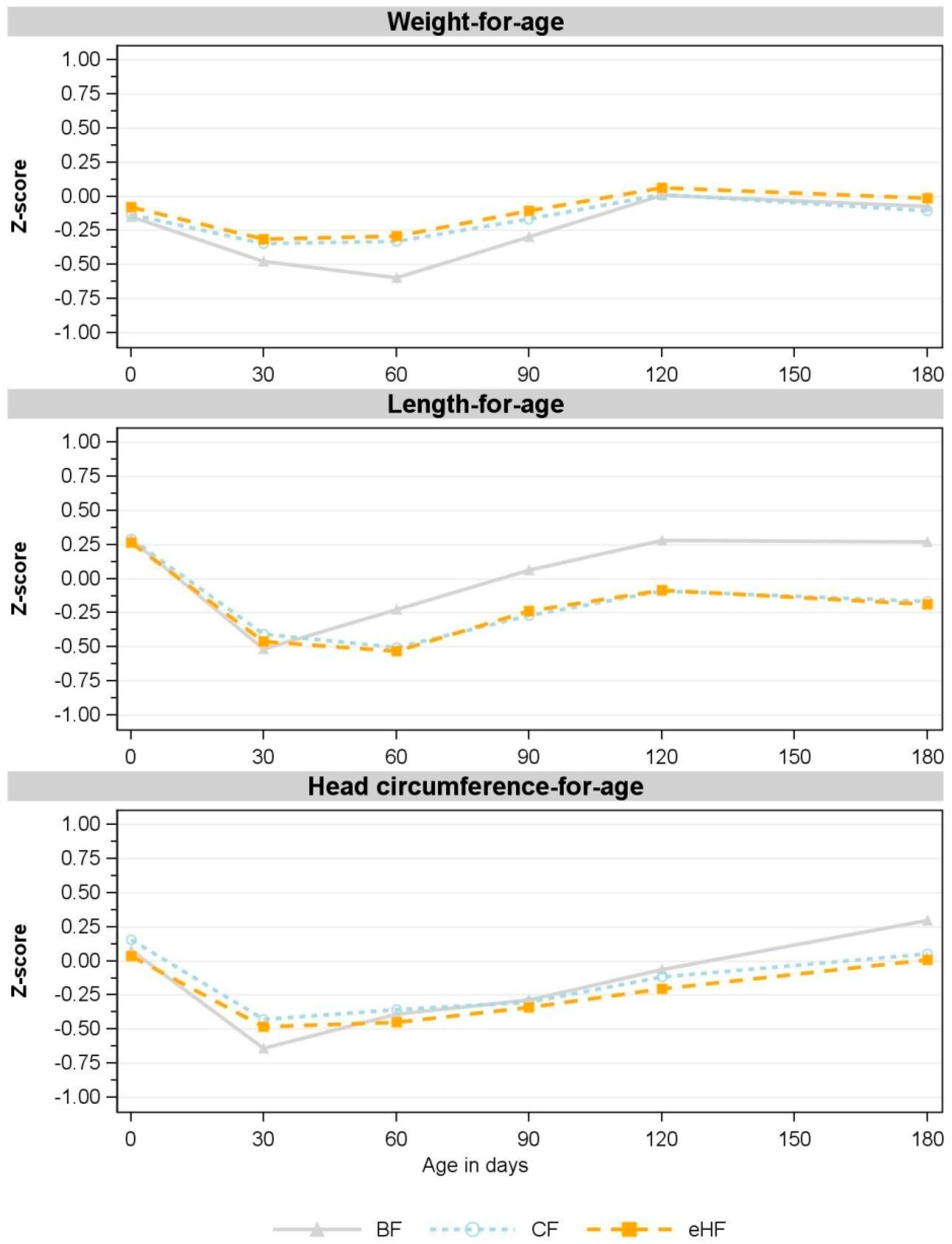
3.4. Secondary Parameters: Further Growth Parameters
3.5. Infant Formula Intake
3.6. Adverse Events Assessment
3.7. Influence of the Coronavirus Pandemic
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koletzko, B.; Godfrey, K.M.; Poston, L.; Szajewska, H.; van Goudoever, J.B.; de Waard, M.; Brands, B.; Grivell, R.M.; Deussen, A.R.; Dodd, J.M.; et al. Nutrition During Pregnancy, Lactation and Early Childhood and Its Implications for Maternal and Long-Term Child Health: The Early Nutrition Project Recommendations. Ann. Nutr. Metab. 2019, 74, 93–106. [Google Scholar] [CrossRef]
- Martin, C.R.; Ling, P.-R.; Blackburn, G.L. Review of Infant Feeding: Key Features of Breast Milk and Infant Formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef]
- Oddy, W.H. The Impact of Breastmilk on Infant and Child Health. Breastfeed. Rev. Prof. Publ. Nurs. Mothers Assoc. Aust. 2002, 10, 5–18. [Google Scholar]
- Eidelman, A.I.; Schanler, R.J.; Johnston, M.; Landers, S.; Noble, L.; Szucs, K.; Viehmann, L.; Section on Breastfeeding. Breastfeeding and the Use of Human Milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef]
- Binns, C.; Lee, M.; Low, W.Y. The Long-Term Public Health Benefits of Breastfeeding. Asia Pac. J. Public Health 2016, 28, 7–14. [Google Scholar] [CrossRef]
- Güngör, D.; Nadaud, P.; LaPergola, C.C.; Dreibelbis, C.; Wong, Y.P.; Terry, N.; Abrams, S.A.; Beker, L.; Jacobovits, T.; Järvinen, K.M.; et al. Infant Milk-Feeding Practices and Food Allergies, Allergic Rhinitis, Atopic Dermatitis, and Asthma throughout the Life Span: A Systematic Review. Am. J. Clin. Nutr. 2019, 109, 772S–799S. [Google Scholar] [CrossRef]
- Mayer-Davis, E.J.; Rifas-Shiman, S.L.; Zhou, L.; Hu, F.B.; Colditz, G.A.; Gillman, M.W. Breast-Feeding and Risk for Childhood Obesity. Diabetes Care 2006, 29, 2231–2237. [Google Scholar] [CrossRef]
- Munblit, D.; Verhasselt, V. Allergy Prevention by Breastfeeding: Possible Mechanisms and Evidence from Human Cohorts. Curr. Opin. Allergy Clin. Immunol. 2016, 16, 427–433. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st Century: Epidemiology, Mechanisms, and Lifelong Effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Qiu, R.; Zhong, Y.; Hu, M.; Wu, B. Breastfeeding and Reduced Risk of Breast Cancer: A Systematic Review and Meta-Analysis. Comput. Math. Methods Med. 2022, 2022, 8500910. [Google Scholar] [CrossRef]
- Horta, B.L.; de Lima, N.P. Breastfeeding and Type 2 Diabetes: Systematic Review and Meta-Analysis. Curr. Diabetes Rep. 2019, 19, 1. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Nutrient Requirements and Dietary Intakes of Infants and Young Children in the European Union. EFSA J. 2013, 11, 3408. [Google Scholar] [CrossRef]
- Halken, S.; Muraro, A.; de Silva, D.; Khaleva, E.; Angier, E.; Arasi, S.; Arshad, H.; Bahnson, H.T.; Beyer, K.; Boyle, R.; et al. EAACI Guideline: Preventing the Development of Food Allergy in Infants and Young Children (2020 Update). Pediatr. Allergy Immunol. 2021, 32, 843–858. [Google Scholar] [CrossRef]
- Schäfer, T.; Bauer, C.-P.; Beyer, K.; Bufe, A.; Friedrichs, F.; Gieler, U.; Gronke, G.; Hamelmann, E.; Hellermann, M.; Kleinheinz, A.; et al. S3-Guideline on Allergy Prevention: 2014 Update. Allergo J. Int. 2014, 23, 186–199. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Latiff, A.H.A.; Fleischer, D.M.; Gutiérrez-Castrellón, P.; Miqdady, M.-I.S.; Smith, P.K.; von Berg, A.; Greenhawt, M.J. Partially Hydrolyzed Formula in Non-Exclusively Breastfed Infants: A Systematic Review and Expert Consensus. Nutrition 2019, 57, 268–274. [Google Scholar] [CrossRef]
- Prell, C.; Bührer, C.; Jochum, F.; Kauth, T.; Körner, A.; Koletzko, B.; Mihatsch, W.; Reinehr, T.; Rudloff, S.; Zimmer, K.-P.; et al. Infant nutrition based on protein hydrolysates for risk reduction of allergic manifestations. Statement of the Nutrition Committee of the German Society for Pediatric and Adolescent Medicine (DGKJ). Mon. Kinderheilkd. 2019, 167, 246–250. [Google Scholar] [CrossRef]
- Karaglani, E.; Thijs-Verhoeven, I.; Gros, M.; Chairistanidou, C.; Zervas, G.; Filoilia, C.; Kampani, T.-M.; Miligkos, V.; Matiatou, M.; Valaveri, S.; et al. A Partially Hydrolyzed Whey Infant Formula Supports Appropriate Growth: A Randomized Controlled Non-Inferiority Trial. Nutrients 2020, 12, 3056. [Google Scholar] [CrossRef]
- Picaud, J.-C.; Pajek, B.; Arciszewska, M.; Tarczón, I.; Escribano, J.; Porcel, R.; Adelt, T.; Hassink, E.; Rijnierse, A.; Abrahamse-Berkeveld, M.; et al. An Infant Formula with Partially Hydrolyzed Whey Protein Supports Adequate Growth and Is Safe and Well-Tolerated in Healthy, Term Infants: A Randomized, Double-Blind, Equivalence Trial. Nutrients 2020, 12, 2072. [Google Scholar] [CrossRef]
- Ng, D.H.C.; Embleton, N.D.; McGuire, W. Hydrolyzed Formula Compared With Standard Formula for Preterm Infants. JAMA 2018, 319, 1717. [Google Scholar] [CrossRef]
- Picaud, J.-C.; Rigo, J.; Normand, S.; Lapillonne, A.; Reygrobellet, B.; Claris, O.; Salle, B.L. Nutritional Efficacy of Preterm Formula with a Partially Hydrolyzed Protein Source: A Randomized Pilot Study. J. Pediatr. Gastroenterol. Nutr. 2001, 32, 555–561. [Google Scholar] [CrossRef]
- Szajewska, H.; Albrecht, P.; Stoińska, B.; Prochowska, A.; Gawecka, A.; Laskowska–Klita, T. Extensive and Partial Protein Hydrolysate Preterm Formulas: The Effect on Growth Rate, Protein Metabolism Indices, and Plasma Amino Acid Concentrations. J. Pediatr. Gastroenterol. Nutr. 2001, 32, 303–309. [Google Scholar] [CrossRef]
- European Commission Directive 2006/141/EC on Infant Formulae and Follow-on Formulae; 30.12.2006. Off. J. Eur. Union 2006, L 401, 1–33. Available online: http://data.europa.eu/eli/dir/2006/141/oj (accessed on 13 December 2021).
- The European Union. European Commission Delegated Regulation (EU) 2016/127 of 25 September 2015 Supplementing Regulation (EU) No 609/2013 of the European Parliament and of the Council as Regards the Specific Compositional and Information Requirements for Infant Formula and Follow-on Formula and as Regards Requirements on Information Relating to Infant and Young Child Feeding. Off. J. Eur. Union 2016, L 59, 1–29. Available online: http://data.europa.eu/eli/reg_del/2016/127/oj (accessed on 14 March 2023).
- Turck, D.; Bresson, J.; Burlingame, B.; Dean, T.; Fairweather-Tait, S.; Heinonen, M.; Hirsch-Ernst, K.I.; Mangelsdorf, I.; McArdle, H.J.; Naska, A.; et al. Scientific and Technical Guidance for the Preparation and Presentation of an Application for Authorisation of an Infant and/or Follow-on Formula Manufactured from Protein Hydrolysates. EFSA J. 2017, 15, e04779. [Google Scholar] [CrossRef]
- EFSA. Explanatory Note to the Scientific and Technical Guidance for the Preparation and Presentation of an Application for Authorisation of an Infant and/or Follow-on Formula Manufactured from Protein Hydrolysates (with a View to Amend Regulation (EU) 2016/127). EFSA Support. Publ. 2020, 17, 1858E. [Google Scholar] [CrossRef]
- American Academy of Pediatrics; Committee on Nutrition Task Force. Clinical Testing of Infant Formulas with Respect to Nutritional Suitability for Term Infants. Available online: https://wayback.archive-it.org/7993/20170722090324/https://www.fda.gov/Food/GuidanceRegulation/GuidanceDocumentsRegulatoryInformation/InfantFormula/ucm170649.htm (accessed on 26 April 2022).
- Voigt, M.; Rochow, N.; Schneider, K.T.M.; Hagenah, H.-P.; Scholz, R.; Hesse, V.; Wittwer-Backofen, U.; Straube, S.; Olbertz, D. New Percentile Values for the Anthropometric Dimensions of Singleton Neonates: Analysis of Perinatal Survey Data of 2007–2011 from all 16 States of Germany. Z. Geburtshilfe Neonatol. 2014, 218, 210–217. [Google Scholar] [CrossRef]
- WHO. Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development. World Health Organization. Available online: https://www.who.int/tools/child-growth-standards/standards (accessed on 17 March 2022).
- Ahrens, B.; Hellmuth, C.; Haiden, N.; Olbertz, D.; Hamelmann, E.; Vusurovic, M.; Fleddermann, M.; Roehle, R.; Knoll, A.; Koletzko, B.; et al. Hydrolyzed Formula with Reduced Protein Content Supports Adequate Growth: A Randomized Controlled Noninferiority Trial. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 822–830. [Google Scholar] [CrossRef]
- Fleddermann, M.; Demmelmair, H.; Grote, V.; Nikolic, T.; Trisic, B.; Koletzko, B. Infant Formula Composition Affects Energetic Efficiency for Growth: The BeMIM Study, a Randomized Controlled Trial. Clin. Nutr. 2014, 33, 588–595. [Google Scholar] [CrossRef]
- Troesch, B.; Demmelmair, J.; Gimpfl, M.; Hecht, C.; Lakovic, G.; Roehle, R.; Sipka, L.; Trisic, B.; Vusurovic, M.; Schoop, R.; et al. Suitability and Safety of L-5-Methyltetrahydrofolate as a Folate Source in Infant Formula: A Randomized-Controlled Trial. PLoS ONE 2019, 14, e0216790. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- WHO. Anthro Survey Analyser and Other Tools. Available online: https://www.who.int/tools/child-growth-standards/software (accessed on 19 January 2023).
- Rigo, J.; Schoen, S.; Verghote, M.; van Overmeire, B.; Marion, W.; Abrahamse-Berkeveld, M.; Alliet, P. Partially Hydrolysed Whey-Based Formulae with Reduced Protein Content Support Adequate Infant Growth and Are Well Tolerated: Results of a Randomised Controlled Trial in Healthy Term Infants. Nutrients 2019, 11, 1654. [Google Scholar] [CrossRef]
- Czerkies, L.A.; Kineman, B.D.; Cohen, S.S.; Reichert, H.; Carvalho, R.S. A Pooled Analysis of Growth and Tolerance of Infants Exclusively Fed Partially Hydrolyzed Whey or Intact Protein-Based Infant Formulas. Int. J. Pediatr. 2018, 2018, 4969576. [Google Scholar] [CrossRef]
- Baker, J.L.; Michaelsen, K.F.; Rasmussen, K.M.; Sørensen, T.I. Maternal Prepregnant Body Mass Index, Duration of Breastfeeding, and Timing of Complementary Food Introduction Are Associated with Infant Weight Gain. Am. J. Clin. Nutr. 2004, 80, 1579–1588. [Google Scholar] [CrossRef] [PubMed]
- Karlberg, J.; Albertsson-Wikland, K.; Baber, F.M.; Low, L.C.; Yeung, C.Y. Born Small for Gestational Age: Consequences for Growth. Acta Paediatr. 1996, 85, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.K.L.; Preece, M.A.; Emmett, P.M.; Ahmed, M.L.; Dunger, D.B.; ALSPAC Study Team. Size at Birth and Early Childhood Growth in Relation to Maternal Smoking, Parity and Infant Breast-Feeding: Longitudinal Birth Cohort Study and Analysis. Pediatr. Res. 2002, 52, 863–867. [Google Scholar] [CrossRef]
- Itabashi, K.; Mishina, J.; Tada, H.; Sakurai, M.; Nanri, Y.; Hirohata, Y. Longitudinal Follow-up of Height up to Five Years of Age in Infants Born Preterm Small for Gestational Age; Comparison to Full-Term Small for Gestational Age Infants. Early Hum. Dev. 2007, 83, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.; Bergström, A.; Charles, M.-A.; Chatzi, L.; Chevrier, C.; Chrousos, G.; et al. Impact of Maternal Body Mass Index and Gestational Weight Gain on Pregnancy Complications: An Individual Participant Data Meta-Analysis of European, North American and Australian Cohorts. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 984–995. [Google Scholar] [CrossRef]
- Villar, J.; Ismail, L.C.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International Standards for Newborn Weight, Length, and Head Circumference by Gestational Age and Sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- EFSA. Application of Systematic Review Methodology to Food and Feed Safety Assessments to Support Decision Making. EFSA J. 2010, 8, 1637. [Google Scholar] [CrossRef]
- EMA/CHMP/295050/2013; Guideline on Adjustment for Baseline Covariates in Clinical Trials. 26 February 2015. Committee for Medicinal Products for Human Use (CHMP): Amsterdam, The Netherlands, 2015.
- Adams, C.B.; Johnston, W.H.; Deulofeut, H.; Leader, J.; Rhodes, R.; Yeiser, M.; Harris, C.L.; Wampler, J.L.; Hill, R.J.; Cooper, T. Growth and Tolerance of Healthy, Term Infants Fed Lower Protein Extensively Hydrolyzed or Amino Acid-Based Formula: Double-Blind, Randomized, Controlled Trial. BMC Pediatr. 2021, 21, 323. [Google Scholar] [CrossRef]
- EFSA. Scientific Opinion on the Essential Composition of Infant and Follow-On Formulae. EFSA J. 2014, 12, 3760. [Google Scholar] [CrossRef]
- Kouwenhoven, S.M.P.; Antl, N.; Finken, M.J.J.; Twisk, J.W.R.; van der Beek, E.M.; Abrahamse-Berkeveld, M.; van de Heijning, B.J.M.; Schierbeek, H.; Holdt, L.M.; van Goudoever, J.B.; et al. A Modified Low-Protein Infant Formula Supports Adequate Growth in Healthy, Term Infants: A Randomized, Double-Blind, Equivalence Trial. Am. J. Clin. Nutr. 2020, 111, 962–974. [Google Scholar] [CrossRef]
- Petersen, H.; Nomayo, A.; Zelenka, R.; Foster, J.; Tvrdík, J.; Jochum, F. Adequacy and Safety of α-Lactalbumin–Enriched Low-Protein Infant Formula: A Randomized Controlled Trial. Nutrition 2020, 74, 110728. [Google Scholar] [CrossRef] [PubMed]
- Escribano, J.; Luque, V.; Ferre, N.; Mendez-Riera, G.; Koletzko, B.; Grote, V.; Demmelmair, H.; Bluck, L.; Wright, A.; Closa-Monasterolo, R. Effect of Protein Intake and Weight Gain Velocity on Body Fat Mass at 6 Months of Age: The EU Childhood Obesity Programme. Int. J. Obes. 2012, 36, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Hester, S.N.; Hustead, D.S.; Mackey, A.D.; Singhal, A.; Marriage, B.J. Is the Macronutrient Intake of Formula-Fed Infants Greater Than Breast-Fed Infants in Early Infancy? J. Nutr. Metab. 2012, 2012, 891201. [Google Scholar] [CrossRef] [PubMed]
- Rios-Leyvraz, M.; Yao, Q. The Volume of Breast Milk Intake in Infants and Young Children: A Systematic Review and Meta-Analysis. Breastfeed. Med. 2023, 18, bfm.2022.0281. [Google Scholar] [CrossRef]
- Patro-Goab, B.; Zalewski, B.; Kouwenhoven, S.; Karaś, J.; Koletzko, B.; Goudoever, J.; Szajewska, H. Protein Concentration in Milk Formula, Growth, and Later Risk of Obesity: A Systematic Review. J. Nutr. 2016, 146, 551–564. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Nutrients | eHF | CF | ||
|---|---|---|---|---|
| Per 100 kcal | Per 100 mL Ready to Drink a | Per 100 kcal | Per 100 mL Ready to Drink a | |
| Energy (kJ) | 275 | 276 | ||
| (kcal) | 100 | 66 | 100 | 66 |
| Protein (g) | 1.9 | 1.2 | 1.9 | 1.3 |
| Carbohydrates (g) | 10.8 | 7.1 | 10.6 | 7.0 |
| Fat (g) | 5.4 | 3.5 | 5.4 | 3.6 |
| Variable | eHF (n = 158) | CF (n = 157) | BF (n = 41) |
|---|---|---|---|
| Sex, female (n (%)) | 69 (43.7) | 69 (43.9) | 23 (56.1) |
| Gestational age (weeks, mean (SD)) | 38.8 (1.0) | 39.0 (1.0) | 38.6 (1.1) |
| Mode of birth | |||
| Caesarian section, n (%) | 92 (58.2) | 92 (58.6) | 17 (41.5) |
| Vaginal birth, n (%) | 66 (41.8) | 65 (41.4) | 24 (58.5) |
| Weight at birth (g, mean (SD)) | 3275 (389) | 3251 (424) | 3233 (452) |
| Length at birth (cm, mean (SD)) | 50.0 (1.6) | 49.9 (1.7) | 50.0 (2.0) |
| Head circumference at birth (cm, mean (SD)) | 34.3 (1.2) | 34.4 (1.2) | 34.2 (1.4) |
| Maternal age at delivery (years, mean (SD)) | 28.1 (5.6) | 27.4 (5.4) | 27.9 (5.7) |
| Maternal BMI before pregnancy (kg/m2, mean (SD)) | 21.7 (2.7) | 21.7 (4.0) | 21.2 (2.1) |
| Maternal weight gain during pregnancy (kg, mean (SD)) | 15.9 (6.6) | 14.7 (5.2) | 15.3 (5.3) |
| Level of education mother | |||
| Primary, n (%) | 27 (17.1) | 36 (22.9) | 6 (14.6) |
| Secondary, n (%) | 92 (58.2) | 83 (52.9) | 26 (63.4) |
| Tertiary, n (%) | 39 (24.7) | 38 (24.2) | 9 (22.0) |
| Variable | Visit | Age at Visit (Days) | eHF (n = 158) a | CF (n = 157) b | BF (n = 41) c |
|---|---|---|---|---|---|
| Weight (g) | 1 | 30 | 4169 (444) | 4155 (500) | 4047 (497) |
| 2 | 60 | 5178 (493) | 5155 (530) | 4928 (518) | |
| 3 | 90 | 6058 (550) | 6011 (530) | 5855 (533) | |
| 4 | 120 | 6791 (586) | 6744 (536) | 6675 (570) | |
| 5 | 180 | 7650 (747) | 7551 (605) | 7509 (635) | |
| Length (cm) | 1 | 30 | 53.3 (2.0) | 53.4 (2.1) | 53.1 (2.4) |
| 2 | 60 | 56.7 (2.4) | 56.7 (2.5) | 57.1 (2.7) | |
| 3 | 90 | 60.1 (3.0) | 60.1 (3.0) | 60.5 (3.3) | |
| 4 | 120 | 62.8 (3.1) | 62.8 (3.3) | 63.4 (3.5) | |
| 5 | 180 | 66.3 (3.8) | 66.3 (3.9) | 67.0 (4.6) | |
| Head circumference (cm) | 1 | 30 | 36.4 (1.3) | 36.4 (1.3) | 36.1 (1.5) |
| 2 | 60 | 38.2 (1.4) | 38.3 (1.4) | 38.1 (1.3) | |
| 3 | 90 | 39.6 (1.4) | 39.7 (1.4) | 39.6 (1.2) | |
| 4 | 120 | 40.9 (1.4) | 41.0 (1.4) | 40.9 (1.3) | |
| 5 | 180 | 42.8 (1.5) | 42.8 (1.6) | 43.0 (1.4) |
| Visit | Age at Visit (Days) | eHF (n = 158) | CF (n = 157) a | BF (n = 41) | |
|---|---|---|---|---|---|
| Average number of feedings per day b | 1 | 30 | 7.1 (0.9) | 7.0 (0.8) | 7.4 (0.6) |
| 2 | 60 | 6.1 (0.5) | 6.1 (0.5) | 6.6 (0.5) | |
| 3 | 90 | 5.8 (0.6) | 5.7 (0.5) | 5.8 (0.5) | |
| 4 | 120 | 5.7 (0.7) | 5.6 (0.6) | 5.5 (0.5) | |
| 5 | 180 | 4.7 (0.7) | 4.6 (0.7) | 4.5 (0.6) | |
| Average amount of study product per day (mL/day) | 1 | 30 | 738.0 (128.9) | 743.7 (125.3) | - |
| 2 | 60 | 777.8 (92.1) | 778.0 (91.4) | - | |
| 3 | 90 | 815.4 (68.0) c | 797.3 (64.0) | - | |
| 4 | 120 | 858.2 (83.8) | 844.9 (56.2) | - | |
| 5 | 180 | 842.8 (116.7) | 837.7 (121.1) | - | |
| Average energy intake from study product (kcal/day). | 1 | 30 | 487.1 (85.1) | 490.8 (82.7) | - |
| 2 | 60 | 513.3 (60.8) | 513.5 (60.4) | - | |
| 3 | 90 | 538.2 (44.9) c | 526.2 (42.2) | - | |
| 4 | 120 | 566.4 (55.3) | 557.7 (37.1) | - | |
| 5 | 180 | 556.2 (77.1) | 552.9 (79.9) | - |
| eHF (n = 160) | CF (n = 158) | BF (n = 41) | ||||
|---|---|---|---|---|---|---|
| Infants n (%) | Events n | Infants n (%) | Events n | Infants n (%) | Events n | |
| All adverse events | 10 (6.3) | 10 | 6 (3.8) | 7 | 0 (0.0) | 0 |
| All serious adverse events | 0 (0.0) | 0 | 1 (0.6) | 1 | 0 (0.0) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otten, L.; Schelker, E.; Petersen, H.; Nomayo, A.; Fleddermann, M.; Arendt, B.M.; Britzl, T.; Haberl, E.M.; Jochum, F., on behalf of the HASI Study Group. Safety and Suitability of an Infant Formula Manufactured from Extensively Hydrolysed Protein in Healthy Term Infants. Nutrients 2023, 15, 1901. https://doi.org/10.3390/nu15081901
Otten L, Schelker E, Petersen H, Nomayo A, Fleddermann M, Arendt BM, Britzl T, Haberl EM, Jochum F on behalf of the HASI Study Group. Safety and Suitability of an Infant Formula Manufactured from Extensively Hydrolysed Protein in Healthy Term Infants. Nutrients. 2023; 15(8):1901. https://doi.org/10.3390/nu15081901
Chicago/Turabian StyleOtten, Lindsey, Elisabeth Schelker, Hanna Petersen, Antonia Nomayo, Manja Fleddermann, Bianca M. Arendt, Theresa Britzl, Elisabeth M. Haberl, and Frank Jochum on behalf of the HASI Study Group. 2023. "Safety and Suitability of an Infant Formula Manufactured from Extensively Hydrolysed Protein in Healthy Term Infants" Nutrients 15, no. 8: 1901. https://doi.org/10.3390/nu15081901
APA StyleOtten, L., Schelker, E., Petersen, H., Nomayo, A., Fleddermann, M., Arendt, B. M., Britzl, T., Haberl, E. M., & Jochum, F., on behalf of the HASI Study Group. (2023). Safety and Suitability of an Infant Formula Manufactured from Extensively Hydrolysed Protein in Healthy Term Infants. Nutrients, 15(8), 1901. https://doi.org/10.3390/nu15081901