
Does Aging Have an Impact on Vitamin C Status and Requirements? A Scoping Review of Comparative Studies of Aging and Institutionalisation


Abstract
1. Introduction
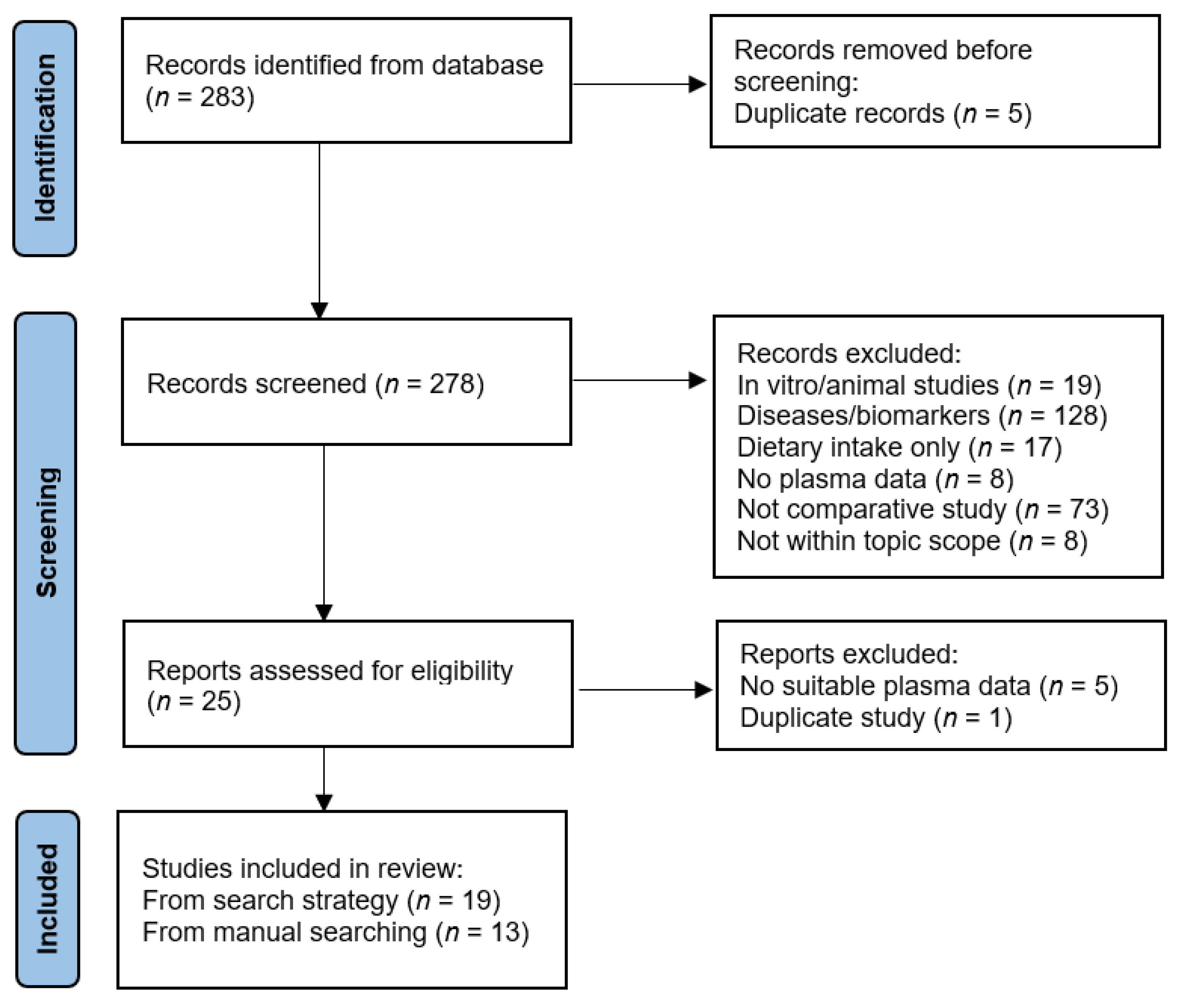
2. Materials and Methods
3. Results
3.1. Vitamin C Status Relative to Age
3.2. Vitamin C Status Relative to Intake Stratified by Age
3.3. Vitamin C Status Relative to Residential Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prince, M.J.; Wu, F.; Guo, Y.; Gutierrez Robledo, L.M.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Cheng, X.; Yang, Y.; Schwebel, D.C.; Liu, Z.; Li, L.; Cheng, P.; Ning, P.; Hu, G. Population ageing and mortality during 1990–2017: A global decomposition analysis. PLoS Med. 2020, 17, e1003138. [Google Scholar] [CrossRef]
- Eggersdorfer, M.; Berger, M.M.; Calder, P.C.; Gombart, A.F.; Ho, E.; Laviano, A.; Meydani, S.N. Perspective: Role of Micronutrients and Omega-3 Long-Chain Polyunsaturated Fatty Acids for Immune Outcomes of Relevance to Infections in Older Adults-A Narrative Review and Call for Action. Adv. Nutr. 2022, 13, 1415–1430. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID-19: People at Increased Risk. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.html (accessed on 28 December 2022).
- Chernoff, R. Micronutrient requirements in older women. Am. J. Clin. Nutr. 2005, 81, 1240s–1245s. [Google Scholar] [CrossRef]
- Carr, A.C.; Maggini, S. Vitamin C and immune function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef]
- Lykkesfeldt, J.; Tveden-Nyborg, P. The pharmacokinetics of vitamin C. Nutrients 2019, 11, 2412. [Google Scholar] [CrossRef]
- Carr, A.C.; Rowe, S. Factors affecting vitamin C status and prevalence of deficiency: A global health perspective. Nutrients 2020, 12, 19. [Google Scholar] [CrossRef]
- Holford, P.; Carr, A.C.; Zawari, M.; Vizcaychipi, M.P. Vitamin C intervention for critical COVID-19: A pragmatic review of the current level of evidence. Life 2021, 11, 1166. [Google Scholar] [CrossRef]
- Travica, N.; Ried, K.; Sali, A.; Scholey, A.; Hudson, I.; Pipingas, A. Vitamin C status and cognitive function: A systematic review. Nutrients 2017, 9, 960. [Google Scholar] [CrossRef]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Dietary intake and blood concentrations of antioxidants and the risk of cardiovascular disease, total cancer, and all-cause mortality: A systematic review and dose-response meta-analysis of prospective studies. Am. J. Clin. Nutr. 2018, 108, 1069–1091. [Google Scholar] [CrossRef]
- Assmann, K.E.; Andreeva, V.A.; Jeandel, C.; Hercberg, S.; Galan, P.; Kesse-Guyot, E. Healthy aging 5 years after a period of daily supplementation with antioxidant nutrients: A post hoc analysis of the French randomized trial SU.VI.MAX. Am. J. Epidemiol. 2015, 182, 694–704. [Google Scholar] [CrossRef]
- Carr, A.C.; Lykkesfeldt, J. Discrepancies in global vitamin C recommendations: A review of RDA criteria and underlying health perspectives. Crit. Rev. Food Sci. Nutr. 2021, 61, 742–755. [Google Scholar] [CrossRef]
- Martin, A. Apports Nutritionnels Conseilles Pour La Population Francaise (Recommended Dietary Intakes for the French Population); AFSSA: Austin, TX, USA, 2001. [Google Scholar]
- European Food Safety Authority Panel on Dietetic Products Nutrition and Allergies. Scientific opinion on dietary reference values for vitamin C. EFSA J. Eur. Food Saf. Auth. 2013, 11, 3418. [Google Scholar] [CrossRef]
- Powers, C.D.; Sternberg, M.R.; Patel, S.B.; Pfeiffer, C.M.; Storandt, R.J.; Schleicher, R.L. Vitamin C status of US adults assessed as part of the National Health and Nutrition Examination Survey remained unchanged between 2003–2006 and 2017–2018. J. Appl. Lab. Med. 2023. [Google Scholar] [CrossRef]
- Crook, J.; Horgas, A.; Yoon, S.J.; Grundmann, O.; Johnson-Mallard, V. Insufficient vitamin C levels among adults in the United States: Results from the NHANES surveys, 2003–2006. Nutrients 2021, 13, 3910. [Google Scholar] [CrossRef]
- Schleicher, R.L.; Carroll, M.D.; Ford, E.S.; Lacher, D.A. Serum vitamin C and the prevalence of vitamin C deficiency in the United States: 2003-2004 National Health and Nutrition Examination Survey (NHANES). Am. J. Clin. Nutr. 2009, 90, 1252–1263. [Google Scholar] [CrossRef] [PubMed]
- Faure, H.; Preziosi, P.; Roussel, A.M.; Bertrais, S.; Galan, P.; Hercberg, S.; Favier, A. Factors influencing blood concentration of retinol, alpha-tocopherol, vitamin C, and beta-carotene in the French participants of the SU.VI.MAX trial. Eur. J. Clin. Nutr. 2006, 60, 706–717. [Google Scholar] [CrossRef]
- Galan, P.; Viteri, F.E.; Bertrais, S.; Czernichow, S.; Faure, H.; Arnaud, J.; Ruffieux, D.; Chenal, S.; Arnault, N.; Favier, A.; et al. Serum concentrations of beta-carotene, vitamins C and E, zinc and selenium are influenced by sex, age, diet, smoking status, alcohol consumption and corpulence in a general French adult population. Eur. J. Clin. Nutr. 2005, 59, 1181–1190. [Google Scholar] [CrossRef]
- Nakamura, Y.K.; Read, M.H.; Elias, J.W.; Omaye, S.T. Oxidation of serum low-density lipoprotein (LDL) and antioxidant status in young and elderly humans. Arch. Gerontol. Geriatr. 2006, 42, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Heseker, H.; Schneider, R. Requirement and supply of vitamin C, E and beta-carotene for elderly men and women. Eur. J. Clin. Nutr. 1994, 48, 118–127. [Google Scholar] [PubMed]
- Newton, H.M.; Schorah, C.J.; Habibzadeh, N.; Morgan, D.B.; Hullin, R.P. The cause and correction of low blood vitamin C concentrations in the elderly. Am. J. Clin. Nutr. 1985, 42, 656–659. [Google Scholar] [CrossRef]
- Sasaki, R.; Kurokawa, T.; Kobayasi, T.; Tero-Kubota, S. Influences of sex and age on serum ascorbic acid. Tohoku J. Exp. Med. 1983, 140, 97–104. [Google Scholar] [CrossRef]
- McClean, H.E.; Dodds, P.M.; Abernethy, M.H.; Stewart, A.W.; Beaven, D.W. Vitamin C concentration in plasma and leucocytes of men related to age and smoking habit. N. Z. Med. J. 1976, 83, 226–229. [Google Scholar]
- Burr, M.L.; Sweetnam, P.M.; Hurley, R.J.; Powell, G.H. Letter: Effects of age and intake on plasma-ascorbic-acid levels. Lancet 1974, 1, 163–164. [Google Scholar] [CrossRef]
- Sharma, Y.; Miller, M.; Shahi, R.; Doyle, A.; Horwood, C.; Hakendorf, P.; Thompson, C. Vitamin C deficiency in Australian hospitalized patients: An observational study. Intern. Med. J. 2019, 49, 189–196. [Google Scholar] [CrossRef]
- Forster, S.; Gariballa, S. Age as a determinant of nutritional status: A cross sectional study. Nutr. J. 2005, 4, 28. [Google Scholar] [CrossRef]
- Jungert, A.; Neuhäuser-Berthold, M. Interrelation between plasma concentrations of vitamins C and E along the trajectory of ageing in consideration of lifestyle and body composition: A longitudinal study over two decades. Nutrients 2020, 12, 2944. [Google Scholar] [CrossRef]
- Ravindran, R.D.; Vashist, P.; Gupta, S.K.; Young, I.S.; Maraini, G.; Camparini, M.; Jayanthi, R.; John, N.; Fitzpatrick, K.E.; Chakravarthy, U.; et al. Prevalence and risk factors for vitamin C deficiency in north and south India: A two centre population based study in people aged 60 years and over. PLoS ONE 2011, 6, e28588. [Google Scholar] [CrossRef]
- Birlouez-Aragon, I.; Delcourt, C.; Tessier, F.; Papoz, L. Associations of age, smoking habits and diabetes with plasma vitamin C of elderly of the POLA study. Int. J. Vitam. Nutr. Res. 2001, 71, 53–59. [Google Scholar] [CrossRef]
- Mecocci, P.; Polidori, M.C.; Troiano, L.; Cherubini, A.; Cecchetti, R.; Pini, G.; Straatman, M.; Monti, D.; Stahl, W.; Sies, H.; et al. Plasma antioxidants and longevity: A study on healthy centenarians. Free Radic. Biol. Med. 2000, 28, 1243–1248. [Google Scholar] [CrossRef]
- Barnes, K.J.; Chen, L.H. Vitamin C status of institutionalized and non-institutionalized elderly in Central Kentucky. Arch. Gerontol. Geriatr. 1990, 10, 123–127. [Google Scholar] [CrossRef]
- Mandal, S.K.; Ray, A.K. Vitamin C status of elderly patients on admission into an assessment geriatric ward. J. Int. Med. Res. 1987, 15, 96–98. [Google Scholar] [CrossRef]
- Blanchard, J.; Conrad, K.A.; Mead, R.A.; Garry, P.J. Vitamin C disposition in young and elderly men. Am. J. Clin. Nutr. 1990, 51, 837–845. [Google Scholar] [CrossRef]
- Blanchard, J.; Conrad, K.A.; Garry, P.J. Effects of age and intake on vitamin C disposition in females. Eur. J. Clin. Nutr. 1990, 44, 447–460. [Google Scholar]
- Blanchard, J.; Conrad, K.A.; Watson, R.R.; Garry, P.J.; Crawley, J.D. Comparison of plasma, mononuclear and polymorphonuclear leucocyte vitamin C levels in young and elderly women during depletion and supplementation. Eur. J. Clin. Nutr. 1989, 43, 97–106. [Google Scholar]
- Murata, A.; Kang, K.; Miyata, S.; Fuji, J.; Tamai, H.; Mino, M.; Itokawa, Y.; Kimura, M. Impaired vitamin C status of hospitalized elderly patients and its improvement by daily multivitamin supplementation. Vitamins 1995, 69, 85–92. [Google Scholar]
- Murata, A.; Lho, I.; Miyata, S.; Tamai, H.; Mino, M.; Kimura, M.; Itokawa, Y. Vitamin C status of elderly patients in a hospital for a long term. Vitamins 1993, 67, 609–616. [Google Scholar]
- Paniz, C.; Bairros, A.; Valentini, J.; Charão, M.; Bulcão, R.; Moro, A.; Grune, T.; Garcia, S.C. The influence of the serum vitamin C levels on oxidative stress biomarkers in elderly women. Clin. Biochem. 2007, 40, 1367–1372. [Google Scholar] [CrossRef]
- Bates, C.J.; Prentice, A.; Cole, T.J.; van der Pols, J.C.; Doyle, W.; Finch, S.; Smithers, G.; Clarke, P.C. Micronutrients: Highlights and research challenges from the 1994-5 National Diet and Nutrition Survey of people aged 65 years and over. Br. J. Nutr. 1999, 82, 7–15. [Google Scholar] [CrossRef]
- Löwik, M.R.; Hulshof, K.F.; Schneijder, P.; Schrijver, J.; Colen, A.A.; van Houten, P. Vitamin C status in elderly women: A comparison between women living in a nursing home and women living independently. J. Am. Diet. Assoc. 1993, 93, 167–172. [Google Scholar] [CrossRef]
- Marazzi, M.C.; Mancinelli, S.; Palombi, L.; Martinoli, L.; D’Alessandro de Luca, E.; Buonomo, E.; Riccardi, F. Vitamin C and nutritional status of institutionalized and noninstitutionalized elderly women in Rome. Int. J. Vitam. Nutr. Res. 1990, 60, 351–359. [Google Scholar] [PubMed]
- Vir, S.C.; Love, A.H. Vitamin C status of institutionalised and non-institutionalised aged. Int. J. Vitam. Nutr. Res. 1978, 48, 274–280. [Google Scholar]
- McClean, H.E.; Stewart, A.W.; Riley, C.G.; Beaven, D.W. Vitamin C status of elderly men in a residential home. N. Z. Med. J. 1977, 86, 379–382. [Google Scholar]
- Teixeira, A.; Carrie, A.S.; Genereau, T.; Herson, S.; Cherin, P. Vitamin C deficiency in elderly hospitalized patients. Am. J. Med. 2001, 111, 502. [Google Scholar] [CrossRef]
- Mishra, S.; Stierman, B.; Gahche, J.J.; Potischman, N. Dietary supplement use among adults: United States, 2017–2018. NCHS Data Brief 2021, 399, 1–8. [Google Scholar]
- Pullar, J.M.; Bayer, S.; Carr, A.C. Appropriate handling, processing and analysis of blood samples is essential to avoid oxidation of vitamin C to dehydroascorbic acid. Antioxidants 2018, 7, E29. [Google Scholar] [CrossRef]
- Brubacher, D.; Moser, U.; Jordan, P. Vitamin C concentrations in plasma as a function of intake: A meta-analysis. Int. J. Vitam. Nutr. Res. 2000, 70, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Viveky, N.; Billinsky, J.; Thorpe, L.; Alcorn, J.; Whiting, S.J.; Hadjistavropoulos, T. Challenges in planning long-term care menus that meet dietary recommendations. Can. J. Diet. Pract. Res. 2013, 74, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Trang, S.; Fraser, J.; Wilkinson, L.; Steckham, K.; Oliphant, H.; Fletcher, H.; Tzianetas, R.; Arcand, J. A multi-center assessment of nutrient levels and foods provided by hospital patient menus. Nutrients 2015, 7, 9256–9264. [Google Scholar] [CrossRef]
- Carr, A.C. Vitamin C in pneumonia and sepsis. In Vitamin C: New Biochemical and Functional Insights; Chen, Q., Vissers, M., Eds.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2020; pp. 115–135. [Google Scholar]
- Lykkesfeldt, J.; Poulsen, H.E. Is vitamin C supplementation beneficial? Lessons learned from randomised controlled trials. Br. J. Nutr. 2010, 103, 1251–1259. [Google Scholar] [CrossRef]
- Carr, A.C.; Bozonet, S.M.; Pullar, J.M.; Simcock, J.W.; Vissers, M.C. Human skeletal muscle ascorbate is highly responsive to changes in vitamin C intake and plasma concentrations. Am. J. Clin. Nutr. 2013, 97, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.; Atkinson, S.J.; Ridge, B.D.; Wyn-Jones, C. A comparison of vitamin C status of elderly in-patients with that of elderly out-patients. Proc. Nutr. Soc. 1973, 32, 45a–46a. [Google Scholar] [PubMed]
- Andrews, J.; Brook, M.; Allen, M.A. Influence of abode and season on the vitamin C status of the elderly. Gerontol. Clin. 1966, 8, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C. Principles of Nutritional Assessment: Vitamin C. In Principles of Nutritional Assessment, 3rd ed.; Gibson, R., Ed.; Open Access, 2022; Available online: https://nutritionalassessment.org/vitaminC/2022 (accessed on 28 December 2022).
- Thomas, A.J.; Briggs, R.S.; Monro, P. Is leucocyte ascorbic acid an unreliable estimate of vitamin C deficiency? Age Ageing 1984, 13, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Bozonet, S.; Pullar, J.; Spencer, E.; Rosengrave, P.; Shaw, G. Neutrophils isolated from septic patients exhibit elevated uptake of vitamin C and normal intracellular concentrations despite a low vitamin C milieu. Antioxidants 2021, 10, 1607. [Google Scholar] [CrossRef] [PubMed]
- Davies, H.E.; Davies, J.E.; Hughes, R.E.; Jones, E. Studies on the absorption of L-xyloascorbic acid (vitamin C) in young and elderly subjects. Hum. Nutr. Clin. Nutr. 1984, 38, 469–471. [Google Scholar]
- Subramanian, V.S.; Sabui, S.; Subramenium, G.A.; Marchant, J.S.; Said, H.M. Tumor Necrosis Factor alpha (TNF-alpha) reduces intestinal vitamin C uptake: A role for NF-kappaB mediated signaling. Am. J. Physiol. Gastrointest. Liver Physiol. 2018, 315, G241–G248. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Population (Location) | n | Age (Years) | Vitamin C Intake (mg/d) | Vitamin C Status (µmol/L) | Vitamin C Deficiency (%) | p-Value a |
|---|---|---|---|---|---|---|---|
| Younger adults vs. older adults | |||||||
| Powers 2023 [16] | 4932 representative sampling of non-institutionalised population (NHANES, USA) | 1463 | 20–39 | NR | 48 (45, 52) | 7 (5, 9) | <0.001 |
| 1563 | 40–59 | 49 (46, 53) | 6 (4, 9) | ||||
| 1906 | ≥60 | 57 (53, 61) | 7 (5, 10) | ||||
| Crook 2021 [17] | 7607 representative sampling of non-institutionalised population (NHANES, USA) | 2751 | 20–39 | NR | NR | 7 ± 1 | |
| 2295 | 40–59 | 8 ± 1 | |||||
| 2561 | ≥60 | 5 ± 1 | <0.001 | ||||
| Schleicher 2009 [18] | 4438 representative sampling of noninstitutionalised population (NHANES, USA) | 725/815 b | 20–39 | NR | 42/49 b | 11/8 b | |
| 628/638 | 40–59 | 43/52 | 11/8 | ||||
| 800/832 | ≥60 | 53/63 | 7/4 | <0.001 | |||
| Faure 2006 [19] | 7074 people enrolled in the SU.VI.MAX study (France) | 109/1798 b | 35–45 | 99/95 b | 53/59 b | NR | |
| 1006/1222 | 45–50 | 101/97 | 54/61 | ||||
| 1375/1349 | 50–60 | 100/98 | 55/61 | ||||
| 113/102 | 60–63 | 104/101 | 54/63 | 0.6 | |||
| Galan 2005 [20] | 3128 people enrolled in the SU.VI.MAX study (France) | NR | <45 | NR | NR/60 b | NR | |
| 45–50 | 50/60 | ||||||
| 50–55 | 50/59 | ||||||
| >55 | 51/62 | 0.6/0.9 b | |||||
| Nakamura 2006 [21] | 76 healthy non-smoking people (USA) | 31 | 19–30 | 297 ± 278 c | 31 ± 8 | NR | |
| 45 | 59–86 | 565 ± 463 | 36 ± 12 | 0.02 | |||
| Heseker 1994 [22] | 2006 healthy people (Germany) | 396/558 b | 18–39 | 101/103 b | RC –0.21/–0.005 b | NR | 0.001/0.4 b |
| 270/370 | 40–59 | 85/101 | |||||
| 196/216 | 60–88 | 87/108 | |||||
| Newton 1985 [23] | 139 young and active older women (UK) | 72 | ~36 | NR | 54 ± 22 | NR | NR |
| 57 | ~73 | 58 (18–156) | 44 ± 28 | ||||
| Sasaki 1983 [24] | 217 healthy people (Japan) | 96/122 b | 12–96 | NR | r –0.453/–0.526 b | NR | <0.001 |
| McClean 1976 [25] | 80 non-smoking men (New Zealand) | 22 | 17–29 | NR | 50 | NR | NR |
| 4 | 30–39 | 64 | |||||
| 17 | 40–49 | 35 | |||||
| 24 | 50–59 | 47 | |||||
| 13 | 60–69 | 40 | |||||
| Burr 1974 [26] | 34 nuns aged >65 and <65 years (UK) | 22 | 19–63 | NR | 40 | NR | |
| 12 | 69–89 | 24 | <0.01 | ||||
| Hospitalised | |||||||
| Sharma 2019 [27] | 147 general medical inpatients (Australia) | 19 | 25–45 | NR | NR | 53 d | 0.03 |
| 28 | 45–65 | 75 | |||||
| 100 | >65 | 82 | |||||
| Forster 2005 [28] | 322 randomly selected hospitalised patients (UK) | 129 | <75 | NR | 21 (19, 36) | NR | |
| 193 | ≥75 | 15 (5, 33) | <0.01 | ||||
| Older adults vs. the very old | |||||||
| Jungert 2020 [29] | 399 people aged ≥60 years (Germany) | 399 | 60–96 | CE 0.001 | CE –0.075 | NR | NS |
| Ravindran 2011 [30] | 7228 randomly sampled clusters of rural and urban populations (India) | 985/1080 c | 60–64 | NR | NR | 69/37 e | |
| 658/864 | 65–69 | 72/39 | |||||
| 552/575 | 70–74 | 81/42 | |||||
| 287/275 | 75–79 | 79/45 | |||||
| 186/176 | ≥80 | 85/51 | <0.001 | ||||
| Birlouez-Aragon 2001 [31] | 1987 people aged >60 years (France) | 189/276 b | 60–64 | NR | ↓/X b | ↑/X b | 0.02/0.2 b |
| 192/251 | 65–69 | ||||||
| 142/253 | 70–74 | ||||||
| 63/118 | 75–79 | ||||||
| 54/86 | >80 | ||||||
| Mecocci 2000 [32] | 107 community-dwelling people (Italy) | 24 | <60 | NR | 58 ± 3 | NR | |
| 34 | 60–79 | 53 ± 3 | |||||
| 17 | 80–99 | 42 ± 2 | <0.01 | ||||
| 32 | ≥100 | 30 ± 2 | <0.01 | ||||
| Barnes 1990 [33] | 139 older people aged 60 to 90 years (USA) | 54 | 60–70 | NR | 79 ± 32 | NR | |
| 56 | 71–80 | 87 ± 37 | |||||
| 29 | 81–90 | 79 ± 44 | NS | ||||
| Mandal 1987 [34] | 277 older people newly admitted to assessment geriatric ward (UK) | 58 | 65–74 | NR | NR | 40 | NR |
| 143 | 75–84 | 40 | |||||
| 76 | ≥85 | 41 | |||||
| Reference | Population (Location) | n | Age (Years) | Vitamin C Dose (mg) and Time | Baseline Vitamin C (µmol/L) | Post-Suppl. Vitamin C (µmol/L) | p Value a |
|---|---|---|---|---|---|---|---|
| Blanchard 1990 [35] | 30 healthy young and older men (USA) | 15 | 25 ± 3 | 500 (4–5 h) | NR | 53 ± 24 | |
| 15 | 69 ± 3 | 500 (4–5 h) | NR | 45 ± 16 | NS | ||
| Blanchard 1990 [36] | 28 healthy young and older women (USA) | 14 | 26 ± 3 | 500 (4–5 h) | NR | 56 ± 27 | |
| 14 | 68 ± 3 | 500 (4–5 h) | NR | 57 ± 24 | NS | ||
| Blanchard 1989 [37] | 16 healthy young and older women (USA) | 8 | 20–29 | 500 (3 wk) | 78 ± 24 | 93 ± 23 | |
| 8 | 65–71 | 500 (3 wk) | 93 ± 40 | 104 ± 15 | NS | ||
| Murata 1995 [38] | 40 long-term hospitalised older people and healthy young adults (Japan) | 20 | 19–40 | 250 (28 d) | 29 ± 9 | 59 ± 10 | |
| 20 | 70–90 | 250 (28 d) | 15 ± 6 | 47 ± 8 | <0.01 | ||
| Murata 1993 [39] | 39 long-term hospitalised older people and healthy young adults (Japan) | 20 | 19–35 | 250 (24 h) | 31 ± 9 | 34 ± 9 | |
| 19 | 66–96 | 250 (24 h) | 17 ± 8 | 19 ± 7 | <0.01 |
| Reference | Population (Location) | n and Residential Status | Age (Years) | Vitamin C Intake (mg/d) | Vitamin C Status (µmol/L) | Vitamin C Deficiency (%) | p Value a |
|---|---|---|---|---|---|---|---|
| Institutionalised vs. community dwelling | |||||||
| Paniz 2007 [40] | 67 older women (Brazil) | 22 non-institutionalised | 68 ± 6 | NR | 76 ± 6 | NR | |
| 45 retirement home | 71 ± 6 | 54 ± 4 | 0.002 | ||||
| Bates 1999 [41] | >1000 older people (NDNS, UK) | >785 free-living | ≥65 | 33% b | 44 ± 25 | 14 | NR |
| >230 institutionalised | ≥65 | 45% | 25 ± 21 | 40 | |||
| Löwik 1993 [42] | 135 older women (the Netherlands) | 52 independent living | ≥65 | 146 ± 75 | 61 ± 21 | 0 | |
| 29 serviced flats | ≥65 | 135 ± 188 | 54 ± 19 | 4 | |||
| 54 nursing home | ≥65 | 55 ± 28 | 24 ± 18 | 35 | <0.001 | ||
| Barnes 1990 [33] | 139 older people (USA) | 89 non-institutionalised | 60–90 | NR | 89 ± 35 | NR | |
| 50 institutionalised | 60–90 | 70 ± 37 | <0.01 | ||||
| Marazzi 1990 [43] | 129 older women (Italy) | 65 non-institutionalised | 60–90 | 102 ± 68 | 59 ± 30 | 2 | |
| 64 institutionalised | 60–90 | 88 ± 42 | 37 ± 24 | 11 | <0.001 | ||
| Newton 1985 [23] | 79 older women (UK) | 57 active older people | ~73 | 58 (18–156) | 44 ± 28 | NR | NR |
| 12 long-stay hospital | ~81 | 14 (9–22) | 13 ± 7 | ||||
| 10 long-stay hospital | ~88 | 26 (7–37) | 10 ± 3 | ||||
| Vir 1978 [44] | 186 older people (Northern Ireland) | 37 home | 70–91 | NR | 22/30 c | 30/23 c | NR |
| 43 hospital | 65–94 | 16/27 | 30/14 | ||||
| 20 sheltered dwelling | 68–89 | 11/27 | 33/13 | ||||
| 26 residential | 65–95 | 10/23 | 67/24 | ||||
| McClean 1977 [45] | 70 older men (New Zealand) | 35 living alone | NR | 31 ± 29 | 26 ± 20 | NR | |
| 35 residential home | >70 | 21 | 16 ± 15 | 83 d | <0.005 | ||
| Hospitalised | |||||||
| Sharma 2019 [27] | 149 general medical inpatients aged ≥18 years (Australia) | 142 home | NR | NR | NR | 75 | |
| 61 home alone | 80 | ||||||
| 7 nursing home | 100 | NS | |||||
| Teixeira 2001 [46] | 50 older patients admitted to internal medicine unit (France) | 50 total cohort e | 80 ± 9 | NR | 18 ± 18 | 88 | |
| 5 nursing home | ≥65 | 7 ± 1 | NR | 0.05 | |||
| Mandal 1987 [34] | 277 patients newly admitted to assessment geriatric ward (UK) | 120 with family | ≥65 | NR | NR | 43 | NR |
| 94 living alone | ≥65 | 33 | |||||
| 20 sheltered residence | ≥65 | 35 | |||||
| 43 institutions | ≥65 | 49 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carr, A.C.; Zawari, M. Does Aging Have an Impact on Vitamin C Status and Requirements? A Scoping Review of Comparative Studies of Aging and Institutionalisation. Nutrients 2023, 15, 915. https://doi.org/10.3390/nu15040915
Carr AC, Zawari M. Does Aging Have an Impact on Vitamin C Status and Requirements? A Scoping Review of Comparative Studies of Aging and Institutionalisation. Nutrients. 2023; 15(4):915. https://doi.org/10.3390/nu15040915
Chicago/Turabian StyleCarr, Anitra C., and Masuma Zawari. 2023. "Does Aging Have an Impact on Vitamin C Status and Requirements? A Scoping Review of Comparative Studies of Aging and Institutionalisation" Nutrients 15, no. 4: 915. https://doi.org/10.3390/nu15040915
APA StyleCarr, A. C., & Zawari, M. (2023). Does Aging Have an Impact on Vitamin C Status and Requirements? A Scoping Review of Comparative Studies of Aging and Institutionalisation. Nutrients, 15(4), 915. https://doi.org/10.3390/nu15040915