
Effects of Protein Supplementation Combined with Resistance Exercise Training on Walking Speed Recovery in Older Adults with Knee Osteoarthritis and Sarcopenia

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
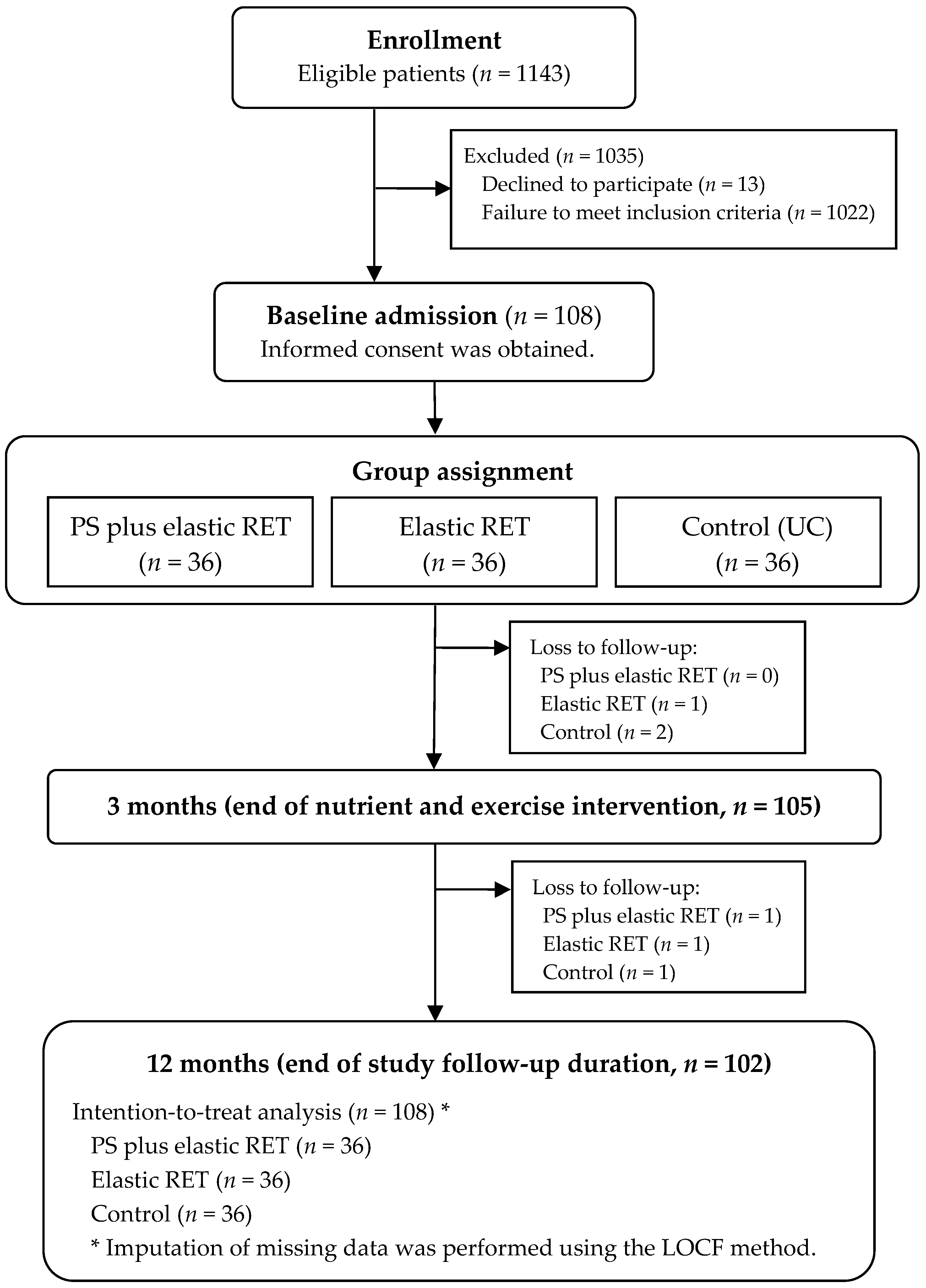
2.1. Study Design
2.2. Participants
2.3. Identification of Sarcopenia
2.4. Resistance Exercise Training
2.5. Assessment of Protein Intake and Dietary Protein Supplementation
2.6. Usual Care
2.7. Identification of Successful Recovery from Slow Walking Speed
2.8. Statistical Analysis
3. Results
3.1. Patient Demographics and Clinical Characteristics
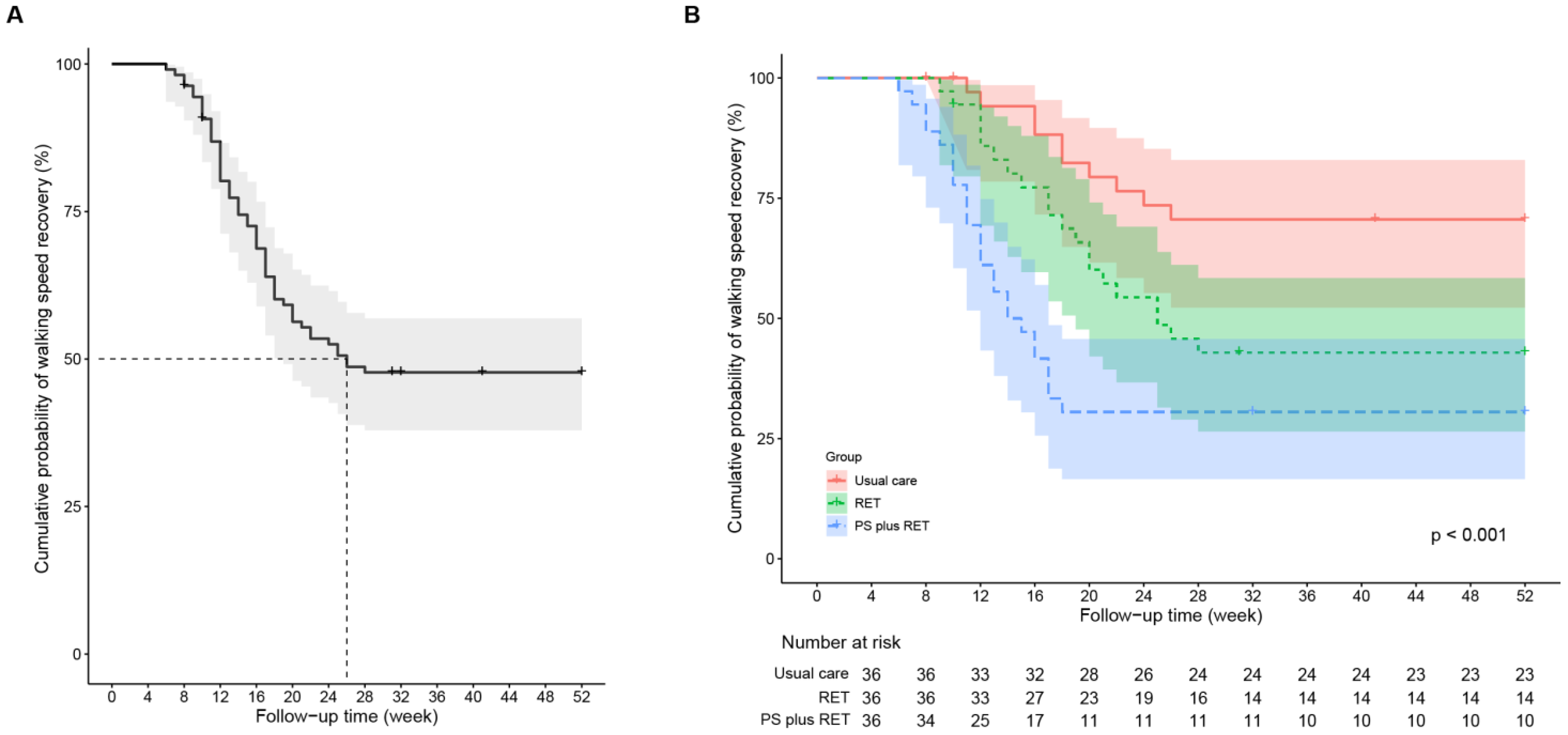
3.2. Intervention Effects on Walking Speed
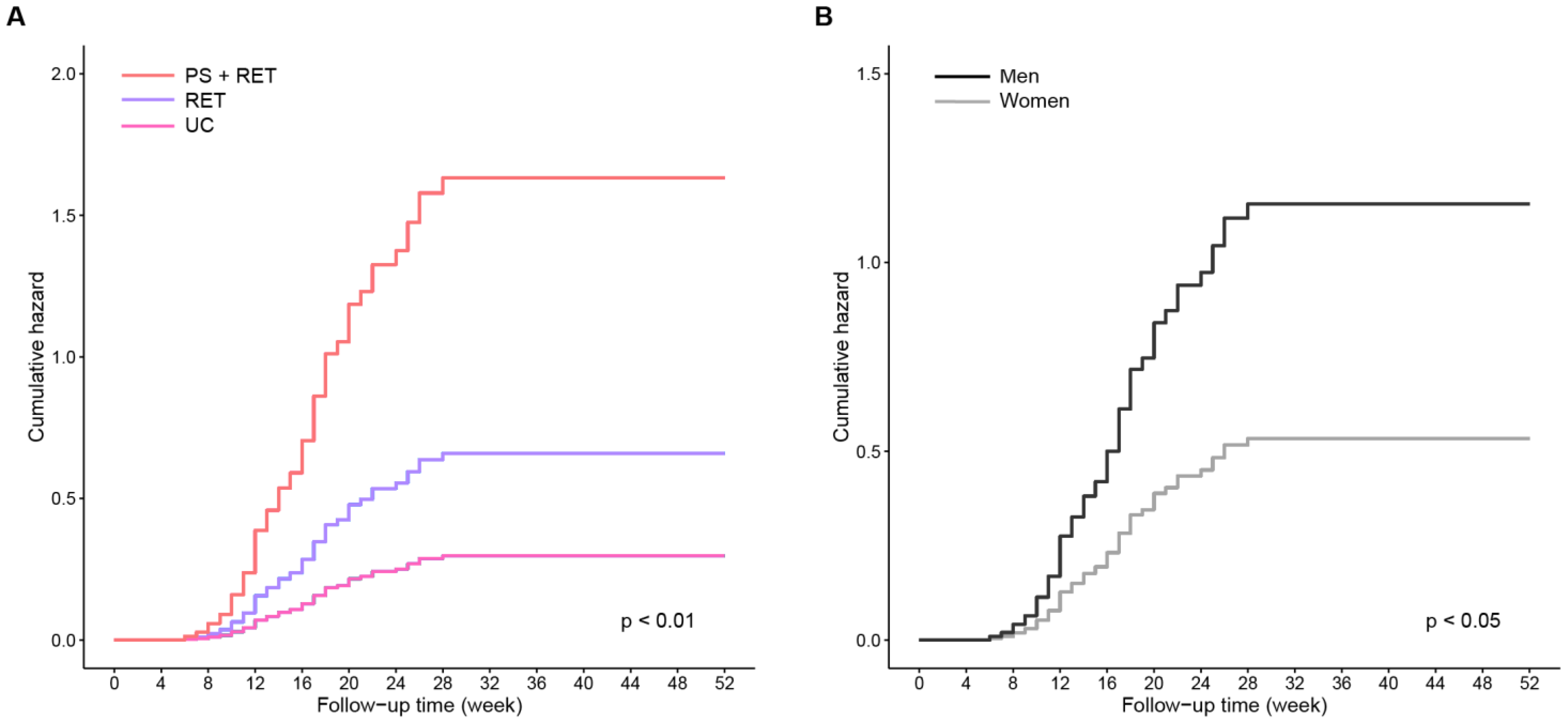
3.3. Survival Time for Recovery from Slow Walking Speed
3.4. Effects of Interventions on Time to Successful Walking Speed Recovery and Its Moderators
3.5. Compliance with Protein Supplementation and Exercise
4. Discussion
4.1. Summary of Main Findings
4.2. Sarcopenia Prevalence in Study Cohort
4.3. WS Recovery Pattern over the Follow-Up Period
4.4. Effect of RET on Time to Normal WS
4.5. Treatment Efficiency of PS+RET on Time to Recovery to Normal WS
4.6. Moderators Influencing Treatment Efficiency
4.7. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Palazzo, C.; Ravaud, J.-F.; Papelard, A.; Ravaud, P.; Poiraudeau, S. The burden of musculoskeletal conditions. Osteoarthr. Cartil. 2014, 9, S218–S219. [Google Scholar] [CrossRef]
- Nielsen, L.A.; Schepman, P.; Blakeman, K.H.; Wilhelm, S.; Robinson, R.; Beck, C.; Hansen, J.L.; Rolfson, O. Prescription patterns and predictors of unmet pain relief in patients with difficult-to-treat osteoarthritis in the Nordics: Analyses from the BISCUITS study. Scand. J. Pain 2022, 23, 149–160. [Google Scholar] [CrossRef]
- Quicke, J.G.; Foster, N.E.; Croft, P.R.; Ogollah, R.O.; Holden, M.A. Change in physical activity level and clinical outcomes in older adults with knee pain: A secondary analysis from a randomised controlled trial. BMC Musculoskelet. Disord. 2018, 19, 59. [Google Scholar] [CrossRef]
- Edwards, M.H.; van der Pas, S.; Denkinger, M.D.; Parsons, C.; Jameson, K.A.; Schaap, L.; Zambon, S.; Castell, M.V.; Herbolsheimer, F.; Nasell, H.; et al. Relationships between physical performance and knee and hip osteoarthritis: Findings from the European Project on Osteoarthritis (EPOSA). Age Ageing 2014, 43, 806–813. [Google Scholar] [CrossRef]
- White, D.K.; Niu, J.; Zhang, Y. Is symptomatic knee osteoarthritis a risk factor for a trajectory of fast decline in gait speed? Results from a longitudinal cohort study. Arthritis Care Res. 2012, 65, 187–194. [Google Scholar] [CrossRef]
- Zhakhina, G.; Gusmanov, A.; Sakko, Y.; Yerdessov, S.; Semenova, Y.; Saginova, D.; Batpen, A.; Gaipov, A. The Regional Burden and Disability-Adjusted Life Years of Knee Osteoarthritis in Kazakhstan 2014–2020. Biomedicines 2023, 11, 216. [Google Scholar] [CrossRef]
- Çay, H.F.; Akıncı, A.; Altan, L.; Ataman, Ş.; Aydoğdu, S.; Dıraçoğlu, D.; Genç, H.; Hepgüler, S.; Ketenci, A.; Öneş, K.; et al. Evaluation of disease burden, patient journey, unmet diagnosis and treatment needs of patients with HIP and knee osteoarthritis in Turkey: A study through Delphi Methodology. Osteoarthr. Cartil. Open 2023, 5, 100332. [Google Scholar] [CrossRef]
- Zitko, P.; Bilbeny, N.; Balmaceda, C.; Abbott, T.; Carcamo, C.; Espinoza, M. Prevalence, burden of disease, and lost in health state utilities attributable to chronic musculoskeletal disorders and pain in Chile. BMC Public Health 2021, 21, 937. [Google Scholar] [CrossRef]
- Kiadaliri, A.A.; Lohmander, L.S.; Moradi-Lakeh, M.; Petersson, I.F.; Englund, M. High and rising burden of hip and knee osteoarthritis in the Nordic region, 1990–2015. Acta. Orthop 2018, 89, 177–183. [Google Scholar] [CrossRef]
- Palazzo, C.; Nguyen, C.; Lefevre-Colau, M.-M.; Rannou, F.; Poiraudeau, S. Risk factors and burden of osteoarthritis. Ann. Phys. Rehabil. Med. 2016, 59, 134–138. [Google Scholar] [CrossRef]
- Øiestad, B.E.; White, D.K.; Booton, R.; Niu, J.; Zhang, Y.; Torner, J.; Lewis, C.E.; Nevitt, M.; Lavalley, M.; Felson, D.T. Longitudinal Course of Physical Function in People with Symptomatic Knee Osteoarthritis: Data from the Multicenter Osteoarthritis Study and the Osteoarthritis Initiative. Arthritis Care Res. 2016, 68, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Davison, M.J.; Ioannidis, G.; Maly, M.R.; Adachi, J.D.; Beattie, K.A. Intermittent and constant pain and physical function or performance in men and women with knee osteoarthritis: Data from the osteoarthritis initiative. Clin. Rheumatol. 2014, 35, 371–379. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Parra-Soto, S.; Cid, V.; Venegas, P.; Huidobro, A.; Ferreccio, C.; Celis-Morales, C. The association between walking pace and grip strength and all-cause mortality: A prospective analysis from the MAUCO cohort. Maturitas 2023, 168, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Grazzi, G.; Mazzoni, G.; Myers, J.; Codecà, L.; Pasanisi, G.; Napoli, N.; Guerzoni, F.; Volpato, S.; Conconi, F.; Chiaranda, G. Improved walking speed is associated with lower hospitalisation rates in patients in an exercise-based secondary prevention programme. Heart 2016, 102, 1902–1908. [Google Scholar] [CrossRef] [PubMed]
- Yokota, A.; Maeshima, E.; Sasaki, K.; Ooi, T.; Sainoh, T.; Hosokawa, H. Physical functions associated with health-related quality of life in older adults diagnosed with knee osteoarthritis. J. Phys. Ther. Sci. 2023, 35, 60–65. [Google Scholar] [CrossRef]
- Christensen, J.C.; Jakiela, J.T.; White, D.K. Factors Associated with Trajectories of Physical Activity over 8 Years in Knee Osteoarthritis. Eur. J. Rheumatol. 2022, 10, 1–7. [Google Scholar] [CrossRef]
- Hsu, M.-F.; Hsieh, C.-M.; Chiu, A.-F. Factors Affecting Physical Activity of People with Knee Osteoarthritis in Southern Taiwan: A Multiple Logistic Regression Analysis. Int. J. Clin. Pr. 2022, 2022, 4736231. [Google Scholar] [CrossRef]
- Zanker, J.; Sim, M.; Anderson, K.; Balogun, S.; Brennan-Olsen, S.L.; Dent, E.; Duque, G.; Girgis, C.M.; Grossmann, M.; Hayes, A.; et al. Consensus guidelines for sarcopenia prevention, diagnosis and management in Australia and New Zealand. J. Cachexia. Sarcopenia Muscle 2022, 14, 142–156. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Hu, K.; Yan, C.; Zhao, B.; Mei, F.; Chen, F.; Zhao, L.; Shang, Y.; Ma, Y.; Ma, B. Associated Factors of Sarcopenia in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 4291. [Google Scholar] [CrossRef]
- Swan, L.; Warters, A.; O’Sullivan, M. Socioeconomic Disadvantage is Associated with Probable Sarcopenia in Community-Dwelling Older Adults: Findings from the English Longitudinal Study of Ageing. J. Frailty Aging 2022, 11, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Teschler, M.; Goisser, S.; Bebenek, M.; Von Stengel, S.; Bollheimer, L.C.; Sieber, C.C.; Freiberger, E. Prevalence of sarcopenia in Germany and the corresponding effect of osteoarthritis in females 70 years and older living in the community: Results of the FORMoSA study. Clin. Interv. Aging 2015, 10, 1565–1573. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Stefanac, S.; Koyanagi, A.; Al-Daghri, N.M.; Sabico, S.; Cooper, C.; Rizzoli, R.; Reginster, J.Y.; Barbagallo, M.; Dominguez, L.J.; et al. Lower Limb Muscle Strength and Muscle Mass Are Associated with Incident Symptomatic Knee Osteoarthritis: A Longitudinal Cohort Study. Front. Endocrinol (Lausanne) 2021, 12, 804560. [Google Scholar] [CrossRef]
- Pérez-Sousa, M.; del Pozo-Cruz, J.; Cano-Gutiérrez, C.A.; Izquierdo, M.; Ramírez-Vélez, R. High Prevalence of Probable Sarcopenia in a Representative Sample From Colombia: Implications for Geriatrics in Latin America. J. Am. Med. Dir. Assoc. 2020, 22, 859–864.e1. [Google Scholar] [CrossRef] [PubMed]
- Misra, D.; Fielding, R.A.; Felson, D.T.; Niu, J.; Brown, C.; Nevitt, M.; Lewis, C.E.; Torner, J.; Neogi, T. Risk of Knee Osteoarthritis with Obesity, Sarcopenic Obesity, and Sarcopenia. Arthritis Rheumatol 2019, 71, 232–237. [Google Scholar] [CrossRef]
- Kim, H.T.; Kim, H.J.; Ahn, H.Y.; Hong, Y.H. An analysis of age-related loss of skeletal muscle mass and its significance on osteoarthritis in a Korean population. Korean, J. Intern Med. 2016, 31, 585–593. [Google Scholar] [CrossRef]
- Lee, D.C.; Shook, R.P.; Drenowatz, C.; Blair, S.N. Physical activity and sarcopenic obesity: Definition, assessment, prevalence and mechanism. Future Sci. OA 2016, 2, FSO127. [Google Scholar] [CrossRef]
- Pickering, M.-E.; Chapurlat, R. Where Two Common Conditions of Aging Meet: Osteoarthritis and Sarcopenia. Calcif. Tissue Int. 2020, 107, 203–211. [Google Scholar] [CrossRef]
- Bindawas, S.M.; Vennu, V. Longitudinal Effects of Physical Inactivity and Obesity on Gait Speed in Older Adults with Frequent Knee Pain: Data from the Osteoarthritis Initiative. Int. J. Environ. Res. Public Health 2015, 12, 1849–1863. [Google Scholar] [CrossRef]
- Sun, R.; Tomkins-Lane, C.; Muaremi, A.; Kuwabara, A.; Smuck, M. Physical activity thresholds for predicting longitudinal gait decline in adults with knee osteoarthritis. Osteoarthr. Cartil. 2021, 29, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Aslan, S.G.; Genç, H. Sarcopenia in knee osteoarthritis: The association with clinical and sonographic findings, physical function, and nutrition. Ir. J. Med. Sci. 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Shorter, E.; Sannicandro, A.J.; Poulet, B.; Goljanek-Whysall, K. Skeletal Muscle Wasting and Its Relationship with Osteoarthritis: A Mini-Review of Mechanisms and Current Interventions. Curr. Rheumatol. Rep. 2019, 21, 40. [Google Scholar] [CrossRef]
- Veronese, N.; Punzi, L.; Sieber, C.; Bauer, J.; Reginster, J.Y.; Maggi, S. Sarcopenic osteoarthritis: A new entity in geriatric medicine? Eur. Geriatr. Med. 2018, 9, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef]
- Brophy, R.H.; Fillingham, Y.A. AAOS Clinical Practice Guideline Summary: Management of Osteoarthritis of the Knee (Nonarthroplasty), Third Edition. J. Am. Acad. Orthop. Surg. 2022, 30, e721–e729. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef]
- Skou, S.T.; Roos, E.M. Physical therapy for patients with knee and hip osteoarthritis: Supervised, active treatment is current best practice. Clin. Exp. Rheumatol. 2019, 37 (Suppl. S120), 112–117. [Google Scholar]
- Ferreira, L.F.; Scariot, E.L.; da Rosa, L.H.T. The effect of different exercise programs on sarcopenia criteria in older people: A systematic review of systematic reviews with meta-analysis. Arch. Gerontol. Geriatr. 2023, 105, 104868. [Google Scholar] [CrossRef]
- Wang, H.; Huang, W.Y.; Zhao, Y. Efficacy of Exercise on Muscle Function and Physical Performance in Older Adults with Sarcopenia: An Updated Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8212. [Google Scholar] [CrossRef]
- Lu, L.; Mao, L.; Feng, Y.; Ainsworth, B.E.; Liu, Y.; Chen, N. Effects of different exercise training modes on muscle strength and physical performance in older people with sarcopenia: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 78. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.; Chen, H.; Kuo, Y.; Tsauo, J.; Huang, S.; Liou, T. Effects of Muscle Strength Training on Muscle Mass Gain and Hypertrophy in Older Adults with Osteoarthritis: A Systematic Review and Meta-Analysis. Arthritis Care Res. 2019, 72, 1703–1718. [Google Scholar] [CrossRef]
- Li, S.; Ng, W.H.; Abujaber, S.; Shaharudin, S. Effects of resistance training on gait velocity and knee adduction moment in knee osteoarthritis patients: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16104. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-D.; Tsauo, J.-Y.; Chiu, Y.-S.; Ku, J.-W.; Huang, S.-W.; Liou, T.-H. Effects of Elastic Resistance Exercise after Total Knee Replacement on Muscle Mass and Physical Function in Elderly Women with Osteoarthritis: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2020, 99, 381–389. [Google Scholar] [CrossRef]
- Liao, C.-D.; Liao, Y.-H.; Liou, T.-H.; Hsieh, C.-Y.; Kuo, Y.-C.; Chen, H.-C. Effects of Protein-Rich Nutritional Composition Supplementation on Sarcopenia Indices and Physical Activity during Resistance Exercise Training in Older Women with Knee Osteoarthritis. Nutrients 2021, 13, 2487. [Google Scholar] [CrossRef]
- Liao, C.-D.; Tsauo, J.-Y.; Huang, S.-W.; Ku, J.-W.; Hsiao, D.-J.; Liou, T.-H. Effects of elastic band exercise on lean mass and physical capacity in older women with sarcopenic obesity: A randomized controlled trial. Sci. Rep. 2018, 8, 2317. [Google Scholar] [CrossRef]
- Carcelén-Fraile, M.D.C.; Lorenzo-Nocino, M.F.; Afanador-Restrepo, D.F.; Rodríguez-López, C.; Aibar-Almazán, A.; Hita-Contreras, F.; Achalandabaso-Ochoa, A.; Castellote-Caballero, Y. Effects of different intervention combined with resistance training on musculoskeletal health in older male adults with sarcopenia: A systematic review. Front. Public Health 2023, 10, 1037464. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-H.; Roh, Y. Which intervention is more effective in improving sarcopenia in older adults? A systematic review with meta-analysis of randomized controlled trials. Mech. Ageing Dev. 2023, 210, 111773. [Google Scholar] [CrossRef]
- Negm, A.M.; Lee, J.; Hamidian, R.; Jones, C.A.; Khadaroo, R.G. Management of Sarcopenia: A Network Meta-Analysis of Randomized Controlled Trials. J. Am. Med. Dir. Assoc. 2022, 23, 707–714. [Google Scholar] [CrossRef]
- Maldonado, E.C.; Marqués-Jiménez, D.; Casas-Agustench, P.; Bach-Faig, A. Effect of supplementation with leucine alone, with other nutrients or with physical exercise in older people with sarcopenia: A systematic review. Endocrinol. Diabetes Nutr. 2022, 69, 601–613. [Google Scholar] [CrossRef]
- Kirwan, R.P.; Mazidi, M.; García, C.R.; Lane, K.E.; Jafari, A.; Butler, T.; de Heredia, F.P.; Davies, I.G. Protein interventions augment the effect of resistance exercise on appendicular lean mass and handgrip strength in older adults: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2021, 115, 897–913. [Google Scholar] [CrossRef] [PubMed]
- Perez-Sousa, M.A.; Venegas-Sanabria, L.C.; Chavarro-Carvajal, D.A.; Cano-Gutierrez, C.A.; Izquierdo, M.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Gait speed as a mediator of the effect of sarcopenia on dependency in activities of daily living. J. Cachex- Sarcopenia Muscle 2019, 10, 1009–1015. [Google Scholar] [CrossRef]
- Miller, M.E.; Magaziner, J.; Marsh, A.P.; Fielding, R.A.; Gill, T.M.; King, A.C.; Kritchevsky, S.; Manini, T.; McDermott, M.M.; Neiberg, R.; et al. Gait Speed and Mobility Disability: Revisiting Meaningful Levels in Diverse Clinical Populations. J. Am. Geriatr. Soc. 2018, 66, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Akune, T.; Muraki, S.; Oka, H.; Tanaka, S.; Kawaguchi, H.; Tokimura, F.; Yoshida, H.; Suzuki, T.; Nakamura, K.; Yoshimura, N. Incidence of certified need of care in the long-term care insurance system and its risk factors in the elderly of Japanese population-based cohorts: The ROAD study. Geriatr. Gerontol. Int. 2013, 14, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum 1986, 29, 1039–1049. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Abizanda Soler, P.; Paterna Mellinas, G.; Martinez Sanchez, E.; Lopez Jimenez, E. Comorbidity in the elderly: Utility and validity of assessment tools. Rev. Esp. Geriatr Gerontol. 2010, 45, 219–228. [Google Scholar] [CrossRef]
- Lyons, J.G.; Heeren, T.; Stuver, S.O.; Fredman, L. Assessing the Agreement between 3-Meter and 6-Meter Walk Tests in 136 Community-Dwelling Older Adults. J. Aging Health 2014, 27, 594–605. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Tsauo, J.Y.; Lin, L.F.; Huang, S.W.; Ku, J.W.; Chou, L.C.; Liou, T.H. Effects of elastic resistance exercise on body composition and physical capacity in older women with sarcopenic obesity: A CONSORT-compliant prospective randomized controlled trial. Medicine 2017, 96, e7115. [Google Scholar] [CrossRef]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Andersen, L.L.; Andersen, C.H.; Mortensen, O.S.; Poulsen, O.M.; Bjørnlund, I.B.T.; Zebis, M.K. Muscle Activation and Perceived Loading During Rehabilitation Exercises: Comparison of Dumbbells and Elastic Resistance. Phys. Ther. 2010, 90, 538–549. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Lührmann, P.M.; Herbert, B.M.; Gaster, C.; Neuhäuser-Berthold, M. Validation of a self-administered 3-day estimated dietary record for use in the elderly. Eur. J. Nutr. 1999, 38, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Byrne, G. MyFitnessPal. Nurs. Stand 2015, 29, 31. [Google Scholar] [CrossRef]
- Laing, B.Y.; Mangione, C.M.; Tseng, C.H.; Leng, M.; Vaisberg, E.; Mahida, M.; Bholat, M.; Glazier, E.; Morisky, D.E.; Bell, D.S. Effectiveness of a smartphone application for weight loss compared with usual care in overweight primary care patients: A randomized, controlled trial. Ann. Intern Med. 2014, 161, S5–S12. [Google Scholar] [CrossRef]
- Heo, S.; McSweeney, J.; Prewitt, T.E.; Lee, J.Y.; Moser, D.K.; Shaw-Devine, A.; Morell, A.; Kim, J.; Yeary, K.H.K. A Tailored Dietary Sodium Intervention Using Technology and Psychosocial Support: A Pilot Study. J. Cardiovasc. Nurs. 2019, 34, 137–140. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Arai, H.; Kritchevsky, S.B.; Guralnik, J.; Bauer, J.M.; Pahor, M.; Clark, B.C.; Cesari, M.; et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef]
- Navarrete-Villanueva, D.; Gómez-Cabello, A.; Marín-Puyalto, J.; Moreno, L.A.; Vicente-Rodríguez, G.; Casajús, J.A. Frailty and Physical Fitness in Elderly People: A Systematic Review and Meta-analysis. Sports Med. 2020, 51, 143–160. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Greiwe, J.S.; Cheng, B.; Rubin, D.C.; Yarasheski, K.E.; Semenkovich, C.F. Resistance exercise decreases skeletal muscle tumor necrosis factor α in frail elderly humans. FASEB J. 2001, 15, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.I.; Ahn, S.H.; Kim, Y.; Lee, J.E.; Choi, E.; Seo, S.K. Effects of sarcopenia and sarcopenic obesity on joint pain and degenerative osteoarthritis in postmenopausal women. Sci. Rep. 2022, 12, 1–8. [Google Scholar] [CrossRef]
- Therakomen, V.; Petchlorlian, A.; Lakananurak, N. Prevalence and risk factors of primary sarcopenia in community-dwelling outpatient elderly: A cross-sectional study. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Gorial, F.I.; Yahya, R.D. Sarcopenia among Patients with Knee Osteoarthritis: An Observational Descriptive Study. Int. J. Sci. Res. 2019, 8, 1163–1167. [Google Scholar]
- Jin, W.S.; Choi, E.J.; Lee, S.Y.; Bae, E.J.; Lee, T.H.; Park, J. Relationships among Obesity, Sarcopenia, and Osteoarthritis in the Elderly. J. Obes. Metab. Syndr. 2017, 26, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J. Use It or Lose It? A Meta-Analysis on the Effects of Resistance Training Cessation (Detraining) on Muscle Size in Older Adults. Int. J. Environ. Res. Public Heal. 2022, 19, 14048. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-D.; Chen, H.-C.; Huang, S.-W.; Liou, T.-H. The Role of Muscle Mass Gain Following Protein Supplementation Plus Exercise Therapy in Older Adults with Sarcopenia and Frailty Risks: A Systematic Review and Meta-Regression Analysis of Randomized Trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef]
- Zhao, H.; Cheng, R.; Song, G.; Teng, J.; Shen, S.; Fu, X.; Yan, Y.; Liu, C. The Effect of Resistance Training on the Rehabilitation of Elderly Patients with Sarcopenia: A Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15491. [Google Scholar] [CrossRef]
- Wang, H.; Chen, D.; Pan, Q.; Hueman, M.T. Using Weighted Differences in Hazards as Effect Sizes for Survival Data. J. Stat. Theory Pr. 2022, 16, 1–35. [Google Scholar] [CrossRef]
- Azuero, A. A note on the magnitude of hazard ratios. Cancer 2016, 122, 1298–1299. [Google Scholar] [CrossRef]
- Skvortsov, D.; Kaurkin, S.; Prizov, A.; Altukhova, A.; Troitskiy, A.; Lazko, F. Biomechanical Changes in Gait Patterns of Patients with Grade II Medial Gonarthritis. Diagnostics 2021, 11, 1242. [Google Scholar] [CrossRef] [PubMed]
- Hirase, T.; Okubo, Y.; Delbaere, K.; Menant, J.C.; Lord, S.R.; Sturnieks, D.L. Predictors of development and persistence of musculoskeletal pain in community-dwelling older people: A two -year longitudinal study. Geriatr. Gerontol. Int. 2021, 21, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-D.; Chen, H.-C.; Huang, S.-W.; Liou, T.-H. Impact of sarcopenia on rehabilitation outcomes after total knee replacement in older adults with knee osteoarthritis. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X21998508. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.-J.; Liao, C.-D.; Tsai, M.-W.; Chen, C.-N. Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis. Nutrients 2019, 11, 2163. [Google Scholar] [CrossRef]
- Yin, Y.-H.; Liu, J.Y.W.; Välimäki, M. Effectiveness of non-pharmacological interventions on the management of sarcopenic obesity: A systematic review and meta-analysis. Exp. Gerontol. 2020, 135, 110937. [Google Scholar] [CrossRef]
- Luo, D.; Lin, Z.; Li, S.; Liu, S.-J. Effect of nutritional supplement combined with exercise intervention on sarcopenia in the elderly: A meta-analysis. Int. J. Nurs. Sci. 2017, 4, 389–401. [Google Scholar] [CrossRef]
- Huang, L.-P.; Condello, G.; Kuo, C.-H. Effects of Milk Protein in Resistance Training-Induced Lean Mass Gains for Older Adults Aged ≥ 60 y: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2815. [Google Scholar] [CrossRef]
- Liao, C.-D.; Wu, Y.-T.; Tsauo, J.-Y.; Chen, P.-R.; Tu, Y.-K.; Chen, H.-C.; Liou, T.-H. Effects of Protein Supplementation Combined with Exercise Training on Muscle Mass and Function in Older Adults with Lower-Extremity Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Trials. Nutrients 2020, 12, 2422. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznaric, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef]
- Miller, M.S.; Callahan, D.M.; Tourville, T.W.; Slauterbeck, J.R.; Kaplan, A.; Fiske, B.R.; Savage, P.D.; Ades, P.A.; Beynnon, B.D.; Toth, M.J. Moderate-intensity resistance exercise alters skeletal muscle molecular and cellular structure and function in inactive older adults with knee osteoarthritis. J. Appl. Physiol. 2017, 122, 775–787. [Google Scholar] [CrossRef]
- Jones, M.D.; Wewege, M.A.; Hackett, D.A.; Keogh, J.W.L.; Hagstrom, A.D. Sex Differences in Adaptations in Muscle Strength and Size Following Resistance Training in Older Adults: A Systematic Review and Meta-analysis. Sports Med. 2020, 51, 503–517. [Google Scholar] [CrossRef] [PubMed]
- Da Boit, M.; Sibson, R.; Meakin, J.R.; Aspden, R.M.; Thies, F.; Mangoni, A.A.; Gray, S.R. Sex differences in the response to resistance exercise training in older people. Physiol. Rep. 2016, 4, e12834. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Villareal, D.T.; Sinacore, D.R.; Shah, K.; Mittendorfer, B. Muscle protein synthesis response to exercise training in obese, older men and women. Med. Sci. Sport. Exerc. 2012, 44, 1259–1266. [Google Scholar] [CrossRef] [PubMed]
- White, D.K.; Keysor, J.J.; LaValley, M.P.; Lewis, C.E.; Torner, J.C.; Nevitt, M.C.; Felson, D.T. Clinically Important Improvement in Function Is Common in People with or at High Risk of Knee OA: The MOST Study. J. Rheumatol. 2010, 37, 1244–1251. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | UC | RET | PS+RET | p |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| n a | 36 | 36 | 36 | |
| Women, n (%) | 23(63.9) | 26(72.2) | 25(69.4) | 0.740 c |
| Age (years) | 74.9 ± 6.6 | 73.8 ± 5.7 | 73.5 ± 6.3 | 0.540 b |
| ASMMI (kg/m2) | ||||
| Men | 6.2 ± 0.6 | 6.3 ± 0.6 | 6.2 ± 0.7 | 0.973 b |
| Women | 5.1 ± 0.4 | 5.1 ± 0.5 | 5.1 ± 0.5 | 0.996 b |
| BMI (kg/m2) | 27.4 ± 3.3 | 28.2 ± 3.4 | 28.1 ± 3.7 | 0.567 b |
| CIRS score | 14.9 ± 4.6 | 15.2 ± 4.7 | 13.7 ± 4.4 | 0.376 b |
| Disease duration (year) | 10.8 ± 7.9 | 9.2 ± 8.2 | 9.9± 8.6 | 0.714 b |
| Involved leg, n (%) | 0.856 c | |||
| Right | 20(55.6) | 18(50.0) | 22(61.1) | |
| Left | 9(25.0) | 12(33.3) | 9(25.0) | |
| Bilateral | 7(19.4) | 6(16.7) | 5(13.9) | |
| KL grade, n (%) | 0.612 c | |||
| 2 | 7(19.4) | 11(30.6) | 10(27.8) | |
| 3 | 24(66.7) | 19(52.8) | 18(50.0) | |
| 4 | 5(13.9) | 6(16.7) | 8(22.2) | |
| Number of comorbidities, n (%) | 0.789 c | |||
| 1 | 11(30.6) | 11(30.6) | 12(33.3) | |
| 2 | 11(30.6) | 11(30.6) | 14(38.9) | |
| 3 | 8(22.2) | 11(30.6) | 6(16.7) | |
| >3 | 6(16.7) | 3(8.2) | 4(11.1) | |
| Protein intake (g/kg/day) | 0.84 ± 0.26 | 0.79 ± 0.25 | 0.81 ± 0.24 | 0.699 b |
| Pain (VAS) | 7.5 ± 1.4 | 7.1 ± 1.4 | 7.7 ± 1.4 | 0.193 b |
| Walking speed (m/s) | 0.72 ± 0.16 | 0.75 ± 0.14 | 0.73 ± 0.15 | 0.743 b |
| Model Established | Coefficient (B) | SE (B) | Hazard Ratio | 95% CI (Lower, Upper) | p |
|---|---|---|---|---|---|
| Covariates | |||||
| Crude model (n = 108; overall χ2 = 16.91, p < 0.001) | |||||
| Group (ref: UC) | |||||
| RET | 0.82 | 0.39 | 2.27 | (1.06, 4.86) | 0.03 |
| PS plus RET | 1.44 | 0.38 | 4.21 | (2.01, 8.79) | <0.001 |
| Adjusted model (n = 108; overall χ2 = 44.75, p < 0.001) | |||||
| Group (ref: UC) | |||||
| RET | 0.79 | 0.40 | 2.21 | (1.01, 4.82) | 0.04 |
| PS plus RET | 1.67 | 0.39 | 5.48 | (2.48, 11.23) | <0.001 |
| Sex (ref: women) | |||||
| Men | 0.75 | 0.32 | 2.12 | (1.13, 3.97) | 0.02 |
| KL grade (ref: grade 2) | |||||
| Grade 3 | −0.14 | 0.33 | 0.87 | (0.46, 1.65) | 0.67 |
| Grade 4 | −0.26 | 0.49 | 0.77 | (0.29, 2.03) | 0.60 |
| Age | –0.05 | 0.03 | 0.95 | (0.90, 1.01) | 0.11 |
| BMI | –0.04 | 0.04 | 0.96 | (0.88, 1.05) | 0.39 |
| CIRS score | –0.02 | 0.03 | 0.98 | (0.92, 1.05) | 0.61 |
| Pain score (baseline) | –0.07 | 0.11 | 0.93 | (0.75, 1.16) | 0.51 |
| Walking speed (baseline) | 3.07 | 1.22 | 21.63 | (1.97, 237.09) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, C.-D.; Huang, S.-W.; Chen, H.-C.; Huang, Y.-Y.; Liou, T.-H.; Lin, C.-L. Effects of Protein Supplementation Combined with Resistance Exercise Training on Walking Speed Recovery in Older Adults with Knee Osteoarthritis and Sarcopenia. Nutrients 2023, 15, 1552. https://doi.org/10.3390/nu15071552
Liao C-D, Huang S-W, Chen H-C, Huang Y-Y, Liou T-H, Lin C-L. Effects of Protein Supplementation Combined with Resistance Exercise Training on Walking Speed Recovery in Older Adults with Knee Osteoarthritis and Sarcopenia. Nutrients. 2023; 15(7):1552. https://doi.org/10.3390/nu15071552
Chicago/Turabian StyleLiao, Chun-De, Shih-Wei Huang, Hung-Chou Chen, Yu-Yun Huang, Tsan-Hon Liou, and Che-Li Lin. 2023. "Effects of Protein Supplementation Combined with Resistance Exercise Training on Walking Speed Recovery in Older Adults with Knee Osteoarthritis and Sarcopenia" Nutrients 15, no. 7: 1552. https://doi.org/10.3390/nu15071552
APA StyleLiao, C.-D., Huang, S.-W., Chen, H.-C., Huang, Y.-Y., Liou, T.-H., & Lin, C.-L. (2023). Effects of Protein Supplementation Combined with Resistance Exercise Training on Walking Speed Recovery in Older Adults with Knee Osteoarthritis and Sarcopenia. Nutrients, 15(7), 1552. https://doi.org/10.3390/nu15071552