

Controlling Nutritional Status (CONUT) Score as a Potential Prognostic Indicator of In-Hospital Mortality, Sepsis and Length of Stay in an Internal Medicine Department

 ,
,  ,
,  ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Lab Tests
2.3. Calculations
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics, Medical History, and Comorbidities of the Patients According to the CONUT Score
3.2. Clinical Outcomes According to the CONUT Score Groups
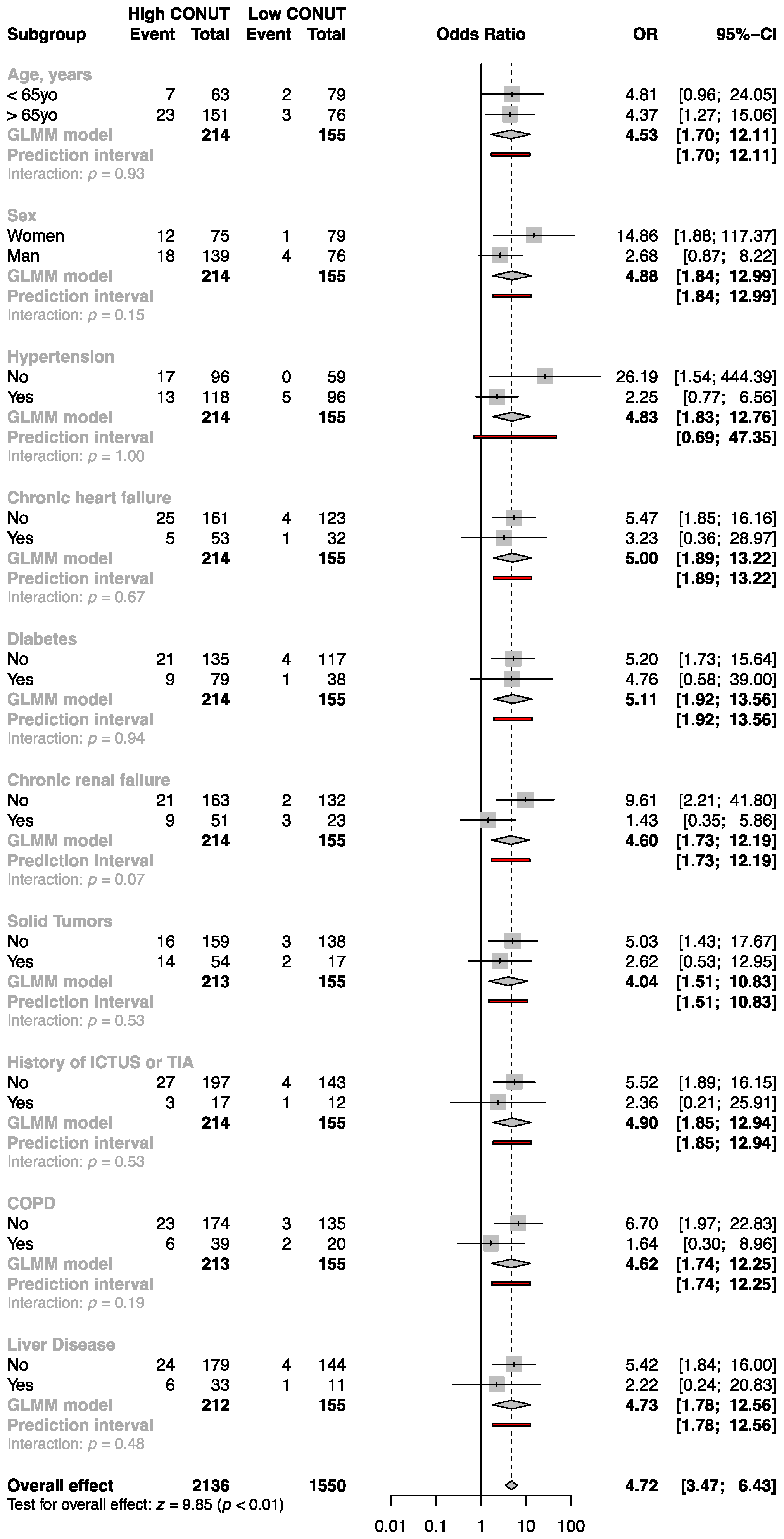
3.3. Multivariable Logistic Analysis and Subgroup Analysis for the Primary Outcome Measure; High versus Low CONUT Score Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN Guidelines on Definitions and Terminology of Clinical Nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Lim, S.L.; Ong, K.C.B.; Chan, Y.H.; Loke, W.C.; Ferguson, M.; Daniels, L. Malnutrition and Its Impact on Cost of Hospitalization, Length of Stay, Readmission and 3-Year Mortality. Clin. Nutr. 2012, 31, 345–350. [Google Scholar] [CrossRef]
- Norman, K.; Pichard, C.; Lochs, H.; Pirlich, M. Prognostic Impact of Disease-Related Malnutrition. Clin. Nutr. 2008, 27, 5–15. [Google Scholar] [CrossRef]
- Barker, L.; Gout, B.; Crowe, T. Hospital Malnutrition: Prevalence, Identification and Impact on Patients and the Healthcare System. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional Status in Older Persons According to Healthcare Setting: A Systematic Review and Meta-Analysis of Prevalence Data Using MNA®. Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef]
- Hao, R.; Qi, X.; Xia, X.; Wang, L.; Li, X. Malnutrition on Admission Increases the In-hospital Mortality and Length of Stay in Elder Adults with Acute Ischemic Stroke. Clin. Lab. Anal. 2022, 36, e24132. [Google Scholar] [CrossRef]
- Zagami, R.M.; Di Pino, A.; Urbano, F.; Piro, S.; Purrello, F.; Rabuazzo, A.M. Low Circulating Vitamin D Levels Are Associated with Increased Arterial Stiffness in Prediabetic Subjects Identified According to HbA1c. Atherosclerosis 2015, 243, 395–401. [Google Scholar] [CrossRef]
- Cereda, E.; Pedrolli, C.; Zagami, A.; Vanotti, A.; Piffer, S.; Faliva, M.; Rondanelli, M.; Caccialanza, R. Nutritional Risk, Functional Status and Mortality in Newly Institutionalised Elderly. Br. J. Nutr. 2013, 110, 1903–1909. [Google Scholar] [CrossRef] [PubMed]
- Riso, S.; Para, O.; Collo, A.; Campanini, M.; Rotunno, S.; Giorgetti, G.; Zanetti, M.; Manfellotto, D. Clinical Nutrition in Internal Medicine: An Italian Survey by the Scientific Societies FADOI and SINPE. Nutrition 2022, 98, 111623. [Google Scholar] [CrossRef] [PubMed]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.P.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A Tool for Controlling Nutritional Status. First Validation in a Hospital Population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Wada, H.; Dohi, T.; Miyauchi, K.; Doi, S.; Konishi, H.; Naito, R.; Tsuboi, S.; Ogita, M.; Kasai, T.; Okazaki, S.; et al. Prognostic Impact of Nutritional Status Assessed by the Controlling Nutritional Status Score in Patients with Stable Coronary Artery Disease Undergoing Percutaneous Coronary Intervention. Clin. Res. Cardiol. 2017, 106, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Zhao, H.; Zheng, M.; Peng, J. The Impact of Malnutrition on Atrial Fibrillation Recurrence Post Ablation. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Li, M.; Wang, T.; Ma, G.; Deng, Y.; Pu, D.; Liu, Z.; Wu, Q.; Liu, X.; Zhou, Q. Controlling Nutritional Status (CONUT) Score Is a Prognostic Factor in Patients with Resected Breast Cancer. Sci. Rep. 2020, 10, 6633. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C–Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- Barbar, S.; Noventa, F.; Rossetto, V.; Ferrari, A.; Brandolin, B.; Perlati, M.; De Bon, E.; Tormene, D.; Pagnan, A.; Prandoni, P. A Risk Assessment Model for the Identification of Hospitalized Medical Patients at Risk for Venous Thromboembolism: The Padua Prediction Score: Padua Prediction Score. J. Thromb. Haemost. 2010, 8, 2450–2457. [Google Scholar] [CrossRef]
- Marinho, R.; Pessoa, A.; Lopes, M.; Rosinhas, J.; Pinho, J.; Silveira, J.; Amado, A.; Silva, S.; Oliveira, B.M.P.M.; Marinho, A.; et al. High Prevalence of Malnutrition in Internal Medicine Wards—A Multicentre ANUMEDI Study. Eur. J. Intern. Med. 2020, 76, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Yaku, H.; Morimoto, T.; Inuzuka, Y.; Tamaki, Y.; Yamamoto, E.; Yoshikawa, Y.; Kitai, T.; Taniguchi, R.; Iguchi, M.; et al. Association with Controlling Nutritional Status (CONUT) Score and In-Hospital Mortality and Infection in Acute Heart Failure. Sci. Rep. 2020, 10, 3320. [Google Scholar] [CrossRef]
- Li, H.; Zhou, P.; Zhao, Y.; Ni, H.; Luo, X.; Li, J. Prediction of All-Cause Mortality with Malnutrition Assessed by Controlling Nutritional Status Score in Patients with Heart Failure: A Systematic Review and Meta-Analysis. Public Health Nutr. 2022, 25, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Yang, H.; Zhou, Y.; Liu, X.; Zou, C.; Ji, S.; Liang, T. Prediction of All-Cause Mortality with Malnutrition Assessed by Nutritional Screening and Assessment Tools in Patients with Heart Failure: A Systematic Review. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1361–1374. [Google Scholar] [CrossRef]
- Ma, X.; Zou, W.; Sun, Y. Prognostic Value of Pretreatment Controlling Nutritional Status Score for Patients with Pancreatic Cancer: A Meta-Analysis. Front. Oncol. 2022, 11, 770894. [Google Scholar] [CrossRef]
- Peng, L.; Meng, C.; Li, J.; You, C.; Du, Y.; Xiong, W.; Xia, Z.; Cao, D.; Li, Y. The Prognostic Significance of Controlling Nutritional Status (CONUT) Score for Surgically Treated Renal Cell Cancer and Upper Urinary Tract Urothelial Cancer: A Systematic Review and Meta-Analysis. Eur. J. Clin. Nutr. 2022, 76, 801–810. [Google Scholar] [CrossRef]
- Peng, J.; Hao, Y.; Rao, B.; Cao, Y. Prognostic Impact of the Pre-Treatment Controlling Nutritional Status Score in Patients with Non-Small Cell Lung Cancer: A Meta-Analysis. Medicine 2021, 100, 26. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Liu, H.; Pan, J.; Yu, W.; Lv, J.; Yan, J.; Gao, J.; Wang, X.; Ge, X.; Zhou, W. Preoperative Controlling Nutritional Status (CONUT) Score Predicts Short-Term Outcomes of Patients with Gastric Cancer after Laparoscopy-Assisted Radical Gastrectomy. World J. Surg. Oncol. 2021, 19, 25. [Google Scholar] [CrossRef] [PubMed]
- Akirov, A.; Masri-Iraqi, H.; Atamna, A.; Shimon, I. Low Albumin Levels Are Associated with Mortality Risk in Hospitalized Patients. Am. J. Med. 2017, 130, 1465.e11–1465.e19. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Chewcharat, A.; Mao, M.A.; Thirunavukkarasu, S.; Kashani, K.B. Impacts of Admission Serum Albumin Levels on Short-Term and Long-Term Mortality in Hospitalized Patients. QJM Int. J. Med. 2020, 113, 393–398. [Google Scholar] [CrossRef]
- Hu, Y.; Long, H.; Cao, Y.; Guo, Y. Prognostic Value of Lymphocyte Count for In-Hospital Mortality in Patients with Severe AECOPD. BMC Pulm. Med. 2022, 22, 376. [Google Scholar] [CrossRef]
- Mohammadshahi, J.; Ghobadi, H.; Matinfar, G.; Boskabady, M.H.; Aslani, M.R. Role of Lipid Profile and Its Relative Ratios (Cholesterol/HDL-C, Triglyceride/HDL-C, LDL-C/HDL-C, WBC/HDL-C, and FBG/HDL-C) on Admission Predicts In-Hospital Mortality COVID-19. J. Lipids 2023, 2023, 6329873. [Google Scholar] [CrossRef] [PubMed]
- Garwe, T.; Albrecht, R.M.; Stoner, J.A.; Mitchell, S.; Motghare, P. Hypoalbuminemia at Admission Is Associated with Increased Incidence of In-Hospital Complications in Geriatric Trauma Patients. Am. J. Surg. 2016, 212, 109–115. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lymphocyte (/mL) | Points | Total Cholesterol (mg/dL) | Points | Albumin (g/dL) | Points |
|---|---|---|---|---|---|
| <800 | 3 | <100 | 3 | <2.5 | 6 |
| 800–1200 | 2 | 100–140 | 2 | 2.5–3 | 4 |
| 1200–1600 | 1 | 140–180 | 1 | 3–3.5 | 2 |
| >1600 | 0 | >180 | 0 | >3.5 | 0 |
| CONUT Score | ||||
|---|---|---|---|---|
| Low | High | |||
| Normal (0–2) n = 45 | Mild (3–4) n = 110 | Moderate–High (5–8) n = 149 | Marked High (9–12) n = 65 | |
| Age (years) | 56.6 ± 21.1 | 64.6 ± 19.7 * | 69.1 ± 16.1 *# | 72.3 ± 9.7 *# |
| Sex (M%) | 40 | 52.7 | 61 * | 73.8 *# |
| Systolic Pressure (mmHg) | 125.3 ± 18.8 | 126.2 ± 17.6 | 126.5 ± 20.5 | 123.2 ± 20.4 |
| Diastolic Pressure (mmHg) | 70.3 ± 10.9 | 74.0 ± 12.3 | 71.6 ± 9.7 | 69.2 ± 10.5 # |
| Glycemia (mg/dL) | 95.9 ± 36.4 | 112.6 ± 56.6 | 110.1 ± 47.7 | 112.7 ± 57.2 |
| Serum Creatinine (mg/dL) | 0.7 ± 0.3 | 1.3 ± 1.8 * | 1.3 ± 1.3 * | 1.1 ± 1.2 |
| eGFR (ml/min/1.74 m2) | 94.7 ± 27.5 | 78.8 ± 33.7 * | 70.7 ± 34.4 *# | 73.8 ± 29.1 * |
| Total cholesterol (mg/dL) | 189.4 ± 35.9 | 164.4 ± 48.5 * | 137.2 ± 40.2 *# | 102.4 ± 26.3 *#@ |
| Triglycerides (mg/dL) | 134.7 ± 56.7 | 128.9 ± 65.1 | 130.2 ± 62.4 | 103.4 ± 44.5 |
| HDL-c (mg/dL) | 46.5 ± 13.7 | 37.5 ± 14.6 * | 31.6 ± 13.6 *# | 21.2 ± 9.1 *#@ |
| LDL-c (mg/dL) | 115.8 ± 34.7 | 100.2 ± 43.8 * | 80.6 ± 35.3 *# | 60.3 ± 23.6 *#@ |
| Total Proteins (g/dL) | 6.8 ± 0.5 | 6.3 ± 0.6 * | 5.8 ± 0.6 *# | 5.3 ± 0.7 *#@ |
| Albumin (g/dL) | 4.5 ± 4.0 | 3.5 ± 0.4 * | 2.9 ± 0.4 *# | 2.4 ± 0.3 *#@ |
| AST (U/L) ≥ 35 (%) | 24 | 25 | 30 | 37 |
| ALT (U/L) ≥ 56 (%) | 18 | 21 | 17 | 12 |
| NT-proBNP > 260 (pg/mL) (%) | 4.4 | 23.6 * | 22.1 * | 30.7 * |
| Procalcitonin > 0.5 (µg/L) (%) | 2.2 | 13.6 * | 27.5 *# | 30.7 *# |
| Hs-CRP (mg/dL) | 2.4 ± 3.4 | 6.1 ± 8.8 | 8.1 ± 8.1 * | 16.9 ± 22.2 *#@ |
| Padua Prediction Score | 2.2 ± 1.8 | 2.9 ± 1.8 * | 3.8 ± 1.7 *# | 4 ± 1.6 *# |
| WBC (103/μL) | 9.6 ± 6.2 | 8.9 ± 4.6 | 11.0 ± 14.7 | 8.0 ± 5.9 |
| Lymphocyte (103/μL) | 1.8 (1.6–2.8) | 1.6(1.17–2) * | 1.2(0.87–1.7) * | 0.7 (0.5–1.1) * |
| RBC (106/μL) | 4.4 ± 0.5 | 3.9 ± 0.8 | 6.5 ± 30.1 | 3.5 ± 0.8 |
| Hemoglobin (g/dL) | 13.3 ± 4.6 | 11.4 ± 2.2 * | 10.4 ± 1.8 *# | 9.7 ± 1.8 *#@ |
| Hematocrit (%) | 38.7 ± 9.5 | 34.3 ± 6.2 * | 31.4 ± 5.6 *# | 30.4 ± 8.1 *# |
| PLT (103/μL) | 253 ± 94 | 243 ± 142 | 222 ± 121 | 188 ± 122 *# |
| INR | 1.9 ± 4.4 | 2.1 ± 5.2 | 1.6 ± 4.0 | 1.3 ± 0.2 |
| CONUT Score | ||
|---|---|---|
| Low (0–4) (n = 155) | High (5–12) (n = 214) | |
| Age (years) | 62.3 ± 20.4 | 70.1 ± 14.6 |
| Sex (M%) | 49 | 65 * |
| Systolic Pressure (mmHg) | 125.9 ± 17.9 | 125.5 ± 20.6 |
| Diastolic Pressure (mmHg) | 72.9 ± 12.0 | 70.9 ± 10.0 |
| Glycemia (mg/dL) | 107.8 ± 52.1 | 110.9 ± 50.6 |
| Serum Creatinine (mg/dL) | 1.18 ± 1.6 | 1.27 ± 1.33 |
| eGFR (mL/min/1.74 m2) | 83.4 ± 32.8 | 71.6 ± 32.9 |
| Total cholesterol (mg/dL) | 171.8 ± 46.5 | 127.1 ± 39.9 * |
| Triglycerides (mg/dL) | 130.6 ± 62.7 | 122.4 ± 58.9 |
| HDL-c(mg/dL) | 40.2 ± 14.9 | 28.6 ± 13.4 * |
| LDL-c (mg/dL) | 104.8 ± 41.9 | 74.7 ± 33.6 * |
| Total Proteins (g/dL) | 6.5 ± 0.7 | 5.7 ± 0.7 * |
| Albumin (g/dL) | 3.8 ± 2.2 | 2.7 ± 0.4 * |
| AST (U/L) ≥ 35 (%) | 25 | 32 |
| ALT (U/L) ≥ 56 (%) | 20 | 15 |
| NT-proBNP > 260 (pg/mL) (%) | 18 | 24.7 |
| Procalcitonin > 0.5 (µg/L) (%) | 10.3 | 28 * |
| Hs-CRP (mg/dL) | 5.0 ± 7.8 | 10.7 ± 14.4 * |
| Padua Prediction Score | 2.7 ± 1.8 | 3.9 ± 1.7 * |
| WBC (103/μL) | 9.1 ± 5.1 | 10.0 ± 12.6 |
| Lymphocyte (103/μL) | 1.7 (1.3–2.2) | 1.0 (0.7–1.5) * |
| RBC (106/μL) | 4.1 ± 0.7 | 3.6 ± 0.8 * |
| Hemoglobin (g/dL) | 11.9 ± 3.2 | 10.2 ± 1.8 * |
| Hematocrit (%) | 35.6 ± 7.6 | 31.1 ± 6.5 * |
| PLT (103/μL) | 247 ± 130 | 211 ± 122 * 1.56 ± 3.3 |
| INR | 2.1 ± 4.9 | |
| CONUT Score | ||||
|---|---|---|---|---|
| Low | High | |||
| Normal (0–2) n = 45 | Mild (3–4) n = 110 | Moderate–High (5–8) n = 149 | Marked High (9–12) n = 65 | |
| Blood Transfusion (%) | 8.8 | 16.3 | 18.8 | 29.7 *# |
| Diabetes Mellitus (%) | 17.7 | 27.2 | 34.2 * | 45.1 *# |
| Hypertension (%) | 48.8 | 67.2 * | 61 | 44.2 #@ |
| Chronic Heart Failure (%) | 13.3 | 23.6 | 24.8 | 26.2 |
| Previous Stroke (%) | 6 | 13.5 | 10 | 12.2 |
| Chronic Kidney Failure (%) | 2.2 | 19.1 * | 24.1 * | 8.3 * |
| Neoplasm (%) | 18.1 | 14.8 | 30.5 # | 39.1 *# |
| Chronic Obstructive Pulmonary Disease (%) | 6.7 | 17.2 | 24.1 * | 25 * |
| Chronic Liver Disease (%) | 6.6 | 7.2 | 11.4 | 26.2 *#@ |
| CONUT Score | ||
|---|---|---|
| Low (0–4) n = 155 | High (5–12) n = 214 | |
| Blood Transfusion (%) | 14.2 | 22.0 * |
| Diabetes Mellitus (%) | 24.5 | 32.7 * |
| Hypertension (%) | 61.9 | 51.4 |
| Chronic Heart Failure (%) | 20.6 | 25.2 |
| Previous Stroke (%) | 11.6 | 10.7 |
| Chronic Kidney Failure (%) | 14.2 | 19.1 * |
| Neoplasm (%) | 15.6 | 32.7 * |
| Chronic Obstructive Pulmonary Disease (%) | 14.1 | 24.2 * |
| Chronic Liver Disease (%) | 7.1 | 15.9 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miano, N.; Di Marco, M.; Alaimo, S.; Coppolino, G.; L’Episcopo, G.; Leggio, S.; Scicali, R.; Piro, S.; Purrello, F.; Di Pino, A. Controlling Nutritional Status (CONUT) Score as a Potential Prognostic Indicator of In-Hospital Mortality, Sepsis and Length of Stay in an Internal Medicine Department. Nutrients 2023, 15, 1554. https://doi.org/10.3390/nu15071554
Miano N, Di Marco M, Alaimo S, Coppolino G, L’Episcopo G, Leggio S, Scicali R, Piro S, Purrello F, Di Pino A. Controlling Nutritional Status (CONUT) Score as a Potential Prognostic Indicator of In-Hospital Mortality, Sepsis and Length of Stay in an Internal Medicine Department. Nutrients. 2023; 15(7):1554. https://doi.org/10.3390/nu15071554
Chicago/Turabian StyleMiano, Nicoletta, Maurizio Di Marco, Salvatore Alaimo, Giuseppe Coppolino, Giuseppe L’Episcopo, Stefano Leggio, Roberto Scicali, Salvatore Piro, Francesco Purrello, and Antonino Di Pino. 2023. "Controlling Nutritional Status (CONUT) Score as a Potential Prognostic Indicator of In-Hospital Mortality, Sepsis and Length of Stay in an Internal Medicine Department" Nutrients 15, no. 7: 1554. https://doi.org/10.3390/nu15071554
APA StyleMiano, N., Di Marco, M., Alaimo, S., Coppolino, G., L’Episcopo, G., Leggio, S., Scicali, R., Piro, S., Purrello, F., & Di Pino, A. (2023). Controlling Nutritional Status (CONUT) Score as a Potential Prognostic Indicator of In-Hospital Mortality, Sepsis and Length of Stay in an Internal Medicine Department. Nutrients, 15(7), 1554. https://doi.org/10.3390/nu15071554