
Does Aging Affect Vitamin C Status Relative to Intake? Findings from NHANES 2017–2018



Abstract
1. Introduction
2. Materials and Methods
2.1. NHANES 2017–2018 Cohort
2.2. Demographic and Health Data
2.3. Vitamin C Dietary Intake Data
2.4. Circulating Vitamin C Concentrations
2.5. Data Analyses
3. Results
3.1. Cohort Characteristics
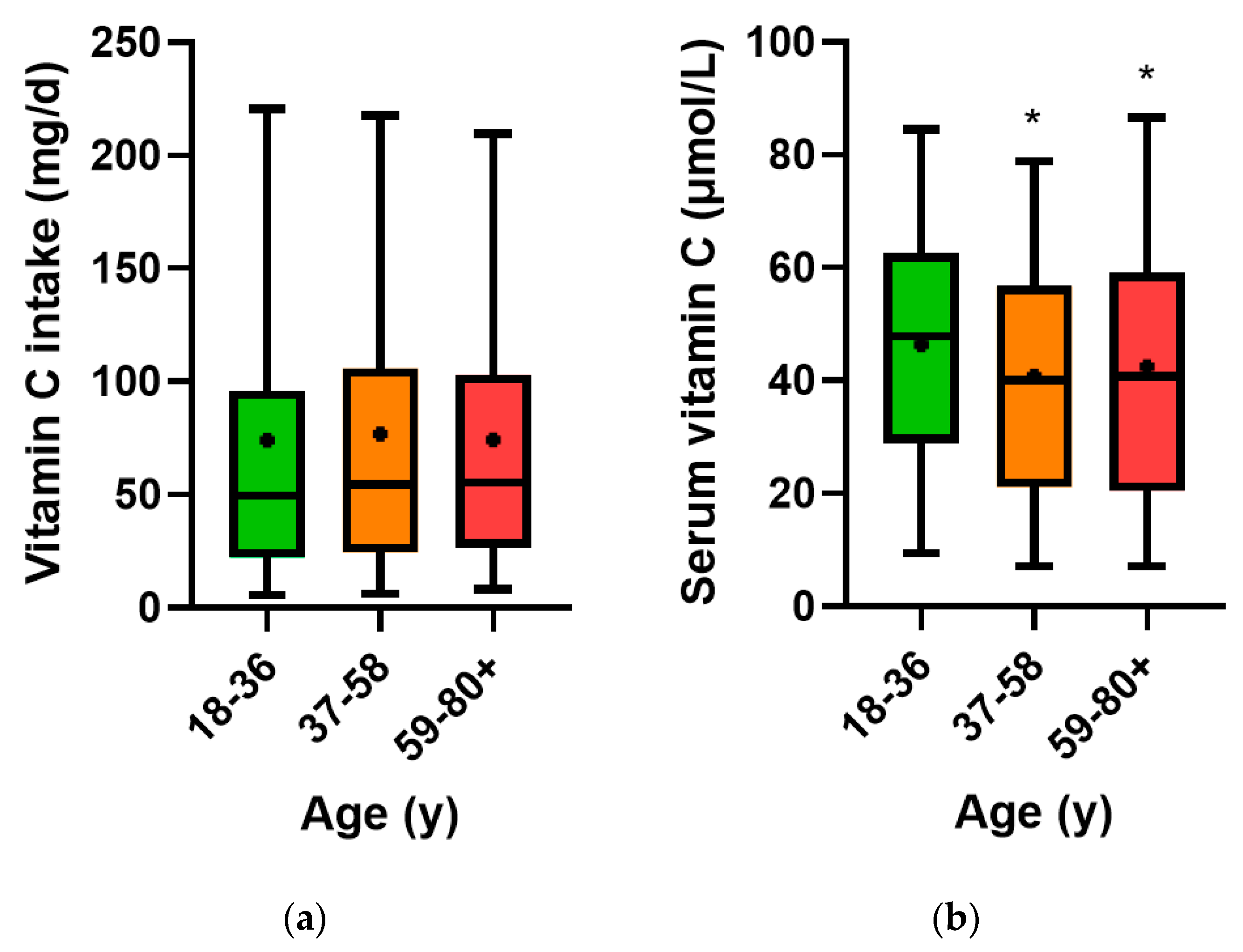
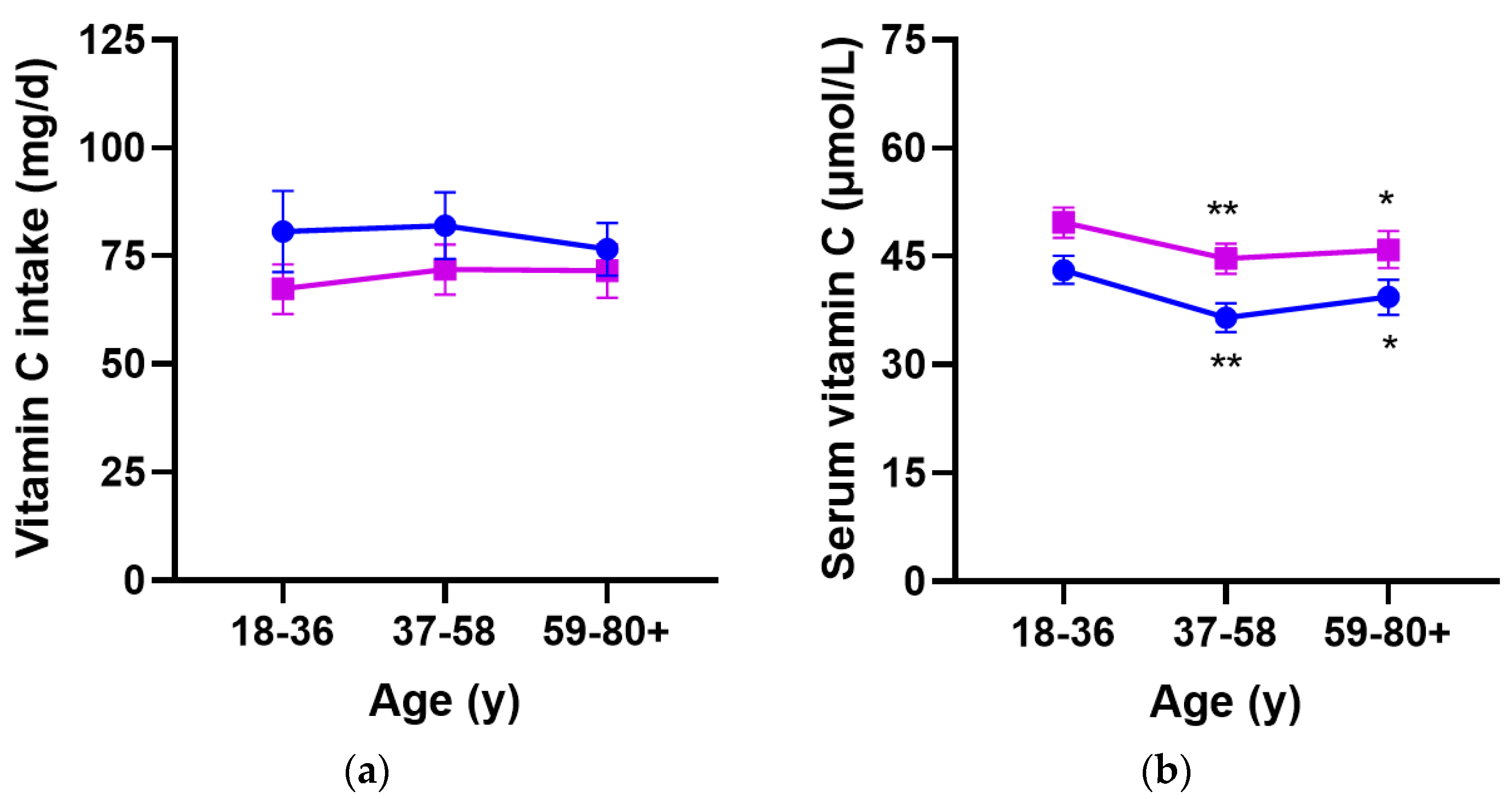
3.2. Vitamin C Intake and Circulating Concentrations Relative to Age
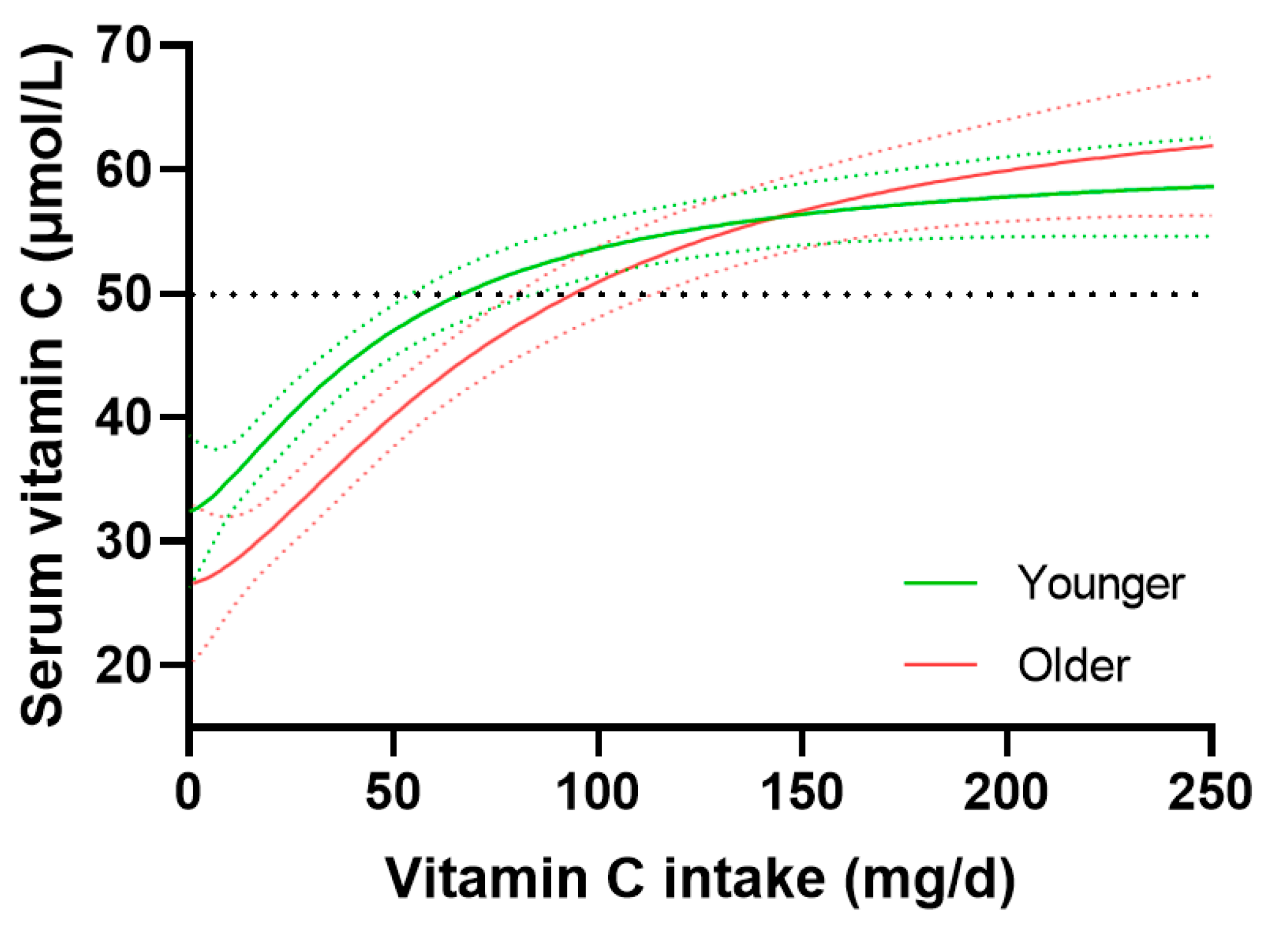
3.3. Vitamin C Dose–Concentration Relationship Relative to Age
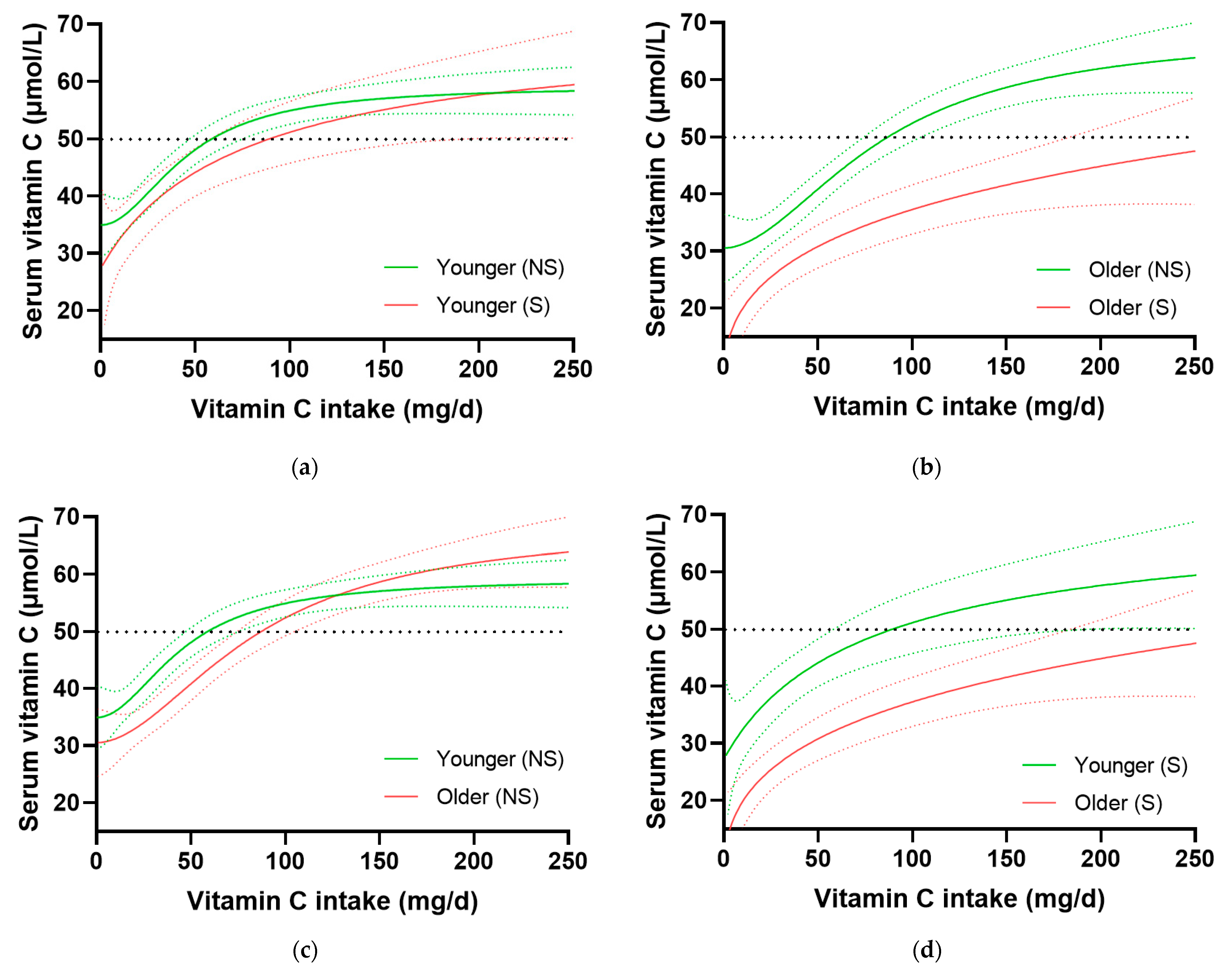
3.4. Impact of Smoking on Age-Related Dose–Concentration Relationship
3.5. Prevalence of Health Conditions in Lower and Higher Intake Groups Relative to Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lykkesfeldt, J. Vitamin C pharmacokinetics. In Vitamin C.; Chen, Q., Vissers, M., Eds.; CRC Press: Boca Raton, FL, USA, 2020; pp. 53–69. [Google Scholar]
- Michels, A.J.; Hagen, T.M. Vitamin C status declines with age. In Vitamin C—Functions and Biochemistry in Animals and Plants; Asard, H., May, J.M., Smirnoff, N., Eds.; Taylor & Francis: London, UK, 2004; pp. 203–227. [Google Scholar]
- Powers, C.D.; Sternberg, M.R.; Patel, S.B.; Pfeiffer, C.M.; Storandt, R.J.; Schleicher, R.L. Vitamin C status of US adults assessed as part of the National Health and Nutrition Examination Survey remained unchanged between 2003–2006 and 2017–2018. J. Appl. Lab. Med. 2023, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Panel on Dietary Antioxidants and Related Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press: Washington, DC, USA, 2000; p. 529. [Google Scholar]
- Carr, A.C.; Lykkesfeldt, J. Discrepancies in global vitamin C recommendations: A review of RDA criteria and underlying health perspectives. Crit. Rev. Food Sci. Nutr. 2020, 61, 742–755. [Google Scholar] [CrossRef] [PubMed]
- Martin, A. Apports Nutritionnels Conseilles Pour la Population Francaise (Recommended Dietary Intakes for the French Population); Tec & Doc: Dijon, Paris, 2001. [Google Scholar]
- European Food Safety Authority Panel on Dietetic Products Nutrition and Allergies. Scientific opinion on dietary reference values for vitamin C. EFSA J. Eur. Food Saf. Auth. 2013, 11, 3418. [Google Scholar] [CrossRef]
- Prince, M.J.; Wu, F.; Guo, Y.; Gutierrez Robledo, L.M.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey 2017–2018. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 29 September 2022).
- Pirkle, J.L. Laboratory Procedure Manual: Vitamin C (Ascorbic Acid) NHANES 2017–2018. CDC Environmental Health: Atlanta, GA, USA, 2020; p. 26. [Google Scholar]
- Lykkesfeldt, J.; Christen, S.; Wallock, L.M.; Chang, H.H.; Jacob, R.A.; Ames, B.N. Ascorbate is depleted by smoking and repleted by moderate supplementation: A study in male smokers and nonsmokers with matched dietary antioxidant intakes. Am. J. Clin. Nutr. 2000, 71, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, J.; Conrad, K.A.; Mead, R.A.; Garry, P.J. Vitamin C disposition in young and elderly men. Am. J. Clin. Nutr. 1990, 51, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, J.; Conrad, K.A.; Garry, P.J. Effects of age and intake on vitamin C disposition in females. Eur. J. Clin. Nutr. 1990, 44, 447–460. [Google Scholar] [PubMed]
- Blanchard, J.; Conrad, K.A.; Watson, R.R.; Garry, P.J.; Crawley, J.D. Comparison of plasma, mononuclear and polymorphonuclear leucocyte vitamin C levels in young and elderly women during depletion and supplementation. Eur. J. Clin. Nutr. 1989, 43, 97–106. [Google Scholar] [PubMed]
- Lykkesfeldt, J.; Viscovich, M.; Poulsen, H.E. Plasma malondialdehyde is induced by smoking: A study with balanced antioxidant profiles. Br. J. Nutr. 2004, 92, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Lykkesfeldt, J. On the effect of vitamin C intake on human health: How to (mis)interprete the clinical evidence. Redox Biol. 2020, 34, 101532. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Karp, J.; Sun, K.M.; Weaver, C.M. Decreasing vitamin C intake, low serum vitamin C level and risk for US adults with diabetes. Nutrients 2022, 14, 3902. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Bozonet, S.M.; Pullar, J.M.; Simcock, J.W.; Vissers, M.C. Human skeletal muscle ascorbate is highly responsive to changes in vitamin C intake and plasma concentrations. Am. J. Clin. Nutr. 2013, 97, 800–807. [Google Scholar] [CrossRef] [PubMed]
- McGregor, G.P.; Biesalski, H.K. Rationale and impact of vitamin C in clinical nutrition. Curr. Opin. Clin. Nutr. Metab. Care 2006, 9, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Bates, C.J.; Prentice, A.; Cole, T.J.; van der Pols, J.C.; Doyle, W.; Finch, S.; Smithers, G.; Clarke, P.C. Micronutrients: Highlights and research challenges from the 1994-5 National Diet and Nutrition Survey of people aged 65 years and over. Br. J. Nutr. 1999, 82, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Löwik, M.R.; Hulshof, K.F.; Schneijder, P.; Schrijver, J.; Colen, A.A.; van Houten, P. Vitamin C status in elderly women: A comparison between women living in a nursing home and women living independently. J. Am. Diet. Assoc. 1993, 93, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Marazzi, M.C.; Mancinelli, S.; Palombi, L.; Martinoli, L.; D’Alessandro de Luca, E.; Buonomo, E.; Riccardi, F. Vitamin C and nutritional status of institutionalized and noninstitutionalized elderly women in Rome. Int. J. Vitam. Nutr. Res. 1990, 60, 351–359. [Google Scholar] [PubMed]
- Newton, H.M.; Schorah, C.J.; Habibzadeh, N.; Morgan, D.B.; Hullin, R.P. The cause and correction of low blood vitamin C concentrations in the elderly. Am. J. Clin. Nutr. 1985, 42, 656–659. [Google Scholar] [CrossRef] [PubMed]
- Travica, N.; Ried, K.; Sali, A.; Scholey, A.; Hudson, I.; Pipingas, A. Vitamin C status and cognitive function: A systematic review. Nutrients 2017, 9, 960. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cohort (n = 2828) | Younger Age Group (n = 942) | Middle Age Group (n = 942) | Older Age Group (n = 944) | p-Value Y vs. O 1 |
|---|---|---|---|---|---|
| Age, years: | |||||
| range | 18–80+ | 18–36 | 37–58 | 59–80+ | |
| median (Q1, Q3) | 48 (32, 62) | 26 (25, 32) | 48 (42, 53) | 66 (62, 73) | <0.0001 |
| Sex, n (%): | |||||
| Male | 1425 (50) | 475 (50) | 452 (48) | 498 (53) | |
| Female | 1402 (50) | 467 (50) | 490 (52) | 446 (47) | 0.3 |
| Ethnicity: | |||||
| Non-Hispanic White | 940 (33) | 298 (32) | 281 (30) | 361 (38) | |
| Non-Hispanic Black | 728 (26) | 225 (24) | 235 (25) | 268 (28) | |
| Mexican American | 399 (14) | 143 (15) | 149 (16) | 107 (11) | |
| Non-Hispanic Asian | 328 (12) | 130 (14) | 133 (14) | 65 (7) | |
| Other Hispanic | 281 (10) | 85 (9) | 89 (9) | 107 (11) | |
| Other/Multi-race | 152 (5) | 61 (6) | 55 (6) | 36 (4) | 0.04 |
| Smoker 2 | 681 (25) | 246 (27) | 269 (29) | 166 (18) | <0.0001 |
| Body weight, kg | 80 (68, 97) | 79 (66, 96) | 83 (70, 100) | 80 (69, 95) | 0.3 |
| Body mass index, kg/m2 | 29 (25, 34) | 28 (23, 34) | 30 (26, 35) | 29 (26,34) | <0.0001 |
| Vitamin C intake, mg/d | 53 (24, 102) | 50 (22, 96) | 54 (25, 106) | 55 (27, 103) | 0.03 |
| Serum vitamin C, µmol/L | 43 (23, 60) | 48 (29, 63) | 40 (21, 57) | 41 (21, 49) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carr, A.C.; Lykkesfeldt, J. Does Aging Affect Vitamin C Status Relative to Intake? Findings from NHANES 2017–2018. Nutrients 2023, 15, 892. https://doi.org/10.3390/nu15040892
Carr AC, Lykkesfeldt J. Does Aging Affect Vitamin C Status Relative to Intake? Findings from NHANES 2017–2018. Nutrients. 2023; 15(4):892. https://doi.org/10.3390/nu15040892
Chicago/Turabian StyleCarr, Anitra C., and Jens Lykkesfeldt. 2023. "Does Aging Affect Vitamin C Status Relative to Intake? Findings from NHANES 2017–2018" Nutrients 15, no. 4: 892. https://doi.org/10.3390/nu15040892
APA StyleCarr, A. C., & Lykkesfeldt, J. (2023). Does Aging Affect Vitamin C Status Relative to Intake? Findings from NHANES 2017–2018. Nutrients, 15(4), 892. https://doi.org/10.3390/nu15040892