
25 Hydroxyvitamin D Serum Concentration and COVID-19 Severity and Outcome—A Retrospective Survey in a Romanian Hospital

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Vitamin D Analysis
2.4. Variables
2.5. Statistical Analyses
3. Results
3.1. Patients Characteristics
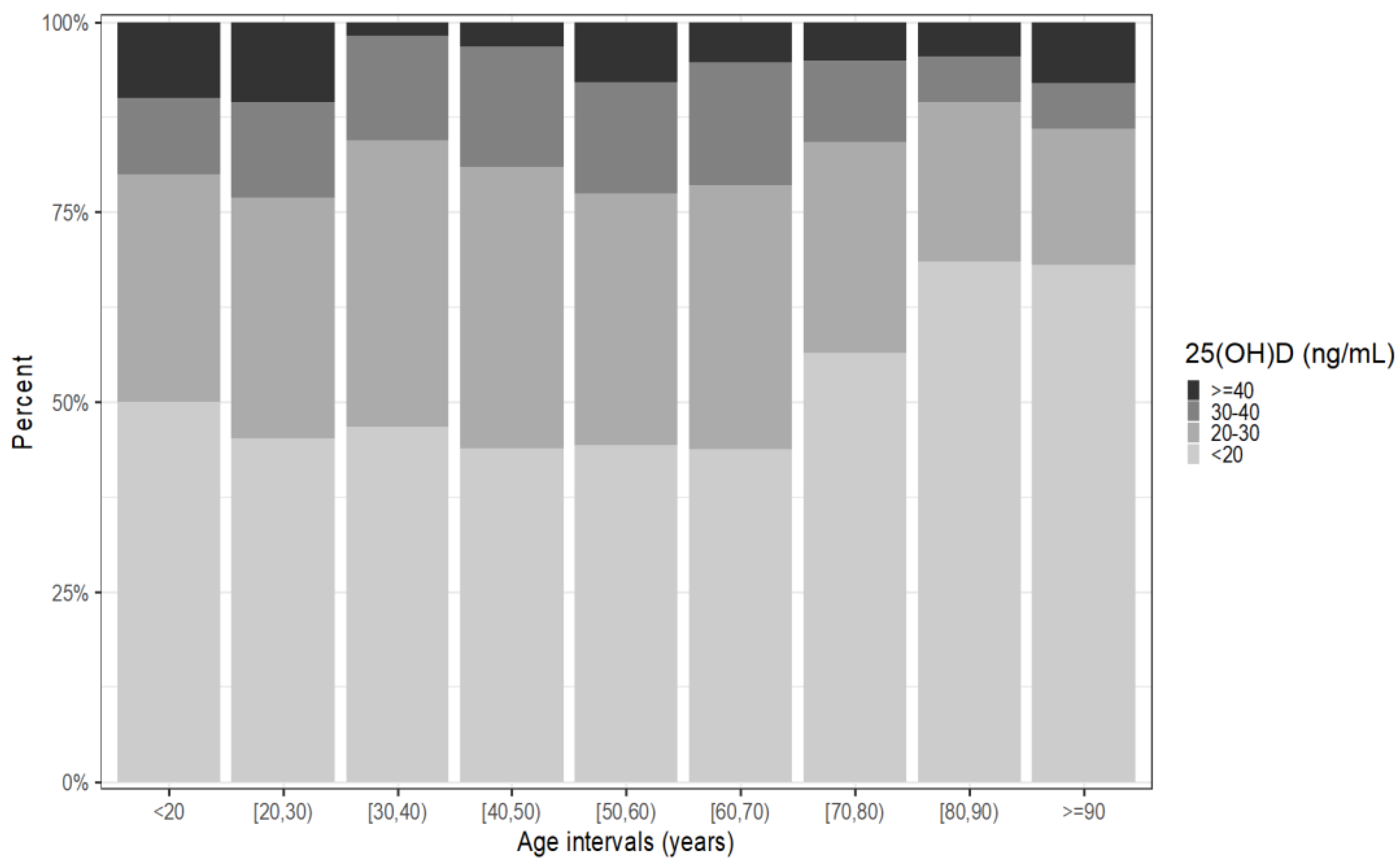
3.2. 25(OH)D and Age
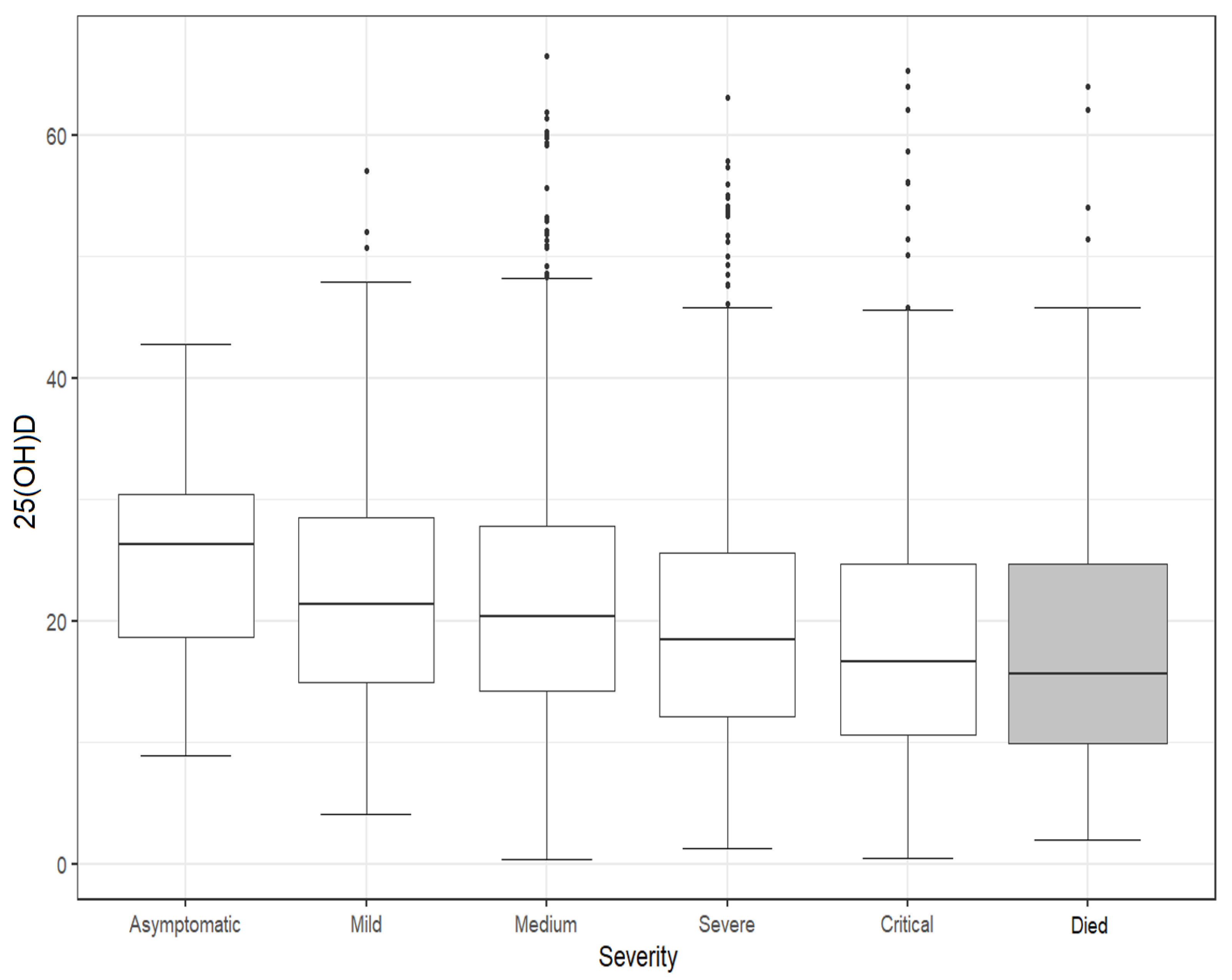
3.3. 25(OH)D According to COVID-19 Severity and Death Outcome
3.4. Multivariate Analyses Predicting Severe/Critical COVID-19, ICU Needs, and Death
4. Discussion
Limitations and Strength
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 22 January 2023).
- World Health Organization. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---25-january-2023 (accessed on 1 February 2023).
- World Health Organization. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2023.1 (accessed on 1 February 2023).
- UK Health Security Agency. COVID-19 Vaccine Surveillance Report. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1050721/Vaccine-surveillance-report-week-4.pdf (accessed on 3 December 2022).
- Thompson, M.G.; Natarajan, K.; Irving, S.A.; Rowley, E.A.; Griggs, E.P.; Gaglani, M.; Klein, N.P.; Grannis, S.J.; DeSilva, M.B.; Stenehjem, E.; et al. Effectiveness of a Third Dose of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal Wkly. Rep. 2022, 71, 139–145. [Google Scholar]
- Harrison, S.L.; Buckley, B.J.R.; Rivera-Caravaca, J.M.; Zhang, J.; Lip, G.Y.H. Cardiovascular risk factors, cardiovascular disease, and COVID-19: An umbrella review of systematic reviews. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 330–339. [Google Scholar] [CrossRef]
- Seneviratne, S.L.; Wijerathne, W.; Yasawardene, P.; Somawardana, B. COVID-19 in cancer patients. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 767–797. [Google Scholar] [CrossRef] [PubMed]
- Seidu, S.; Gillies, C.; Zaccardi, F.; Kunutsor, S.K.; Hartmann-Boyce, J.; Yates, T.; Singh, A.K.; Davies, M.J.; Khunti, K. The impact of obesity on severe disease and mortality in people with SARS-CoV-2: A systematic review and meta-analysis. Endocrinol. Diabetes Metab. 2020, 4, e00176. [Google Scholar] [CrossRef]
- Our World in Data. Available online: https://ourworldindata.org/mortality-risk-covid (accessed on 1 February 2023).
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The health effects of vitamin D supplementation: Evidence from human studies. Nat. Rev. Endocrinol. 2022, 18, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D metabolism, mechanism of action, and clinical applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority EEFS. Scientific opinion on dietary reference values for vitamin D. EFSA J. 2016, 14, 4547. [Google Scholar]
- Cianferotti, L.; Bertoldo, F.; Bischoff-Ferrari, H.A.; Bruyere, O.; Cooper, C.; Cutolo, M.; Kanis, J.A.; Kaufman, J.M.; Reginster, J.Y.; Rizzoli, R.; et al. Vitamin D supplementation in the prevention and management of major chronic diseases not related to mineral homeostasis in adults: Research for evidence and a scientific statement from the European society for clinical and economic aspects of osteoporosis and osteoarthritis (ESCEO). Endocrine 2017, 56, 245–261. [Google Scholar]
- Pike, J.W.; Meyer, M.B.; Lee, S.M.; Onal, M.; Benkusky, N.A. The vitamin D receptor: Contemporary genomic approaches reveal new basic and translational insights. J. Clin. Investig. 2017, 127, 1146–1154. [Google Scholar] [CrossRef]
- Aranow, C. Vitamin D and the immune system. J. Investig. Med. 2011, 59, 881–886. [Google Scholar] [CrossRef]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Martineau, A.R.; Cantorna, M.T. Vitamin D for COVID-19: Where are we now? Nat. Rev. Immunol. 2022, 22, 529–530. [Google Scholar] [CrossRef]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 illness in native and immunosuppressed states: A clinical-therapeutic staging proposal. J. Heart Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [PubMed]
- Urashima, M.; Segawa, T.; Okazaki, M.; Kurihara, M.; Wada, Y.; Ida, H. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am. J. Clin. Nutr. 2010, 91, 1255–1260. [Google Scholar] [CrossRef]
- Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/publications/i/item/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19) (accessed on 1 February 2022).
- International Statistical Classification of Diseases and Related Health Problems 10th Revision. Available online: https://icd.who.int/browse10/2016/en#/ (accessed on 2 February 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; ISBN 3-900051-07-0. Available online: http://www.R-project.org/ (accessed on 29 August 2022).
- Ferrari, D.; Locatelli, M.; Briguglio, M.; Lombardi, G. Is there a link between vitamin D status, SARS-CoV-2 infection risk and COVID-19 severity? Cell Biochem. Funct. 2021, 39, 35–47. [Google Scholar] [CrossRef]
- Munshi, R.; Hussein, M.H.; Toraih, E.A.; Elshazli, R.M.; Jardak, C.; Sultana, N.; Youssef, M.R.; Omar, M.; Attia, A.S.; Fawzy, M.S.; et al. Vitamin D insufficiency as a potential culprit in critical COVID-19 patients. J. Med. Virol. 2021, 93, 733–740. [Google Scholar] [CrossRef]
- Chiodini, I.; Gatti, D.; Soranna, D.; Merlotti, D.; Mingiano, C.; Fassio, A.; Adami, G.; Falchetti, A.; Eller-Vainicher, C.; Rossini, M.; et al. Vitamin D Status and SARS-CoV-2 Infection and COVID-19 Clinical Outcomes. Front. Public Health 2021, 9, 736665. [Google Scholar] [CrossRef]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Alcalá Díaz, J.F.; López Miranda, J.; Bouillon, R.; Quesada Gomez, J.M. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid. Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef]
- Cereda, E.; Bogliolo, L.; Lobascio, F.; Barichella, M.; Zecchinelli, A.L.; Pezzoli, G.; Caccialanza, R. Vitamin D supplementation and outcomes in coronavirus disease 2019 (COVID-19) patients from the outbreak area of Lombardy, Italy. Nutrition 2021, 82, 111055. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Mei, K.; Xie, L.; Yuan, P.; Ma, J.; Yu, P.; Zhu, W.; Zheng, C.; Liu, X. Low 25(OH)D concentration do not aggravate COVID-19 risk or death, and vitamin D supplementation does not improve outcomes in hospitalized patients with COVID-19: A meta-analysis and GRADE assessment of cohort studies and RCTs. Nutr. J. 2021, 20, 89. [Google Scholar] [CrossRef]
- Dissanayake, H.A.; de Silva, N.L.; Sumanatilleke, M.; de Silva, S.D.N.; Gamage, K.K.K.; Dematapitiya, C.; Kuruppu, D.C.; Ranasinghe, P.; Pathmanathan, S.; Katulanda, P. Prognostic and Therapeutic Role of Vitamin D in COVID-19: Systematic Review and Meta-analysis. J. Clin. Endocrinol. Metab. 2022, 107, 1484–1502. [Google Scholar] [CrossRef]
- Hosseini, B.; El Abd, A.; Ducharme, F.M. Effects of Vitamin D Supplementation on COVID-19 Related Outcomes: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2134. [Google Scholar] [CrossRef]
- Argano, C.; Mallaci Bocchio, R.; Natoli, G.; Scibetta, S.; Lo Monaco, M.; Corrao, S. Protective Effect of Vitamin D Supplementation on COVID-19-Related Intensive Care Hospitalization and Mortality: Definitive Evidence from Meta-Analysis and Trial Sequential Analysis. Pharmaceuticals 2023, 16, 130. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe:pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Berisha, A.T.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Daly, R.M.; Gagnon, C.; Lu, Z.X.; Magliano, D.J.; Dunstan, D.W.; Sikaris, K.A.; Zimmet, P.Z.; Ebeling, P.R.; Shaw, J.E. Prevalence of vitamin D deficiency and its determinants in Australian adults aged 25 years and older: A national, population-based study. Clin. Endocrinol. 2012, 77, 26–35. [Google Scholar] [CrossRef]
- Chirita-Emandi, A.; Socolov, D.; Haivas, C.; Calapiș, A.; Gheorghiu, C.; Puiu, M. Vitamin D Status: A Different Story in the Very Young versus the Very Old Romanian Patients. PLoS ONE 2015, 10, e0128010. [Google Scholar] [CrossRef] [PubMed]
- Niculescu, D.A.; Capatina, C.A.M.; Dusceac, R.; Caragheorgheopol, A.; Ghemigian, A.; Poiana, C. Seasonal variation of serum 25(OH)D concentration in Romania. Arch Osteoporos 2017, 12, 113. [Google Scholar] [CrossRef] [PubMed]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L.; Stepan, J.; El-Hajj Fuleihan, G.; Bouillon, R. Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: A position statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 1, P23–P54. [Google Scholar] [CrossRef]
- Avdeeva, V.A.; Suplotova, L.A.; Pigarova, E.A.; Rozhinskaya, L.Y.; Troshina, E.A. Vitamin D deficiency in Russia: The first results of a registered, non-interventional study of the frequency of vitamin D deficiency and insufficiency in various geographic regions of the country. Probl. Endokrinol. 2021, 67, 84–92. [Google Scholar] [CrossRef]
- Kupisz-Urbańska, M.; Płudowski, P.; Marcinowska-Suchowierska, E. Vitamin D Deficiency in Older Patients-Problems of Sarcopenia, Drug Interactions, Management in Deficiency. Nutrients 2021, 13, 1247. [Google Scholar] [CrossRef] [PubMed]
- de la Guía-Galipienso, F.; Martínez-Ferran, M.; Vallecillo, N.; Lavie, C.J.; Sanchis-Gomar, F.; Pareja-Galeano, H. Vitamin D and cardiovascular health. Clin. Nutr. 2021, 40, 2946–2957. [Google Scholar] [CrossRef]
- Scragg, R.; Sowers, M.; Bell, C. Serum 25-hydroxyvitamin D, Ethnicity, and Blood Pressure in the Third National Health and Nutrition Examination Survey. Am. J. Hypertens. 2007, 20, 713–719. [Google Scholar] [CrossRef]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D Deficiency and Risk of Cardiovascular Disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Levy, D.; Vasan, R.S.; Wang, T.J. The Framingham Heart Study and the epidemiology of cardiovascular disease: A historical perspective. Lancet 2014, 383, 999–1008. [Google Scholar] [CrossRef]
- Witte, K.K.; Byrom, R.; Gierula, J.; Paton, M.F.; Jamil, H.A.; Lowry, J.E.; Gillott, R.G.; Barnes, S.A.; Chumun, H.; Kearney, L.C.; et al. Effects of Vitamin D on Cardiac Function in Patients With Chronic HF: The VINDICATE Study. J. Am. Coll. Cardiol. 2016, 67, 2593–2603. [Google Scholar] [CrossRef] [PubMed]
- Pál, É.; Ungvári, Z.; Benyó, Z.; Várbíró, S. Role of Vitamin D Deficiency in the Pathogenesis of Cardiovascular and Cerebrovascular Diseases. Nutrients 2023, 15, 334. [Google Scholar] [CrossRef]
- Garland, C.F.; Gorham, E.D.; Mohr, S.B.; Garland, F.C. Vitamin D for cancer prevention: Global perspective. Ann. Epidemiol. 2009, 19, 468–483. [Google Scholar] [CrossRef]
- Giovannucci, E. The epidemiology of vitamin D and cancer incidence and mortality: A review (United States). Cancer Causes Control 2005, 16, 83–95. [Google Scholar] [CrossRef]
- Virtanen, J.K.; Nurmi, T.; Aro, A.; Bertone-Johnson, E.R.; Hyppönen, E.; Kröger, H.; Lamberg-Allardt, C.; Manson, J.E.; Mursu, J.; Mäntyselkä, P.; et al. Vitamin D supplementation and prevention of cardiovascular disease and cancer in the Finnish Vitamin D Trial: A randomized controlled trial. Am. J. Clin. Nutr. 2022, 115, 1300–1310. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Arora, S.; Khan, S.; Mohsin, M.; Mohan, A.; Manda, K.; Syed, M.A. Vitamin D and its therapeutic relevance in pulmonary diseases. J. Nutr. Biochem. 2021, 90, 108571. [Google Scholar] [CrossRef] [PubMed]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Santos, M.; Costa, P.R.; Assis, A.M.; Santos, C.A.; Santos, D.B. Obesity and vitamin D deficiency: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef]
- Vranić, L.; Mikolašević, I.; Milić, S. Vitamin D Deficiency: Consequence or Cause of Obesity? Medicina 2019, 55, 541. [Google Scholar] [CrossRef]
- Buckley, L.; Guyatt, G.; Fink, H.A.; Cannon, M.; Grossman, J.; Hansen, K.E.; Humphrey, M.B.; Lane, N.E.; Magrey, M.; Miller, M.; et al. 2017 American College of Rheumatology Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. Arthritis Rheumatol. 2017, 69, 1521–1537. [Google Scholar] [CrossRef]
- Kim, D. The Role of Vitamin D in Thyroid Diseases. Int. J. Mol. Sci. 2017, 18, 1949. [Google Scholar] [CrossRef]
- Galușca, D.; Popoviciu, M.S.; Babeș, E.E.; Vidican, M.; Zaha, A.A.; Babeș, V.V.; Jurca, A.D.; Zaha, D.C.; Bodog, F. Vitamin D Implications and Effect of Supplementation in Endocrine Disorders: Autoimmune Thyroid Disorders (Hashimoto’s Disease and Grave’s Disease), Diabetes Mellitus and Obesity. Medicina 2022, 58, 194. [Google Scholar] [CrossRef]
- Bennouar, S.; Cherif, A.B.; Kessira, A.; Bennouar, D.E.; Abdi, S. Vitamin D deficiency and low serum calcium as predictors of poor prognosis in patients with severe COVID-19. J. Am. Coll. Nutr. 2021, 40, 104–110. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Sahraian, M.A.; Ebrahimi, M.; Pazoki, M.; Kafan, S.; Tabriz, H.M.; Hadadi, A.; Montazeri, M.; Nasiri, M.; Shirvani, A.; et al. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLoS ONE 2020, 15, e0239799. [Google Scholar] [CrossRef]
- Our World in Data. Available online: https://ourworldindata.org/coronavirus/country/romania#daily-confirmed-deaths-how-do-they-compare-to-other-countries (accessed on 1 February 2023).
- Infante, M.; Buoso, A.; Pieri, M.; Lupisella, S.; Nuccetelli, M.; Bernardini, S.; Fabbri, A.; Iannetta, M.; Andreoni, M.; Colizzi, V.; et al. Low Vitamin D Status at Admission as a Risk Factor for Poor Survival in Hospitalized Patients With COVID-19: An Italian Retrospective Study. J. Am. Nutr. Assoc. 2022, 41, 250–265. [Google Scholar] [CrossRef]
- De Smet, D.; De Smet, K.; Herroelen, P.; Gryspeerdt, S.; Martens, G.A. Serum 25(OH)D Level on Hospital Admission Associated With COVID-19 Stage and Mortality. Am. J. Clin. Pathol. 2021, 155, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. [Google Scholar] [CrossRef] [PubMed]
- Huțanu, A.; Georgescu, A.M.; Voidăzan, S.; Andrejkovits, A.V.; Negrea, V.; Dobreanu, M. Low Serum Vitamin D in COVID-19 Patients Is Not Related to Inflammatory Markers and Patients’ Outcomes—A Single-Center Experience and a Brief Review of the Literature. Nutrients 2022, 14, 1998. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-COVID-19—8-February-2022 (accessed on 21 January 2023).



{kind=link}
{kind=link}
| Characteristics | All (n = 2342) | 25(OH)D < 20 ng/mL (n = 1194) | 25(OH)D ≥ 20 ng/mL (n = 1148) | p |
|---|---|---|---|---|
| Age (years), median (IQR) | 65 (50–75) | 68 (52–78) | 62 (48–72) | <0.001 |
| Age ≥ 65 years (Yes), n (%) | 1172 (50.04) | 663 (55.53) | 509 (44.34) | <0.001 |
| Sex, n (%) | 0.075 | |||
| Female | 1282 (54.74) | 675 (56.53) | 607 (52.87) | |
| Male | 1060 (45.26) | 519 (43.47) | 541 (47.13) | |
| Cardiovascular, n (%) | 1412 (60.29) | 769 (64.41) | 643 (56.01) | <0.001 |
| Neurological, n (%) | 297 (12.68) | 212 (17.76) | 85 (7.4) | <0.001 |
| Diabetes, n (%) | 509 (21.73) | 283 (23.7) | 226 (19.69) | 0.019 |
| Cancer, n (%) | 197 (8.41) | 115 (9.63) | 82 (7.14) | 0.03 |
| Pulmonary, n (%) | 287 (12.25) | 168 (14.07) | 119 (10.37) | 0.006 |
| Obesity, n (%) | 689 (29.42) | 348 (29.15) | 341 (29.7) | 0.767 |
| Rheumatological, n (%) | 77 (3.29) | 41 (3.43) | 36 (3.14) | 0.686 |
| Endocrine, n (%) | 176 (7.51) | 63 (5.28) | 113 (9.84) | <0.001 |
| Hepatic, n (%) | 127 (5.42) | 66 (5.53) | 61 (5.31) | 0.819 |
| Renal, n (%) | 145 (6.19) | 83 (6.95) | 62 (5.4) | 0.12 |
| ICU stay, n (%) | 271 (11.57) | 157 (13.15) | 114 (9.93) | 0.015 |
| Died, n (%) | 179 (7.64) | 118 (9.88) | 61 (5.31) | <0.001 |
| Severe/critical COVID-19, n (%) | 992 (42.36) | 560 (46.9) | 432 (37.63) | <0.001 |
| Vaccinated, n (%) | 495 (21.14) | 254 (21.27) | 241 (20.99) | 0.868 |
| Doses, n (%) | 0.991 | |||
| 0: | 0: 1847 (78.9) | 940 (78.73) | 907 (79.08) | |
| 1: | 1: 61 (2.61) | 31 (2.6) | 30 (2.62) | |
| 2: | 2: 330 (14.1) | 171 (14.32) | 159 (13.86) | |
| 3: | 3: 103 (4.4) | 52 (4.36) | 51 (4.45) |
| Characteristics | OR Adjusted | (95% CI) | p-Value |
|---|---|---|---|
| Age ≥ 65 years | 1.74 | (1.42–2.13) | <0.001 |
| Cardiovascular | 1.86 | (1.52–2.28) | <0.001 |
| Diabetes | 1.56 | (1.25–1.93) | <0.001 |
| Obesity | 1.79 | (1.47–2.18) | <0.001 |
| Pulmonary diseases | 1.3 | (1–1.7) | 0.051 |
| Renal diseases | 1.74 | (1.21–2.52) | 0.003 |
| Hepatic diseases | 1.11 | (0.76–1.63) | 0.576 |
| Rheumatic diseases | 1.57 | (0.97–2.56) | 0.068 |
| Neurological diseases | 1.84 | (1.4–2.42) | <0.001 |
| Cancer | 1.32 | (0.96–1.81) | 0.092 |
| Vaccine Doses (1 vs. 0) | 0.53 | (0.29–0.93) | 0.03 |
| Vaccine Doses (2 vs. 0) | 0.54 | (0.41–0.7) | <0.001 |
| Vaccine Doses (3 vs. 0) | 0.27 | (0.16–0.45) | <0.001 |
| Vitamin D (ng/mL) (<20 vs. ≥20) | 1.23 | (1.03–1.47) | 0.023 |
| Characteristics | OR Adjusted | (95% CI) | p-Value |
|---|---|---|---|
| Age ≥ 65 years | 2.91 | (1.92–4.52) | <0.001 |
| Cardiovascular | 2.37 | (1.53–3.78) | <0.001 |
| Diabetes | 1.12 | (0.78–1.59) | 0.518 |
| Obesity | 1.41 | (0.97–2.02) | 0.066 |
| Pulmonary diseases | 1.18 | (0.75–1.8) | 0.459 |
| Renal diseases | 1.75 | (1.03–2.87) | 0.03 |
| Hepatic diseases | 1.01 | (0.46–1.97) | 0.975 |
| Rheumatic diseases | 0.68 | (0.2–1.71) | 0.471 |
| Neurological diseases | 2.05 | (1.38–3) | <0.001 |
| Cancer | 1.69 | (1–2.75) | 0.042 |
| Vaccine Doses (1 vs. 0) | 0.79 | (0.23–2.05) | 0.671 |
| Vaccine Doses (2 vs. 0) | 0.53 | (0.3–0.89) | 0.024 |
| Vaccine Doses (3 vs. 0) | 0.59 | (0.22–1.3) | 0.233 |
| 25(OH)D (ng/mL) (<20 vs. ≥20) | 1.49 | (1.06–2.08) | 0.02 |
| Characteristics | OR Adjusted | (95% CI) | p-Value |
|---|---|---|---|
| Age ≥ 65 years | 1.04 | (0.77–1.4) | 0.81 |
| Cardiovascular | 1.83 | (1.33–2.52) | <0.001 |
| Diabetes | 1.22 | (0.9–1.64) | 0.189 |
| Obesity | 1.77 | (1.33–2.35) | <0.001 |
| Pulmonary diseases | 1.55 | (1.08–2.2) | 0.015 |
| Renal diseases | 1.92 | (1.2–2.98) | 0.005 |
| Hepatic diseases | 1.09 | (0.6–1.87) | 0.762 |
| Rheumatic diseases | 0.69 | (0.26–1.49) | 0.391 |
| Neurological diseases | 1.91 | (1.33–2.71) | <0.001 |
| Cancer | 1.6 | (1.01–2.47) | 0.037 |
| Vaccine Doses (1 vs. 0) | 0.7 | (0.26–1.54) | 0.417 |
| Vaccine Doses (2 vs. 0) | 0.59 | (0.38–0.88) | 0.013 |
| Vaccine Doses (3 vs. 0) | 0.13 | (0.02–0.4) | 0.004 |
| Vitamin D (ng/mL) (<20 vs. ≥20) | 1.18 | (0.90–1.54) | 0.235 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Topan, A.; Lupse, M.; Calin, M.; Jianu, C.; Leucuta, D.-C.; Briciu, V. 25 Hydroxyvitamin D Serum Concentration and COVID-19 Severity and Outcome—A Retrospective Survey in a Romanian Hospital. Nutrients 2023, 15, 1227. https://doi.org/10.3390/nu15051227
Topan A, Lupse M, Calin M, Jianu C, Leucuta D-C, Briciu V. 25 Hydroxyvitamin D Serum Concentration and COVID-19 Severity and Outcome—A Retrospective Survey in a Romanian Hospital. Nutrients. 2023; 15(5):1227. https://doi.org/10.3390/nu15051227
Chicago/Turabian StyleTopan, Adriana, Mihaela Lupse, Mihai Calin, Cristian Jianu, Daniel-Corneliu Leucuta, and Violeta Briciu. 2023. "25 Hydroxyvitamin D Serum Concentration and COVID-19 Severity and Outcome—A Retrospective Survey in a Romanian Hospital" Nutrients 15, no. 5: 1227. https://doi.org/10.3390/nu15051227
APA StyleTopan, A., Lupse, M., Calin, M., Jianu, C., Leucuta, D.-C., & Briciu, V. (2023). 25 Hydroxyvitamin D Serum Concentration and COVID-19 Severity and Outcome—A Retrospective Survey in a Romanian Hospital. Nutrients, 15(5), 1227. https://doi.org/10.3390/nu15051227