
“What Made My Eating Disorder Worse?” The Impact of the COVID-19 Pandemic from the Perspective of Adolescents with Anorexia Nervosa



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Original Questionnaire and Adjustments
2.3. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. Changes in AN Symptomatology
3.3. Changes in Social Media Use, Mirror Checking, Cooking, and Conflicts with Parents
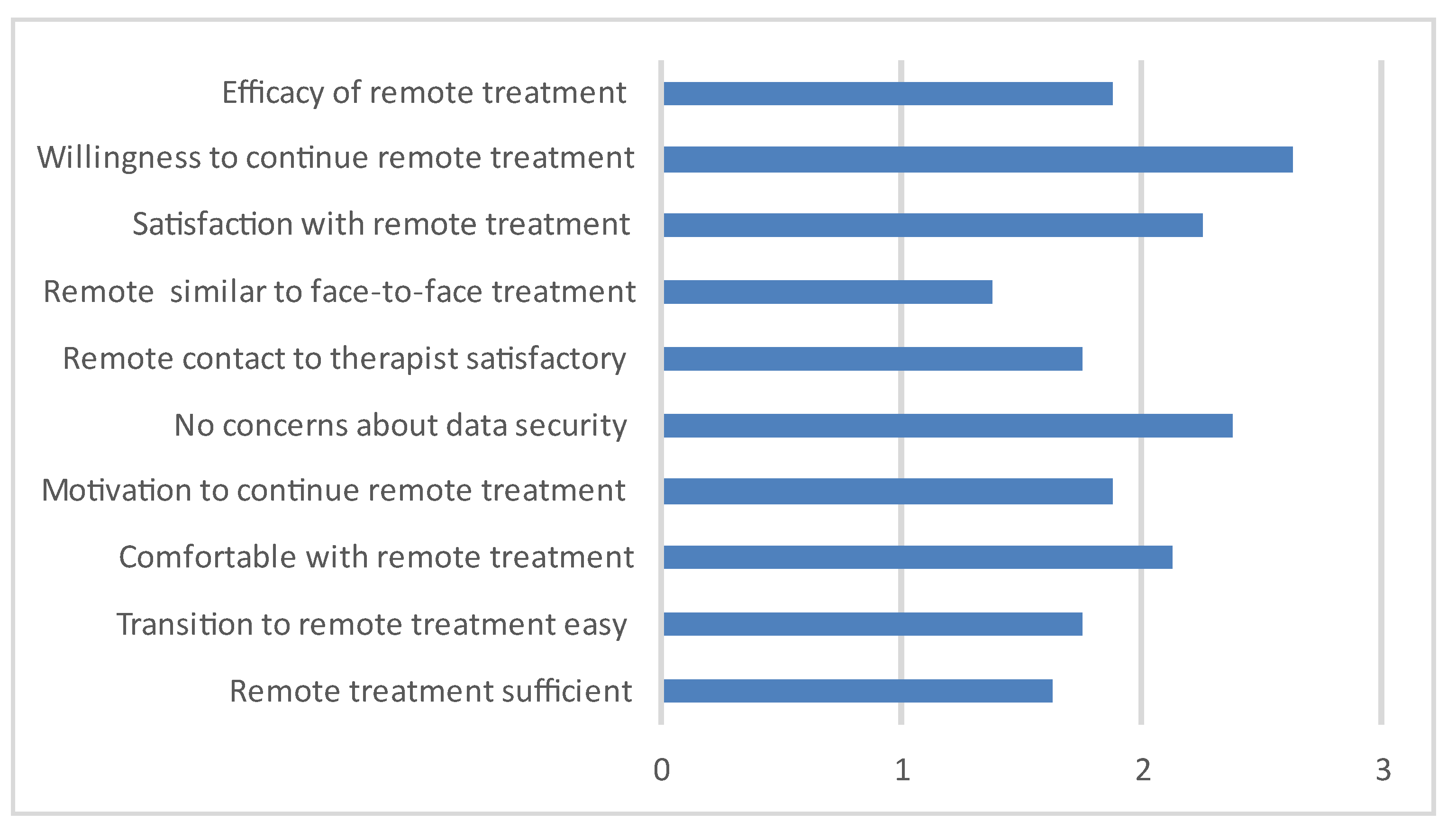
3.4. Remote Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, E.A.K.; Mitra, A.K.; Bhuiyan, A.R. Impact of COVID-19 on mental health in adolescents: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 2470. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2021, 25, 879–889. [Google Scholar] [CrossRef]
- J Devoe, D.; Han, A.; Anderson, A.; Katzman, D.K.; Patten, S.B.; Soumbasis, A.; Flanagan, J.; Paslakis, G.; Vyver, E.; Marcoux, G.; et al. The impact of the COVID-19 pandemic on eating disorders: A systematic review. Int. J. Eat. Disord. 2022, 56, 5–25. [Google Scholar] [CrossRef]
- Herpertz-Dahlmann, B.; Dahmen, B. Children in need—Diagnostics, epidemiology, treatment and outcome of early onset anorexia nervosa. Nutrients 2019, 11, 1932. [Google Scholar] [CrossRef] [PubMed]
- Gilsbach, S.; Plana, M.T.; Castro-Fornieles, J.; Gatta, M.; Karlsson, G.P.; Flamarique, I.; Raynaud, J.-P.; Riva, A.; Solberg, A.-L.; van Elburg, A.A.; et al. Increase in admission rates and symptom severity of childhood and adolescent anorexia nervosa in Europe during the COVID-19 pandemic: Data from specialized eating disorder units in different European countries. Child Adolesc. Psychiatry Ment. Health 2022, 16, 46. [Google Scholar] [CrossRef] [PubMed]
- Herpertz-Dahlmann, B.; Dempfle, A.; Eckardt, S. The youngest are hit hardest: The influence of the COVID-19 pandemic on the hospitalization rate for children, adolescents, and young adults with anorexia nervosa in a large German representative sample. Eur. Psychiatry 2022, 65, e84. [Google Scholar] [CrossRef] [PubMed]
- Otto, A.K.; Jary, J.M.; Sturza, J.; Miller, C.A.; Prohaska, N.; Bravender, T.; Van Huysse, J. Medical admissions among adolescents with eating disorders during the COVID-19 Pandemic. Pediatrics 2021, 148, e2021052201. [Google Scholar] [CrossRef]
- Agostino, H.; Burstein, B. 104 New Presentations of Anorexia Nervosa and Atypical Anorexia Nervosa In Adolescents During the COVID-19 Pandemic. Paediatr. Child Health 2021, 26 (Suppl. 1), e74. [Google Scholar] [CrossRef]
- Gao, Y.; Bagheri, N.; Furuya-Kanamori, L. Has the COVID-19 pandemic lockdown worsened eating disorders symptoms among patients with eating disorders? A systematic review. J. Public Health 2022, 30, 2743–2752. [Google Scholar] [CrossRef]
- Matthews, A.; Kramer, R.A.; Peterson, C.M.; Mitan, L. Higher admission and rapid readmission rates among medically hospitalized youth with anorexia nervosa/atypical anorexia nervosa during COVID-19. Eat. Behav. 2021, 43, 101573. [Google Scholar] [CrossRef]
- Graell, M.; Morón-Nozaleda, M.G.; Camarneiro, R.; Villaseñor, Á.; Yáñez, S.; Muñoz, R.; Martínez-Núñez, B.; Miguélez-Fernández, C.; Muñoz, M.; Faya, M. Children and adolescents with eating disorders during COVID-19 confinement: Difficulties and future challenges. Eur. Eat. Disord. Rev. 2020, 28, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, L.; Ziv, A.; Vardi, Y.; Hadas, S.; Zuabi, T.; Yeshareem, L.; Gur, T.; Steinling, S.; Scheuerman, O.; Levinsky, Y. The effect of COVID-19 pandemic on hospitalizations and disease characteristics of adolescents with anorexia nervosa. Eur. J. Pediatr. 2022, 181, 1767–1771. [Google Scholar] [CrossRef] [PubMed]
- Springall, G.; Cheung, M.; Sawyer, S.M.; Yeo, M. Impact of the coronavirus pandemic on anorexia nervosa and atypical anorexia nervosa presentations to an Australian tertiary paediatric hospital. J. Paediatr. Child Health 2022, 58, 491–496. [Google Scholar] [CrossRef]
- Akgül, S.; Akdemir, D.; Nalbant, K.; Derman, O.; Ersöz Alan, B.; Tüzün, Z.; Kanbur, N. The effects of the COVID-19 lockdown on adolescents with an eating disorder and identifying factors predicting disordered eating behaviour. Early Interv. Psychiatry 2022, 16, 544–551. [Google Scholar] [CrossRef]
- Baenas, I.; Caravaca-Sanz, E.; Granero, R.; Sánchez, I.; Riesco, N.; Testa, G.; Vintró-Alcaraz, C.; Treasure, J.; Jiménez-Murcia, S.; Fernández-Aranda, F. COVID-19 and Eating Disorders during Confinement: Analysis of Factors Associated with Resilience and Aggravation of Symptoms. Eur. Eat. Disord. Rev. 2020, 28, 855–863. [Google Scholar] [CrossRef]
- Schlegl, S.; Maier, J.; Meule, A.; Voderholzer, U. Eating disorders in times of the COVID-19 pandemic—Results from an online survey of patients with anorexia nervosa. Int. J. Eat. Disord. 2020, 53, 1791–1800. [Google Scholar] [CrossRef]
- Branley-Bell, D.; Talbot, C.V. “It is the only constant in what feels like a completely upside down and scary world”: Living with an eating disorder during COVID-19 and the importance of perceived control for recovery and relapse. Appetite 2021, 167, 105596. [Google Scholar] [CrossRef]
- Zeiler, M.; Wittek, T.; Kahlenberg, L.; Gröbner, E.M.; Nitsch, M.; Wagner, G.; Truttmann, S.; Krauss, H.; Waldherr, K.; Karwautz, A. Impact of Covid-19 Confinement on Adolescent Patients with Anorexia Nervosa: A Qualitative Interview Study Involving Adolescents and Parents. Int. J. Environ. Res. Public Health 2021, 18, 4251. [Google Scholar] [CrossRef]
- Fernández-Aranda, F.; Munguía, L.; Mestre-Bach, G.; Steward, T.; Etxandi, M.; Baenas, I.; Granero, R.; Sánchez, I.; Ortega, E.; Andreu, A.; et al. COVID Isolation Eating Scale (CIES): Analysis of the Impact of Confinement in Eating Disorders and Obesity—A Collaborative International Study. In European Eating Disorders Review; John Wiley and Sons Ltd.: Hoboken, NJ, USA, 2020; Volume 28, pp. 871–883. [Google Scholar] [CrossRef]
- Gilsbach, S.; Herpertz-Dahlmann, B.; Konrad, K. Psychological Impact of the COVID-19 Pandemic on Children and Adolescents With and Without Mental Disorders. Front. Public Health 2021, 9, 679041. [Google Scholar] [CrossRef] [PubMed]
- Cost, K.T.; Crosbie, J.; Anagnostou, E.; Birken, C.S.; Charach, A.; Monga, S.; Kelley, E.; Nicolson, R.; Maguire, J.L.; Burton, C.L.; et al. Mostly worse, occasionally better: Impact of COVID-19 pandemic on the mental health of Canadian children and adolescents. Eur. Child Adolesc. Psychiatry 2022, 31, 671–684. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Schmidt, S.C.E.; Anedda, B.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Nigg, C.; Niessner, C.; Oriwol, D.; Worth, A.; Woll, A. Physical activity and screen time of children and adolescents before and during the COVID-19 lockdown in Germany: A natural experiment. Sci. Rep. 2020, 10, 21780. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.H.; Chen, Y.C.; Chen, W.Y.; Chen, C.Y.; Hsu, W.Y.; Chou, Y.; Chang, Y.H. Weight gain associated with COVID-19 lockdown in children and adolescents: A systematic review and meta-analysis. Nutrients 2021, 13, 3668. [Google Scholar] [CrossRef] [PubMed]
- Stavridou, A.; Kapsali, E.; Panagouli, E.; Thirios, A.; Polychronis, K.; Bacopoulou, F.; Psaltopoulou, T.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Obesity in children and adolescents during COVID-19 pandemic. Children 2021, 8, 135. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L. Weight Stigma and the “Quarantine-15. ” Obesity 2020, 28, 1180–1181. [Google Scholar] [CrossRef]
- Mento, C.; Silvestri, M.C.; Muscatello, M.R.A.; Rizzo, A.; Celebre, L.; Praticò, M.; Zoccali, R.A.; Bruno, A. Psychological impact of pro-anorexia and pro-eating disorder websites on adolescent females: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 2186. [Google Scholar] [CrossRef]
- Rodgers, R.F.; Lombardo, C.; Cerolini, S.; Franko, D.L.; Omori, M.; Fuller-Tyszkiewicz, M.; Linardon, J.; Courtet, P.; Guillaume, S. The impact of the COVID-19 pandemic on eating disorder risk and symptoms. Int. J. Eat. Disord. 2020, 53, 1166–1170. [Google Scholar] [CrossRef] [PubMed]
- Baenas, I.; Etxandi, M.; Munguía, L.; Granero, R.; Mestre-Bac, G.; Sánchez, I.; Ortega, E.; Andreu, A.; Moize, V.L.; Fernández-Real, J.M.; et al. Impact of COVID-19 Lockdown in Eating Disorders: A Multicentre Collaborative International Study. Nutrients 2022, 14, 100. [Google Scholar] [CrossRef]


{kind=link}
| Mean Age | Years (SD) 15.1 (1.7), Range 12–18 | |
|---|---|---|
| Type of treatment | Current (n/%) | Before the onset of the COVID-19 pandemic (n/%) |
| None | 0 | 29/76.3 |
| Outpatient | 9/23.7 | 7/18.4 |
| Inpatient | 27/71.1 | 1/2.6 |
| Day patient | 1/2.6 | 0 |
| Home treatment | 1/2.6 | 0 |
| Not specified | 0 | 1/2.6 |
| Average length of treatment in months (SD) | - | 11.6 (16.3) range: 2–48 |
| Comorbidities (self-report) | ||
| Depressive symptoms | 12/31.6 | |
| Anxiety disorder | 5/13.2 | |
| Social phobia | 5/13.2 | |
| Obsessive–compulsive disorder | 2/5.3 | |
| Other | 3/7.9 | |
| More than one comorbidity | 10/26.3 |
| Pre | Current | |||||
|---|---|---|---|---|---|---|
| n = 38 | Mean | (SD) | Mean | (SD) | p | │d│ |
| BMI | 20.1 | (3.1) | 17.4 | (2.3) | <0.001 | 0.78 |
| Impact on ED symptoms (F1) | 11.8 | (5.4) | 18.2 | (5.2) | <0.001 | 0.99 |
| Changes—eating related style (F2) | 7.5 | (5.8) | 8 | (6.1) | 0.65 | 0.08 |
| Changes—depression/anxiety (F3) | 11.6 | (7.7) | 18.4 | (8.7) | <0.001 | 0.91 |
| Changes—emotional regulation (F4) | 5.8 | (3.7) | 8.5 | (5.0) | <0.001 | 0.98 |
| Pre | Current | |||||
|---|---|---|---|---|---|---|
| Mean | (SD) | Mean | (SD) | p | │d│ | |
| Engaging in social media glorifying AN (“pro-ANA”) | 0.3 | 1.0 | 0.6 | 1.1 | 0.016 | 0.41 |
| Following models and influencers on social media | 1.9 | 1.2 | 2.4 | 0.9 | 0.002 | 0.54 |
| Using apps for weight loss | 0.8 | 1.2 | 1.8 | 1.6 | 0.002 | 0.56 |
| Preoccupied with cooking recipes | 2.0 | 1.2 | 2.8 | 0.9 | 0.001 | 0.62 |
| Preoccupied with cooking | 2.3 | 0.8 | 2.6 | 1.2 | 0.201 | 0.21 |
| Mirror checking | 2.5 | 0.8 | 3.2 | 1.1 | <0.001 | 0.65 |
| Conflicts with parents—due to eating | 1.3 | 1.2 | 2.6 | 1.0 | <0.001 | 0.95 |
| Conflicts with parents—not due to eating | 1.7 | 0.7 | 1.7 | 1.0 | 0.474 | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilsbach, S.; Herpertz-Dahlmann, B. “What Made My Eating Disorder Worse?” The Impact of the COVID-19 Pandemic from the Perspective of Adolescents with Anorexia Nervosa. Nutrients 2023, 15, 1242. https://doi.org/10.3390/nu15051242
Gilsbach S, Herpertz-Dahlmann B. “What Made My Eating Disorder Worse?” The Impact of the COVID-19 Pandemic from the Perspective of Adolescents with Anorexia Nervosa. Nutrients. 2023; 15(5):1242. https://doi.org/10.3390/nu15051242
Chicago/Turabian StyleGilsbach, Susanne, and Beate Herpertz-Dahlmann. 2023. "“What Made My Eating Disorder Worse?” The Impact of the COVID-19 Pandemic from the Perspective of Adolescents with Anorexia Nervosa" Nutrients 15, no. 5: 1242. https://doi.org/10.3390/nu15051242
APA StyleGilsbach, S., & Herpertz-Dahlmann, B. (2023). “What Made My Eating Disorder Worse?” The Impact of the COVID-19 Pandemic from the Perspective of Adolescents with Anorexia Nervosa. Nutrients, 15(5), 1242. https://doi.org/10.3390/nu15051242