

Estimation of Glomerular Filtration Rate in Obese Patients: Utility of a New Equation
 ,
,
Abstract
1. Introduction
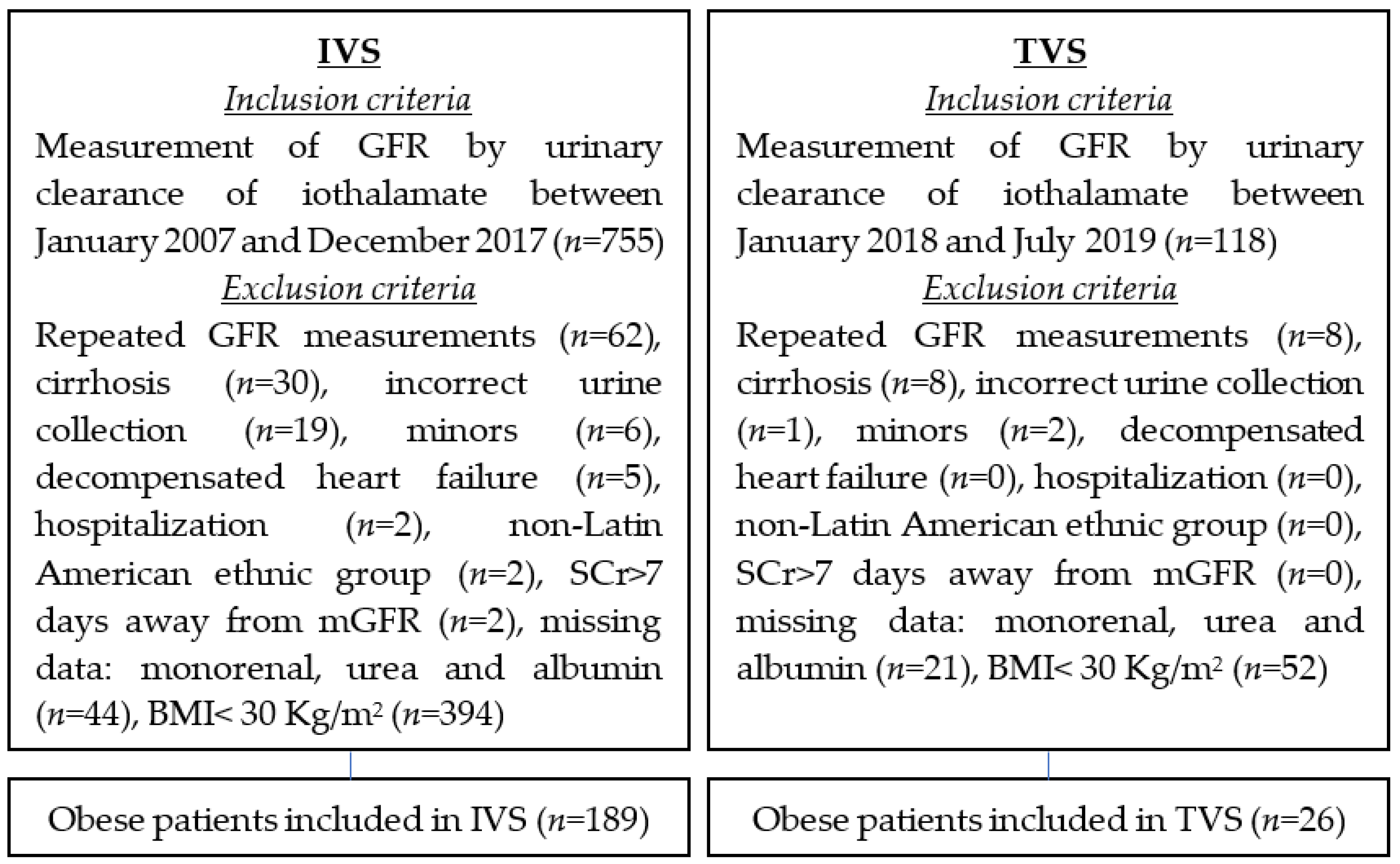
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The Global Obesity Pandemic: Shaped by Global Drivers and Local Environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, Regional, and National Prevalence of Overweight and Obesity in Children and Adults during 1980-2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Willett, W.C.; Dietz, W.H.; Colditz, G.A. Guidelines for Healthy Weight. N. Engl. J. Med. 1999, 341, 427–434. [Google Scholar] [CrossRef]
- Field, A.E.; Coakley, E.H.; Must, A.; Spadano, J.L.; Laird, N.; Dietz, W.H.; Rimm, E.; Colditz, G.A. Impact of Overweight on the Risk of Developing Common Chronic Diseases during a 10-Year Period. Arch. Intern. Med. 2001, 161, 1581–1586. [Google Scholar] [CrossRef]
- Hsu, C.; McCulloch, C.E.; Iribarren, C.; Darbinian, J.; Go, A.S. Body Mass Index and Risk for End-Stage Renal Disease. Ann. Intern. Med. 2006, 144, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Iseki, K.; Ikemiya, Y.; Kinjo, K.; Inoue, T.; Iseki, C.; Takishita, S. Body Mass Index and the Risk of Development of End-Stage Renal Disease in a Screened Cohort. Kidney Int. 2004, 65, 1870–1876. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, X.; Song, Y.; Caballero, B.; Cheskin, L.J. Association between Obesity and Kidney Disease: A Systematic Review and Meta-Analysis. Kidney Int. 2008, 73, 19–33. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.S.; Larson, M.G.; Leip, E.P.; Culleton, B.; Wilson, P.W.F.; Levy, D. Predictors of New-Onset Kidney Disease in a Community-Based Population. JAMA 2004, 291, 844–850. [Google Scholar] [CrossRef]
- Vivante, A.; Golan, E.; Tzur, D.; Leiba, A.; Tirosh, A.; Skorecki, K.; Calderon-Margalit, R. Body Mass Index in 1.2 Million Adolescents and Risk for End-Stage Renal Disease. Arch. Intern. Med. 2012, 172, 1644–1650. [Google Scholar] [CrossRef]
- D’Agati, V.D.; Chagnac, A.; de Vries, A.P.J.; Levi, M.; Porrini, E.; Herman-Edelstein, M.; Praga, M. Obesity-Related Glomerulopathy: Clinical and Pathologic Characteristics and Pathogenesis. Nat. Rev. Nephrol. 2016, 12, 453–471. [Google Scholar] [CrossRef]
- Smith, H.W. The Kidney: Structure and Function in Health and Disease; Oxford University Press: Oxford, UK, 1951. [Google Scholar]
- Elwood, C.M.; Sigman, E.M.; Treger, C. The Measurement of Glomerular Filtration Rate with 125I-Sodium Iothalamate (Conray). Br. J. Radiol. 1967, 40, 581–583. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Tighiouart, H.; Greene, T.; Inker, L.A. Measured and Estimated Glomerular Filtration Rate: Current Status and Future Directions. Nat. Rev. Nephrol. 2020, 16, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Cushen, S.J.; Orsso, C.E.; Ryan, A.M. Sarcopenia and Cachexia in the Era of Obesity: Clinical and Nutritional Impact. Proc. Nutr. Soc. 2016, 75, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Obesity: Preventing and Managing the Global Epidemic-World Health Organization-Google Libros. Available online: https://books.google.com.ar/books?hl=es&lr=&id=AvnqOsqv9doC&oi=fnd&pg=PA1&dq=12.%09World+Health+Organization.+Obesity:+preventing+and+managing+the+global+epidemic.+World+Health+Organization+2000.&ots=6WK04oZX9J&sig=0rvBh3liLHEnJY2Hwc3sp_5PmiA&redir_esc=y#v=onepage&q=12.%09World%20Health%20Organization.%20Obesity%3A%20preventing%20and%20managing%20the%20global%20epidemic.%20World%20Health%20Organization%202000.&f=false (accessed on 3 December 2022).
- Cockcroft, D.W.; Gault, M.H. Prediction of Creatinine Clearance from Serum Creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Janmahasatian, S.; Duffull, S.B.; Ash, S.; Ward, L.C.; Byrne, N.M.; Green, B. Quantification of Lean Bodyweight. Clin. Pharmacokinet. 2005, 44, 1051–1065. [Google Scholar] [CrossRef] [PubMed]
- Salazar, D.E.; Corcoran, G.B. Predicting Creatinine Clearance and Renal Drug Clearance in Obese Patients from Estimated Fat-Free Body Mass. Am. J. Med. 1988, 84, 1053–1060. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Chronic Kidney Disease Epidemiology Collaboration Using Standardized Serum Creatinine Values in the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C–Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- Fernández, P.; Chiurchiu, C.; de Arteaga, J.; Douthat, W.; Campazzo, M.; Lujan, P.; de la Fuente, J. Filtrado glomerular estimado por fórmulas en pacientes obesos. Nefrol. Latinoam. 2017, 14, 56–62. [Google Scholar] [CrossRef]
- Lombi, F.; Papaginovic, M.M.; Fayad, A.; Diez, G.R.; Lombi, F.; Papaginovic, M.M.; Fayad, A.; Diez, G.R. XXII Congreso Argentino de Nefrología CAN 2021. Rev. Nefrol. Dialisis Traspl. 2022, 42, 1–3. [Google Scholar]
- Dunn, P.K.; Smyth, G.K. (Eds.) Chapter 8: Generalized Linear Models: Diagnostics. In Generalized Linear Models with Examples in R; Springer: New York, NY, USA, 2018; pp. 297–331. ISBN 978-1-4419-0118-7. [Google Scholar]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. (Eds.) Resampling Methods. In An Introduction to Statistical Learning: With Applications in R; Springer: New York, NY, USA, 2013; pp. 175–201. ISBN 978-1-4614-7138-7. [Google Scholar]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 5–14. [Google Scholar]
- Abouchacra, S.; Chaaban, A.; Gebran, N.; Hussein, Q.; Ahmed, M.; Bernieh, B.; Torab, F.; Kayyal, Y.; Al Omary, H.; Nagelkerke, N. GFR Estimation in the Morbidly Obese Pre- and Postbariatric Surgery: One Size Does Not Fit All. Int. Urol. Nephrol. 2013, 45, 157–162. [Google Scholar] [CrossRef]
- Demirovic, J.A.; Pai, A.B.; Pai, M.P. Estimation of Creatinine Clearance in Morbidly Obese Patients. Am. J. Health-Syst. Pharm. 2009, 66, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Donker, E.M.; Bet, P.; Nurmohamed, A.; Serné, E.; Burchell, G.L.; Friedman, A.N.; Bouquegneau, A.; Lemoine, S.; Ebert, N.; Cirillo, M.; et al. Estimation of Glomerular Filtration Rate for Drug Dosing in Patients with Very High or Low Body Mass Index. Clin. Transl. Sci. 2022, 15, 2206–2217. [Google Scholar] [CrossRef]
- López-Martínez, M.; Luis-Lima, S.; Morales, E.; Navarro-Díaz, M.; Negrín-Mena, N.; Folgueras, T.; Escamilla, B.; Estupiñán, S.; Delgado-Mallén, P.; Marrero-Miranda, D.; et al. The Estimation of GFR and the Adjustment for BSA in Overweight and Obesity: A Dreadful Combination of Two Errors. Int. J. Obes. 2020, 44, 1129–1140. [Google Scholar] [CrossRef]
- Bouquegneau, A.; Vidal-Petiot, E.; Vrtovsnik, F.; Cavalier, E.; Rorive, M.; Krzesinski, J.-M.; Delanaye, P.; Flamant, M. Modification of Diet in Renal Disease versus Chronic Kidney Disease Epidemiology Collaboration Equation to Estimate Glomerular Filtration Rate in Obese Patients. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2013, 28 (Suppl. S4), iv122–iv130. [Google Scholar] [CrossRef] [PubMed]
- Bouquegneau, A.; Vidal-Petiot, E.; Moranne, O.; Mariat, C.; Boffa, J.-J.; Vrtovsnik, F.; Scheen, A.-J.; Krzesinski, J.-M.; Flamant, M.; Delanaye, P. Creatinine-Based Equations for the Adjustment of Drug Dosage in an Obese Population. Br. J. Clin. Pharmacol. 2016, 81, 349–361. [Google Scholar] [CrossRef]
- Guebre-Egziabher, F.; Brunelle, C.; Thomas, J.; Pelletier, C.C.; Normand, G.; Juillard, L.; Dubourg, L.; Lemoine, S. Estimated Glomerular Filtration Rate Bias in Participants with Severe Obesity Regardless of Deindexation. Obesity 2019, 27, 2011–2017. [Google Scholar] [CrossRef]
- Lemoine, S.; Guebre-Egziabher, F.; Sens, F.; Nguyen-Tu, M.-S.; Juillard, L.; Dubourg, L.; Hadj-Aissa, A. Accuracy of GFR Estimation in Obese Patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 720–727. [Google Scholar] [CrossRef]
- Delanaye, P.; Björk, J.; Courbebaisse, M.; Couzi, L.; Ebert, N.; Eriksen, B.O.; Dalton, R.N.; Dubourg, L.; Gaillard, F.; Garrouste, C.; et al. Performance of Creatinine-Based Equations to Estimate Glomerular Filtration Rate with a Methodology Adapted to the Context of Drug Dosage Adjustment. Br. J. Clin. Pharmacol. 2022, 88, 2118–2127. [Google Scholar] [CrossRef]
- Nacife, C.; Livino, P.; Fuhr, L.; Bezerra, R.; Teles, F. Assessment of Glomerular Filtration Rate by Formulas in Obese Patients: What Is the Best Choice? Clin. Nephrol. 2022, 98, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Busse, D.; Borghardt, J.M.; Petroff, D.; Pevzner, A.; Dorn, C.; El-Najjar, N.; Huisinga, W.; Wrigge, H.; Simon, P.; Kloft, C. Evaluating Prediction Methods for Glomerular Filtration to Optimise Drug Doses in Obese and Nonobese Patients. Br. J. Clin. Pharmacol. 2022, 88, 2973–2981. [Google Scholar] [CrossRef]
- Wedderburn, R.W.M. Quasi-Likelihood Functions, Generalized Linear Models, and the Gauss-Newton Method. Biometrika 1974, 61, 439–447. [Google Scholar] [CrossRef]
- Kaufman, J.M.; Siegel, N.J.; Hayslett, J.P. Functional and Hemodynamic Adaptation to Progressive Renal Ablation. Circ. Res. 1975, 36, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.M.; DiMeola, H.J.; Siegel, N.J.; Lytton, B.; Kashgarian, M.; Hayslett, J.P. Compensatory Adaptation of Structure and Function Following Progressive Renal Ablation. Kidney Int. 1974, 6, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Herrera, J.; Rodríguez-Iturbe, B. Stimulation of Tubular Secretion of Creatinine in Health and in Conditions Associated with Reduced Nephron Mass. Evidence for a Tubular Functional Reserve. Nephrol. Dial. Transplant. 1998, 13, 623–629. [Google Scholar] [CrossRef]
- Rodríguez-Iturbe, B.; Herrera, J.; Marín, C.; Mañalich, R. Tubular Stress Test Detects Subclinical Reduction in Renal Functioning Mass. Kidney Int. 2001, 59, 1094–1102. [Google Scholar] [CrossRef]
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef]
- Earley, A.; Miskulin, D.; Lamb, E.J.; Levey, A.S.; Uhlig, K. Estimating Equations for Glomerular Filtration Rate in the Era of Creatinine Standardization: A Systematic Review. Ann. Intern. Med. 2012, 156, 785–795. [Google Scholar] [CrossRef]
- Shen, C.; Landsittel, D.; Irazabal, M.V.; Yu, A.S.L.; Chapman, A.B.; Mrug, M.; Grantham, J.J.; Bae, K.T.; Bennett, W.M.; Flessner, M.F.; et al. Performance of the CKD-EPI Equation to Estimate GFR in a Longitudinal Study of Autosomal Dominant Polycystic Kidney Disease. Am. J. Kidney Dis. 2017, 69, 482–484. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Huang, H.; Yan, X.; Hapca, S.; Bell, S.; Qu, F.; Liu, L.; Chen, X.; Zhang, S.; Shi, Q.; et al. Glycated Haemoglobin A1c Variability Score Elicits Kidney Function Decline in Chinese People Living with Type 2 Diabetes. J. Clin. Med. 2022, 11, 6692. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Lucisano, G.; Prattichizzo, F.; Eliasson, B.; Franzén, S.; Svensson, A.-M.; Nicolucci, A. Variability in Body Weight and the Risk of Cardiovascular Complications in Type 2 Diabetes: Results from the Swedish National Diabetes Register. Cardiovasc. Diabetol. 2021, 20, 173. [Google Scholar] [CrossRef]
- Inserra, F.; Greloni, G. Nuevas ecuaciones basadas en creatinina y cistatina C para la TFGe, sin incluir raza. Rev. Nefrol. Diálisis Traspl. 2022, 42, 99–102. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | All (n = 215) | IVS (n = 189) | TVS (n = 26) | p |
|---|---|---|---|---|
| Age (years) a | 50 (40.2–59.8) | 50 (40.2–59.8) | 50.5 (41–59) | 0.840 |
| Female gender b Male gender b | 112 (52.1) 103 (47.9) | 100 (52.9) 89 (47.1) | 12 (46.2) 14 (53.8) | 0.518 |
| Body mass index (kg/m2) a | 33.3 (31.7–37.5) | 33.3 (31.6–37.7) | 32.7 (31.7–36.5) | 0.605 |
| Grade I obesity b Grade II obesity b Grade III obesity b | 129 (60) 54 (25.1) 32 (14.9) | 112 (59.2) 47 (24.9) 30 (15.9) | 17 (65.4) 7 (26.9) 2 (7.7) | 0.604 |
| Diabetes b | 37 (18.1) | 34 (19.1) | 3 (11.5) | 0.427 |
| Hypertension b | 96 (47.1) | 86 (48.3) | 10 (38.5) | 0.347 |
| Single kidney b | 19 (9.3) | 17 (9.6) | 2 (7.7) | 1 |
| Creatinine (mg/dL) a | 0.85 (0.71–1.1) | 0.84 (0.69–1.09) | 0.97 (0.82–1.18) | 0.019 |
| Urea (mg/dL) a | 31.1 (25.2–41.7) | 31.2 (25.2–41.7) | 30.3 (26.1–41.1) | 0.751 |
| Albumin (g/L) a | 4.2 (3.94–4.44) | 4.19 (3.94–4.43) | 4.34 (3.93–4.51) | 0.303 |
| mGFR (mL/min/1.73 m2) a | 91.2 (70.2–116.2) | 92.6 (71.6–117.3) | 80.2 (70.2–96.2) | 0.109 |
| mGFR < 60 mL/min/1.73 m2 b | 45 (20.9) | 39 (20.6) | 6 (23.1) | 0.774 |
| Equations | Bias (Q1/Q3) | P30 (%) | r (95% CI) | %CC |
|---|---|---|---|---|
| LBM_CG | −22.6 (−36.3/−4.5) | 65.3 | 0.74 (0.67–0.80) | 55.7 |
| SC | 5.1 (−7.8/21.9) | 76.1 | 0.73 (0.65–0.79) | 64.8 |
| MDRD4 | −8.4 (−18.9/6.3) | 81.8 | 0.81 (0.76–0.86) | 63.1 |
| MDRD6 | −7.3 (−18.4/5.8) | 83.5 | 0.83 (0.78–0.87) | 63.1 |
| CKD-MCQ | 3.7 (−8.6/12.2) | 78.9 | 0.86 (0.82–0.89) | 72.6 |
| CKD-EPI 2009 | −4.4 (−15.8/7.7) | 84 | 0.86 (0.81–0.89) | 70.4 |
| CKD-EPI 2021 | 0.5 (−11.3/11) | 82.4 | 0.86 (0.82–0.89) | 72.6 |
| AE | −0.4 (−11.5/10.2) | 85.2 | 0.86 (0.82–0.89) | 74.4 |
| Equations | Bias (Q1/Q3) | P30 (%) | r (95% CI) | %CC |
|---|---|---|---|---|
| Grade I obesity (n = 112) | ||||
| LBM_CG | −21.9 (−37.5/−5) | 63.1 | 0.83 (0.75–0.88) | 54.4 |
| SC | 1.8 (−10.6/15.4) | 79.6 | 0.83 (0.76–0.88) | 66 |
| MDRD4 | −8.7 (−20.9/5) | 83.5 | 0.85 (0.79–0.90) | 63.1 |
| MDRD6 | −6.7 (−18.4/5.2) | 85.4 | 0.87 (0.81–0.91) | 62.1 |
| CKD-MCQ | 2.9 (−8.6/10.2) | 81.6 | 0.89 (0.84–0.92) | 75.7 |
| CKD-EPI 2009 | −4.6 (−16.3/6.8) | 86.4 | 0.88 (0.83–0.92) | 71.8 |
| CKD-EPI 2021 | 0.6 (−11.7/9.9) | 83.5 | 0.89 (0.84–0.92) | 72.8 |
| AE | −0.4 (−11.2/8.7) | 87.4 | 0.89 (0.84–0.92) | 74.8 |
| Grade II obesity (n = 47) | ||||
| LBM_CG | −26.1 (−39/−9.1) | 62.2 | 0.77 (0.61–0.87) | 60 |
| SC | 4.5 (−11.6/21.8) | 77.8 | 0.77 (0.62–0.87) | 66.7 |
| MDRD4 | −13.2 (−18.9/5.2) | 77.8 | 0.81 (0.68–0.89) | 64.4 |
| MDRD6 | −8.9 (−19.5/3.5) | 82.2 | 0.86 (0.77–0.92) | 68.9 |
| CKD-MCQ | 2 (−9/9.4) | 82.2 | 0.89 (0.80–0.94) | 73.3 |
| CKD-EPI 2009 | −6.1 (−17.3/4.2) | 84.4 | 0.88 (0.80–0.93) | 75.6 |
| CKD-EPI 2021 | −1.9 (−12.8/7.1) | 84.4 | 0.88 (0.80–0.93) | 75.6 |
| AE | −3 (−14.6/7.4) | 82.2 | 0.88 (0.79–0.93) | 75.6 |
| Grade III obesity (n = 30) | ||||
| LBM_CG | −16.2 (−29/5.7) | 78.6 | 0.64 (0.34–0.82) | 57.1 |
| SC | 23.4 (8.7/44.7) | 60.7 | 0.61 (0.31–0.80) | 57.1 |
| MDRD4 | −2.5 (−13.1/13.3) | 78.6 | 0.69 (0.43–0.85) | 64.3 |
| MDRD6 | −4.4 (−13.8/12.1) | 78.6 | 0.64 (0.35–0.82) | 60.7 |
| CKD-MCQ | 9.9 (−2.7/30.4) | 64.3 | 0.74 (0.51–0.87) | 64.3 |
| CKD-EPI 2009 | 2.6 (−9.3/18.7) | 75 | 0.76 (0.54–0.88) | 60.7 |
| CKD-EPI 2021 | 6.3 (−5.4/22.5) | 75 | 0.76 (0.55–0.89) | 67.9 |
| AE | 4.2 (−10.1/22.3) | 82.1 | 0.71 (0.46–0.86) | 67.9 |
| Equations | Bias (Q1/Q3) | P30 (%) | r (95% CI) | %CC |
|---|---|---|---|---|
| LBM_CG | −21.5 (−30.9/−10.6) | 61.5 | 0.89 (0.78–0.95) | 69.2 |
| SC | 1.6 (−10.5/13.6) | 84.6 | 0.89 (0.77–0.95) | 73.1 |
| MDRD4 | −11.3 (−16.4/0.6) | 80.8 | 0.87 (0.73–0.94) | 65.4 |
| MDRD6 | −6.6 (−14.1/2.2) | 88.5 | 0.86 (0.71–0.94) | 65.4 |
| CKD-MCQ | 5.4 (−1.1/12.2) | 84.6 | 0.89 (0.77–0.95) | 80.8 |
| CKD-EPI 2009 | −3.9 (−10.9/7.1) | 84.6 | 0.87 (0.74–0.94) | 73.1 |
| CKD-EPI 2021 | 1.1 (−6.8/12.1) | 84.6 | 0.89 (0.76–0.95) | 84.6 |
| AE | 2.6 (−4.3/8.6) | 88.5 | 0.89 (0.78–0.95) | 84.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández, P.; Nores, M.L.; Douthat, W.; de Arteaga, J.; Luján, P.; Campazzo, M.; de La Fuente, J.; Chiurchiu, C. Estimation of Glomerular Filtration Rate in Obese Patients: Utility of a New Equation. Nutrients 2023, 15, 1233. https://doi.org/10.3390/nu15051233
Fernández P, Nores ML, Douthat W, de Arteaga J, Luján P, Campazzo M, de La Fuente J, Chiurchiu C. Estimation of Glomerular Filtration Rate in Obese Patients: Utility of a New Equation. Nutrients. 2023; 15(5):1233. https://doi.org/10.3390/nu15051233
Chicago/Turabian StyleFernández, Pehuén, María Laura Nores, Walter Douthat, Javier de Arteaga, Pablo Luján, Mario Campazzo, Jorge de La Fuente, and Carlos Chiurchiu. 2023. "Estimation of Glomerular Filtration Rate in Obese Patients: Utility of a New Equation" Nutrients 15, no. 5: 1233. https://doi.org/10.3390/nu15051233
APA StyleFernández, P., Nores, M. L., Douthat, W., de Arteaga, J., Luján, P., Campazzo, M., de La Fuente, J., & Chiurchiu, C. (2023). Estimation of Glomerular Filtration Rate in Obese Patients: Utility of a New Equation. Nutrients, 15(5), 1233. https://doi.org/10.3390/nu15051233