

Twelve-Month Outcomes in Patients with Obesity Following Bariatric Surgery—A Single Centre Experience
 ,
, 
 , and
, and
Abstract
1. Introduction
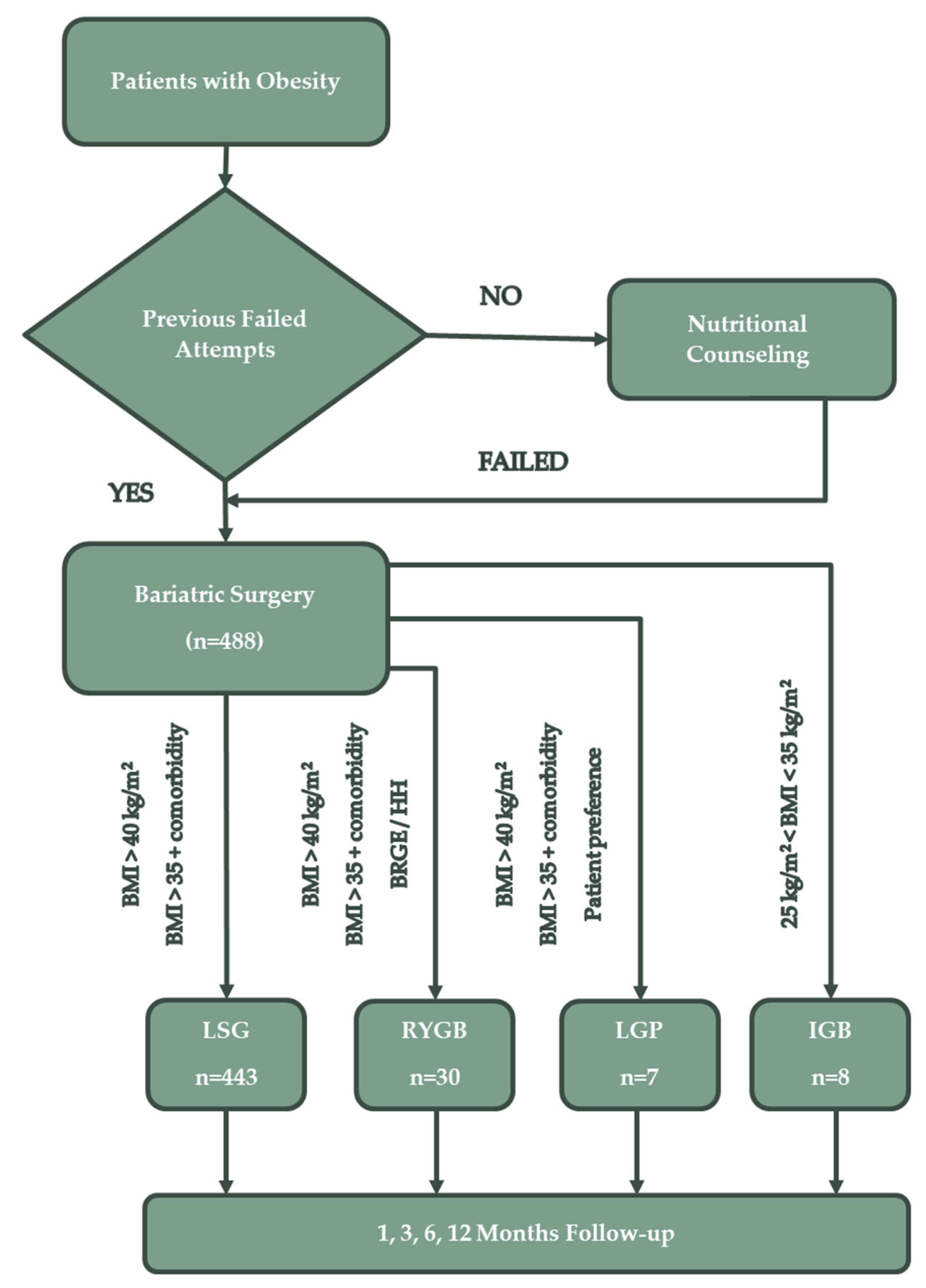
2. Materials and Methods
- patients with a BMI > 40 kg/m2 with or without coexisting medical conditions and who do not present a high anaesthetic-surgical risk;
- patients with a BMI > 34.9 kg/m2 with one or more obesity-related comorbidities or with a significant impairment in quality of life (T2DM, essential hypertension, dyslipidaemia, sleep apnoea syndrome or non-alcoholic fatty liver disease—NAFLD);
- patients over 18 years old.
3. Results
3.1. Patient Distribution
3.2. Demographic Characteristics
3.3. Distribution by Type of Procedure Performed
3.4. Preoperative Comorbidities and Morphologic Characteristics
3.5. Outcomes
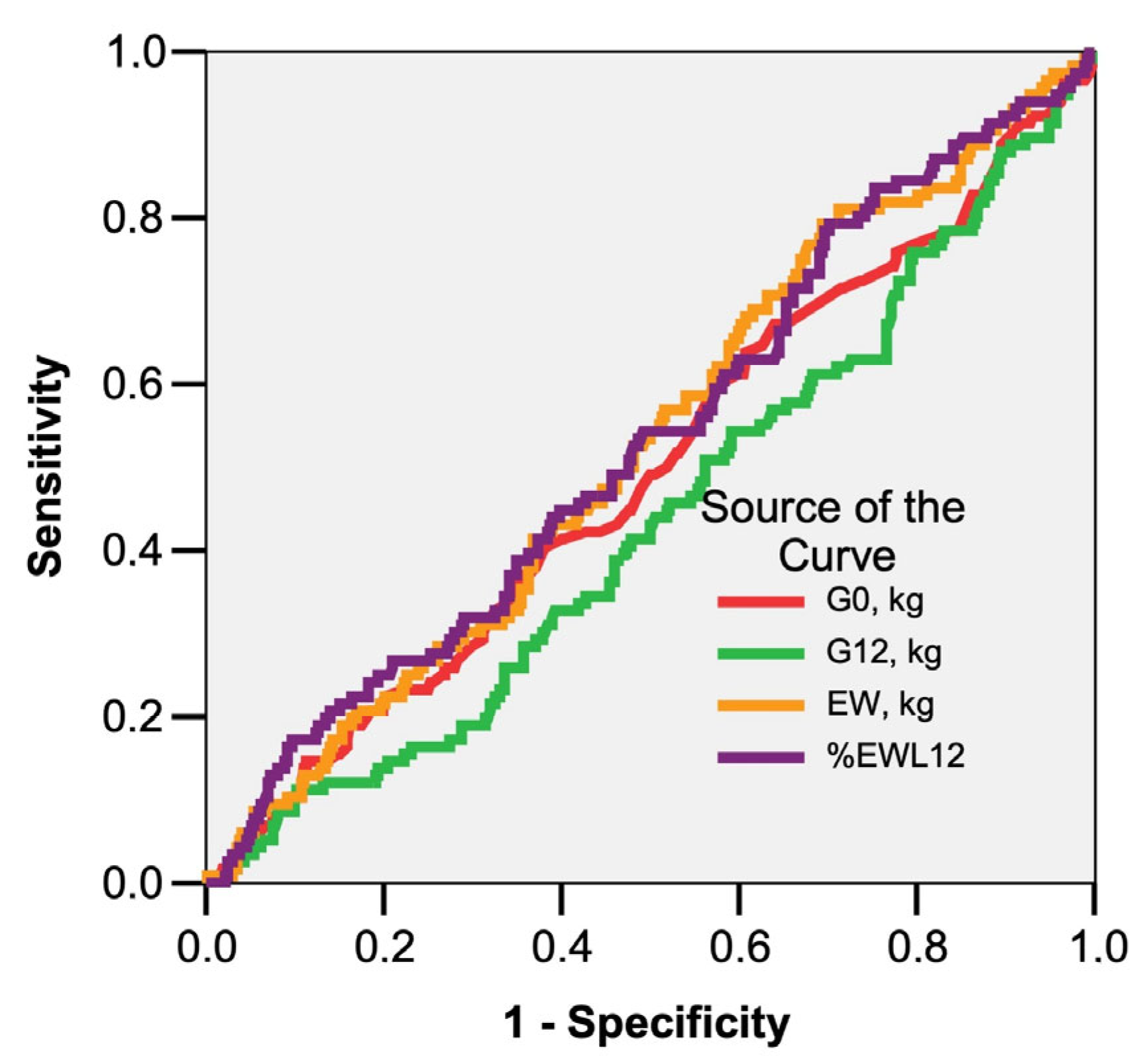
- Body Mass Index (BMI) = Weight (kg)/Height2 (m);
- Ideal Body Weight (IBW) = 50 + [0.91 × (height in cm − 152.4)] in men;
- Ideal Body Weight (IBW) = 45.5 + [0.91 × (height in cm − 152.4)] in women;
- Excess Weight (EW) = Actual weight − IBW;
- Percentage of Weight Loss (%EWL) = (postoperative weight loss)/(preoperative EW) × 100.
4. Discussion
- complete T2DM remission—fasting plasma glucose < 100 mg/dL and/or HbA1c < 6% for at least 1 year after surgery in the absence of glucose-lowering pharmacologic treatment;
- partial T2DM remission—fasting plasma glucose < 126 mg/dL and/or HbA1c < 6.5% without antidiabetic medication for at least 1 year.
- patients with a BMI > 35 kg/m2 with or without coexisting medical conditions and who do not present a high anaesthetic-surgical risk;
- patients with a BMI of 30–34.9 kg/m2 with one or more obesity-related comorbidities or with a significant impairment in quality of life (T2DM, essential hypertension, dyslipidaemia, sleep apnoea syndrome or NAFLD).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tuljapurkar, S. Future Mortality: A Bumpy Road to Shangri-La? Sci. Aging Knowl. Environ. 2005, 2005, pe9. [Google Scholar] [CrossRef]
- Colquitt, J.L.; Pickett, K.; Loveman, E.; Frampton, G.K. Surgery for Weight Loss in Adults. Cochrane Database Syst. Rev. 2014, 2014, CD003641. [Google Scholar] [CrossRef]
- Courcoulas, A.P.; King, W.C.; Belle, S.H.; Berk, P.; Flum, D.R.; Garcia, L.; Gourash, W.; Horlick, M.; Mitchell, J.E.; Pomp, A.; et al. Seven-Year Weight Trajectories and Health Outcomes in the Longitudinal Assessment of Bariatric Surgery (LABS) Study. JAMA Surg. 2018, 153, 427–434. [Google Scholar] [CrossRef]
- Jakobsen, G.S.; Småstuen, M.C.; Sandbu, R.; Nordstrand, N.; Hofsø, D.; Lindberg, M.; Hertel, J.K.; Hjelmesæth, J. Association of Bariatric Surgery vs Medical Obesity Treatment With Long-Term Medical Complications and Obesity-Related Comorbidities. JAMA 2018, 319, 291–301. [Google Scholar] [CrossRef]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 16 February 2023).
- De Lorenzo, A.; Romano, L.; Di Renzo, L.; Di Lorenzo, N.; Cenname, G.; Gualtieri, P. Obesity: A Preventable, Treatable, but Relapsing Disease. Nutrition 2020, 71, 110615. [Google Scholar] [CrossRef]
- Schauer, P.R.; Bhatt, D.L.; Kirwan, J.P.; Wolski, K.; Aminian, A.; Brethauer, S.A.; Navaneethan, S.D.; Singh, R.P.; Pothier, C.E.; Nissen, S.E.; et al. Bariatric Surgery versus Intensive Medical Therapy for Diabetes—5-Year Outcomes. N. Engl. J. Med. 2017, 376, 641–651. [Google Scholar] [CrossRef]
- Ribaric, G.; Buchwald, J.N.; McGlennon, T.W. Diabetes and Weight in Comparative Studies of Bariatric Surgery vs Conventional Medical Therapy: A Systematic Review and Meta-Analysis. Obes. Surg. 2014, 24, 437–455. [Google Scholar] [CrossRef]
- Ikramuddin, S.; Korner, J.; Lee, W.-J.; Thomas, A.J.; Connett, J.E.; Bantle, J.P.; Leslie, D.B.; Wang, Q.; Inabnet, W.B.; Jeffery, R.W.; et al. Lifestyle Intervention and Medical Management With vs Without Roux-En-Y Gastric Bypass and Control of Hemoglobin A1c, LDL Cholesterol, and Systolic Blood Pressure at 5 Years in the Diabetes Surgery Study. JAMA 2018, 319, 266–278. [Google Scholar] [CrossRef]
- Ghiassi, S.; Morton, J.M. Safety and Efficacy of Bariatric and Metabolic Surgery. Curr. Obes. Rep. 2020, 9, 159–164. [Google Scholar] [CrossRef]
- Moon, R.C.; Alkhairi, L.; Wier, A.J.; Teixeira, A.F.; Jawad, M.A. Conversions of Roux-En-Y Gastric Bypass to Duodenal Switch (SADI-S and BPD-DS) for Weight Regain. Surg. Endosc. 2020, 34, 4422–4428. [Google Scholar] [CrossRef]
- Melissas, J.; Stavroulakis, K.; Tzikoulis, V.; Peristeri, A.; Papadakis, J.A.; Pazouki, A.; Khalaj, A.; Kabir, A. Sleeve Gastrectomy vs Roux-En-Y Gastric Bypass. Data from IFSO-European Chapter Center of Excellence Program. Obes. Surg. 2017, 27, 847–855. [Google Scholar] [CrossRef]
- Adams, T.D.; Davidson, L.E.; Litwin, S.E.; Kim, J.; Kolotkin, R.L.; Nanjee, M.N.; Gutierrez, J.M.; Frogley, S.J.; Ibele, A.R.; Brinton, E.A.; et al. Weight and Metabolic Outcomes 12 Years after Gastric Bypass. N. Engl. J. Med. 2017, 377, 1143–1155. [Google Scholar] [CrossRef]
- Abdelgawad, M.; Elgeidie, A.; Sorogy, M.E.; Elrefai, M.; Hamed, H.; El-Magd, E.-S.A. Long-Term Outcomes of Laparoscopic Gastric Plication for Treatment of Morbid Obesity: A Single-Center Experience. Obes. Surg. 2022, 32, 3324–3331. [Google Scholar] [CrossRef]
- Lari, E.; Burhamah, W.; Lari, A.; Alsaeed, T.; Al-Yaqout, K.; Al-Sabah, S. Intra-Gastric Balloons—The Past, Present and Future. Ann. Med. Surg. 2021, 63, 102138. [Google Scholar] [CrossRef]
- Arterburn, D.E.; Telem, D.A.; Kushner, R.F.; Courcoulas, A.P. Benefits and Risks of Bariatric Surgery in Adults: A Review. JAMA 2020, 324, 879–887. [Google Scholar] [CrossRef]
- Chen, G.; Zhang, G.-X.; Peng, B.-Q.; Cheng, Z.; Du, X. Roux-En-Y Gastric Bypass Versus Sleeve Gastrectomy Plus Procedures for Treatment of Morbid Obesity: Systematic Review and Meta-Analysis. Obes. Surg. 2021, 31, 3303–3311. [Google Scholar] [CrossRef]
- de Brito E Silva, M.B.; Tustumi, F.; de Miranda Neto, A.A.; Dantas, A.C.B.; Santo, M.A.; Cecconello, I. Gastric Bypass Compared with Sleeve Gastrectomy for Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Obes. Surg. 2021, 31, 2762–2772. [Google Scholar] [CrossRef]
- Meneses, E.; Zagales, I.; Fanfan, D.; Zagales, R.; McKenney, M.; Elkbuli, A. Surgical, Metabolic, and Prognostic Outcomes for Roux-En-Y Gastric Bypass versus Sleeve Gastrectomy: A Systematic Review. Surg. Obes. Relat. Dis. 2021, 17, 2097–2106. [Google Scholar] [CrossRef]
- Cooper, A.J.; Gupta, S.R.; Moustafa, A.F.; Chao, A.M. Sex/Gender Differences in Obesity Prevalence, Comorbidities, and Treatment. Curr. Obes. Rep. 2021, 10, 458–466. [Google Scholar] [CrossRef]
- Wang, Y.; Beydoun, M.A. The Obesity Epidemic in the United States Gender, Age, Socioeconomic, Racial/Ethnic, and Geographic Characteristics: A Systematic Review and Meta-Regression Analysis. Epidemiol. Rev. 2007, 29, 6–28. [Google Scholar] [CrossRef]
- Carey, M.; Small, H.; Yoong, S.L.; Boyes, A.; Bisquera, A.; Sanson-Fisher, R. Prevalence of Comorbid Depression and Obesity in General Practice: A Cross-Sectional Survey. Br. J. Gen. Pract. 2014, 64, e122–e127. [Google Scholar] [CrossRef]
- Bou Daher, H.; Sharara, A.I. Gastroesophageal Reflux Disease, Obesity and Laparoscopic Sleeve Gastrectomy: The Burning Questions. World J. Gastroenterol. 2019, 25, 4805–4813. [Google Scholar] [CrossRef]
- Popescu, A.-L.; Ioniţa-Radu, F.; Jinga, M.; Gavrilă, A.-I.; Săvulescu, F.-A.; Fierbinţeanu-Braticevici, C. Laparoscopic Sleeve Gastrectomy and Gastroesophageal Reflux. Rom. J. Intern. Med. 2018, 56, 227–232. [Google Scholar] [CrossRef]
- Gomes-Rocha, S.R.; Costa-Pinho, A.M.; Pais-Neto, C.C.; de Araújo Pereira, A.; Nogueiro, J.P.M.; Carneiro, S.P.R.; Santos-Sousa, H.M.T.F.; Lima-da-Costa, E.J.; Bouça-Machado, R.; Preto, J.R.; et al. Roux-En-Y Gastric Bypass Vs Sleeve Gastrectomy in Super Obesity: A Systematic Review and Meta-Analysis. Obes. Surg. 2022, 32, 170–185. [Google Scholar] [CrossRef]
- Mueller, A.; Palilla, S.; Carter, J. Optimal Surgical Treatment for Type 2 Diabetes: Sleeve Gastrectomy or Gastric Bypass? Adv. Surg. 2021, 55, 1–8. [Google Scholar] [CrossRef]
- Peterli, R.; Wölnerhanssen, B.K.; Peters, T.; Vetter, D.; Kröll, D.; Borbély, Y.; Schultes, B.; Beglinger, C.; Drewe, J.; Schiesser, M.; et al. Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-En-Y Gastric Bypass on Weight Loss in Patients With Morbid Obesity: The SM-BOSS Randomized Clinical Trial. JAMA 2018, 319, 255–265. [Google Scholar] [CrossRef]
- Roth, A.E.; Thornley, C.J.; Blackstone, R.P. Outcomes in Bariatric and Metabolic Surgery: An Updated 5-Year Review. Curr. Obes. Rep. 2020, 9, 380–389. [Google Scholar] [CrossRef]
- Buse, J.B.; Caprio, S.; Cefalu, W.T.; Ceriello, A.; Del Prato, S.; Inzucchi, S.E.; McLaughlin, S.; Phillips, G.L.; Robertson, R.P.; Rubino, F.; et al. How Do We Define Cure of Diabetes? Diabetes Care 2009, 32, 2133–2135. [Google Scholar] [CrossRef]
- Mingrone, G.; Panunzi, S.; De Gaetano, A.; Guidone, C.; Iaconelli, A.; Capristo, E.; Chamseddine, G.; Bornstein, S.R.; Rubino, F. Metabolic Surgery versus Conventional Medical Therapy in Patients with Type 2 Diabetes: 10-Year Follow-up of an Open-Label, Single-Centre, Randomised Controlled Trial. Lancet 2021, 397, 293–304. [Google Scholar] [CrossRef]
- Abbasi, J. Unveiling the “Magic” of Diabetes Remission After Weight-Loss Surgery. JAMA 2017, 317, 571–574. [Google Scholar] [CrossRef]
- Koliaki, C.; Liatis, S.; le Roux, C.W.; Kokkinos, A. The Role of Bariatric Surgery to Treat Diabetes: Current Challenges and Perspectives. BMC Endocr. Disord. 2017, 17, 50. [Google Scholar] [CrossRef]
- Panunzi, S.; De Gaetano, A.; Carnicelli, A.; Mingrone, G. Predictors of Remission of Diabetes Mellitus in Severely Obese Individuals Undergoing Bariatric Surgery: Do BMI or Procedure Choice Matter? A Meta-Analysis. Ann. Surg. 2015, 261, 459–467. [Google Scholar] [CrossRef]
- Panunzi, S.; Carlsson, L.; De Gaetano, A.; Peltonen, M.; Rice, T.; Sjöström, L.; Mingrone, G.; Dixon, J.B. Determinants of Diabetes Remission and Glycemic Control After Bariatric Surgery. Diabetes Care 2016, 39, 166–174. [Google Scholar] [CrossRef]
- Eisenberg, D.; Shikora, S.A.; Aarts, E.; Aminian, A.; Angrisani, L.; Cohen, R.V.; de Luca, M.; Faria, S.L.; Goodpaster, K.P.S.; Haddad, A.; et al. 2022 American Society of Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) Indications for Metabolic and Bariatric Surgery. Obes. Surg. 2023, 33, 3–14. [Google Scholar] [CrossRef]
- de Raaff, C.A.L.; Gorter-Stam, M.A.W.; de Vries, N.; Sinha, A.C.; Jaap Bonjer, H.; Chung, F.; Coblijn, U.K.; Dahan, A.; van den Helder, R.S.; Hilgevoord, A.A.J.; et al. Perioperative Management of Obstructive Sleep Apnea in Bariatric Surgery: A Consensus Guideline. Surg. Obes. Relat. Dis. 2017, 13, 1095–1109. [Google Scholar] [CrossRef]
- Furlan, S.F.; Drager, L.F.; Santos, R.N.; Damiani, L.P.; Bersch-Ferreira, A.C.; Miranda, T.A.; Machado, R.H.V.; Santucci, E.V.; Bortolotto, L.A.; Lorenzi-Filho, G.; et al. Three-Year Effects of Bariatric Surgery on Obstructive Sleep Apnea in Patients with Obesity Grade 1 and 2: A Sub-Analysis of the GATEWAY Trial. Int. J. Obes. 2021, 45, 914–917. [Google Scholar] [CrossRef]
- Hariri, K.; Kini, S.U.; Herron, D.M.; Fernandez-Ranvier, G. Resolution of Symptomatic Obstructive Sleep Apnea Not Impacted by Preoperative Body Mass Index, Choice of Operation Between Sleeve Gastrectomy and Roux-En-Y Gastric Bypass Surgery, or Severity. Obes. Surg. 2018, 28, 1402–1407. [Google Scholar] [CrossRef]
- Niroomand, M.; Fotouhi, A.; Irannejad, N.; Hosseinpanah, F. Does High-Dose Vitamin D Supplementation Impact Insulin Resistance and Risk of Development of Diabetes in Patients with Pre-Diabetes? A Double-Blind Randomized Clinical Trial. Diabetes Res. Clin. Pract. 2019, 148, 1–9. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Tsiampalis, T.; Morena, M.; Leung, A.Y.M.; Faka, A.; Chalkias, C.; Tsiodras, S.; Panagiotakos, D. COVID-19 Mortality in Europe, by Latitude and Obesity Status: A Geo-Spatial Analysis in 40 Countries. Nutrients 2022, 14, 471. [Google Scholar] [CrossRef]
- Muniyappa, R.; Gubbi, S. COVID-19 Pandemic, Coronaviruses, and Diabetes Mellitus. Am. J. Physiol. Endocrinol. Metab. 2020, 318, E736–E741. [Google Scholar] [CrossRef]
- Liu, N.; Sun, J.; Wang, X.; Zhang, T.; Zhao, M.; Li, H. Low Vitamin D Status Is Associated with Coronavirus Disease 2019 Outcomes: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2021, 104, 58–64. [Google Scholar] [CrossRef]
- Gesta, S.; Tseng, Y.-H.; Kahn, C.R. Developmental Origin of Fat: Tracking Obesity to Its Source. Cell 2007, 131, 242–256. [Google Scholar] [CrossRef]
- Pinzariu, A.C.; Pasca, S.A.; Sindilar, A.; Drochioi, C.; Balan, M.; Oboroceanu, T.; Niculescu, S.; Crauciuc, D.V.; Crauciuc, E.G.; Luca, A.; et al. Adipose Tissue Remodeling by Prolonged Administration of High Dose of Vitamin D3 in Rats Treated to Prevent Sarcopenia. Rev. Chim. 2017, 68, 2139–2143. [Google Scholar] [CrossRef]
- Pinzariu, A.C.; Oboroceanu, T.; Eloae, F.Z.; Hristov, I.; Costan, V.V.; Labusca, L.; Cianga, P.; Verestiuc, L.; Hanganu, B.; Crauciuc, D.V.; et al. Vitamin D as a Regulator of Adipocyte Differentiation Effects in Vivo and in Vitro. Rev. Chim. 2018, 69, 731–734. [Google Scholar] [CrossRef]
- Gasmi, A.; Bjørklund, G.; Mujawdiya, P.K.; Semenova, Y.; Peana, M.; Dosa, A.; Piscopo, S.; Gasmi Benahmed, A.; Costea, D.O. Micronutrients Deficiences in Patients after Bariatric Surgery. Eur. J. Nutr. 2022, 61, 55–67. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | 1 Month | 3 Months | 6 Months | 12 Months | ||
|---|---|---|---|---|---|---|
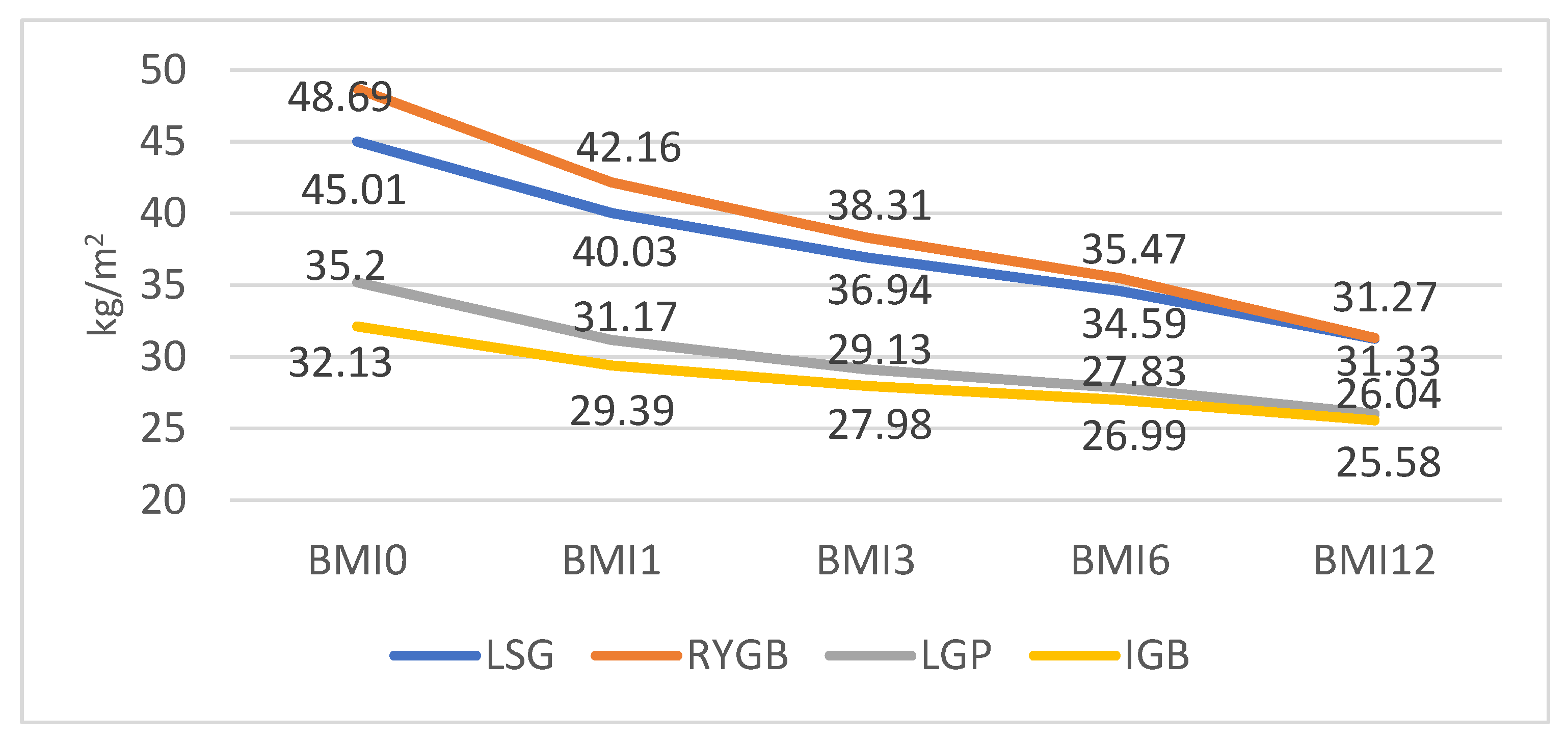
| LSG | 45.01 ± 6.84 | 40.03 ± 6.01 | 36.94 ± 5.46 | 34.59 ± 5.04 | 31.27 ± 4.46 | |
| BMI | RYGB | 48.69 ± 10.81 | 42.16 ± 8.16 | 38.31 ± 6.65 | 35.47 ± 5.71 | 31.33 ± 4.63 |
| kg/m2 | LGP | 35.20 ± 1.92 | 31.17 ± 2.93 | 29.13 ± 2.94 | 27.83 ± 2.96 | 26.04 ± 3.18 |
| IGB | 32.13 ± 1.70 | 29.39 ± 1.55 | 27.98 ± 1.48 | 26.99 ± 1.37 | 25.58 ± 1.30 | |
| LSG | 113.28 ± 63.54 | 95.3 ± 14.87 | 94 ± 12.08 | 88.92 ± 8.7 | 91.3 ± 15.49 | |
| Gluc. | RYGB | 105.16 ± 18.47 | 94.02 ± 24.9 | 91.37 ± 7.17 | 88.3 ± 13.51 | 89.35 ± 17.68 |
| mg/dL | LGP | 102.12 ± 28.2 | 99.73 ± 19.7 | 97.8 ± 15.46 | 94.7 ± 9.31 | 96.49 ± 17.91 |
| IGB | 100.61 ± 20.06 | 98.41 ± 16.53 | 98.29 ± 14.1 | 87.61 ± 17.22 | 93.93 ± 21.71 | |
| LSG | 247.97 ± 46.74 | 237.49 ± 46.1 | 221.91 ± 43.76 | 207.33 ± 42.74 | 193.33 ± 41.51 | |
| Chol. | RYGB | 256.93 ± 39.53 | 245.87 ± 39.99 | 228.9 ± 39.95 | 212 ± 39.82 | 196.13 ± 39.66 |
| mg/dL | LGP | 236.86 ± 39.79 | 228.43 ± 37.56 | 212.14 ± 37.11 | 197.29 ± 35.79 | 184.14 ± 34.04 |
| IGB | 257.25 ± 33.41 | 244.88 ± 33.5 | 228.63 ± 33.34 | 217.88 ± 37.05 | 197.13 ± 33.43 | |
| LSG | 226.53 ± 77.63 | - | 171.67 ± 47.11 | 138.48 ± 28.47 | 97.15 ± 17.38 | |
| LDL | RYGB | 244.63 ± 85.71 | - | 175.57 ± 45.32 | 138.30 ± 25.68 | 100.5 ± 18.59 |
| mg/dL | LGP | 223.29 ± 80.8 | - | 195 ± 45.69 | 146 ± 19.06 | 102.86 ± 17.28 |
| IGB | 242.25 ± 87.6 | - | 197.5 ± 38.72 | 132.75 ± 31.72 | 95.75 ± 23.06 | |
| LSG | 43.84 ± 14.89 | - | 57.58 ± 15.49 | 66.59 ± 15.68 | 74.15 ± 15.84 | |
| HDL | RYGB | 46.33 ± 13.25 | - | 60.60 ± 14.35 | 69.50 ± 14.66 | 77.23 ± 15.27 |
| mg/dL | LGP | 45.29 ± 12.09 | - | 60.86 ± 10.81 | 69.43 ± 11.31 | 78 ± 10.74 |
| IGB | 39.50 ± 18.07 | - | 51.38 ± 17.82 | 61.63 ± 17.16 | 69.88 ± 17.37 | |
| LSG | 350.11 ± 161.2 | 296.33 ± 155.7 | 258.18 ± 150.3 | 233.31 ± 143.4 | 211.18 ± 137.4 | |
| Triglyc. | RYGB | 371.43 ± 151.9 | 321.17 ± 137.4 | 284.1 ± 137.21 | 263.6 ± 130.91 | 242.5 ± 125.86 |
| mg/dL | LGP | 180.86 ± 107.1 | 154 ± 89.95 | 127.29 ± 79.95 | 106.29 ± 73.9 | 104 ± 65.66 |
| IGB | 436.38 ± 111.3 | 356.13 ± 128.1 | 323.38 ± 132.6 | 300.88 ± 134.4 | 286.88 ± 127.9 | |
| LSG | 19.11 ± 9.33 | - | 21.41 ± 11.38 | 29.54 ± 11.44 | 35.47 ± 11.42 | |
| Vit D | RYGB | 18.9 ± 13.21 | - | 21.13 ± 11.87 | 29.40 ± 11.87 | 35.28 ± 11.87 |
| ng/dL | LGP | 20.35 ± 11.27 | - | 24.68 ± 12.67 | 32.95 ± 12.67 | 38.83 ± 12.67 |
| IGB | 20.55 ± 15.84 | - | 21.22 ± 8.2 | 29.49 ± 8.2 | 35.37 ± 9.45 | |
| LSG | 501.20 ± 217.1 | 501.72 ± 215.6 | 488.42 ± 214.2 | 479.03 ± 212.7 | 468.37 ± 211.8 | |
| Vit B12 | RYGB | 440.67 ± 167.9 | 432.8 ± 181.05 | 419.80 ± 181.1 | 408.77 ± 181.1 | 397.67 ± 181.2 |
| pg/dL | LGP | 461.57 ± 292.3 | 477.43 ± 274.1 | 463.00 ± 274.7 | 451.29 ± 274.9 | 438.14 ± 275.8 |
| IGB | 543.25 ± 232.1 | 518.88 ± 228.4 | 501.00 ± 235.3 | 497.25 ± 225.3 | 481.50 ± 231.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soroceanu, R.P.; Timofte, D.V.; Maxim, M.; Platon, R.L.; Vlasceanu, V.; Ciuntu, B.M.; Pinzariu, A.C.; Clim, A.; Soroceanu, A.; Silistraru, I.; et al. Twelve-Month Outcomes in Patients with Obesity Following Bariatric Surgery—A Single Centre Experience. Nutrients 2023, 15, 1134. https://doi.org/10.3390/nu15051134
Soroceanu RP, Timofte DV, Maxim M, Platon RL, Vlasceanu V, Ciuntu BM, Pinzariu AC, Clim A, Soroceanu A, Silistraru I, et al. Twelve-Month Outcomes in Patients with Obesity Following Bariatric Surgery—A Single Centre Experience. Nutrients. 2023; 15(5):1134. https://doi.org/10.3390/nu15051134
Chicago/Turabian StyleSoroceanu, Radu Petru, Daniel Vasile Timofte, Madalina Maxim, Razvan Liviu Platon, Vlad Vlasceanu, Bogdan Mihnea Ciuntu, Alin Constantin Pinzariu, Andreea Clim, Andreea Soroceanu, Ioana Silistraru, and et al. 2023. "Twelve-Month Outcomes in Patients with Obesity Following Bariatric Surgery—A Single Centre Experience" Nutrients 15, no. 5: 1134. https://doi.org/10.3390/nu15051134
APA StyleSoroceanu, R. P., Timofte, D. V., Maxim, M., Platon, R. L., Vlasceanu, V., Ciuntu, B. M., Pinzariu, A. C., Clim, A., Soroceanu, A., Silistraru, I., & Azoicai, D. (2023). Twelve-Month Outcomes in Patients with Obesity Following Bariatric Surgery—A Single Centre Experience. Nutrients, 15(5), 1134. https://doi.org/10.3390/nu15051134